

Abstract
Context:
Spontaneous forniceal rupture is one of the possible complications of urolithiasis. The mechanism of forniceal rupture is not well explained in the literature. Most of the cases presented with sudden onset of acute renal colic and diagnosed by noncontrast CT (NCCT). Until now there is no solid consensus about the ideal management of such a condition.
Aim:
To study indications and validity of conservative management of spontaneous caliceal rupture.
Settings and Design:
This is an observational prospective study.
Materials and Methods:
All cases diagnosed as spontaneous forniceal rupture in our departments from 2011 to 2015 were enrolled. All cases were diagnosed with NCCT or CT-Urography.. Non complicated patients were primarily managed conservatively. Intervention (DJ stent insertion, nephrostomy tube insertion, or urgent ureteroscopy) was reserved to complicated cases or solitary kidney. Drainage of urinoma was done in cases with sizable urinoma (more than 100 ml3).
Results:
A total of 40 patients: Twenty eight (70%) patients had normal serum creatinine level at presentation, while 12 (30%) patients had elevated serum creatinine. Twenty three (57.5%) patients were successfully managed conservatively, their mean size of stone was 6.2 ± 2 mm and the hospital stay was 3.1 ± 1.9 days. Eighteen patients (42.5%) underwent interventions. Their stone size was 4.5 ± 2.1 mm and the hospital stay for the interventional group was 4.2 ± 1.8 days.
Statistical Analysis Used:
Mann-Whitney test was used for testing difference between means because the data groups are not parametric. Otherwise, simple descriptive statestics were used.
Conclusion:
Spontaneous forniceal rupture is more likely to occur with smaller distal ureteric stones. Conservative management is a valid option in non-complicated cases. Intervention should be reserved to complicated cases or cases with sizable urinoma.
Keywords: Forniceal, rupture, stone
INTRODUCTION
Urolithiasis is a major disease worldwide, especially in the Middle East.[1] It has different presentations and complications. Spontaneous forniceal rupture is one of the possible complications of urolithiasis. The mechanism of forniceal rupture is not well explained in literature. Most of the cases presented with sudden onset of acute renal colic and diagnosed by noncontrast computed tomography (NCCT). Although the rate of spontaneous calyceal rupture with obstructing ureteric stone is a relatively uncommon occasion, it still has a high incidence with smaller ureteric stones. Yet, there is no solid consensus about the ideal management of such a condition.[2]
Up to 95% of 2–4 mm ureteric stone will pass spontaneously over a period of 40 days by medical observation alone.[2] Stone passage rate up to 80% for distal ureteric stone with median size of 4.6–6.7 mm has been reported with the help of medical expulsive therapy.[3,4] A period of 2–6 weeks of clinical observation and medical expulsive therapy has been recommended in literature to maximize the chance for spontaneous stone passage.[5]
The clinical concern of forniceal rupture is the reported risk for perinephric abscess formation and urosepsis that carry high morbidity rate.[6] This leads to the current trend to early intervene in the presence of forniceal rupture. Although minimal invasive endourological intervention is the mainstay line of management in literature, it carries its own complications with the associated health and economic burden.
Objectives
In this study, we aim to study the indications and validity of conservative management of spontaneous calyceal rupture.
PATIENTS AND METHODS
It was an observational study, in which we included all cases diagnosed as spontaneous forniceal rupture in our departments from 2011 to 2015. All cases were diagnosed with NCCT. The cases with a history of trauma were excluded from the study. We did CT urography for cases with normal serum creatinine level to confirm the diagnosis and to assess the size of urinoma. We studied the stone side, site, size, and the estimated size of urinoma. Noncomplicated patients were primarily managed conservatively (analgesics, antibiotic, and medical expulsive therapy by oral tamsulosin 0.4 mg once daily). Intervention was reserved to cases with persistent pain, fever, acute kidney injury (raised serum creatinine), sizable urinoma, and/or solitary kidney. Intervention was in the form of urgent double-J (DJ) stent insertion, nephrostomy tube insertion, or urgent ureteroscopy with stone extraction. Drainage of urinoma was needed in cases with sizable urinoma (>100 mL3).
RESULTS
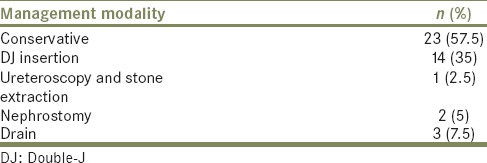
A total of forty patients (28 [70%] males, 12 [30%] females) were included in the study. All the patients had obstructing ureteric stones [Table 1]. Twenty-eight (70%) patients had normal serum creatinine level at presentation, while 12 (30%) patients had acute kidney injury, 2 (5%) patients had fever, and 6 (15%) patients had positive urine culture. The mean size of stone was 4.5 ± 2.1 mm. Extravasation was minimal in 29 (72.5%) patients (just a rim of fluid in the perinephric space), and in 8 (20%) patients, the volume of urinoma was <100 mL3 (median 70 mL3), where only 3 (7.5%) cases had significant amount of urinoma >100 mL3 [Table 2 and Figure 1, 2]. Twenty-three (57.5%) patients were successfully managed conservatively, with the mean hospital stay being 3.1 ± 1.9 days and the mean size of the stones for the conservative group being 4.7 ± 1.8 mm, while 14 (35%) patients underwent DJ stent insertions, followed by ureteroscopy; later, nephrostomy tube was inserted in 2 (5%) patients followed by ureteroscopy, and only 1 (2.5%) patient underwent ureteroscopy with stone extraction. The mean hospital stay for the interventional group was 4.2 ± 1.8 days and the mean size of the stones for the intervention group was 6.2 ± 2.4 mm [Table 3 and Figures 1, 2]. Drainage of urinoma was done in 3 (7.5%) patients along with DJ stent. The median volume of the drained urinoma in the three cases was 145 mL. Follow-up of patients' postdrainage with abdominal ultrasonography showed no collection.
Table 1.
Clinical and radiological findings of the patients
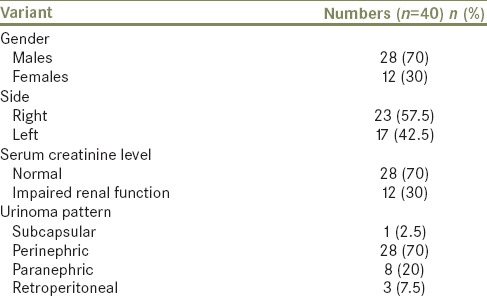
Table 2.
Urinoma size in mL (cc) in relation to the site of the obstructing ureteral stone
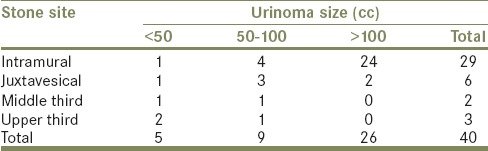
Figure 1.

Noncontrast computed tomography of right distal ureteric stone with perinephric urinoma
Figure 2.
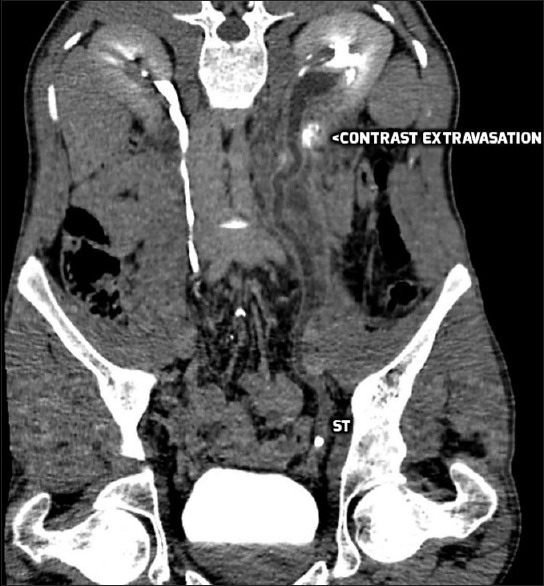
CT with contrast showing left proximal ureteric stone with contrast extravasation
Table 3.
Management options of the patients
DISCUSSION
Forniceal rupture is a serious urologic emergency. Despite meeting such cases in the urologic practice, there is still obscurity about its definite pathogenesis. The situation even more complicates when it comes to definite guidelines for its management.
We prospectively enrolled forty patients presented to our Urology Departments to study different lines of management and their outcomes. Most of the reported series are case series and case reports studied the spontaneous forniceal rupture of all etiologies, while in our study, we focused on at obstruction from ureteric stone as it is the main etiology.[7]
The intrarenal collecting system pressure increases secondary to acute unilateral ureteric obstruction; this leads to urine backflow as a compensatory mechanism to decrease the intrarenal collecting system pressure. Moreover, the increased intrarenal collecting system pressure will induce reduction in renal blood flow secondary to increase in renovascular resistance. With the increase in intrarenal vascular resistance, the diastolic blood flow velocity in intrarenal arteries will diminish and subsequently the renal resistive index is increased.[8] Subsequently, urine production of the obstructed renal unit will decrease, and this mechanism needs time to occur and the kidney to adapt to it, while in sudden acute obstruction, this mechanism may not happen, and further urine production will persist, which adds more to intrapelvic renal pressure that may lead to forniceal rupture. By applying Laplaces's Law (tension = pressure × radius), if a pressure exceeds the tensile strength of the renal fornix, this will lead to forniceal rupture and extravasation of urine as this phenomenon is renoprotective[9] by decreasing the collecting system pressure. This phenomenon is seen more with obstructing ureteric stone due to the sudden sharp increase in the intrarenal pelvis pressure, before the collecting system even can accommodate this increment in pressure. There is no other explanation of spontaneous forniceal rupture due to difficulty to study the momentum of this phenomenon. One of the specific manifestations of forniceal rupture is the sudden pain relief due to the decrease in collecting system pressure.[6] The problem with forniceal rupture is the risk of infection of the urinoma, abscess formation, and sepsis as up to 25% of patients with renal or perirenal abscess had ureteric stone and/or forniceal rupture.[10] This shows the importance of antibiotic coverage of these patients, as it was a standard part of treatment in all our patients, either if they were managed conservatively or underwent intervention. Doehn et al.[6] reported 92% of their case series treated with antibiotics.
In our series, forniceal rupture was mainly secondary to distal ureteric stone (below sacroiliac joint) in (87.5%) of the patients; same findings reported by Autorino et al.[7] in their 108 patients series (75.7% of the patients) and Doehn et al.[6] in their 162 patients series (43.2% of the patients). The mean size of stone in our study was 4.5 ± 2.1 mm, and it was in the intramural part in 29 (72.5%) patients, 6 (15%) in the juxtavesical, 1 (2.5%) in the middle third, and 3 (7.5%) in the upper ureter. We believe that forniceal rupture is more common with small distal ureteric stone, as these stones will rapidly pass the upper and middle ureter, then will suddenly obstruct the distal ureter, which is the most narrow part of the ureter, leading to sudden sharp rise of collecting system pressure before the compensatory mechanisms work and leads to forniceal rupture. Furthermore, the likelihood of intervention is more, the smaller the stone is 6.2 ± 2.4 in conservative group and 4.5 ± 2.1 mm in the intervention group (P < 0.05). The other importance of these findings is the need to redefine the stone-free status and insignificant stone residual definition of all urological procedures as small as 3 mm ureteric stone can cause ureteric obstruction, forniceal rupture, and sizable urinoma.
Kalafatis et al. treated 35 (41%) of 81 cases in a conservative approach (bed rest, intravenous fluid, and antibiotic) and concluded that conservative management can be applied to certain patients with fornix rupture.[11] The majority of our patients were managed conservatively, in the form of analgesics, medical expulsive therapy (tamsulosin 0.4 mg once daily), and antibiotics, accounting for 57.5% of our patients. We believe that conservative management is a valid option of treatment of noncomplicated cases of spontaneous fornix rupture. Noteworthy, limitations of the current study included the few number of patients, heterogeneity of presentations which hinder proper grouping, and thus further investigations in that area is definitely required.
CONCLUSION
Spontaneous forniceal rupture is more likely to occur with smaller distal ureteric stone. Conservative management is a valid option in noncomplicated cases. Intervention should be reserved to complicated cases or cases with sizable urinoma.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Robertson WG. Stone formation in the Middle Eastern Gulf States: A review. Arab J Urol. 2012;10:265–72. doi: 10.1016/j.aju.2012.04.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gershman B, Kulkarni N, Sahani DV, Eisner BH. Causes of renal forniceal rupture. BJU Int. 2011;108:1909–11. doi: 10.1111/j.1464-410X.2011.10164.x. [DOI] [PubMed] [Google Scholar]
- 3.Miller OF, Kane CJ. Time to stone passage for observed ureteral calculi: A guide for patient education. J Urol. 1999;162(3 Pt 1):688–90. doi: 10.1097/00005392-199909010-00014. [DOI] [PubMed] [Google Scholar]
- 4.Porpiglia F, Ghignone G, Fiori C, Fontana D, Scarpa RM. Nifedipine versus tamsulosin for the management of lower ureteral stones. J Urol. 2004;172:568–71. doi: 10.1097/01.ju.0000132390.61756.ff. [DOI] [PubMed] [Google Scholar]
- 5.Agrawal M, Gupta M, Gupta A, Agrawal A, Sarkari A, Lavania P. Prospective randomized trial comparing efficacy of alfuzosin and tamsulosin in management of lower ureteral stones. Urology. 2009;73:706–9. doi: 10.1016/j.urology.2008.11.013. [DOI] [PubMed] [Google Scholar]
- 6.Doehn C, Fiola L, Peter M, Jocham D. Outcome analysis of fornix ruptures in 162 consecutive patients. J Endourol. 2010;24:1869–73. doi: 10.1089/end.2010.0018. [DOI] [PubMed] [Google Scholar]
- 7.Autorino R, De Sio M, Damiano R, Di Lorenzo G, Perdonà S, Russo A, et al. The use of tamsulosin in the medical treatment of ureteral calculi: Where do we stand? Urol Res. 2005;33:460–4. doi: 10.1007/s00240-005-0508-0. [DOI] [PubMed] [Google Scholar]
- 8.Apoku IN, Ayoola OO, Salako AA, Idowu BM. Ultrasound evaluation of obstructive uropathy and its hemodynamic responses in southwest Nigeria. Int Braz J Urol. 2015;41:556–61. doi: 10.1590/S1677-5538.IBJU.2014.0197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Upputalla R, Moore RM, Jim B. Spontaneous forniceal rupture in pregnancy. Case Rep Nephrol 2015. 2015:379061. doi: 10.1155/2015/379061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Coelho RF, Schneider-Monteiro ED, Mesquita JL, Mazzucchi E, Marmo Lucon A, Srougi M. Renal and perinephric abscesses: Analysis of 65 consecutive cases. World J Surg. 2007;31:431–6. doi: 10.1007/s00268-006-0162-x. [DOI] [PubMed] [Google Scholar]
- 11.Kalafatis P, Zougkas K, Petas A. Primary ureteroscopic treatment for obstructive ureteral stone-causing fornix rupture. Int J Urol. 2004;11:1058–64. doi: 10.1111/j.1442-2042.2004.00949.x. [DOI] [PubMed] [Google Scholar]