

Abstract
Background
Despite specific initiatives and identified needs, most neonatal drugs are still used off-label, with variable dosage administrations and schedules. In high risk preterm and term neonates, drug evaluation is challenging and randomized controlled trials (RCT) are difficult to conduct and even more is the use of a placebo, required in the absence of a reference validated drug to be used as comparator.
Methods
We analyzed the complete ClinicalTrials.gov registry 1) to describe neonatal RCT involving a placebo, 2) to report on the medical context and ethical aspects of placebo use.
Results
Placebo versus drug RCT (n = 146), either prevention trials (n = 57, 39%) or therapeutic interventions (n = 89, 61%), represent more than a third of neonatal trials registered in the National Institute of Health clinical trial database (USA) since 1999. They mainly concerned preterm infants, evaluating complications of prematurity. Most trials were conducted in the USA, were single centered, and funded by non-profit organizations. For the three top drug trials evaluating steroids (n = 13, 9.6%), erythropoietin (EPO, n = 10, 6.8%) and nitric oxide (NO, n = 9, 6.2%), the objectives of the trial and follow-up were analyzed in more details.
Conclusion
Although a matter of debate, the use of placebo should be promoted in neonates to evaluate a potential new treatment, in the absence of reference drug. Analysis of the trials evaluating steroids showed that long-term follow-up of exposed patients, although required by international guidelines, is frequently missing and should be planned to collect additional information and optimize drug evaluation in these high-risk patients.
Introduction
Neonates are highly vulnerable compared to older children and adults: preterm and term neonates are characterized by different degrees of physiological immaturity, they develop specific diseases, need adapted drug formulations and dosages, have different responses to drugs and specific risks of adverse events [1–3]. Accordingly, specific drug evaluation is required in neonates and protocols should include short and long term safety studies.
Despite specific initiatives and identified needs [4–6], more than 90% of neonatal drugs are still used unlicensed or off-labeled, with variable dosage administrations and schedules [7–10].
According to the Food and Drug Administration (FDA) and European Medicine Agency (EMA) pediatric decision tree, drug evaluation in pediatrics, including in neonates, has to be optimized by analyzing all available preclinical and clinical data in adults and children, by adapting drug evaluation to diseases specificity related to prematurity, to developmental differences in drug disposition and effects between neonatal age groups, and by considering all ethical issues [11–13]. In addition, the opportunity to use an adaptive trial design that is potentially able to reduce the number of patients to be included in drug trials should be considered, although not frequently used in neonatology until now. [14,15]
Randomized controlled trials (RCT) remain the gold standard for drug evaluation [16,17] but they are challenging and even more is the use of a placebo, required in the absence of a reference validated drug to be used as comparator.
During our previous report on neonatal drug trials registered in the ClinicalTrials.gov database, the number of clinical trials using a placebo appeared surprisingly high [18].Therefore, we further analyzed the studies during which a placebo was administered in order to report on the medical context and ethical aspects of placebo use in neonates.
Methods
Search strategy
We analyzed the complete ClinicalTrials.gov registry between its launch in 1999 and December 31st, 2015. A total of 206 629 records of clinical trials from more than 100 countries were registered. We searched for all records that involved neonates: the registry categorizes age at which participants are eligible for enrollment as child (≤ 17 years), adult (18 to 65 years) and senior (≥ 66 years). To select the records of interest, we used "neonates and drugs" as search words in the free text section and only phases I to IV were selected.
Study selection
Records were analysed individually, evaluated for relevance and duplicates were removed. The initial selection was made by one researcher (ED), deletions or classification were all confirmed by a second researcher (EJA). The characteristics of neonatal recruitment were selected and analysed for all trials that included term and preterm neonates. Only placebo RCT based on study analysis were selected. Therefore, trials were not included if they were not limited to neonates, were not randomised or did not have a placebo arm.
Data extraction
Data were extracted, using a standard extraction form validated previously [18] including study settings, year of beginning and estimated duration, location and number of participating centers, recruitment status (ongoing, completed and suspended), study design, number of participants and characteristics of the population (term, preterm), condition under study, trial phase, drug under testing and comparison treatments, main purpose of study (prevention or curative treatment), previous publication title, and indication of drug use.
The primary sponsor was classified as governmental (NIH, US federal and governments from non-US countries), industry, and non-profit organizations (including clinical research networks, research associations, hospitals, universities, foundations and others).
Drugs were coded according to the Anatomical Therapeutic and Chemical (ATC) classification [19]
Data was extracted from information included in the database. Terms as placebo, prevention and treatment data were individually analyzed after the first extraction, based on ClinicalTrials.gov definition of terms. Placebo is defined as a substance that does not contain active ingredients and is made to be physically indistinguishable (that looks and tastes identical) from the actual drug being studied. Treatment purpose is defined as a protocol designed to evaluate one or more interventions for treating a disease, syndrome or condition. Prevention is defined as a protocol designed to assess one or more interventions aimed at preventing the development of a specific disease or health condition.
Statistical analysis
To facilitate the analysis a database was subsequently designed, and Statistical analysis was done using Excel program. Results are given in number, mean and standard deviation and percentage.
Results
General overview of neonatal placebo/drug trials
Among all (n = 206 629) drug trials registered in ClinicalTrials.gov since 1999, 423 were neonatal therapeutic trials, 146 were drug versus placebo trials involving neonates and represented 34.4% of all therapeutic trials on neonates (Fig 1), 16 and 22 were registered before 2000 and 2005 respectively, 45 between 2006–2010 and 61 between 2011–2015.
Fig 1. Flow chart of ClinicalTrials.gov registry analysis.
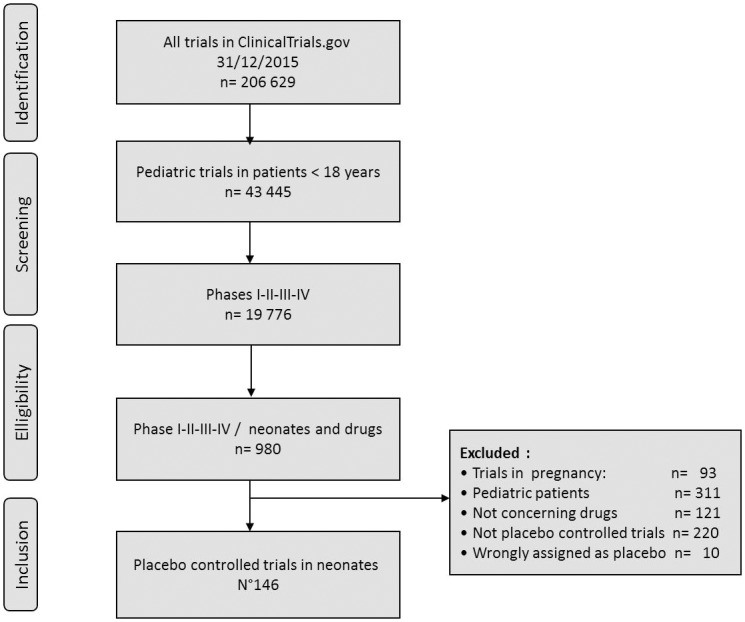
All trials were randomized, blinded (n = 144/146, 98%), double (n = 123, 84.2%) or triple arms (n = 23, 15.8%) and classified phases 1 and 1/2 to phase 4. The number of patients to be included was 299 ± 296 (mean ± SD, range: 7–14035 n = 142) but most trials planned to include less than 100 patients (n = 77, 52.7%). Among the 146 trials, 91 (62.3%) were completed, 21 (14.4%) were still recruiting, 34 (23.3%) were either not recruiting or with unknown status. “Table 1”
Table 1. Characteristics of placebo randomized controlled trials registered in ClinicalTrials.gov (1999–2015).
| N | % | |
|---|---|---|
| TOTAL NUMBER OF TRIALS | 146 | 100.0 |
| NEONATES STUDIED | ||
| Preterm | 70 | 47.9 |
| Term | 35 | 24.0 |
| Preterm and Term | 41 | 28.1 |
| NUMBER OF PATIENTS PLANNED | ||
| 0–50 | 35 | 24.6 |
| 51 to 100 | 42 | 29.5 |
| >100 | 65 | 45.7 |
| unknown | 4 | 0.2 |
| SPONSOR (N) | ||
| Industry | 21 | 14.4 |
| Government* | 22 | 15.0 |
| Non-federal/Non-profit1 | 81 | 55.5 |
| Government+Industry | 2 | 1.4 |
| Non-federal/Non-profit+ Industry | 9 | 6.2 |
| Non-federal/Non-profit+Government | 10 | 6.8 |
| Non-federal+Industry+Governement | 1 | 0.7 |
| STUDY PHASES | ||
| Phases 1 and 1/2 | 21 | 14.4 |
| Phases 2 and 2/3 | 57 | 39.0 |
| Phase 3 | 40 | 27.4 |
| Phase 4 | 28 | 19.2 |
| BLINDING | ||
| Blinded | 144 | 98.6 |
| Open label | 2 | 1.4 |
| LOCATION (N) | ||
| SINGLE CENTER | 81 | 55.5 |
| Africa | 2 | 2.5 |
| Middle East Asia | 22 | 27.2 |
| Europe | 18 | 22.2 |
| North America | 35 | 43.2 |
| South America | 4 | 4.9 |
| Oceania | 0 | 0 |
| MULTICENTER NATIONAL TRIALS | 43 | 29.5 |
| Europa | 4 | 9.3 |
| North America | 38 | 88.4 |
| Asia | 1 | 2.3 |
| MULTICENTER INTERNATIONAL TRIALS | 10 | 6.8 |
| Africa | 1 | 10.0 |
| Middle East Asia | 3 | 30.0 |
| Europe | 10 | 100.0 |
| North America | 5 | 50.0 |
| South America | 1 | 10.0 |
| Oceania | 2 | 20.0 |
| UNKNOWN | 12 | 8.2 |
| RECRUITMENT STATUS2 | ||
| Open—recruiting | 21 | 14.4 |
| Open—not recruiting | 15 | 10.3 |
| Completed | 91 | 62.3 |
| Unknown | 19 | 13.0 |
| LENGHT OF STUDY (as planned—years) | ||
| <1 | 40 | 27.4 |
| 1–2 | 56 | 38.4 |
| 3–4 | 25 | 17.1 |
| >4 | 25 | 17.1 |
| Unknown | 0 | 0.0 |
| PUBLICATION*2 | ||
| Yes | 58 | 39.7 |
| Patients reported in the publication versus planned in the trial | ||
| ± 10% of planned | 35 | 24.0 |
| More than 10% higher | 15 | 10.2 |
| More than 10% lower | 8 | 5.5 |
| No | 88 | 60.3 |
* GOVERNMENT = all the Governmental Institutions + US Federal Agency + NIH (National Institute of Health)
1 NON-FEDERAL = University+ Organization+ Hospital+ Clinical Research Network
2 Updated in December 2017
Trials involving a placebo were conducted with two distinct neonatal strategies: a preventive strategy was evaluated in 57 trials (39.0%), and a therapeutic strategy with evaluation of a “new drug” or a “new indication” in 89 curative trials (61.0%), following different study designs (Table 2). In addition, a few studies were safety studies or modifications of dosages schedules (n = 17, 11.4%).
Table 2. Classification of the placebo–controlled drug trials in neonates in ClinicalTrials.gov (1999–2015) according to design and aim.
| Strategy | Total | Curative Treatment | Disease Prevention |
|---|---|---|---|
| 146 | 89 | 57 | |
| Design | N = 146 | ||
| Placebo versus drug parallel assignement | 105 | 58 | 47 |
| Placebo versus drug trial as add-on therapy | 36 | 25 | 11 |
| Factorial design | 3 | 3 | 0 |
| Cross-over | 2 | 2 | 0 |
| Aim | N = 146 | ||
| Efficacy—Safety | 117 | 64 | 53 |
| Efficacy with rescue treatment | 12 | 11 | 1 |
| Pharmacokinetics | 17 | 15 | 2 |
Neonatal groups and aims
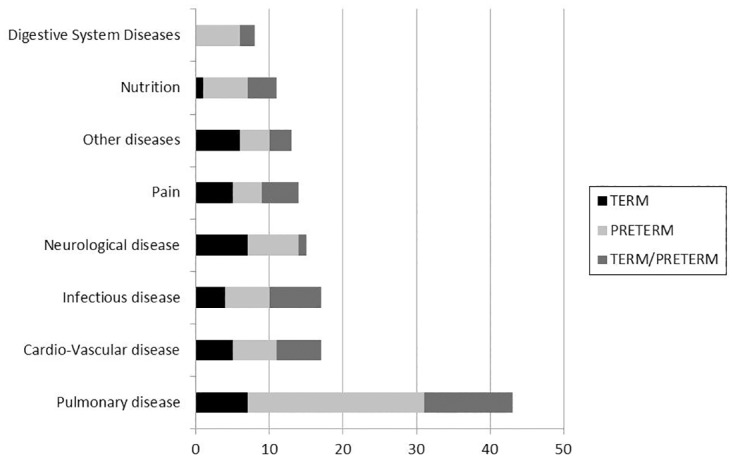
Thirty-five (24.0%) of the trials included exclusively term newborns while 70 (47.9%) and 41 (28.1%) included premature newborns or both preterm and term newborns respectively. Altogether, preterm were present in 111 (76.0%) studies.
Diseases and conditions were different between preterm and term neonates (Fig 2).
Fig 2. Differences in the diseases and conditions between preterm and term neonates in the placebo—drug trials registered in ClinicalTrials.gov.
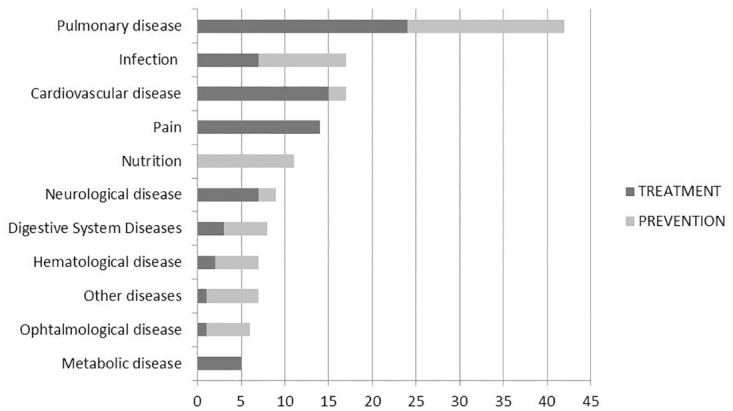
Most trials focused on prevention or treatment of complications of prematurity: bronchopulmonary dysplasia (BPD), enterocolitis, viral and fungal infections, retinopathy or anemia of prematurity (Fig 3).
Fig 3. Differences in neonatal diseases and conditions evaluated in the prevention or treatment placebo—drug trials registered in ClinicalTrials.gov.
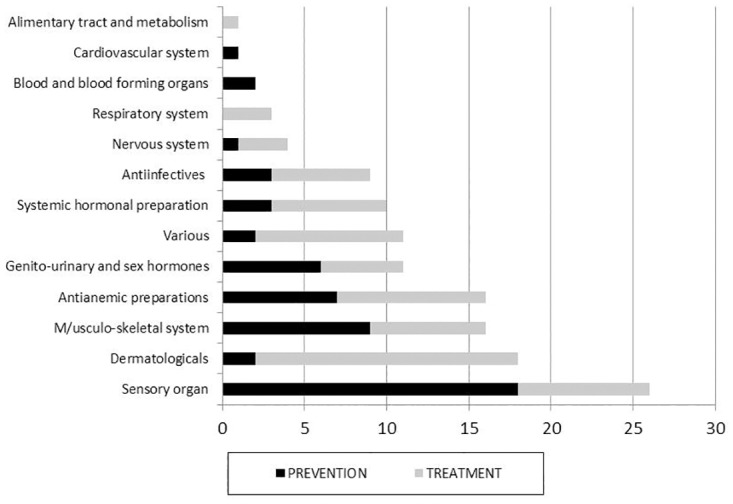
Eighty-three different drugs were under evaluation. ATC classification of the drugs evaluated in these trials is presented in Fig 4.
Fig 4. ATC classification of the drugs evaluated in the neonatal placebo-drug trials in ClinicalTrials.gov.
The primary aim of the trials was either treatment (n = 89, 61.0%) or disease prevention (n = 57, 39.0%). In both groups, design was predominantly placebo drug parallel assignment (n = 105, 72.0%) or add-on therapy (n = 36, 24.7%).
Both prevention and treatment trials were predominantly efficacy and safety trials with parallel assignment between two arms. A total of 36 (24.7%) trials were add-on studies in which all patients received the experimental drug or the placebo in addition to the currently used treatment. Examples include addition of CC10 or lucinactant to surfactant in respiratory distress syndrome, addition of Nitric Oxide to standard of care in respiratory failure, EMLA alone or in addition to glucose to reduce pain during venipuncture (Table 2). Beside clinical efficacy, 3 placebo-drug trials evaluated a biological endpoint in clinically asymptomatic patients and in 4 studies: after the first phase of recommended duration, patients were randomized into two arms and in the first arm, drug treatment was continued while in the second arm, a placebo was administered ».
Three arm interventions had pharmacokinetics as a primary or secondary endpoint (n = 16, 11.0%) with a placebo arm and arms comparing different doses, or had two treatment arms (reference drug and drug under evaluation) and one placebo arm (n = 8, 5.5%).
Geographical repartition and sponsorship
Most placebo trials took place in North America (n = 78, 53.4%), mainly in the USA and were single center (n = 81, 55.5%).
The multicenter trials were predominantly national trials, conducted in a total of 359 centers. They were predominantly conducted in North America (centers: n = 203, 56.5%), Europe (n = 52, 14.5%) and Asia (n = 48, 13.4%). Only 24 (5.3%) of the multicenter trials were international, mainly in Europe (n = 10) and in the United States (n = 5).
The number of neonatal placebo trial registrations was limited in the late 90’s (from 0–3 per year worldwide) but increased in 2002 (1–2 trials per year) mostly in the USA and the first trials were registered after 2004 in Europe and Asia.
The number of trials involving industry or government as only source of funding were 33 (22.6%) and 22 (15.4%) respectively, but governments with or without non-profit organizations funded at least partially, the majority of the trials (n = 113, 77.4%), both single and multicenter. Sponsors were predominantly non-profit organizations (n = 81, 55.5%), and “multiple funding” were less frequent (n = 22, 15.1%) (Table 1)
Analysis of the top drugs (or lecture of drugs)
The three top drugs were steroids (n = 13, 9.6%), erythropoietin (EPO) (n = 10, 6.8%) and nitric oxide (NO, n = 9, 6.2%).
We analyzed in more details the trials evaluating steroids and NO in prevention of BPD, as this indication is specific to the neonatal age group.
Five different steroid drugs were examined: hydrocortisone (n = 6), methylprednisone (n = 1), inhaled budesonide (n = 4), beclomethasone (n = 1), dexamethasone (n = 1). Some of these trials are completed, some are still recruiting or active but not recruiting. Their objectives were disease prevention or treatment of BPD, acute lung injury or transient tachypnea. Their primary objective was in all cases to compare the short-term effects of the drug versus placebo on respiratory function, cardiovascular or neurological effects. Key publications are available for 8 of the 10 completed trials. (Table 3). [20–27]
Table 3. Detailed analysis of randomized-controlled trials evaluating steroids in neonates.
| N | Start / End of study (years) * | Title / Primary outcome / Long-term follow-up | Trial status** Study Chair (SC) or Principal Investigator (PI) (Publications) |
|---|---|---|---|
| RCT hydrocortisone versus placebo | |||
| 1 | 2001/2005 Prevention trial NCT00004669 |
Phase II Pilot Study of Early Cortisol Replacement to Prevent Bronchopulmonary Dysplasia PO: Estimate (versus placebo) the efficacy of cortisol replacement therapy during the first 12 days of life for prevention of bronchopulmonary dysplasia. LT: no |
Completed SC: KL Watterberg [20] |
| 2 | 2005/2015 Prevention trial lNCT00167544 |
Randomized Trial of Hydrocortisone in Very Preterm High-Risk Infants PO: Total Cerebral Volume as Measured by Volumetric Brain MRI LT: no |
Completed PI: NA Parikh [21] |
| 3 | 2006/2011 Treatment trial NCT00358748 |
Early Use of Hydrocortisone in Hypotensive Very Low Birth Weight Infants. PO: Total cumulative dose of dopamine at 48 hours of study drug administration and by day 7 of life in neonates with gestational age ≤ 30 weeks LT: no |
Completed PI: H Osiovich [22] |
| 4 | 2007/2013 Treatment trial NCT00590018 |
Corticosteroids (hydrocortisone) in postoperative critically ill Neonates With Low Cardiac Output syndrome With Congenital Heart Disease PO: HR, BP, mVO2 to assess cardiac output in patients aged <1month LT: no |
Completed PI: HA Dickerson |
| 5 | 2008/2016 Prevention trial NCT 00623740 |
PREMILOC: Trial to Prevent Bronchopulmonary Dysplasia in Very Preterm Neonates PO: survival without BPD at 36 weeks PMA gestational age, in neonates between 24 weeks and 27 weeks + 6 days gestational age LT: neurodevelopmental outcome at 18 months to 3 years |
Completed PI: O Baud [23] |
| 6 | 2014/2018 Treatment trial NCT01954056 |
Hydrocortisone for Term Hypotension PO: Death or neurodevelopmental impairment 34 Weeks’ gestational age and older LT: Neurodevelopmental Impairment [Birth to 22–26 month corrected age] |
Active—Not recruiting SC: E.Fernandez |
| RCT Budesonide versus placebo | |||
| 7 | 2009/ 2013 Prevention trial NCT00883532 |
Prevention of Chronic Lung Disease (CLD) in Preterm Infants PO: Chronic lung disease morbidity among the survival at 36 postconceptional weeks LT: Neurodevelopment at 2 years of age |
Completed PI: TF Yeh [24] |
| 8 | 2010 /2016 Treatment trial NCT01035190 |
Efficacy and Safety of Inhaled Budesonide in Very Preterm Infants at Risk for Bronchopulmonary Dysplasia PO: To determine whether inhalation of Budesonide within 12 hours of life improves survival without BPD at 36 weeks GA in infants born between 23 and 27 weeks GA LT: neurodevelopment at a corrected age of 18–22 months |
Completed PI: D Bassler [25] |
| 10 | 2012 / 2015 Treatment trial NCT01858129 |
Inhaled Corticosteroids for the Treatment of Transient Tachypnea (TTN) of the Newborn PO: assessment of respiratory distress at 48 hours, reflected by TTN clinical score in Infants Born at >34 Weeks Gestation LT: no |
Recruiting PI: A Kugelman |
| 9 | 2016 / 2018 Prevention trial NCT01895075 |
Inhaled budesonide in non-ventilated infants at high risk of bronchopulmonary dysplasia: the i-BUD pilot study. PO: Total days on supplemental oxygen from birth to discharge LT: no |
Not yet recruiting PI: M Dunn |
| RCT of other corticosteroids versus placebo | |||
| 11 | 1992 / 1994 Treatment trial NCT00011362 |
Dexamethasone Therapy in VLBW Infants at Risk of CLD PO: Number of days from randomization to ventilator independence LT: Morbidity and mortality from respiratory causes during the first year (12 months of age) |
Completed PI: LA Papille [26] |
| 12 | 1993/1999 Prevention trial NCT00000576 |
Inhaled Beclomethasone to Prevent Chronic Lung Disease PO: bronchopulmonary dysplasia at 28 days of age in premature infants (birth weight less than 1251 grams, gestational age less than 33 weeks, and postnatal age 3 to f14 days, under mechanical ventilation LT: no |
Completed [27] |
| 13 | 2014/2017 Treatment trial NCT01757899 |
Effects and Safety of Infusion of Low-Doses of Methylprednisolone in Early ALI and ARDS (Acute Lung Injury and Acute Respiratory Distress Syndrome) in patients up to 17 Years (PEDALI) PO: Effects on pulmonary organ function at 24 months of entry LT: Complications at 12 months of entry (safety issue) |
Recruiting SC: MCM Barbosa |
* estimated year,
** Definitions as provided in Clinicaltrial.gov: Completed: "last subject, last visit" has occurred, Terminated: the clinical study has stopped recruiting or enrolling participants early and will not start again, Participants are no longer being examined or treated.
PO: Primary Objective, LO: Long-term, PI: Principal Investigator, SC: Study Chair
We also analyzed in details the trials evaluating iNO versus placebo (nitrogen gas or oxygen). All but one of these trials had a short-term primary outcome evaluating death and BPD at 36 weeks’ post-menstrual age. The results were published in 5 cases, the other trials are completed or still recruiting (Table 4). [28–33]
Table 4. Detailed analysis of randomized-controlled trials evaluating iNO: Inhaled Nitric Oxide (iNO) in neonates.
| N | Estimated dates of Start / End (years) * | Title / Primary outcome / Long-term follow-up | Trial status** Principal Investigator (PI) (Publications) |
|---|---|---|---|
| 1 | 1995 / 1998 NCT00005776 |
Inhaled Nitric Oxide Study for Respiratory Failure in Newborns (NINOS) PO: Death or initiation of ECMO before hospital discharge or 120 days of life LT: outcome assessed at 18 to 24 mos of age. |
Terminated PI: RA. Ehrenkranz [28] |
| 2 | 2000/2006 NCT00000548 |
Inhaled NO in Prevention of Chronic Lung Disease PO: Survival without chronic lung disease (CLD) [Time Frame: 36 weeks] LT: Neurodevelopmental outcome through two years of age |
Completed PI: Ballard R [29] |
| 3 | 2001 / 2006 NCT00016523 |
Inhaled Nitric Oxide for Preterm Infants With Severe Respiratory Failure (Preemie iNO) PO: Death or Bronchopulmonary Dysplasia at 36 weeks post-conceptional age LT: Neurodevelopmental outcome at 18–22 months corrected age |
Terminated PI: KP Van Meurs [30] |
| 4 | 2002 / 2005 NCT00041548 |
Inhaled Nitric Oxide in Neonates With Elevated A-a DO2 (alveolar-arterial oxygen) Gradients Not Requiring Mechanical Ventilation (gestational age >34 completed weeks) PO: PaO2 level at baseline, then every hour for 6 hours LT: no |
Terminated PI: Waldemar Carlo [31] |
| 5 | 2005 /2016 NCT01220687 |
Safety and Efficacy Study of Nitric Oxide for Inhalation on Chronic Lung Disease in Premature Babies PO: Survival Without Bronchopulmonary Dysplasia (BPD) in Preterm Infants With Respiratory Distress at 36 weeks gestational age LT: no |
Active, not recruiting PI: JCMercier [32] |
| 6 | 2007 / 2016 NCT00955487 |
Examining the use of non-invasive inhaled nitic oxide to reduce chronic lung disease on premature newborns. PO: Combined endpoint of bronchopulmonary dysplasia and mortality [Time Frame: Week 36 or earlier, if participants are discharged from the hospital LT: Long term follow up at 1 and 2 years |
Ongoing, but not recruiting PI: J Kinsella [33] |
| 7 | 2008 / 2016 NCT00515281 |
Inhaled Nitric Oxide and Neuroprotection in Premature Infants PO: Bronchopulmonary dysplasia at 36 weeks of age corrected LT: Neurodevelopment at two years |
Active—not recruiting PI: MD. Schreiber |
| 8 | 2009/2011 NCT00922532 |
Inhaled Nitric Oxide (INO) In Hypoxic Respiratory Failure PO: Arterial Blood Gases [Time Frame: Day 1 through Day 6] LT: no |
Withdrawn prior to enrollment. |
| 9 | 2009 / 2014 NCT00931632 |
Inhaled Nitric Oxide (INO) for the Prevention of Bronchopulmonary Dysplasia (BPD) in Preterm Infants PO: Survival Without BPD at 36 Weeks LT: no |
Completed Study Director: J Baldassarre |
| 10 | 2011 / 2016 NCT01220687 |
Inhaled Nitric Oxide (iNO) as an Adjunct to Neonatal Resuscitation PO: To investigate whether iNO decreases the supplemental oxygen exposure in the preterm infants who require continuous positive airway pressure (CPAP) or positive pressure ventilation (PPV) during resuscitation as per Neonatal Resuscitation Program (NRP) protocol. LT: no |
Recruiting PI: Kris Sekar, |
| 11 | 2013 / 2014 NCT01748045 |
Study of Inhaled Nitric Oxide and Respiratory Outcomes in Late Preterm Infants PO: Primary combined endpoint of alive without the need for intubation or mechanical ventilation within the first week of life LT: no |
Terminated PI: Jennifer W Lee |
| 12 | 2016 / 2017 NCT01891500 |
Early iNO for Oxidative Stress, Vascular Tone and Inflammation in Babies With Hypoxic Respiratory Failure (gestational Gestational age ≥ 35 weeks gestation) PO: Biomarkers of oxidative injury. LT: no |
Not yet open for recruitment PI: C Bazacliu |
* estimated year
** Definitions as provided in Clinicaltrial.gov: Completed: "last subject, last visit" has occurred, Terminated: the clinical study has stopped recruiting or enrolling participants early and will not start again, Participants are no longer being examined or treated.
PO: Primary Objective, LO: Long-term, PI: Principal Investigator
Discussion
The present study was undertaken to quantify and discuss the use of a placebo in RCTs conducted in neonates. We identified 146 studies registered in ClinicalTrials.gov from 1999 to 2015. Most of them were prevention trials or add-on studies, while evaluation of therapeutic interventions were less frequent. They mainly concerned preterm infants, evaluating management of complications of prematurity. The majority of the trials were conducted in the USA, were single centered and funded by non-profit organizations, mostly hospitals and universities.
A placebo is defined by its lack of specific pharmacological or physiological efficacy for a patient’s condition. When administered during a RCT, accumulated evidence suggests that in the placebo arm, the observed effect is a genuine psychobiological event attributable to the overall therapeutic context. The overall response of the active treatment arm is the result of the treatment itself and the context in which it is given, quantified by the response to placebo, relying on complex neurobiologic mechanisms, influenced by psychosocial factors [34–37].
Our research focused on neonatal placebo versus drug trials, which represent one third of all neonatal trials and became more frequent after 2002, probably framed by the International Ethical Guidelines for Biomedical Research Involving Human Subjects, ensuring the regulation for the use of placebo [38]. Whatever the medical situation and patients’ groups, the use of a placebo remains controversial and rises major ethical concerns both in clinical research and clinical practice [39–42]. It may be an option only if respecting the principle of clinical equipoise and respect of patients’ wellbeing. Therefore, it is important to carefully evaluate the balance between potential benefits and disadvantages of such design to discuss ethical issues [43–45]
According to our data, neonatal randomized placebo-controlled trials are conducted in the two different contexts of disease prevention or treatment: a prevention trial only aims at health benefit without inducing any harm while a treatment trial aims at improving health care, while limiting harm. Here again, the conduct of neonatal placebo trials remains a matter of debate and controversies with arguments «for and against» [6,46,47]. A placebo can only be used when no standard treatment for that disease exists; in other cases, the new drug should be compared with the gold-standard [48]. On one hand, defenders of placebo advocate that both specificity of neonatal diseases and the absence of reference treatment, ie validated comparator, are strong arguments to use a placebo. This is for example the case for a trial evaluating the efficacy of erythropoietin for neuroprotection in very preterm infants
In our research, the majority of trials were dealing with prematurity and specific related complications or concerned prevention or treatment of diseases occurring only in neonates. In such situations, the natural history and pathophysiology of diseases, developmental pharmacology data and identification and validation of relevant biomarkers are required [1,49] and it is difficult to extrapolate both efficacy and safety from data obtained in older children or adults as drugs are frequently used off label [7,50]. Consequently, uncertainty on neonatal efficacy and high risk of adverse events do exist when extrapolation to neonates is used, justifying specific drug evaluation compared to a placebo in the subgroup of pediatric patients [3] On the other hand, for obvious scientific and medical reasons, and even in the absence of a reference treatment, the use of a placebo cannot be envisaged in medical situations that might lead to a “loss of chance” for the patient. Indeed, many drugs enter the neonatal care arena because of proven efficacy in older pediatric patients or even adults, because clinicians perceive them to have a useful spectrum of activity compared to ‘older’ drugs or even in the absence of drug available in the therapeutic indication. In such cases, resorting to an off-label drug is frequent in neonatal care, while administrating a placebo would be questionable. In addition, although a placebo effect was observed in different pediatric studies and quantified as even higher that in adults [49–54], the placebo effect in neonates is not a consensual reality [55,56].
The debate on the use of placebo in neonatal trials requires a deep analysis of all ethical issues to promote and protect newborn health, here again with arguments “for or against” [48,57] For example, a placebo RCT that compares a drug administrated by intra-muscular injection should better be compared to a sham injection rather than an intra-muscular injection of placebo [58]. During our research, 15 placebo RCT targeted analgesics during painful procedures in neonates and 9 did not have any rescue therapy, although newborns do feel pain but even more, have a lower threshold of pain. In such situations, the use of a placebo should be questioned [59]. Indeed, placebo RCT for pain studies in infants might not be the best methodological approach to prove new pharmacological therapies. The “add-on” trial design where the drug under evaluation and the placebo are added to the “empiric therapy” has been used in many trials with pros and cons: among them, such design allows to maintain current therapy and define the effect of empiric therapy in the placebo arm but has additional safety risks
We also analyzed in more details the studies evaluating corticosteroids used for prevention or treatment of specific neonatal diseases (BPD, cardiovascular or neurological diseases), as the recent guidelines state that there are insufficient evidence to recommend both early or late administration [60,61] (S1 Table). However, important and recent data were obtained against placebo for prophylactic low-dose hydrocortisone, showing that in extremely preterm infants, the rate of survival without BPD at 36 weeks’ postmenstrual age was significantly increased, and for early inhaled budesonide showing a lower incidence of BPD at 36 weeks’ postmenstrual age. Although beneficial effects of both early and late corticosteroids were already identified, such placebo/drug RCT were justified by the absence of reference arm, demonstrating significant benefits for both drugs [62,63]. Benefits associated with early hydrocortisone may not overweight the risks of it use although long-term deleterious effects were mainly associated with dexamethasone and not hydrocortisone and potential undesired effects on neurodevelopment at preschool age should be evaluated in future long-term studies [64]
The 14 trials evaluating iNO were analysed in two Cochrane reviews [65,66], and 12 were included in a recent meta-analysis, 5/14 and 6/12 respectively being iNO versus placebo RCTs trials [67]. Neonates presenting with risks factors of deleterious outcome (gestational age, oxygenation index, pulmonary hypertension…) were enrolled and followed up to 36 weeks of age. Guidelines on the use of iNO were issued by the Canadian Paediatric Society and the American Academy of Pediatrics [68–70](S2 Table). Within the recent NIH Consensus Development Conference Statement, future research directions recommend the use of a placebo control when designing future randomized trials to assess optimal iNO treatment (timing, dose and duration), long-term safety (not a primary outcome in the ongoing trials analyzed here) and predictive markers of outcome (biomarkers, neuroimaging) [71].
Placebo trials in neonates are rare. A bias in data analysis might occur 1) if not all trials are reported, especially single site trials involving a relatively small number of infants, 2) if they are not all identified. Therefore, web-based registries are major tools to increase transparency in the conduct of clinical trials. We selected clinicaltrials.gov registry in our initial research [18] and in this complementary analysis, although it does not focus on pediatric trials. However, the registry the registry started more than 15 years ago, it is public and permits the registration of all clinical trials regardless the disease, age group, type of intervention or country, and therefore allows description of the current scope of pediatric and neonatal trials [72] The only pediatric database that we know of was DEC-net. (Drug Evaluation in Children-network), a web- based register of trials on drug therapy in children was supported by the European Commission in 2006: data collection was oriented to the paediatric population, with a clear definition of age groups. The first data analysis was made available in 2008, but the database closed at the end of the project [73,74]. Other registries or platforms have limitations when it comes to pediatric trials: the International Clinical Trials WHO Registry Platform (ICTRP) [75], the EU Clinical Trials Register [76] containing information on interventional clinical trials since 2004. However, to our knowledge, none of them has a focus on paediatric trials and the absence of identification of paediatric age groups does not to analyze the trials recruiting both neonates and other pediatric patients and to separate premature and term neonates.
In addition, the low number of industry-sponsored trials in neonates is of concern [77,78], although legislation was put in place in the USA and Europe to improve this situation [79–83] Following these major changes in the Regulatory framework of pediatric drug evaluation, the number of pediatric trials increased but the impact of the new regulation remains limited [84,85]. Unfortunately, the significant economic benefits to the pharmaceutical industry are not matched by the benefits for pediatric patients. In addition, elaboration of an undifferentiated placebo may be technically difficult and very expensive.
Conclusion
In the clinical trial database setup by the National Institute of Health in the USA [81] placebo controlled RCT represent more than a third of neonatal trials. Although matter of large debates, a placebo is justified to evaluate efficacy of the potential new treatment when no reference drug is available Medical issues, scientific validity, methodological and ethical specificities are to be taken into account in this high risk patients [86] and all the available data should be analyzed to design and conduct such studies.
Supporting information
(DOCX)
(DOCX)
(DOCX)
Data Availability
All relevant data are within the paper and its Supporting Information files.
Funding Statement
The authors received no specific funding for this work.
References
- 1.Kearns GL, Abdel-Rahman SM, Alander SW, Blowey DL, Leeder JS, Kauffman RE. Developmental pharmacology—drug disposition, action, and therapy in infants and children. N Engl J Med. 2003;349: 1157–1167. 10.1056/NEJMra035092 [DOI] [PubMed] [Google Scholar]
- 2.de Wildt SN, Tibboel D, Leeder JS. Drug metabolism for the paediatrician. Arch Dis Child. 2014;99: 1137–1142. 10.1136/archdischild-2013-305212 [DOI] [PubMed] [Google Scholar]
- 3.Belén Rivas A, Arruza L, Pacheco E, Portoles A, Diz J, Vargas E. Adverse drug reactions in neonates: a prospective study. Arch Dis Child. 2016;101: 371–376. 10.1136/archdischild-2015-309396 [DOI] [PubMed] [Google Scholar]
- 4.Giacoia GP, Taylor-Zapata P, Zajicek A. Drug studies in newborns: a therapeutic imperative. Clin Perinatol. 2012;39: 11–23. 10.1016/j.clp.2011.12.016 [DOI] [PubMed] [Google Scholar]
- 5.Jacqz-Aigrain E. Drug policy in Europe Research and funding in neonates: current challenges, future perspectives, new opportunities. Early Hum Dev. 2011;87 Suppl 1: S27–30. [DOI] [PubMed] [Google Scholar]
- 6.Ligi I, Boubred F, Grandvuillemin I, Simeoni U. Clinical research in newborn infants: difficulties and specificity. Eur J Clin Pharmacol. 2011;67 Suppl 1: 29–32. [DOI] [PubMed] [Google Scholar]
- 7.Conroy S, McIntyre J, Choonara I. Unlicensed and off label drug use in neonates. Arch Dis Child Fetal Neonatal Ed. 1999;80: F142-144-145. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Neubert A, Lukas K, Leis T, Dormann H, Brune K, Rascher W. Drug utilisation on a preterm and neonatal intensive care unit in Germany: a prospective, cohort-based analysis. Eur J Clin Pharmacol. 2010;66: 87–95. 10.1007/s00228-009-0722-8 [DOI] [PubMed] [Google Scholar]
- 9.Kaguelidou F, Pandolfini C, Manzoni P, Choonara I, Bonati M, Jacqz-Aigrain E. European survey on the use of prophylactic fluconazole in neonatal intensive care units. Eur J Pediatr. 2012;171: 439–445. 10.1007/s00431-011-1565-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Pandolfini C, Kaguelidou F, Sequi M, Jacqz-Aigrain E, Choonara I, Turner MA, et al. Wide intra- and inter-country variability in drug use and dosage in very-low-birth-weight newborns with severe infections. Eur J Clin Pharmacol. 2013;69: 1031–1036. 10.1007/s00228-012-1415-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ward RM, Sherwin CMT. Ethics of drug studies in the newborn. Paediatr Drugs. 2015;17: 37–42. 10.1007/s40272-014-0099-8 [DOI] [PubMed] [Google Scholar]
- 12.Davis JM, Connor EM, Wood AJJ. The need for rigorous evidence on medication use in preterm infants: is it time for a neonatal rule? JAMA. 2012;308: 1435–1436. 10.1001/jama.2012.12883 [DOI] [PubMed] [Google Scholar]
- 13.Jacqz-Aigrain E. Editorial commentary: effectiveness or efficacy: which study to evaluate antibiotics in neonates? Clin Infect Dis Off Publ Infect Dis Soc Am. 2012;55: 1503–1504. [DOI] [PubMed] [Google Scholar]
- 14.Kairalla JA, Coffey CS, Thomann MA, Muller KE. Adaptive trial designs: a review of barriers and opportunities. Trials. 2012;13: 145 10.1186/1745-6215-13-145 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bhatt DL, Mehta C. Adaptive Designs for Clinical Trials. N Engl J Med. 2016;375: 65–74. 10.1056/NEJMra1510061 [DOI] [PubMed] [Google Scholar]
- 16.Jaillon P. [Controlled randomized clinical trials]. Bull Acad Natl Med. 2007;191: 739-756-758. [PubMed] [Google Scholar]
- 17.Meldrum ML. A brief history of the randomized controlled trial. From oranges and lemons to the gold standard. Hematol Oncol Clin North Am. 2000;14: 745–760, vii [DOI] [PubMed] [Google Scholar]
- 18.Pansieri C, Bonati M, Choonara I, Jacqz-Aigrain E. Neonatal drug trials: impact of EU and US paediatric regulations. Arch Dis Child Fetal Neonatal Ed. 2014;99: F438 10.1136/archdischild-2013-305900 [DOI] [PubMed] [Google Scholar]
- 19.Anatomical Therapeutic and Chemical (ATC) classification [Internet]. [cited 31 Jan 2017]. https://www.whocc.no/atc_ddd_index/
- 20.Watterberg KL, Gerdes JS, Cole CH, Aucott SW, Thilo EH, Mammel MC, et al. Prophylaxis of early adrenal insufficiency to prevent bronchopulmonary dysplasia: a multicenter trial. Pediatrics. 2004;114: 1649–1657. 10.1542/peds.2004-1159 [DOI] [PubMed] [Google Scholar]
- 21.Parikh NA, Kennedy KA, Lasky RE, McDavid GE, Tyson JE. Pilot randomized trial of hydrocortisone in ventilator-dependent extremely preterm infants: effects on regional brain volumes. J Pediatr. 2013;162: 685–690.e1. 10.1016/j.jpeds.2012.09.054 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hochwald O, Palegra G, Osiovich H. Adding hydrocortisone as 1st line of inotropic treatment for hypotension in very low birth weight infants. Indian J Pediatr. 2014;81: 808–810. 10.1007/s12098-013-1151-3 [DOI] [PubMed] [Google Scholar]
- 23.Baud O, Maury L, Lebail F, Ramful D, El Moussawi F, Nicaise C, et al. Effect of early low-dose hydrocortisone on survival without bronchopulmonary dysplasia in extremely preterm infants (PREMILOC): a double-blind, placebo-controlled, multicentre, randomised trial. Lancet Lond Engl. 2016;387: 1827–1836. [DOI] [PubMed] [Google Scholar]
- 24.Yeh TF, Chen CM, Wu SY, Husan Z, Li TC, Hsieh WS, et al. Intratracheal Administration of Budesonide/Surfactant to Prevent Bronchopulmonary Dysplasia. Am J Respir Crit Care Med. 2016;193: 86–95. 10.1164/rccm.201505-0861OC [DOI] [PubMed] [Google Scholar]
- 25.Bassler D, Plavka R, Shinwell ES, Hallman M, Jarreau P-H, Carnielli V, et al. Early Inhaled Budesonide for the Prevention of Bronchopulmonary Dysplasia. N Engl J Med. 2015;373: 1497–1506. 10.1056/NEJMoa1501917 [DOI] [PubMed] [Google Scholar]
- 26.Papile LA, Tyson JE, Stoll BJ, Wright LL, Donovan EF, Bauer CR, et al. A multicenter trial of two dexamethasone regimens in ventilator-dependent premature infants. N Engl J Med. 1998;338: 1112–1118. 10.1056/NEJM199804163381604 [DOI] [PubMed] [Google Scholar]
- 27.Cole CH, Colton T, Shah BL, Abbasi S, MacKinnon BL, Demissie S, et al. Early inhaled glucocorticoid therapy to prevent bronchopulmonary dysplasia. N Engl J Med. 1999;340: 1005–1010. 10.1056/NEJM199904013401304 [DOI] [PubMed] [Google Scholar]
- 28.Neonatal Inhaled Nitric Oxide Study Group. Inhaled nitric oxide in full-term and nearly full-term infants with hypoxic respiratory failure. N Engl J Med. 1997;336: 597–604. 10.1056/NEJM199702273360901 [DOI] [PubMed] [Google Scholar]
- 29.Ballard RA, Truog WE, Cnaan A, Martin RJ, Ballard PL, Merrill JD, et al. Inhaled nitric oxide in preterm infants undergoing mechanical ventilation. N Engl J Med. 2006;355: 343–353. 10.1056/NEJMoa061088 [DOI] [PubMed] [Google Scholar]
- 30.Van Meurs KP, Wright LL, Ehrenkranz RA, Lemons JA, Ball MB, Poole WK, et al. Inhaled nitric oxide for premature infants with severe respiratory failure. N Engl J Med. 2005;353: 13–22. 10.1056/NEJMoa043927 [DOI] [PubMed] [Google Scholar]
- 31.Ambalavanan N, El-Ferzli GT, Roane C, Johnson R, Carlo WA. Nitric oxide administration using an oxygen hood: a pilot trial. PloS One. 2009;4: e4312 10.1371/journal.pone.0004312 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Mercier J-C, Hummler H, Durrmeyer X, Sanchez-Luna M, Carnielli V, Field D, et al. Inhaled nitric oxide for prevention of bronchopulmonary dysplasia in premature babies (EUNO): a randomised controlled trial. Lancet Lond Engl. 2010;376: 346–354. [DOI] [PubMed] [Google Scholar]
- 33.Kinsella JP, Cutter GR, Steinhorn RH, Nelin LD, Walsh WF, Finer NN, et al. Noninvasive inhaled nitric oxide does not prevent bronchopulmonary dysplasia in premature newborns. J Pediatr. 2014;165: 1104–1108.e1. 10.1016/j.jpeds.2014.06.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Finniss DG, Kaptchuk TJ, Miller F, Benedetti F. Biological, clinical, and ethical advances of placebo effects. Lancet Lond Engl. 2010;375: 686–695. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Benedetti F. The placebo response: science versus ethics and the vulnerability of the patient. World Psychiatry Off J World Psychiatr Assoc WPA. 2012;11: 70–72. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Benedetti F. Drugs and placebos: what’s the difference?: Understanding the molecular basis of the placebo effect could help clinicians to better use it in clinical practice. EMBO Rep. 2014;15: 329–332. 10.1002/embr.201338399 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Kaptchuk TJ, Miller FG. Placebo Effects in Medicine. N Engl J Med. 2015;373: 8–9. 10.1056/NEJMp1504023 [DOI] [PubMed] [Google Scholar]
- 38.CIOMS publications [Internet]. [cited 31 Jan 2017]. http://www.cioms.ch/
- 39.Benedetti F, Carlino E, Pollo A. Hidden administration of drugs. Clin Pharmacol Ther. 2011;90: 651–661. 10.1038/clpt.2011.206 [DOI] [PubMed] [Google Scholar]
- 40.Carlino E, Pollo A, Benedetti F. The placebo in practice: how to use it in clinical routine. Curr Opin Support Palliat Care. 2012;6: 220–225. 10.1097/SPC.0b013e32835269c1 [DOI] [PubMed] [Google Scholar]
- 41.Garattini S, Bertelé V, Banzi R. Placebo? no thanks, it might be bad for me! Eur J Clin Pharmacol. 2013;69: 711–714. 10.1007/s00228-012-1383-6 [DOI] [PubMed] [Google Scholar]
- 42.Miller FG, Colloca L. The legitimacy of placebo treatments in clinical practice: evidence and ethics. Am J Bioeth AJOB. 2009;9: 39–47. [DOI] [PubMed] [Google Scholar]
- 43.Rothman KJ, Michels KB. The continuing unethical use of placebo controls. N Engl J Med. 1994;331: 394–398. 10.1056/NEJM199408113310611 [DOI] [PubMed] [Google Scholar]
- 44.Michels KB, Rothman KJ. Update on unethical use of placebos in randomised trials. Bioethics. 2003;17: 188–204. [DOI] [PubMed] [Google Scholar]
- 45.Ackerman TF. Therapeutic beneficence and placebo controls. Am J Bioeth AJOB. 2002;2: 21–22. [DOI] [PubMed] [Google Scholar]
- 46.Baer GR, Nelson RM, Ethics Group of the Newborn Drug Development Initiative. Ethical challenges in neonatal research: Summary report of the ethics group of the newborn drug development initiative. Clin Ther. 2006;28: 1399–1407. 10.1016/j.clinthera.2006.09.008 [DOI] [PubMed] [Google Scholar]
- 47.Allmark P, Mason S, Gill AB, Megone C. Is it in a neonate’s best interest to enter a randomised controlled trial? J Med Ethics. 2001;27: 110–113. 10.1136/jme.27.2.110 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Guimaraes H, Sanchez-Luna M, Bellieni CV, Buonocore G, Union of European Neonatal and Perinatal Societies. Ethical charter of Union of European Neonatal and Perinatal Societies. J Matern-Fetal Neonatal Med Off J Eur Assoc Perinat Med Fed Asia Ocean Perinat Soc Int Soc Perinat Obstet. 2011;24: 855–858. [DOI] [PubMed] [Google Scholar]
- 49.Wang J, Avant D, Green D, Seo S, Fisher J, Mulberg AE, et al. A Survey of Neonatal Pharmacokinetic and Pharmacodynamic Studies in Pediatric Drug Development. Clin Pharmacol Ther. 2015;98: 328–335. 10.1002/cpt.149 [DOI] [PubMed] [Google Scholar]
- 50.Chalumeau M, Tréluyer JM, Salanave B, Assathiany R, Chéron G, Crocheton N, et al. Off label and unlicensed drug use among French office based paediatricians. Arch Dis Child. 2000;83: 502–505. 10.1136/adc.83.6.502 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Winner P, Rothner AD, Saper J, Nett R, Asgharnejad M, Laurenza A, et al. A randomized, double-blind, placebo-controlled study of sumatriptan nasal spray in the treatment of acute migraine in adolescents. Pediatrics. 2000;106: 989–997. [DOI] [PubMed] [Google Scholar]
- 52.Braga LHP, Bagli DJ, Lorenzo AJ. Placebo-controlled trials in pediatric urology: a cautionary view from an ethical perspective. J Pediatr Urol. 2010;6: 435–442. 10.1016/j.jpurol.2010.02.208 [DOI] [PubMed] [Google Scholar]
- 53.Rheims S, Cucherat M, Arzimanoglou A, Ryvlin P. Greater response to placebo in children than in adults: a systematic review and meta-analysis in drug-resistant partial epilepsy. PLoS Med. 2008;5: e166 10.1371/journal.pmed.0050166 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Cohen D, Deniau E, Maturana A, Tanguy M-L, Bodeau N, Labelle R, et al. Are child and adolescent responses to placebo higher in major depression than in anxiety disorders? A systematic review of placebo-controlled trials. PloS One. 2008;3: e2632 10.1371/journal.pone.0002632 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Barbier P, Lionnet C, Jonville AP, Hamon B, Autret E, Laugier J, et al. [Does the placebo effect exist in newborn infants?]. Therapie. 1994;49: 113–116. [PubMed] [Google Scholar]
- 56.Bachiocco V, Mondardini MC. Julia’s placebo effect. Pain. 2010;150: 582–585. 10.1016/j.pain.2010.05.023 [DOI] [PubMed] [Google Scholar]
- 57.Bevilacqua G, Corradi M, Donzelli GP, Fanos V, Gianotti D, Magnani C, et al. The Parma charter of the rights of the newborn. J Matern-Fetal Neonatal Med Off J Eur Assoc Perinat Med Fed Asia Ocean Perinat Soc Int Soc Perinat Obstet. 2011;24: 171. [DOI] [PubMed] [Google Scholar]
- 58.Cyna AM, Costi D, Middleton P. Viewpoint: Randomised controlled trials using invasive “placebo” controls are unethical and should be excluded from Cochrane Reviews. Cochrane Database Syst Rev. 2011; ED000029 10.1002/14651858.ED000029 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Bellieni CV, Buonocore G. Recommendations for an ethical treatment of newborns involved in clinical trials. Acta Paediatr Oslo Nor 1992. 2010;99: 30–32. [DOI] [PubMed] [Google Scholar]
- 60.Jefferies AL. Postnatal corticosteroids to treat or prevent chronic lung disease in preterm infants. Paediatr Child Health. 2012;17: 573 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Watterberg KL, American Academy of Pediatrics. Committee on Fetus and Newborn. Policy statement—postnatal corticosteroids to prevent or treat bronchopulmonary dysplasia. Pediatrics. 2010;126: 800–808. 10.1542/peds.2010-1534 [DOI] [PubMed] [Google Scholar]
- 62.Doyle LW, Ehrenkranz RA, Halliday HL. Early (< 8 days) postnatal corticosteroids for preventing chronic lung disease in preterm infants. Cochrane Database Syst Rev. 2014; CD001146 10.1002/14651858.CD001146.pub4 [DOI] [PubMed] [Google Scholar]
- 63.Doyle LW, Ehrenkranz RA, Halliday HL. Late (> 7 days) postnatal corticosteroids for chronic lung disease in preterm infants. Cochrane Database Syst Rev. 2014; CD001145 10.1002/14651858.CD001145.pub3 [DOI] [PubMed] [Google Scholar]
- 64.Peltoniemi OM, Lano A, Yliherva A, Kari MA, Hallman M, Neonatal Hydrocortisone Working Group. Randomised trial of early neonatal hydrocortisone demonstrates potential undesired effects on neurodevelopment at preschool age. Acta Paediatr Oslo Nor 1992. 2016;105: 159–164. [DOI] [PubMed] [Google Scholar]
- 65.Barrington KJ, Finer N. Cochrane review: Inhaled nitric oxide for respiratory failure in preterm infants. Evid-Based Child Health Cochrane Rev J. 2010;5: 301–336. [DOI] [PubMed] [Google Scholar]
- 66.Soll RF. Inhaled nitric oxide for respiratory failure in preterm infants. Neonatology. 2012;102: 251–253. 10.1159/000338552 [DOI] [PubMed] [Google Scholar]
- 67.Askie LM, Ballard RA, Cutter GR, Dani C, Elbourne D, Field D, et al. Inhaled nitric oxide in preterm infants: an individual-patient data meta-analysis of randomized trials. Pediatrics. 2011;128: 729–739. 10.1542/peds.2010-2725 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Peliowski A. Inhaled nitric oxide use in newborns. Paediatr Child Health. 2012;17: 95–97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Kumar P, Committee on Fetus and Newborn, American Academy of Pediatrics. Use of inhaled nitric oxide in preterm infants. Pediatrics. 2014;133: 164–170. 10.1542/peds.2013-3444 [DOI] [PubMed] [Google Scholar]
- 70.Allen MC, Donohue P, Gilmore M, Cristofalo E, Wilson RF, Weiner JZ, et al. Inhaled nitric oxide in preterm infants. Evid ReportTechnology Assess. 2010; 1–315. [PMC free article] [PubMed] [Google Scholar]
- 71.Cole FS, Alleyne C, Barks JDE, Boyle RJ, Carroll JL, Dokken D, et al. NIH Consensus Development Conference statement: inhaled nitric-oxide therapy for premature infants. Pediatrics. 2011;127: 363–369. 10.1542/peds.2010-3507 [DOI] [PubMed] [Google Scholar]
- 72.Pasquali SK, Lam WK, Chiswell K, Kemper AR, Li JS. Status of the pediatric clinical trials enterprise: an analysis of the US ClinicalTrials.gov registry. Pediatrics. 2012;130: e1269–1277. 10.1542/peds.2011-3565 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Pandolfini C, Bonati M, Rossi V, Santoro E, Choonara I, Naylor C, et al. The DEC-net European register of paediatric drug therapy trials: contents and context. Eur J Clin Pharmacol. 2008;64: 611–617. 10.1007/s00228-007-0458-2 [DOI] [PubMed] [Google Scholar]
- 74.Pandolfini C, Bonati M, Sammons HM. Registration of trials in children: update of current international initiatives. Arch Dis Child. 2009;94: 717–719. 10.1136/adc.2008.148155 [DOI] [PubMed] [Google Scholar]
- 75.International Clinical Trials WHO Registry Platform (ICTRP). In: WHO [Internet]. [cited 31 Jan 2017]. http://www.who.int/ictrp/en/
- 76.European Clinical Trials Register [Internet]. [cited 31 Jan 2017]. https://www.clinicaltrialsregister.eu/
- 77.Boots I, Sukhai RN, Klein RH, Holl RA, Wit JM, Cohen AF, et al. Stimulation programs for pediatric drug research—do children really benefit? Eur J Pediatr. 2007;166: 849–855. 10.1007/s00431-006-0381-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Li JS, Eisenstein EL, Grabowski HG, Reid ED, Mangum B, Schulman KA, et al. Economic return of clinical trials performed under the pediatric exclusivity program. JAMA. 2007;297: 480–488. 10.1001/jama.297.5.480 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Food and Drug Administration Modernization Act (FDAMA) of 1997 [Internet]. [cited 31 Jan 2017]. http://www.fda.gov/RegulatoryInformation/Legislation/SignificantAmendmentstotheFDCAct/FDAMA/FullTextofFDAMAlaw/default.htm
- 80.Development Resources—Best Pharmaceuticals for Children Act, January 4, 2002 (Public Law No. 107–109) [Internet]. [cited 31 Jan 2017]. http://www.fda.gov/Drugs/DevelopmentApprovalProcess/DevelopmentResources/ucm049876.htm
- 81.Pediatrics Research Equity Act of 2003 [Internet]. http://www.fda.gov/downloads/Drugs/DevelopmentApprovalProcess/DevelopmentResources/UCM077853.pdf
- 82.European Pediatric Regulation of 2007 [Internet]. http://www.ema.europa.eu/docs/en_GB/document_library/Other/2009/09/WC500003693.pdf
- 83.Choonara I. Regulation of drugs for children in Europe. BMJ. 2007;335: 1221–1222. 10.1136/bmj.39400.376424.BE [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Turner MA, Catapano M, Hirschfeld S, Giaquinto C, Global Research in Paediatrics. Paediatric drug development: the impact of evolving regulations. Adv Drug Deliv Rev. 2014;73: 2–13. 10.1016/j.addr.2014.02.003 [DOI] [PubMed] [Google Scholar]
- 85.Korppi M, Lepola P, Vettenranta K, Pakkala S, Hoppu K. Limited impact of EU paediatric regulation on Finnish clinical trials highlights need for Nordic collaboration. Acta Paediatr Oslo Nor 1992. 2013;102: 1035–1040. [DOI] [PubMed] [Google Scholar]
- 86.US National Institutes of Health Clinical trials database [Internet]. [cited 31 Jan 2017]. https://www.clinicaltrials.gov/
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
(DOCX)
(DOCX)
(DOCX)
Data Availability Statement
All relevant data are within the paper and its Supporting Information files.