

Abstract
Combined upper alveolectomy and segmental mandibulectomy are complex defects. Reconstruction of these defects is usually suboptimal. We describe the case of a pediatric patient with vessel-depleted neck with recurrent vascular malformation involving the ramus and coronoid process of mandible and a previous history of maxillectomy and a reconstruction with anterolateral thigh flap. The patient underwent wide resection. The defects involving the upper alveolus and mandible were simultaneously reconstructed with a single free fibula flap.
Keywords: combined maxilla and mandible defect, maxillary reconstruction, mandibular reconstruction, pediatric patient, fibula flap
Vascularized bone flaps form an integral part of head and neck reconstruction. Nevertheless, the best results in complex head and neck defects are far from optimal. A combined defect involving the maxilla and mandible may ideally require two bone flaps for reconstruction. The purpose of this article is to report a case of single-stage bony reconstruction of a combined maxilla and mandible defect after a benign tumor excision in a 7-year-old girl, using a free fibula flap. This case is unique in many aspects such as the age of the patient, the defect created by an arteriovenous malformation, and the case being a failure of a previous bony reconstruction with a vessel-depleted neck.
Case Report
A 7-year-old girl, a case of arteriovenous malformation of left maxilla region, with a history of prior left total maxillectomy, presented with a recurrent lesion involving the ramus of the mandible. The reconstruction was first attempted with a free fibula flap, which failed, and then with an anterolateral thigh (ALT) flap which was successful. The orbital floor reconstruction was done with a titanium mesh. The computed tomographic (CT) scan at presentation showed residual arteriovenous malformation involving ramus and coronoid process of left mandible with cortical destruction (Figs. 1 and 2). There was no evidence of recurrence at previous operated site. A carotid angiogram showed feeders from left external carotid artery with draining veins to both internal jugular veins.
Fig. 1.

Preoperative frontal view photograph of the patient, prior to the latest surgery.
Fig. 2.
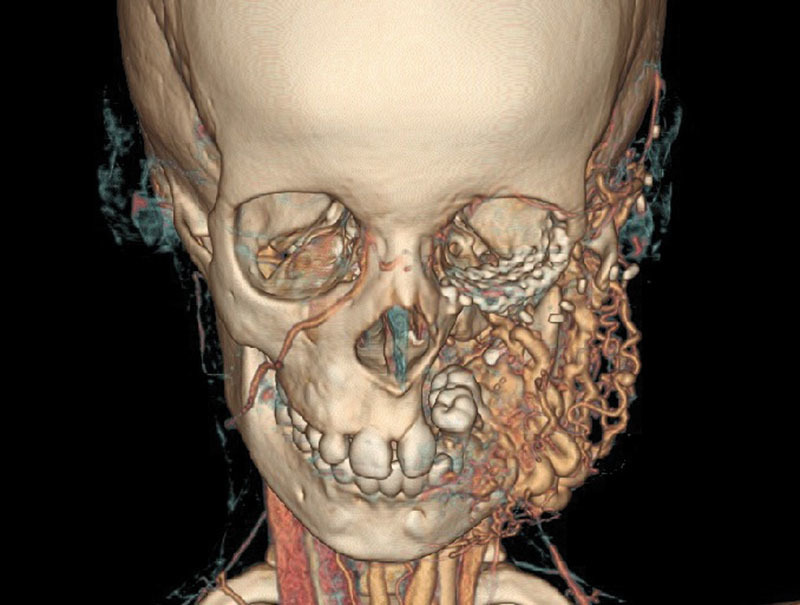
Three dimensional CT scan with angiogram showing the lesion involving the ramus and coronoid region of left hemi-mandible with feeders from left external carotid artery.
She underwent wide excision of the lesion with segmental mandibulectomy through a midline lip split with chin sparing incision and cheek flap approach. Bone resection involved segmental mandibulectomy from first premolar tooth on the left side to the ascending ramus and coronoid, preserving the condyle. The upper alveolus defect of the previous surgery was also considered. This was previously reconstructed with a soft-tissue flap only (Fig. 3). A 2-mm titanium plate was pre bent using three-dimensional, CT-based contouring. This technique has been previously reported by other authors.1 After excision, plating was done with three screws on either side. Free fibula flap was harvested from the right leg with a skin paddle size of 6 × 4 cm. The length of the bone required for mandibular reconstruction was measured and marked. The vascular pedicle of the free fibula flap was dissected and separated in a supraperiosteal plane until the part of bone needed for mandibular reconstruction. Proximal to this, a 2-cm segment of the bone was excised preserving the periosteum circumferentially. Further, a 3-cm-long segment was preserved proximally. This segment was used for maxillary alveolar segment reconstruction. This dissection allowed the proximal bone segment to be solely supplied by the periosteal blood supply. The removal of a 2-cm segment of bone allowed the proximal segment of the bone to be turned upward for maxillary alveolar segment reconstruction (Fig. 4). The proximal segment of fibula was tunneled above the previous ALT flap and secured with miniplates to the upper alveolus remnant (Fig. 5). The distal segment of the fibula was contoured for the mandible according to the pre-bent plate. Anastomosis of peroneal artery was done end to side to external carotid artery and peroneal vein to common facial vein in an end-to-end fashion. The child is doing well, 2 years after the procedure (Figs. 6 and 7), with a satisfactory oral function, taking normal oral diet and has an adequate mouth opening of 3 cm. There was no clinical evidence of any recurrence of the lesion or avascularity of the proximal fibular segment replacing the maxilla. The child has no donor site morbidity except for the skin-grafted area. There is no morbidity related to ambulation or leg growth.
Fig. 3.

Postresection photograph showing segmental mandibulectomy defect, with preservation of a part of vertical ramus and condyle to which the plate has been attached. Note the upper alveolus defect, which has been reconstructed only with a soft-tissue flap.
Fig. 4.

Fibula flap with the design for reconstruction. The intervening bone segment has been removed keeping the periosteum in continuity.
Fig. 5.
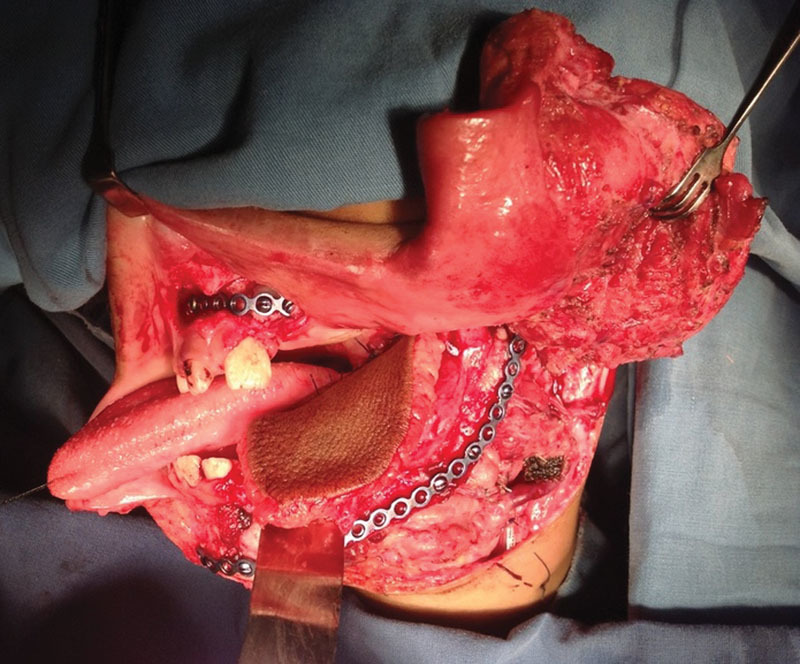
Flap inset has been done to reconstruct the defect. The upper segment of the fibula has been fixed to the upper alveolus stump and the lower segments used to reconstruct the mandible.
Fig. 6.
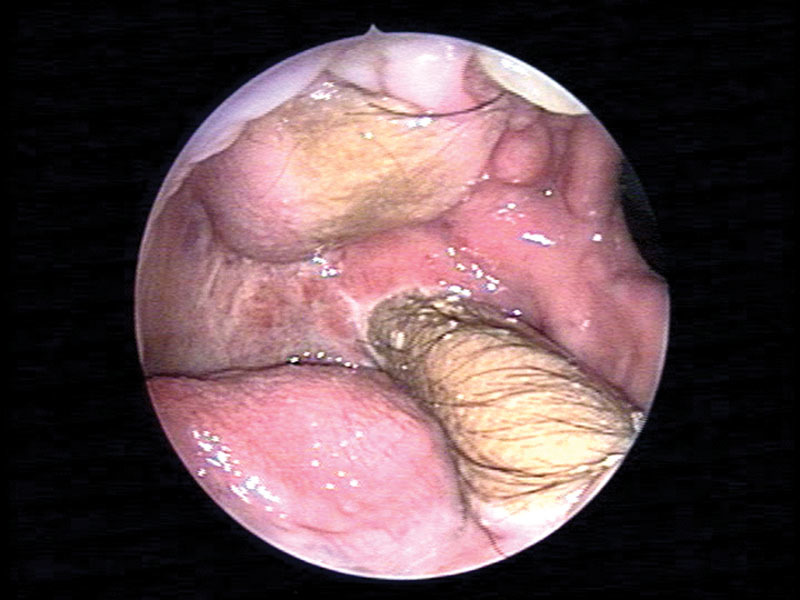
Endoscopic view of oral cavity showing the status 6 months postoperatively.
Fig. 7.

Frontal view of the patient 24 months after surgery.
Discussion
A combined segmental mandibulectomy with maxillectomy defect involves extensive bone loss, leading to significant functional and cosmetic issues. Previous history of two flaps, one failed free fibula and the existing ALT flap in the defect, made the issue complicated. The patient being a child added further to the difficulty. The optimal reconstruction of this defect would demand replacement of lost bone with adequate vascularized bone and soft tissue. The provision of the bone would require a free bone graft or a vascularized bone. The use of double-bone flap will be complicated and risky due to problems with the pedicle length, tunneling of two sets of pedicle vessels, and availability of two pairs of donor vessels on the same side. The method described here is a simple, but useful, modification of the fibula flap design. The remaining contralateral fibula, which was being used for the mandibular reconstruction, was technically modified to provide bone, also for the alveolar segment. The possibility of keeping the pedicle attached to the proximal segment of the bone was considered, but it would have jeopardized the length of the pedicle to reach the neck.
Impressive attempts at simultaneous reconstruction of defects involving both maxilla and mandible using free bone flap have been reported in literature before, though very few in number.2 3 4 These have been mostly used in malignancy2 and accidental injuries.3 5 In one of these articles, the authors describe reconstructing mandible and maxilla defects with the same fibula flap, removing a segment of bone but retaining the periosteal continuity.3 The design of flap here is also similar, except that our case had a history of prior surgery with an existing ALT flap. The upper segment could be tunneled through a pocket made above the previously existing flap. One of the reported cases involved a large bone and soft-tissue defect which was reconstructed with fibula osteocutaneous flap for maxillary and mandibular defects and an anterolateral fasciocutaneous flap for intraoral mucosal, external skin, and soft tissue loss. In another article, the authors describe the use of a differentially split osteomyocutaneous peroneal artery-based combined flap for single-stage reconstruction of left maxillary and right mandibular defects.6
The present case is unique in that this is a pediatric patient who had already undergone a major reconstruction, which used vessels on the same side. As the lesion was benign, a procedure that gave the child an acceptable function and cosmesis with the least possible morbidity was done. Considering the pediatric mandibulo-maxillary reconstruction, growth of the replaced bone is an issue. In case of the mandible, since the condyle is preserved in the present case, a major problem with the disparity of growth may not occur.7 For maxilla, it is difficult to ascertain the damage to the growth center in this particular case of diffuse vascular malformation involving the entire maxilla. Nevertheless, the provision of the bone could help in the dental rehabilitation and maintenance of a harmonious relationship of maxillomandibular dentition in the future and allow the maxilla to grow along with the mandible. The patient will require an orthodontic correction, implant placement with dental rehabilitation, orthognathic procedure, and a corrective procedure for the position of the left lower eyelid in the future.
The use of the contralateral fibula for this case made the reconstruction more difficult and the necessity to create a proximal segment of fibular bone for the maxillary defect based solely on “periosteal blood supply,” made it more challenging. There is a possibility that the blood supply to that segment, giving the length of the random blood supply by the periosteum as 5 cm in total (2 cm removed bone and 3 cm bone at the end), got its blood supply from the surrounding soft tissue. Although there is a long-term follow-up of patient, it is essential to see the status of the reconstructed mandible and maxilla and the fate of the fibula. A long-term imaging, especially to see the vascularity of the fibula, would have been ideal, but considering that the patient was doing well clinically with no evidence of any infection or extrusion, and that the patient had undergone multiple radiological investigations in the past, the parents were not willing to consent for a new one.
To the best of our knowledge, this is the first case of reconstruction of a combined segmental mandibulectomy and maxillectomy defect with the same bone flap in a child who has undergone a previous major resection with free flap in the same area.
References
- 1.Thankappan K, Trivedi N P, Subash P. et al. Three-dimensional computed tomography-based contouring of a free fibula bone graft for mandibular reconstruction. J Oral Maxillofac Surg. 2008;66(10):2185–2192. doi: 10.1016/j.joms.2008.01.035. [DOI] [PubMed] [Google Scholar]
- 2.Punpale A S, Rajendra Prasad J S, Shetty K P, Kadam S, Udupa V. An innovative design for simultaneous reconstruction of complex maxillo-mandibular defects with single free fibula osteocutaneous flap. J Plast Reconstr Aesthet Surg. 2006;59(1):96–101. doi: 10.1016/j.bjps.2005.07.006. [DOI] [PubMed] [Google Scholar]
- 3.Laure B, Sury F, Martin T, Chabut A, Goga D. Reconstruction of bony mandibular and maxillary defects with one single transfer of a free fibula osteocutaneous flap. J Plast Reconstr Aesthet Surg. 2008;61(2):200–203. doi: 10.1016/j.bjps.2007.06.007. [DOI] [PubMed] [Google Scholar]
- 4.Sadove R C, Powell L A. Simultaneous maxillary and mandibular reconstruction with one free osteocutaneous flap. Plast Reconstr Surg. 1993;92(1):141–146. doi: 10.1097/00006534-199307000-00022. [DOI] [PubMed] [Google Scholar]
- 5.Ozkan O, Ozgentas H E, Dikici M B. Simultaneous reconstruction of large maxillary and mandibular defects with a fibular osteocutaneous flap combined with an anterolateral thigh flap. J Reconstr Microsurg. 2004;20(6):451–455. doi: 10.1055/s-2004-833502. [DOI] [PubMed] [Google Scholar]
- 6.Nguyen D H, Wu C W, Huang J J, Chang C S, Cheng M H. Simultaneous left maxillary and right mandibular reconstructions with a split osteomyocutaneous peroneal artery-based combined flap. Head Neck. 2013;35(2):E39–E43. doi: 10.1002/hed.21864. [DOI] [PubMed] [Google Scholar]
- 7.Fowler N M, Futran N D. Utilization of free tissue transfer for pediatric oromandibular reconstruction. Facial Plast Surg Clin North Am. 2014;22(4):549–557. doi: 10.1016/j.fsc.2014.07.001. [DOI] [PubMed] [Google Scholar]