

Abstract
Background: Screen time (ST), including watching television and playing electronic games are the leading cause of a growing obesity epidemic. This study aimed to evaluate ST and its association with physical activity, overweight and socioeconomic status (SES) in children 10 to 12 years of age in Sanandaj.
Methods: This study was designed as a cross-sectional study, which was conducted in Sanandaj in 2015. ST and physical activity data were collected using the Modifiable Activity Questionnaire (MAQ). Overweight indices are defined based on BMI age- and gender-specific percentiles, as proposed by WHO criteria. Considering household assets data, SES was calculated using principal component analysis (PCA). The relationship between ST and different determinants was assessed using logistic regression analysis.
Results: Based on the results obtained in our study, 47.28% (95% CI: 45.33-49.24) of the participants spent more than two hours a day on television and video watching and electronic games playing. People who spend greater time on ST activities, independent of their physical activities, are more susceptible to overweight and obesity (p=0.002). People in higher socioeconomic groups spent more time on watching TV and video and playing electronic games (p=0.001). There was a direct relationship between the residential area and ST (P=0.052). ST in male was found to be greater (p=0.033). In addition, ST was also lower in school-aged children whose mothers had a greater education (p=0.56).
Conclusion: Based on the results of this study, it is recommended to increase the education level and knowledge of mothers and design interventions consistent with children gender and residential location so that to reduce ST and its associated outcomes in children.
Keywords: Screen time behavior, Socio-economic inequality, Inactivity, Physical activity, Children
Introduction
Physical inactivity as a risk factor for mortality leads to 3.2 million deaths annually in the world and 32.1 million disability-adjusted life year (DALY) (1). Increasing physical activity is one of the public health priorities (2). Inactivity, independent of the physical activity, has attracted much attention as a potential risk factor for adverse health consequences (3). Inactivity is associated with mortality, independent of moderate and vigorous physical activities (4). Research has shown that inactivity and physical activity are not contradictory. These are two separated behavioral structures, which have independent impacts on health outcomes, in a way that the consequences of Inactivity negatively affect the benefits obtained from the physical activity (5). Moreover, the Inactivity impact on health lasts even after controlling moderate and vigorous physical activities (6). Inactivity directly plays a role in many health outcomes such as obesity, metabolic syndrome and cardiovascular diseases (7). It is also known as a lifetime reducing factor (8). Inactivity is one of the main causes of morbidity and mortality in developed countries, costs which are mostly paid by disadvantaged people (9). Studies show that children in areas with low SES are less likely to perform physical activities and are willing to participate in inactivity activities. Children with low SES have lower physical activity than children with high SES (1).
Recent strategies in public health have emphasized the importance of reducing inactivity among adolescent and youth (3). Activities such as screen time (ST), including watching television and playing electronic games, are considered as alternative indicators of Inactivity (9,10). Some studies have shown that ST is one of the most effective types of inactivity behaviors on the individual's health compared to other behaviors (11). Based on the recommendations of World Health Organization (WHO), inactivity behaviors, including TV and video watching and electronic games playing should not be more than 2 hours a day (12). However, children spend the bulk of their waking hours (50-80%) on inactivity behaviors (13). Less than 40% of children and youth meet the recommendation in western countries. ENERGY projects in seven European countries among children aged 10-12 years showed that a total of 83.2% and 95.4% of European male and female school-aged children respectively do not have enough activities (14).
Based on our knowledge, the previous studies have been conducted to investigate the relationship between some aspects of SES in inactivity among children. In this study, while measuring ST, we aimed to investigate its relationship with physical activity, overweight and multiple dimensions of SES among children aged between 10 to 12 years in Sanandaj using PCA method.
Methods
Data and Instruments
This study was a cross-sectional study which was conducted in 2015 in Sanandaj, the capital city of Kurdistan province, located in the Western part of Iran. The study samples included 2506 male and female students studying in the fifth and sixth grades of primary school (aged 10-12 years old); the subjects were chosen from schools located in Sanandaj city. The sampling framework included two regions of Sanandaj Education and Training Office; the first region included 84 schools and the second region included 42 schools. To select the samples, multistage sampling method was used. Accordingly, the two regions were selected as the two main strata, and the schools in each stratum were selected as clusters. The sample size allocated to each stratum was in proportion to the size of that stratum; accordingly, 1600 people from the first region and 900 people from the second region were enrolled into the study. In view of that, 39 schools (clusters) from the first region and 24 schools from the second region were selected. Moreover, within each school, again the educational grades were selected as the main strata and the classes at each grade were considered as clusters of that stratum. The number of classes in each cluster and the number of students in each cluster were selected in proportion to their sizes. Finally, of the samples allocated to each stratum, the required number of the subjects was selected via random convenience sampling method.
A total of six interviewers conducted the survey; they were divided into two groups, with three members in each group. In addition, two supervisors were assigned to monitor the interviews and examination in each group. The interviewers and supervisors were trained prior to the initiation of the study. To collect the required data. First, the students were examined at school and were interviewed to complete a questionnaire. Then, parents with the cooperation of the students completed the questionnaires at home or via phone calls. To enroll the students in the study and to examine them, informed consent was obtained from all the participants and their parents.
Screen Time data were collected by trained interviewers using the international Modifiable Activity Questionnaire for Adolescents (MAQ), and children who did not meet the standard recommendation (less than two hours a day) were considered as ‘inactive.' Based on the previous studies, the reliability and validity of the questionnaire were 0.97% and 0.47%, respectively (p=0.01) (15). To assess the physical activity, information on the frequency and duration of physical activity were collected from the participants using the MAQ questionnaire. There is certainly a metabolic equivalent (MET) for each physical activity. One MET is the equivalent amount of energy used per minute by the individual at resting state. The level of physical activity, as hours of activity per week and MET-h / WK was calculated using the formula, based on which participants' efforts were divided into three groups of low activity (MET<3), moderate activity (MET between 3 to 6), and heavy activity (MET>6). People with physical activity less than 3 MET were considered as participants with insufficient activity and those with moderate and vigorous physical activities were considered as participants with sufficient levels of activity (16,17).
To measure the participants’ heights, they were set in a standing position, without shoes, with their feet flat together, with their shoulders level, and with their backs against a wall with a measuring tape on it. The heights were measured by touching the ruler on the top of the head. The participants’ weights were measured using a digital scale, with minimum clothing, with a precision of 100 grams. We also calculated the individual body mass index or BMI (weight in kilograms divided by the square of the height in meters). Following the recommendations by the WHO, to define overweight and obesity we used age- and gender-specific BMI criteria which are used globally as a standard measure of obesity for children and adolescents aged 2-19 years old. Accordingly, overweight is defined as a percentile over 85 and obesity is defined as a percentile over 95 (18,19).
To determine the socioeconomic situation, a method by O'Donnell et al. (2006) was used. Accordingly, a questionnaire including a number of household assets namely, separate bathroom, separate kitchen, vacuum cleaners, computers, separate refrigerators, washing machine, color TV, LCD TV, mobile phone, dishwasher, microwave oven, internet access, personal car, landline telephone, personal home, number of rooms, heating appliances, oven, microwave and furniture was used. Asset index was calculated for every person on the basis of each asset, using principal component analysis (PCA). According to the index, the population was divided into five quintiles of very poor, poor, moderate, rich, and very rich (20-22).
Statistical analysis
Logistic regression was used for analysis of data and evaluation of the relationship between ST and independent variables including physical activity, overweight, household's SES, child's age and gender, parents' education level and residential area. Crude and adjusted odds ratios were calculated for each of the variables in the model. Use of cellphones and tablets were separately evaluated in the studied variables and crude and adjusted odds ratios were calculated using logistic regression. The significance level of 0.05 was considered in all models. Data analysis was conducted using Stata13 and SPSS 20.
Results
The prevalence of ST in each quintile (very poor, poor, moderate, rich, and very rich) was respectively 40.53%, 46.88%, 55.61%, 56.50% and 54.80%. Of all, 47.28% (95%CI: 45.33-49.24) spent more than 2 hours a day to watch television and videos and play electronic games. 24.1% (95%CI: 22.42-25.77) and 11.57% (95%CI: 10-12) of the participants were overweight and obese, respectively. 59.09% (95%CI: 57.17-61.02) of the participants had sufficient activity, and 40.90% (95%CI: 38.97-
42.82) had insufficient levels of activity. The median ST time was 2 hours per day for female and male children (Interquartile Range (IQR)=2-3). The median time spent on moderate and vigorous physical activities throughout the year was equal to 3 hours per week (IQR=1-3) for male and 2 (IQR=1-3) hours per week for female children. Accordingly, the median time spent on vigorous physical activity (MET<6) throughout the year was 3 hours per day (IQR=1-3) for male and 2 hours per week (IQR=2-4) for female children. Moreover, median hours of using tablet per day was equal to 2 (IQR=1-2). A total of 55.51 % of respondents reported that they participated in sport competitions at or outside of school at least once a year.
Table 1 shows the prevalence of the screen time activities for each of the independent variables including overweight, physical activity, age, gender, parents' educational level, parental age and economic groups. In this study, 50.08% (47.58 to 54.02) of male and 45.21% (42.75 to 47.67) of female children spent more than 2 hours a day watching TV and video and playing electronic games. This difference is statistically significant (p=0.033) (Fig. 1).
Table 1. Distribution of Screen Time according different variable .
|
Screen Time N (%) |
Using Cell phone & tablet N (%) |
|
| Sex | ||
| Male | 472(50.80) | 211(22.71) |
| Female | 713(45.21) | 267(16.93) |
| Physical Activity | ||
| Inadequate PA | 440(42.92) | 175(17.07) |
| Adequate PA | 745(50.30) | 303(20.45) |
| weight | ||
| Low/Normal | 860(45.21) | 357(18.76) |
| Obese Overweight | 325(53.80) | 121(20.03) |
| Mother Education | ||
| Illiterate | 200(42.28) | 77(16.27) |
| Elementary | 295(46.09) | 118(18.43) |
| Guidance | 191(47.16) | 76(18.76) |
| High school | 284(51.82) | 122(22.26) |
| Academic | 215(49.08) | 85(19.40) |
| Education Father | ||
| Uneducated | 93(42.66) | 27(12.38) |
| Elementary | 220(43.91) | 85(16.96) |
| Guidance | 189(45) | 94(22.38) |
| High school | 270(47.78) | 101(17.87) |
| Academic | 409(51.44) | 171(21.50) |
| SES | ||
| Poorest SES | 454(40.53) | 160(14.28) |
| Poor SES | 218(46.88) | 68(14.62) |
| Middle SES | 198(55.61) | 94(26.40) |
| Rich SES | 178(56.50) | 83(26.34) |
| Richest SES | 137(54.80) | 73(29.20) |
| Mother Age | ||
| 30< | 87(49.71) | 42(24) |
| 30-39 | 748(47.52) | 302(19.18) |
| 40< | 350(46.35) | 134(17.74) |
| Father Age | ||
| 30< | 456(47.01) | 189(19.48) |
| 30-39 | 607(47.34) | 241(18.79) |
| 40< | 116(47.54) | 46(18.85) |
| Residential Area | ||
| 1th | 132(37.18) | 43(12.11) |
| 2th | 280(46.35) | 124(20.52) |
| 3th | 430(48.69) | 172(19.47) |
| 4th | 185(49.59) | 68(18.23) |
| 5th | 158(54.29) | 71(24.39) |
| Age | ||
| 10 | 189(50.53) | 71(18.98) |
| 11 | 492(47.12) | 194(18.58) |
| 12 | 504(46.32) | 213(19.57) |
SES socioeconomic statue, residential areas are classified by socioeconomic status from the lowest to the highest
Fig. 1.
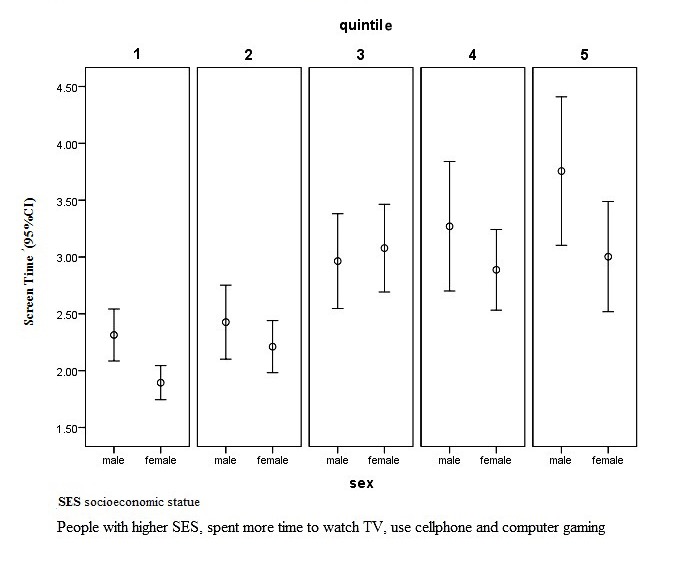
Screen time by sex in different socioeconomic status
A total of 53.80% of people, who were overweight, had inactivity behaviors. According to the results shown in Table 2, there was a direct relationship between inactivity and overweight (p=0.002). People who spent more time on ST activities, independent of physical activity, were at greater risk of obesity and overweight. Moreover, people with higher SES spent more time on watching TV, using a cellphone, and engaging in computer gaming (p =0.001). There was a direct relationship between residential area and ST in a way that those living in areas with high socioeconomic level had higher ST (p=0.052). In this study, ST was low in children with college-educated mothers (p=0.56). According to the findings in this study, those who were more physically active were more likely to spend their leisure time on ST activities. However, this relationship was not significant (p=0.12). Furthermore, there was no significant relationship between parental age, father's education, and ST.
Table 2. Screen Time according to different independent variable .
| Screen Time | Using Cell phone & tablet | |||||
| (Crude) OR | (Adjust) OR | p | (Crude) OR | (Adjust) OR | p | |
| Sex | ||||||
| Male | 1 | 1 | 1 | 1 | ||
| Female | 0.79(0.67-0.93) | 0.82(0.69-0.98) | 0.03 | 0.69(0.56-0.84) | 0.68(0.55-0.85) | 0.001 |
| Physical Activity | ||||||
| Inadequate | 1 | 1 | 1 | 1 | ||
| PA | ||||||
| Adequate PA | 1.34(1.14-1.57) | 0.87(0.73-1.03) | 0.12 | 1.24(1.01-1.53) | 1.01(0.81-1.26) | 0.90 |
| weight | ||||||
| Low/Normal | 1 | 1 | 1 | 1 | ||
| Obese | 1.41(1.17-1.69) | 1.34(1.11-1.61) | 0.002 | 1.08(0.86-1.36) | 1.00(0.79-1.27) | 0.95 |
| &Overweight Mother Education | ||||||
| Illiterate | 1 | 1 | 1 | 1 | ||
| Elementary | 1.16(0.91-1.48) | 1.13(0.87-1.46) | 0.35 | 1.16(0.84-1.59) | 0.99(0.70-1.40) | 0.98 |
| Guidance | 1.21(0.93-1.59) | 1.04(0.77-1.41) | 0.76 | 1.18(0.83-1.68) | 0.87(0.59-1.28) | 0.49 |
| High school | 1.46(1.14-1.88) | 1.20(0.88-1.62) | 0.23 | 1.47(1.07-2.02) | 1.14(0.78-1.68) | 0.47 |
| Academic | 1.31(1.01-1.70) | 0.90(0.64-1.27) | 0.56 | 1.23(0.88-1.74) | 0.75(0.48-1.16) | 0.20 |
| Education Father | ||||||
| Uneducated | 1 | 1 | 1 | 1 | ||
| Elementary | 1.05(0.76-1.52) | 0.95(0.68-1.34) | 0.79 | 1.44(0.90-2.30) | 1.42(0.86-2.32) | 0.16 |
| Guidance | 1.09(0.79-1.52) | 0.93(0.65-1.34) | 0.72 | 2.03(1.28-3.24) | 1.97(1.19-3.26) | 0.008 |
| High school | 1.23(0.89-1.68) | 0.91(0.63-1.31) | 0.61 | 1.53(0.97-2.43) | 1.21(0.71-2.04) | 0.46 |
| Academic | 1.42(1.05-1.92) | 1.00(0.69-1.46) | 0.97 | 1.93(1.25-3.00) | 1.52(0.89-2.57) | 0.11 |
| SES | ||||||
| Poorest SES | 1 | 1 | 1 | 1 | ||
| Poor SES | 1.29(1.04-1.60) | 1.21(0.96-1.72) | 0.09 | 1.02(0.75-1.39) | 1.03(0.74-1.42) | 0.84 |
| Middle SES | 1.83(1.44-2.33) | 1.67(1.29-2.17) | 0.000 | 2.15(1.61-2.87) | 2.22(1.61-3.05) | 0.000 |
| Rich SES | 1.90(1.48-2.45) | 1.74(1.32-2.31) | 0.000 | 2.14(1.58-2.90) | 2.31(1.65-3.25) | 0.000 |
| Richest SES | 1.77(1.34-2.34) | 1.66(1.22-2.26) | 0.001 | 2.47(1.79-3.40) | 2.77(0.99-2.53) | 0.000 |
| Mother Age | ||||||
| 30> | 1 | 1 | 1 | 1 | ||
| 30-39 | 0.91(0.67-1.25) | 0.85(0.61-1.18) | 0.35 | 0.75(0.51-1.08) | .68(0.46-1.01) | 0.05 |
| 40< | 0.87(0.62-1.21) | 0.79(0.54-1.16) | 0.23 | 0.68(0.46-1.01) | 0.58(0.36-0.93) | 0.02 |
| Father Age | ||||||
| 30> | 1 | 1 | 1 | 1 | ||
| 30-39 | 1.01(0.85-1.19) | 1.02(0.83-1.24) | 0.82 | 0.95(0.77-1.18) | 0.96(0.75-1.24) | 0.78 |
| 40< | 1.02(0.77-1.35) | 1.08(0.77-1.53) | 0.62 | 0.96(0.67-1.37) | 1.06(0.68-1.66) | 0.77 |
| Residential Area | ||||||
| 1th | 1 | 1 | 1 | 1 | ||
| 2th | 1.45(1.11-1.90) | 1.30(0.99-1.72) | 0.05 | 1.87(1.28-2.72) | 1.68(1.14-2.48) | 0.008 |
| 3th | 1.60(1.24-2.06) | 1.24(0.95-1.63) | 0.10 | 1.75(1.22-2.51) | 1.25(0.85-1.84) | 0.23 |
| 4th | 1.66(1.23-2.23) | 1.24(0.89-1.73) | 0.19 | 1.61(1.07-2.44) | 1.18(0.75-1.88) | 0.46 |
| 5th | 2.00(1.46-2.75) | 1.41(0.99-2.01) | 0.052 | 2.34(1.54-3.55) | 1.58(0.99-2.53) | 0.05 |
| Age | ||||||
| 10 | 1 | 1 | 1 | 1 | ||
| 11 | 0.87(0.68-1.10) | 0.87(0.68-1.11) | 0.28 | 0.97(0.72-1.31) | 0.99(0.72-1.35) | 0.97 |
| 12 | 0.84(0.66-1.06) | 0.86(0.68-1.10) | 0.25 | 1.03(0.77-1.40) | 1.05(0.77-1.43) | 0.73 |
SES socioeconomic statue, residential area are classified by socioeconomic status from the lowest to the highest
In this study, cellphones and tablets were used for more than two hours a day by a total of 19.07% (17.53-20.61) of the respondents, of which a lower portion was female children, OR=0.68 (95% CI: 0.55-0.85). Subjects in groups with higher SES used cellphones and tablets more than those in other groups. Moreover, as the maternal age increased, the use of cellphones and tablets was significantly decreased OR=0.58 (95% CI: 0.36-0.93).
Discussion
This study aimed to evaluate the screen time and its association with physical activity, overweight and socioeconomic factors in children 10-12 years old in Sanandaj. According to the results of this study, a total of 47.28% of the respondents spent more than two hours a day watching television and video and playing electronic games. Moreover, a total of 40.90% of the children had not sufficient levels of physical exercise. According to the findings, a total of 24.1% of the children were overweight and obese. As the results showed, people who spent more time on ST activities, were significantly at greater risk of obesity and overweight, even in people who had enough physical activity. Our findings are in line with the results obtained in the study by Ghavamzadeh et al. (23), in Urmia. In this study, inactivity, independent of physical activity and high-calorie foods, is reported to be a risk factor for the prevalence of obesity and overweight (p<0.001). In addition, the results are consistent with those of the studies by Dutra et al.(24) (p<0.001) and Tremblay et al. 1.36 (95% CI : 1.02-1.30) (25). In these studies, there is a direct relationship between obesity prevalence and inactivity behaviors.
The results of our study showed that screen time activities were greater in male children than in female ones, which are consistent with the results of the study by Chen et al. (p<0.05) (26) who reported higher rates of inactivity among male children. However, our results are inconsistent with the results of the studies conducted by Dutra et al. (24) (p<0.05) and the Ferreira (27) et al., 2.14 (95% CI: 1.03-1.46). In these studies, unlike our study, the prevalence of inactivity has been reported to be more among female children.
In this study, people with high SES spent more time on TV and video watching and electronic games playing. The results are consistent with those of the study conducted by Ferreira et al. (27) in which by an increase in SES, time spent on watching television and playing electronic games increased OR=2.53 (95% CI: 2.19-2.94). However, the results are not consistent with those of the studies carried out by Lioret et al. (28) (p<0.0001) and Drenowatz et al. (29) (p<0.05). In these studies, people in high socioeconomic groups spent less time on watching television than those in lower socioeconomic groups.
ST was inversely associated with maternal education, which was consistent with the results of the studies by Finger et al. (11) OR=0.7 (95% CI: 0.5-0.9) and Proctor et al. (30) who reported less inactivity time in educated mothers. The results of these studies showed that people with high maternal education spent less time on ST behaviors, and maternal education had a protective role in these behaviors.
According to the findings of the present study, the ST was directly related to the residential area. People living in areas with higher SES spent more time on watching television and playing electronic games. The results of the study are inconsistent with those of the study conducted by Andrew et al. (31). In this study, compared with people living in the city, individuals living on the outskirts OR=1.54 (95% CI: 1.18-2.02) and those living in the village OR=1.40 (95% CI: 0.99-1.98) spent more time on watching TV. The results of the study are inconsistent with those of the study conducted by Zheng et al. (32). In this study, individuals residing in the village are more likely to spend their leisure time on inactivity behaviors compared with those living in the city (p<0.0001). The results are also inconsistent with the results of the study conducted by Proctor et al. (30) who reported a higher prevalence of inactivity among people living in slum areas.
This study had some limitations; first, the study was conducted in the city of Sanandaj. Therefore, it cannot be generalized to the whole country. There are also biases in this regard due to the self-report nature of the questionnaires. Moreover, there are recall biases considering the fact that questions related to the activities, which are done over the past year.
Conclusion
In this study, inactivity, independent of physical activity, was concluded to be the main cause of overweight and obesity in individuals with high SES. Therefore, it seems necessary to pay special attention to levels of maternal education, neighborhoods and groups with high SES, and children's gender in managing and controlling the prevalence of inactivity.
Acknowledgments
This paper was extracted from an MS thesis. This study was approved and supported by Kurdistan University of Medical Sciences.
Conflict of interest
The authors declare that they have no conflict of interest.
Cite this article as: Moradi G, Mostafavi F, Azadi N, Esmaeilnasab N, Nouri B. Evaluation of screen time activities and their relationship with physical activity, overweight and socioeconomic status in children 10-12 years of age in Sanandaj, Iran: A cross-sectional study in 2015. Med J Islam Repub Iran 2016 (26 November). Vol. 30:448.
References
- 1. World Health Organization (2010) Global recommendations on Physical Activity for Health. Available:http://whqlibdoc.who.int/publications/2010/9789241599979_eng.pdf. [PubMed]
- 2.Cheval B, Sarrazin P, Pelletier L. Impulsive Approach Tendencies towards Physical Activity and Sedentary Behaviors, but Not Reflective Intentions, Prospectively Predict Non-Exercise Activity Thermogenesis. Plos One . December 19, 2014;10(1371):1–14. doi: 10.1371/journal.pone.0115238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Coombs N, Shelton N, Rowlands A, Stamatakis E. Children's and adolescents' sedentary behaviour in relation to socioeconomic position. Journal of epidemiology and community health. 2013;67(10):868–74. doi: 10.1136/jech-2013-202609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Pyky R, Jauho AM, Ahola R, Ikäheimo TM, Koivumaa-Honkanen H, Mäntysaari M. et al. Profiles of sedentary and non-sedentary young men–a population-based MOPO study. BMC public health. 2015;15(1):1. doi: 10.1186/s12889-015-2495-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Salmon J, Dunstan D, Owen N. Should we be concerned about children spending extended periods of time in sedentary pursuits even among the highly active? International journal of pediatric obesity. 2008;3(2):66–8. doi: 10.1080/17477160802169672. [DOI] [PubMed] [Google Scholar]
- 6.McCormack GR, Mardinger C. Neighbourhood urban form and individual-level correlates of leisure-based screen time in Canadian adults. BMJ open. 2015;5(11):e009418. doi: 10.1136/bmjopen-2015-009418. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.de Rezende LFM, Lopes MR, Rey-López JP, Matsudo VKR, do Carmo Luiz O. Sedentary behavior and health outcomes: an overview of systematic reviews. PloS one. 2014;9(8):e105620. doi: 10.1371/journal.pone.0105620. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Katzmarzyk PT, Lee IM. Sedentary behaviour and life expectancy in the USA: a cause-deleted life table analysis. BMJ open. 2012;2(4):e000828. doi: 10.1136/bmjopen-2012-000828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Atkin AJ, Gorely T, Clemes SA, Yates T, Edwardson C, Brage S. et al. Methods of measurement in epidemiology: sedentary behaviour. International Journal of Epidemiology. 2012;41(5):1460–71. doi: 10.1093/ije/dys118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Zheng J, An R. Satisfaction with local exercise facility: a rural-urban comparison in China. Available: http://www.rrh.org.au/articles/subviewnew.asp?ArticleID=2990 Rural and Remote Health (Internet) 2015;15(2990). [PubMed]
- 11.Finger JD, Mensink GB, Banzer W, Lampert T, Tylleskär T. Physical activity, aerobic fitness and parental socio-economic position among adolescents: the German Health Interview and Examination Survey for Children and Adolescents 2003–2006 (KiGGS) Int J Behav Nutr Phys Act. 2014;11(1):43. doi: 10.1186/1479-5868-11-43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Loprinzi PD, Cardinal BJ, Loprinzi KL, Lee H. Benefits and environmental determinants of physical activity in children and adolescents. Obesity Facts. 2012;5(4):597–610. doi: 10.1159/000342684. [DOI] [PubMed] [Google Scholar]
- 13.De Craemer M, De Decker E, Verloigne M, De Bourdeaudhuij I, Manios Y, Cardon G. The effect of a cluster randomised control trial on objectively measured sedentary time and parental reports of time spent in sedentary activities in Belgian preschoolers: the ToyBox-study. International Journal of Behavioral Nutrition and Physical Activity. 2016;13(1):1. doi: 10.1186/s12966-015-0325-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.De Lepeleere S, De Bourdeaudhuij I, Cardon G, Verloigne M. Do specific parenting practices and related parental self-efficacy associate with physical activity and screen time among primary schoolchildren? A cross-sectional study in Belgium. BMJ open. 2015;5(9):e007209. doi: 10.1136/bmjopen-2014-007209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Delshad M, Sarbazi N, Rezaei_Ghaleh N, Ghanbarian A, Azizi F. Reliability and validity of the Modifiable Activity Questionnaire (MAQ) in an Iranian urban adult population. Archives of Iranian medicine. 2012;15(5):279. [PubMed] [Google Scholar]
- 16.Broderick C, Herbert R, Latimer J, Doorn N. Patterns of physical activity in children with haemophilia. Haemophilia. 2013;19(1):59–64. doi: 10.1111/j.1365-2516.2012.02904.x. [DOI] [PubMed] [Google Scholar]
- 17.Nixon PA, Orenstein DM, Kelsey SF. Habitual physical activity in children and adolescents with cystic fibrosis. Medicine and science in sports and exercise. 2001;33(1):30–5. doi: 10.1097/00005768-200101000-00006. [DOI] [PubMed] [Google Scholar]
- 18.Bammann K, Gwozdz W, Lanfer A, Barba G, De Henauw S, Eiben G. et al. Socioeconomic factors and childhood overweight in Europe: results from the multi‐centre IDEFICS study. Pediatric Obesity. 2013;8(1):1–12. doi: 10.1111/j.2047-6310.2012.00075.x. [DOI] [PubMed] [Google Scholar]
- 19. Emamian MH, Zeraati H, Majdzadeh R, Shariati M, Hashemi H, Fotouhi A. The gap of visual impairment between economic groups in Shahroud, Iran: a Blinder-Oaxaca decomposition. American journal of epidemiology 2011:kwr050. [DOI] [PubMed]
- 20.Moradi G, Ardakani HM, Majdzadeh R, Bidarpour F, Mohammad K, Holakouie-Naieni K. Socioeconomic inequalities in nonuse of seatbelts in cars and helmets on motorcycles among people living in Kurdistan Province, Iran. Iranian journal of public health. 2014;43(9):1239. [PMC free article] [PubMed] [Google Scholar]
- 21. Gamache P, Pampalon R, Hamel D. Methodological guide-The material and social deprivation index: a summary. Institut national de santé publique Québec 2010.
- 22. Moradi G, Mohammad K, Majdzadeh R, Ardakani HM, Naieni KH. Socioeconomic inequality of non-communicable risk factors among people living in Kurdistan Province, Islamic Republic of Iran. International journal of preventive medicine 2013;4(6). [PMC free article] [PubMed]
- 23.Ghavamzadeh S, Khalkhali HR, Alizadeh M. TV viewing, independent of physical activity and obesogenic foods, increases overweight and obesity in adolescents. Journal of Health, Population and Nutrition. 2013;31(3):334. doi: 10.3329/jhpn.v31i3.16825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Dutra GF, Kaufmann CC, Pretto AD, Albernaz EP. Television viewing habits and their influence on physical activity and childhood overweight. Jornal de Pediatria (Versão em Português) 2015;91(4):346–51. doi: 10.1016/j.jped.2014.11.002. [DOI] [PubMed] [Google Scholar]
- 25.Tremblay MS, LeBlanc AG, Kho ME, Saunders TJ, Larouche R, Colley RC. et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth. Int J Behav Nutr Phys Act. 2011;8(1):98. doi: 10.1186/1479-5868-8-98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Chen Y, Zheng Z, Yi J, Yao S. Associations between physical inactivity and sedentary behaviors among adolescents in 10 cities in China. BMC public health. 2014;14(1):1. doi: 10.1186/1471-2458-14-744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Ferreira RW, Rombaldi AJ, Ricardo LIC, Hallal PC, Azevedo MR. Prevalence of sedentary behavior and its correlates among primary and secondary school students. Revista Paulista de Pediatria (English Edition) 2015. [DOI] [PMC free article] [PubMed]
- 28.Lioret S, Touvier M, Lafay L, Volatier J-L, Maire B. Dietary and physical activity patterns in French children are related to overweight and socioeconomic status. The Journal of Nutrition. 2008;138(1):101–7. doi: 10.1093/jn/138.1.101. [DOI] [PubMed] [Google Scholar]
- 29.Drenowatz C, Eisenmann JC, Pfeiffer KA, Welk G, Heelan K, Gentile D. et al. Influence of socio-economic status on habitual physical activity and sedentary behavior in 8-to 11-year old children. BMC Public Health. 2010;10(1):214. doi: 10.1186/1471-2458-10-214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Proctor M, Moore L, Gao D, Cupples L, Bradlee M, Hood M. et al. Television viewing and change in body fat from preschool to early adolescence: The Framingham Children's Study. International journal of obesity. 2003;27(7):827–33. doi: 10.1038/sj.ijo.0802294. [DOI] [PubMed] [Google Scholar]
- 31. Perez A, Kelder S. Prevalence of physical activity and sedentary behaviors by metropolitan status in 4th-, 8th-, and 11th-grade students in Texas, 2004-2005 2009. [PMC free article] [PubMed]
- 32. Zheng J, An R. Satisfaction with local exercise facility: a rural-urban comparison in China. Rural and remote health 2015;15(2990). [PubMed]