

Abstract
Purpose:
The purpose of the study was to evaluate the presentation and management of posthysterectomy ureteral injuries.
Patients and Methods:
Fourteen patients with ureteric injuries after hysterectomy for benign diseases were evaluated. The diagnosis was done based on clinical presentation, intravenous urogram, computed tomography, cystoscopy, and retrograde pyelogram (RGP) depending on the clinical situation.
Results:
Sixteen iatrogenic ureteric injuries in 14 patients over a 2-year period were evaluated. Hysterectomy was the cause of injury in all the cases, 12 abdominal and 2 were vaginal. Two patients presented with anuria, one had ureteric, and bladder injury with hemoperitoneum underwent emergency laparotomy and bilateral ureteral reimplantation. Another patient underwent RGP followed by stenting on the right side, left side unable to put stent so percutaneous nephrostomy (PCN) was done followed by antegrade stenting later. Two patients presented with septicemia and pyonephrosis were managed initially with PCN followed by balloon dilatation and JJ stenting. RGP and retrograde stenting was done in seven of the remaining ten patients and ureteric reimplantation in three patients.
Conclusion:
Patient with ureteric injury should be evaluated and intervened at the earliest. Patients presenting early, within 2 weeks after hysterectomy have higher chances of success with endourological procedures, obviating the need for open surgery.
Keywords: “JJ” stent, stenting, ureterovaginal fistula
INTRODUCTION
Injury to the ureter is a risk of any pelvic or abdominal surgery, including laparoscopy and ureteroscopy. The ureter is especially susceptible to injury during vascular, gynecologic, urologic, and colonic operations. Gynecological surgery remains the most common cause of ureteral injuries; total abdominal hysterectomy is the operation most commonly responsible for a ureteral injury.[1] Other rare causes are secondary to cervicocystopexies both pubic or vaginal, ovarian surgeries, and uterine aspiration.[2] The overall incidence of ureteral injury varies between 0.5% and 10%. Damage to the ureter after external violence is quite rare, occurring in <4% of all penetrating and < 1% of all cases of blunt trauma. Analysis of 13 published studies concluded that the following procedures contribute to iatrogenic ureteral injuries: hysterectomy (54%), colorectal surgery (14%), pelvic procedures such as ovarian tumor removal (8%), transabdominal urethropexy (8%), and abdominal vascular surgery (6%). The total incidence of ureteral injury after gynecologic surgery is reported to be 0.5% to 1.5%, and after abdominoperineal colon resection, it ranges from 0.3% to 5.7%. Currently, the reported rate of ureteral injury varies between 0.5% (experienced surgeons) and 14% (inexperienced surgeons) after laparoscopic hysterectomy presently, laparoscopic assisted vaginal hysterectomy is the most common cause of iatrogenic ureteric injury worldwide, however, in developing, countries open gynecological surgeries still remain the most common cause. Risk factors for the development of ureterovaginal fistulae include endometriosis, obesity, pelvic inflammatory disease, as well as radiation therapy and pelvic malignancy. Nevertheless, Symmonds has noted that the patient with a ureteral injury following gynecologic surgery is typically one who had an uncomplicated, technically easy hysterectomy for the minimal disease. Thus, except for those oncologic cases where a segment of ureter is deliberately excised, many ureteral injuries are likely due to technical or iatrogenic factors.[3] The morbidity associated with such injury may be serious, resulting in increased hospital stay, compromise of the original surgical outcome, secondary invasive interventions, reoperation, potential loss of renal function, and deterioration of the patient's quality of life. To decrease the incidence of iatrogenic ureteral injury, a sound knowledge of abdominal and pelvic anatomy is essential. Loss of continuity of the ureter may result from division or laceration, or from ischemic necrosis related to clamping, ligation, or damage to the blood supply of the ureter.[4] Traditionally, most ureterovaginal fistulas have been repaired by ureteroneocystostomy.[5] Endourological techniques are highly successful in treating posthysterectomy ureteral injuries.[6]
PATIENTS AND METHODS
This study involved patients referred and managed in the department of urology for posthysterectomy ureteric injuries for benign conditions during 2 years from March 2011 to February 2013. During this period, a total of 14 patients with 16 ureteric injuries were treated. The mean age was 38.5 years (24–60-year-old).
All 14 patients suspected to have genitourinary injuries underwent, pretreatment evaluations including history and physical examination. Information was sought on, primary surgery done, intraoperative difficulties and postoperative complications. The various investigations done included: ultrasound of the urinary tract, serum creatinine, urine culture and sensitivity, intravenous urogram (IVU)/computed tomography (CT) scan, cystoscopy and retrograde pyelography (RGP) [Figures 1–7].
Figure 1.

Intravenous urogram of patient s/o right lower ureteric injury
Figure 7.
Computed tomography kidneys, ureters, bladder (P + C) of patient with right ureterovaginal fistula
Figure 2.

Intravenous urogram of patient with left ureterovaginal fistula posthysterectomy showing leak
Figure 3.

Retrograde pyelogram showing in initial difficulty in passing guidewire in patient with left ureterovaginal fistula
Figure 4.

After manipulation of scope guide wire passed across the stricture
Figure 5.

Left nephrostogram in patient in whom percutaneous nephrostomy was done for pyonephrosis s/o left ureterovesicular junction stricture
Figure 6.
Computed tomography kidneys, ureters, bladder (P + C) of patient with right hydroureter and right ureterovaginal fistula
RESULTS
There were 16 iatrogenic ureteric injuries in 14 patients over a 2-year period. Hysterectomy was the cause of injury in all the cases, among whom 12 were abdominal, and 2 were vaginal hysterectomies. The clinical presentation and the radiological findings of all the patients are tabularized in Table 1. Two patients presented with anuria, among whom one had ureteric, and bladder injury with hemoperitoneum as detected by ultrasonography (USG) underwent emergency laparotomy and bilateral ureteral reimplantation with bladder repair. Another patient underwent RGP followed by stenting on the right side, on the left side, we were unable to put a stent, so percutaneous nephrostomy (PCN) was done followed by antegrade stenting later. Two patients presented with septicemia and pyonephrosis were managed initially with PCN followed by balloon dilatation and JJ stenting. Of ten patients who presented with urinary leak, seven patients were successfully stented. Another three patients, in whom stenting was not possible initially and PCN was also not possible due to compact PCS as the ureter directly opened into the vagina, underwent ureteric reimplantation [Table 2]. No nephrectomies were performed. The overall successful resolution of ureteric injuries in JJ stent group in this series was 100%. Complications were wound infection in one patient, prolonged urinary leak in 1, both of which were managed conservatively and incisional hernia in one which required surgical correction. There was no mortality attributable to these ureteric injuries. Follow-up in all these patients was done at 1 month, 3 months, and 9 months after stent removal or definitive procedure. IVU was done in only those patients who showed hydronephrosis on USG [Figure 8]. In this study, two patients who underwent ureteric reimplantation showed hydronephrosis at 3 months follow-up, however, IVP showed no obstruction.
Table 1.
Clinical and radiological findings
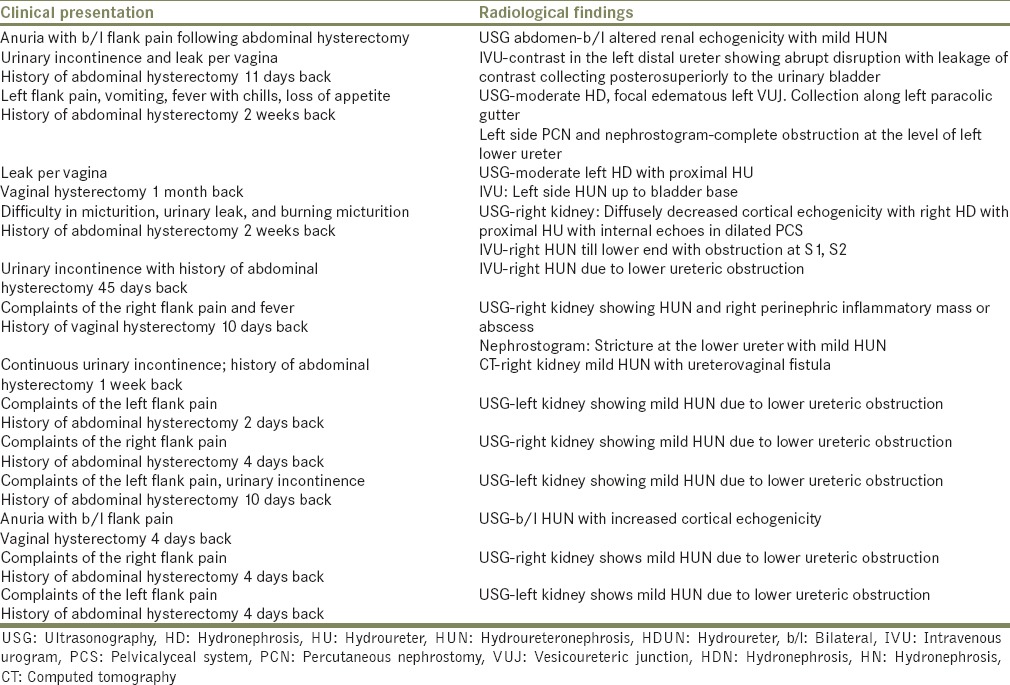
Table 2.
Surgical procedures undertaken
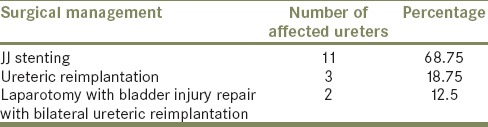
Figure 8.

Postoperative intravenous urogram of patient who underwent laparotomy and B/l ureteric reimplantation
DISCUSSION
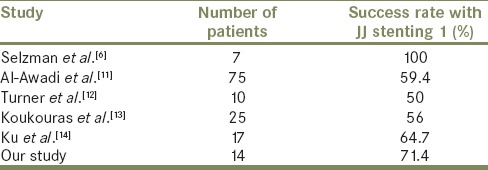
Injury to ureter is a known complication of pelvic or abdominal surgery, including laparoscopy and ureteroscopy.[7] The incidence of iatrogenic ureteral injury during major gynecologic surgery is estimated to be about 0.5%–1.5%. The most common etiology for ureterovaginal fistulae is a surgical injury to the distal ureter, which is most commonly caused by gynecologic procedures. The vast majority of ureterovaginal fistulae occur during procedures for benign rather than malignant indications, hysterectomy being the most common cause.[3] Iatrogenic ureteric injuries have increased markedly during the past two decades. Gynecological laparoscopic procedures account for more than half of the injuries, and the most common location is the lower ureter.[8] The injury or fistula may become apparent either immediately or much more commonly, in a delayed fashion several days to weeks after surgery. Constitutional symptoms may result from hydronephrosis secondary to ureteral obstruction or urinary extravasation into the retroperitoneal space. The clinical history of ureterovaginal fistula is usually straightforward. Typically, a gynecologic procedure, such as hysterectomy, is involved. Poor intraoperative exposures, coupled with heavy bleeding at the operative site, are often the risk factors. The presence of normal upper tracts on imaging essentially rules out ureteral injury; however, the finding of partial ureteral obstruction associated with urinary leakage from the vagina strongly suggests the presence of an ureterovaginal fistula.[9] Various investigations such as USG abdomen, three gauze test, IVU, Cystoscopy and RGP, CT urography, and magnetic resonance (MR) urography can be used to confirm the clinical diagnosis. USG abdomen shows hydroureteronephrosis/pyonephrosis. Three gauze test differentiates vesicovaginal fistula (VVF), ureterovaginal fistula, and stress incontinence. In this test, 100 ml of 1:5 diluted methylene blue solution is instilled into the bladder through an urethral catheter after placing three dry sterile swabs in the upper, middle, and lower third of the vagina. The patient is then asked to walk around for 10 min, after which the swabs are removed and examined. If the lower swab is wet and stained blue, it indicates stress incontinence. If the upper swabs are wet and blue, that indicates VVF, and if the upper swabs are wet but not stained blue, it is an indication of ureterovaginal fistula. IVU demonstrates ureteric injury and hydroureteronephrosis, with cutoff of the contrast at the injured site of the ureter and contrast leak. CT and MR urography are used increasingly for detection of ureteric injuries and demonstrates hydroureteronephrosis due to ureteric stricture and ureterovaginal fistula. An RGP is helpful to diagnose ureteral injury, and the placement of ureteral stent could be attempted at the same time.[10] In our series, open hysterectomy done for benign diseases was the cause of ureteric injury in all the patients. The presenting symptoms were leak per vagina, abdominal pain, fever, and anuria. JJ stenting was possible in patients who presented early (<2 weeks). Leak resolved completely in whom stenting was possible (100% success in all ten patients). In those patients where stenting was not possible underwent ureteric reimplantation because of failed antegrade stenting or failure to do PCN. If we look into the literature [Table 3] Selzman et al. reported that ureterovaginal fistulas resolved in all seven patients treated with an internal ureteral stent.[6] Al-Awadi et al. reported a success rate of 59.4% with “JJ” stent insertion in their series of 75 patients with ureteral injuries.[11] A combined ureteroscopic and fluoroscopic technique to re-establish ureteral integrity has been reported to be a successful treatment.[15] Early intervention is recommended in the treatment of the iatrogenic ureterovaginal fistula, to minimize morbidity, discomfort, and cost.[16] JJ stenting should be attempted in all patients presenting with ureteric injuries. If unsuccessful, these are the candidates for PCN or ureteric reimplantation depending on the clinical situation.
Table 3.
Literature review
CONCLUSION
Posthysterectomy ureteric injury is not an uncommon complication of pelvic surgery. Simple hysterectomy for benign diseases is the most common cause of injury. The patient with ureteric injury should be evaluated and intervened at the earliest. Patients presenting early, within 2 weeks after hysterectomy have higher chances of success with endourological procedures, obviating the need for open surgery.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.McVary KT, Marshall FF. In: Urinary fistulae. Adult and Pediatric Urology. 4th ed. Gillenwater JY, editor. Philadelphia: Lippincott Williams and Wilkins; 2002. pp. 1271–95. [Google Scholar]
- 2.Mteta KA, Mbwambo J, Mvungi M. Iatrogenic ureteric and bladder injuries in obstetric and gynaecologic surgeries. East Afr Med J. 2006;83:79–85. doi: 10.4314/eamj.v83i2.9392. [DOI] [PubMed] [Google Scholar]
- 3.Rovner ES. In: Urinary tract fistulae. Campbell-Walsh Urology. 10th ed. Wein AJ, Kavoussi LR, Novick AC, Partin AW, Peters CA, editors. Philadelphia: Elsevier Saunders; 2012. pp. 2242–6. [Google Scholar]
- 4.Ross G., Jr . In: Ureterovaginal fistula. Current Urologic Therapy. 3rd ed. Seidman EJ, Hannon PM, editors. Philadelphia: W. B. Saunders; 1994. pp. 242–5. [Google Scholar]
- 5.Mandal AK, Sharma SK, Vaidyanathan S, Goswami AK. Ureterovaginal fistula: Summary of 18 years' experience. Br J Urol. 1990;65:453–6. doi: 10.1111/j.1464-410x.1990.tb14785.x. [DOI] [PubMed] [Google Scholar]
- 6.Selzman AA, Spirnak JP, Kursh ED. The changing management of ureterovaginal fistulas. J Urol. 1995;153(3 Pt 1):626–8. doi: 10.1097/00005392-199503000-00020. [DOI] [PubMed] [Google Scholar]
- 7.Watterson JD, Mahoney JE, Futter NG, Gaffield J. Iatrogenic ureteric injuries: Approaches to etiology and management. Can J Surg. 1998;41:379–82. [PMC free article] [PubMed] [Google Scholar]
- 8.Parpala-Spårman T, Paananen I, Santala M, Ohtonen P, Hellström P. Increasing numbers of ureteric injuries after the introduction of laparoscopic surgery. Scand J Urol Nephrol. 2008;42:422–7. doi: 10.1080/00365590802025857. [DOI] [PubMed] [Google Scholar]
- 9.Gerber GS, Schoenberg HW. Female urinary tract fistulas. J Urol. 1993;149:229–36. doi: 10.1016/s0022-5347(17)36045-7. [DOI] [PubMed] [Google Scholar]
- 10.Flynn JT, Tiptaft RC, Woodhouse CR, Paris AM, Blandy JP. The early and aggressive repair of iatrogenic ureteric injuries. Br J Urol. 1979;51:454–7. doi: 10.1111/j.1464-410x.1979.tb03577.x. [DOI] [PubMed] [Google Scholar]
- 11.Al-Awadi K, Kehinde EO, Al-Hunayan A, Al-Khayat A. Iatrogenic ureteric injuries: Incidence, aetiological factors and the effect of early management on subsequent outcome. Int Urol Nephrol. 2005;37:235–41. doi: 10.1007/s11255-004-7970-4. [DOI] [PubMed] [Google Scholar]
- 12.Turner WH, Cranston DW, Davies AH, Fellows GJ, Smith JC. Double J stents in the treatment of gynaecological injury to the ureter. J R Soc Med. 1990;83:623–4. doi: 10.1177/014107689008301009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Koukouras D, Petsas T, Liatsikos E, Kallidonis P, Sdralis EK, Adonakis G, et al. Percutaneous minimally invasive management of iatrogenic ureteral injuries. J Endourol. 2010;24:1921–7. doi: 10.1089/end.2010.0153. [DOI] [PubMed] [Google Scholar]
- 14.Ku JH, Kim ME, Jeon YS, Lee NK, Park YH. Minimally invasive management of ureteral injuries recognized late after obstetric and gynaecologic surgery. Injury. 2003;34:480–3. doi: 10.1016/s0020-1383(02)00412-6. [DOI] [PubMed] [Google Scholar]
- 15.Beaghler MA, Taylor FC, McLaughlin KP. A combined antegrade and retrograde technique for reestablishing ureteral continuity. Tech Urol. 1997;3:44–8. [PubMed] [Google Scholar]
- 16.Elabd S, Ghoniem G, Elsharaby M, Emran M, Elgamasy A, Felfela T, et al. Use of endoscopy in the management of postoperative ureterovaginal fistula. Int Urogynecol J Pelvic Floor Dysfunct. 1997;8:185–90. doi: 10.1007/BF02765810. [DOI] [PubMed] [Google Scholar]