

Abstract
Background
Alcohol use is a key risk factor for young adult mortality and disease, but limited research has focused on high-risk alcohol use among individuals moving from early young adulthood into building and maintaining an initial structure of adult life. This study estimated the prevalence of a range of alcohol use behaviors among US young adults aged 25/26, examined evidence for historical change in prevalence rates, and estimated associations between alcohol use and key demographic, substance use, and adult social role characteristics.
Methods
Data were obtained from 3,542 individuals selected for follow-up from the nationally-representative 12th grade student Monitoring the Future study. Respondents self-reported alcohol use behaviors at age 25/26 during calendar years 2005–2014.
Results
Two-fifths (39.9%) of young adults aged 25/26 reported being intoxicated at least once in the past 30 days; 25.6% reported usually experiencing a sustained high of 3 or more hours when drinking alcohol. Past two-week binge drinking (5+ drinks in a row) was reported by 36.3% of respondents. Past two-week high-intensity drinking (10+ drinks in a row) was reported by 12.4%. These age 25/26 alcohol use prevalence rates remained stable over the ten years of data examined, in contrast to significant declines over historical time in alcohol prevalence rates among these same individuals at age 18. High-risk drinking was particularly associated with being male, White, unmarried, employed, a non-parent, and an alcohol user before finishing high school.
Conclusions
Among US young adults in their mid-twenties, alcohol use was highly normative and frequently included participation in high-risk drinking behaviors. High-risk alcohol use prevention approaches developed specifically to reach young adults in their mid-twenties are needed, as well as efforts to increase proactive clinician screening to identify young adults participating in high-risk alcohol use.
Keywords: Alcohol consumption, young adult, binge drinking, high-intensity drinking, alcoholic intoxication
INTRODUCTION
Alcohol use is the third leading global risk factor for disease, and the leading worldwide risk factor for mortality and disease for individuals aged 15–49.1 Within the US, annual alcohol-attributable deaths (AADs) due to excessive alcohol use claim more than 87,000 lives.2 Individuals aged 20–34 bear the largest share of AADs due to acute causes such as traffic accidents,2 and the annual prevalence of alcohol use disorders is highest among young adults aged 18–29.3 Both acute and long-term risks to the public and to individual users rise exponentially as the amount of alcohol consumed increases.4, 5 Importantly, the average number of drinks consumed during a binge episode among US young adults aged 18–24 was 9.5.6 A growing number of researchers are calling for increased attention to the issue of very high-risk drinking, such as consumption 10+ or even 15+ drinks on a single occasion.4, 5 Annual and 30-day alcohol use prevalence increase through late adolescence and early young adulthood, peak in the 20s, and then decrease to some degree thereafter.7–9 Binge drinking (5+ drinks in a row) generally peaks in the early 20s.8–10 Perhaps not surprisingly, a great deal of alcohol use research has focused on the early 20s, when individuals transition from adolescence to initial early adulthood and reach lifetime peaks in binge drinking. A substantive body of research has examined drinking behaviors and consequences among college students, in particular. 11–14
Levinson15 identified a second major transition in young adulthood, when individuals move from initial early adulthood into building and maintaining the initial structure of adult life (roughly ages 22–28). According to Levinson, the two major tasks of this developmental period are to simultaneously (1) expand and explore options available for structure in regards to relationships, occupation, and geographical location, and (2) choose among available options to create an initial, stable adult life.16 Similarly, Erikson17 asserts that young adults’ primary task is developing intimacy. High-risk alcohol use during the second major transition in young adulthood may compromise an individual’s ability to successfully navigate these key developmental tasks. Adolescent and early young adult drinking has been associated with impaired brain function and development,18 and research now confirms that brain development—especially that of the frontal lobe, which is involved in executive functions such as decision making, planning, and impulse control—continues throughout the 20s.19, 20 Yet, little is known about high-risk alcohol use during the second transition in young adulthood.
Research indicates that several alcohol use behaviors—including annual use, binge drinking, and high-intensity drinking (10+ drinks in a row)—have significantly decreased in prevalence across historical time during late adolescence (age 18).21, 22 The degree to which such decreases have persisted into the mid-twenties is not fully known. Studies have found that in conjunction with the decreasing rate of binge drinking at age 18 over time, there has been a co-occurring increase in the acceleration rate of binge drinking through the early years of young adulthood (i.e., 21/22) and slower deceleration rate thereafter.23, 24 Similar research on other high-risk drinking behaviors has been unavailable. The likelihood of discussing alcohol use with a doctor or other health professional has been shown to decrease sharply after age 24,25 but empirical studies of high-risk alcohol use among this group have not been available to indicate if such decreased clinician communication overall is warranted, or which subgroups may be at highest risk. More detailed information on high-risk alcohol use behaviors—including consuming large quantities of alcohol and drinking to intoxication—among individuals undergoing the second major transition in young adulthood is needed.
Population studies on binge drinking are available that combine prevalence rates across young adults aged 26–3426 and 25–34.10, 25, 27–29 Rates of binge drinking, high-intensity drinking, and intoxication (reporting being drunk or very high from drinking in the past 30 days) have also been released that combine rates across young adults aged 19–28.8 These studies indicate that high-risk alcohol use remains prevalent during young adulthood overall, but the age range is too broad to provide estimates specifically for individuals undergoing the second major young adulthood transition. Published estimates of intoxication and binge drinking among more discrete young adult age groups have been limited to single-year estimates only.8 The current paper contributes to the literature by examining a range of high-risk alcohol use behaviors (intoxication, binge drinking, high-intensity drinking, and length of time usually stay drunk) among young adults aged 25/26, historical change in these behaviors, and associations with key demographic and social role characteristics.
Several demographic and social role characteristics are known to be associated with high-risk alcohol use, but the extent to which these remain strong indicators of behavior in the mid-twenties is unknown. Adult high-risk drinking behaviors are particularly prevalent among males10, 27, 28 and the unemployed.10 Adult high-risk drinking behaviors are also associated with race/ethnicity, education level, and annual family income, but association directions vary based on the specific drinking behavior examined.10, 27, 28 Among individuals aged 19–32, social roles of being a full-time college student, single, and a non-parent are associated with increased binge drinking.30 Age of alcohol use initiation and co-occurring use of substances other than alcohol also are likely to be strong correlates of high-risk alcohol use during the mid-twenties. Alcohol-related problems throughout adulthood are associated with early (prior to age 15) alcohol initiation.31 For college students, high-risk alcohol behaviors are more likely among those who also use cigarettes, marijuana, and illicit drugs.9, 32, 33 Prevention and screening efforts to reduce high-risk drinking (and associated harms) among individuals undergoing the second major transition of young adulthood will have the best likelihood to succeed if informed by clear data on populations most at risk.
The current study focuses on high-risk alcohol use among US young adults aged 25–26. Three research questions guided analyses: (1) What are the prevalence rates of 30-day intoxication, usually experiencing a sustained high of 3+ hours, past 2-week binge drinking (5+ drinks in a row), and past 2-week high-intensity drinking (10+ drinks in a row)? (2) Have prevalence rates changed over historical time, and is there evidence that the decreasing levels of alcohol use observed among adolescents have persisted as the same individuals enter their mid-twenties? (3) Does prevalence vary based on key demographics, substance use, and adult social roles?
METHODS
Data, Setting, and Study Population
The study utilizes data from Monitoring the Future (MTF), a national cohort-sequential study. Detailed methodology, including informed consent procedures, is provided elsewhere.8, 34 Briefly, a nationally representative sample of approximately 15,000 12th graders (modal age 18; hereafter referred to as age 18) from about 130 schools has been surveyed annually since 1975 yielding sequential cohorts. Students complete self-administered surveys, typically during a normal class period. A representative random sub-sample of about 2,400 seniors is selected from each annual sample for longitudinal follow-up; substance users are over-sampled (analyses include weights accounting for sampling procedures). Respondents are randomly divided with half surveyed in odd-numbered years (starting at modal age 19) and half in even-numbered years (starting at modal age 20). Follow-up questionnaires are mailed in the spring with a modest monetary incentive of $20–$25. Approval was obtained from the Institutional Review Board for this study.
Due to our interest in high-risk alcohol behavior measures added to the MTF study in 2005, the current analyses utilize items asked from 2005 onwards on two of the six questionnaire forms (distributed randomly) used for data collection. Thus, the current sample was limited to 12th-grade cohorts from 1997–2007 who provided data at modal age 25/26 (hereafter referred to as age 25/26) during calendar years 2005–2014 (see Supplemental Table 1). The average age 18 response rate for these cohorts was 82.5%. A total of 8,074 individuals from the 1997–2007 cohorts responded to the relevant questionnaire forms at age 18 and were selected for longitudinal participation as described above. Of these, 3,609 individuals (44.7%) responded at age 25/26 in calendar years 2005–2014. Data on at least one alcohol use outcome included in the current analyses were available for 98.1% of responding individuals, yielding a total analytical sample of 3,542 respondents (43.9% of the eligible sample). Adjustments for attrition are discussed in the Analysis section below.
Measures
Alcohol use
Six alcohol use behaviors were used in these analyses: Past 12-month use (1=any; 0=none); Past 30-day use (1=any; 0=none); Intoxication in past 30 days (1=ever drunk or very high from drinking; 0=never); Sustained high (1=usually stay drunk or high for three or more hours; 0=two or fewer hours or usually don’t get high); Binge drinking (1=5+ drinks in a row the past two weeks; 0=never); and High-intensity drinking (1=10+ drinks in a row in the last two weeks; 0=never). (See Supplemental Table 2 for complete wording of alcohol use measures.)
Demographics and alcohol initiation (age 18)
Gender was coded as male or female. Self-identified race/ethnicity was coded as White, Black, Hispanic, or Other. Parental education indicated whether at least one parent had graduated from college. Alcohol initiation (first trying more than just a few sips of alcohol) was coded as before high school (grade 8 or below), during high school (grades 9–12), or high school abstainer (reporting no lifetime drinking when surveyed at age 18).
Concurrent substance use and social roles (age 25/26)
Separate measures were coded for any past 30-day cigarette use, past 30-day marijuana use, and past 12-month use of illicit drugs other than marijuana (LSD, other psychedelics, cocaine, amphetamines, barbiturates, tranquilizers, heroin, other narcotics). Marital status (not married vs. married), parental status (no children vs. any children), employment status (no paid vs. paid employment), and college degree status (graduated from a 4-year college vs. not) were used to assess social roles at age 25/26.
Analysis
Descriptive and regression analyses were conducted using SAS 13.2. Bivariate and multivariable models were estimated using PROC LOGISTIC. Historical trend analyses were modeled using Joinpoint 4.0.1.35, 36 All analyses were weighted using attrition weights, calculated as the inverse of the probability of participation at age 25/26 based on the following covariates measured at age 18: gender, race/ethnicity, college plans, high school grades, number of parents in the home, religiosity, parental education, alcohol use, cigarette use, marijuana use, region, cohort, and sampling weight correcting for over-sampling of age 18 substance users. Previous research has indicated that while the effects of attrition within the MTF panel data are statistically significant, they are small in magnitude.24 Supplemental Table 3 provides a comparison of the total possible age 18 sample selected for follow-up with the analytic sample used in these analyses weighted using the attrition weights. Missing data on covariates were modeled with missing data indicators.
RESULTS
Sample Characteristics
Table 1 provides descriptive statistics. The sample reflected national gender and racial/ethnic distributions. Age 25/26 social role prevalence measures indicated approximately one quarter were married (26.7%) and/or had children (25.9%), slightly less than half had graduated from a 4-year college (43.6%), and most had some type of paid employment (83.7%).
Table 1.
Descriptive Statistics
| Proportion | SD | Proportion | SD | ||
|---|---|---|---|---|---|
| Alcohol use outcomes measured at age 25/26 | |||||
| Any past 12-month use | 0.883 | 0.321 | Sustained highb | 0.256 | 0.437 |
| Any past 30-day use | 0.747 | 0.435 | Binge drinkingc | 0.363 | 0.481 |
| Intoxicationa | 0.399 | 0.490 | High-intensity drinkingd | 0.124 | 0.330 |
| Demographics measured at age 18 | |||||
| Male | 0.459 | 0.498 | Parental education | ||
| Race/ethnicity | Less than college degree | 0.458 | 0.498 | ||
| White | 0.667 | 0.471 | College degree | 0.496 | 0.500 |
| Black | 0.111 | 0.314 | Missing | 0.047 | 0.212 |
| Hispanic | 0.113 | 0.317 | Initiation of alcohol use | ||
| Other | 0.087 | 0.282 | High school abstainer | 0.195 | 0.397 |
| Missing | 0.022 | 0.147 | During high school | 0.456 | 0.498 |
| Before high school | 0.239 | 0.426 | |||
| Missing | 0.109 | 0.312 | |||
| Concurrent substance use and social roles measured at age 25/26 | |||||
| Past 12-month use of illicit drugs other than marijuana | Parental status | ||||
| None | 0.796 | 0.403 | No children | 0.736 | 0.441 |
| Any | 0.168 | 0.374 | Any children | 0.259 | 0.438 |
| Missing | 0.035 | 0.185 | Missing | 0.005 | 0.072 |
| Past 30-day cigarette use | College degree status (4-year college) | ||||
| None | 0.746 | 0.435 | Had not graduated | 0.543 | 0.498 |
| Any | 0.238 | 0.426 | Had graduated | 0.436 | 0.496 |
| Missing | 0.016 | 0.126 | Missing | 0.020 | 0.141 |
| Past 30-day marijuana use | Employment status | ||||
| None | 0.837 | 0.369 | No paid employment | 0.147 | 0.354 |
| Any | 0.150 | 0.357 | Any paid employment | 0.837 | 0.369 |
| Missing | 0.013 | 0.111 | Missing | 0.016 | 0.125 |
| Marital status | |||||
| Not married | 0.727 | 0.446 | |||
| Married | 0.267 | 0.442 | |||
| Missing | 0.006 | 0.078 | |||
Note. Total N (unweighted) = 3,542. For specific outcomes, unweighted n is as follows: 12-month use 3,521; 30-day use 3,526; intoxication 1,755; sustained high 1,736; binge drinking 3,501; high-intensity drinking 1,739. Missing data on non-outcome measures modeled using missing data indicators as shown.
Ever drunk or very high from drinking in past 30 days
Usually stay drunk or high for 3 or more hours when drinking.
Having 5 or more drinks in a row on at least one occasion in the past two weeks.
Having 10 or more drinks in a row on at least one occasion in the past two weeks.
Research Question (RQ) 1: Age 25/26 Alcohol Use Prevalence
Any past 12-month or 30-day alcohol use was normative (88.3% and 74.7%, respectively; see Table 1). Two-fifths (39.9%) reported being intoxicated at least once in the past 30 days. Slightly more than one-quarter (25.6%) reported usually experiencing a sustained high when drinking alcohol. In the past 2 weeks, binge drinking (5+ drinks) was reported by more than one-third (36.3%) of respondents, and high-intensity drinking (10+ drinks) was reported by 12.4% of respondents. Additional cross tabulations enabling a more nuanced understanding of alcohol use among these young adults showed that among individuals reporting any past 30-day alcohol use, approximately half reported getting intoxicated (54.6%) and/or binge drinking (48.5%). Among respondents reporting binge drinking, half (49.3%) usually experienced a sustained high and more than one-third (36.8%) reported high-intensity drinking.
RQ 2: Historical Trends in Age 25/26 Alcohol Use
Prevalence rates of all age 25/26 alcohol use outcomes included in the current analyses (past 12-month and 30-day alcohol use, intoxication, sustained high, binge drinking, and high-intensity drinking) remained statistically unchanged from 2005 through 2014 (see Figure 1 and Table 2). Such stability was in contrast to the significant declines across historical time in past 12-month and 30-day alcohol use, and binge drinking reported by the same individuals at age 18 (Table 2). (High-intensity drinking [added in 2005] was not available from the majority of these individuals at age 18, so no comparison could be made for that indicator.)
Figure 1.
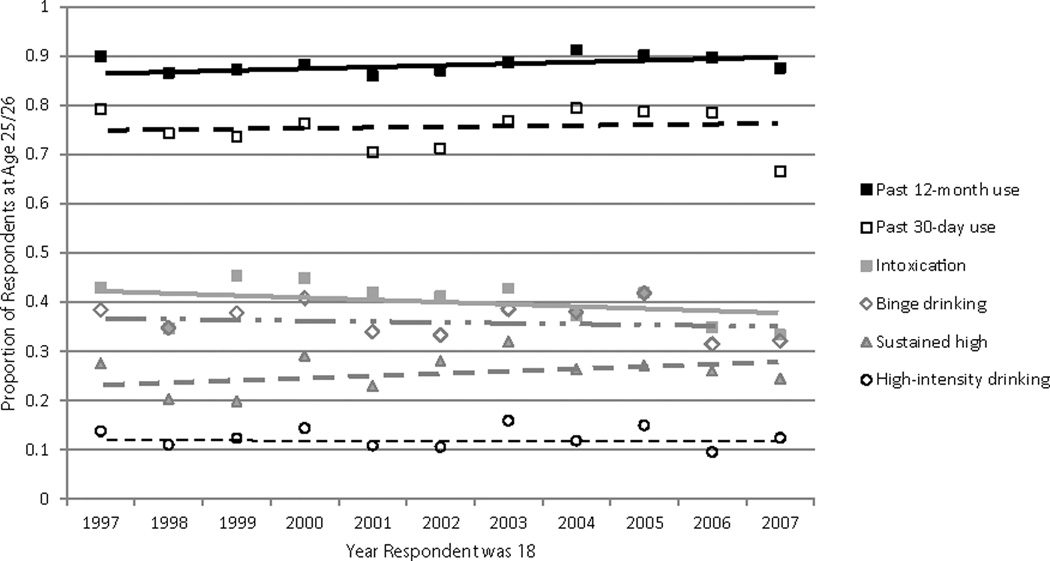
Historical trends in the prevalence of selected alcohol use behaviors at age 25/26 among 11 cohorts of US high school seniors. Age 25/26 data collected in calendar years 2005–2014. Intoxication defined as ever drunk or very high from drinking in past 30 days. Binge drinking defined as having 5 or more drinks in a row on at least 1 occasion in the past 2 weeks. Sustained high defined as usually stay drunk or high for 3 or more hours when drinking. High-intensity drinking defined as having 10 or more drinks in a row on at least 1 occasion in the past 2 weeks.
Table 2.
Comparative Historical Trends in Selected Alcohol Use Behaviors at Ages 18 and 25/26 among 11 Cohorts (1997–2007) of US High School Seniors
| Age 18 | Age 25/26 | |||||
|---|---|---|---|---|---|---|
| Slope | SE | p | Slope | SE | p | |
| Past 12-month alcohol use | −0.008 | 0.003 | 0.034 | 0.003 | 0.002 | 0.122 |
| Past 30-day alcohol use | −0.010 | 0.004 | 0.021 | 0.002 | 0.004 | 0.532 |
| Intoxicationa | −0.006 | 0.005 | 0.232 | −0.005 | 0.004 | 0.284 |
| Sustained highb | −0.001 | 0.004 | 0.775 | 0.006 | 0.004 | 0.151 |
| Binge drinkingc | −0.011 | 0.004 | 0.020 | −0.002 | 0.004 | 0.588 |
| High-intensity drinkingd | -- | -- | -- | −0.001 | 0.002 | 0.635 |
Note. Age 18 data collected during calendar years 1997–2007. Age 25/26 data collected during calendar years 2005–2014.
Ever drunk or very high from drinking in past 30 days
Usually stay drunk or high for 3 or more hours when drinking.
Having 5 or more drinks in a row on at least one occasion in the past two weeks.
Having 10 or more drinks in a row on at least one occasion in the past two weeks. This measure was first asked in 2005; thus, historical trends for this measure at age 18 are not available.
FIGURE 1 Historical trends in the prevalence of selected alcohol use behaviors at age 25/26 among eleven cohorts of US high school seniors. Notes. Age 25/26 data collected in calendar years 2005–2014. Intoxication defined as ever drunk or very high from drinking in past 30 days. Binge drinking defined as having 5 or more drinks in a row on at least one occasion in the past two weeks. Sustained high defined as usually stay drunk or high for 3 or more hours when drinking. High-intensity drinking defined as having 10 or more drinks in a row on at least one occasion in the past two weeks.
RQ 3: Demographic, Substance Use, and Social Role Associations with Age 25/26 Alcohol Use
Table 3 presents unadjusted cell percentages of each independent variable category reporting the four examined age 25/26 high-risk alcohol use outcomes: intoxication, sustained high, binge drinking, and high-intensity drinking. Full multivariable logistic regression results are also reported.
Table 3.
Demographic, Substance Use, and Social Role Associations with Perceived Alcohol Intoxication, Binge and High-Intensity Drinking among US Young Adults aged 25/26
| Intoxicationa | Sustained highb | Binge drinkingc | High-intensity drinkingd | |||||
|---|---|---|---|---|---|---|---|---|
| %e | AORf (95% CIg) p | % | AOR (95% CI) p | % | AOR (95% CI) p | % | AOR (95% CI) p | |
| Demographics measured at age 18 | ||||||||
| Gender | ||||||||
| Female | 34.2 | (ref) | 25.8 | (ref) | 27.0 | (ref) | 6.3 | (ref) |
| Male | 46.9 | 1.54 (1.31–1.82) <.001 | 25.4 | 0.89 (0.75–1.06) 0.196 | 47.4 | 2.50 (2.23–2.81) <.001 | 19.5 | 4.02 (3.12–5.19) <.001 |
| Race/ethnicity | ||||||||
| White | 44.1 | (ref) | 26.8 | (ref) | 40.1 | (ref) | 14.0 | 1.50 (1.13–1.98) 0.005 |
| Black | 22.0 | 0.35 (0.26–0.49) <.001 | 20.0 | 0.73 (0.54–0.99) 0.045 | 19.7 | 0.42 (0.34–0.52) <.001 | -- | |
| Hispanic | 34.8 | 1.03 (0.79–1.34) 0.834 | 25.7 | 1.00 (0.76–1.31) 0.979 | 34.3 | 0.90 (0.75–1.09) 0.273 | -- | |
| Other | 33.5 | 0.53 (0.39–0.73) <.001 | 23.1 | 0.83 (0.61–1.11) 0.203 | 30.0 | 0.58 (0.47–0.71) <.001 | -- | |
| B/H/Oh | -- | -- | -- | 8.5 | (ref) | |||
| Parental education | ||||||||
| Less than college degree | 34.1 | (ref) | 26.0 | (ref) | 34.6 | (ref) | 10.7 | (ref) |
| College degree | 46.6 | 1.37 (1.15–1.63) <.001 | 24.2 | 0.86 (0.71–1.03) 0.099 | 38.3 | 0.95 (0.84–1.08) 0.441 | 13.3 | 1.11 (0.86–1.44) 0.411 |
| Initiation of alcohol use | ||||||||
| During high school | 45.2 | (ref) | 27.8 | (ref) | 41.0 | (ref) | 13.4 | (ref) |
| Before high school | 49.9 | 1.17 (0.94–1.44) 0.163 | 32.4 | 1.22 (1.00–1.48) 0.050 | 45.2 | 1.10 (0.96–1.27) 0.181 | 18.1 | 1.33 (1.03–1.71) 0.029 |
| High school abstainer | 20.8 | 0.40 (0.32–0.51) <.001 | 10.9 | 0.43 (0.32–0.57) <.001 | 17.1 | 0.37 (0.31–0.44) <.001 | 4.3 | 0.40 (0.26–0.63) <.001 |
| Concurrent substance use and social roles measured at age 25/26 | ||||||||
| Past 12-month use of illicit drugs other than marijuana | ||||||||
| None | 33.9 | (ref) | 19.8 | (ref) | 30.5 | (ref) | 8.7 | (ref) |
| Any | 72.7 | 2.27 (1.77–2.92) <.001 | 51.9 | 3.04 (2.46–3.74) <.001 | 61.5 | 2.03 (1.73–2.38) <.001 | 28.7 | 2.52 (1.92–3.31) <.001 |
| Past 30-day cigarette use | ||||||||
| None | 33.2 | (ref) | 20.7 | (ref) | 29.3 | (ref) | 7.7 | (ref) |
| Any | 62.1 | 2.61 (2.12–3.20) <.001 | 41.2 | 1.88 (1.54–2.29) <.001 | 58.6 | 2.59 (2.25–2.97) <.001 | 27.0 | 2.96 (2.29–3.83) <.001 |
| Past 30-day marijuana use | ||||||||
| None | 34.3 | (ref) | 22.5 | (ref) | 31.3 | (ref) | 9.5 | (ref) |
| Any | 72.8 | 3.12 (2.37–4.09) <.001 | 44.5 | 1.39 (1.11–1.75) 0.004 | 61.8 | 1.98 (1.67–2.34) <.001 | 27.8 | 1.72 (1.29–2.29) <.001 |
| Marital status | ||||||||
| Not married | 45.8 | (ref) | 29.0 | (ref) | 40.8 | (ref) | 14.5 | (ref) |
| Married | 26.1 | 0.51 (0.42–0.63) <.001 | 15.2 | 0.56 (0.45–0.71) <.001 | 24.0 | 0.59 (0.51–0.68) <.001 | 6.2 | 0.68 (0.48–0.96) 0.027 |
| Parental status | ||||||||
| No children | 44.8 | (ref) | 27.7 | (ref) | 40.2 | (ref) | 14.7 | (ref) |
| Any children | 26.2 | 0.70 (0.55–0.88) 0.002 | 19.6 | 0.79 (0.62–1.00) 0.051 | 25.4 | 0.70 (0.60–0.82) <.001 | 5.7 | 0.43 (0.30–0.62) <.001 |
| Employment | ||||||||
| No paid employment | 32.5 | (ref) | 24.1 | (ref) | 26.2 | (ref) | 6.2 | (ref) |
| Any paid employment | 41.2 | 1.22 (0.96–1.55) 0.112 | 26.0 | 1.05 (0.82–1.35) 0.680 | 38.2 | 1.56 (1.31–1.85) <.001 | 13.8 | 3.02 (1.97–4.65) <.001 |
| Graduated from 4-year college | ||||||||
| No | 36.4 | (ref) | 25.7 | (ref) | 35.0 | (ref) | 11.8 | (ref) |
| Yes | 44.7 | 1.66 (1.38–1.99) <.001 | 26.0 | 1.20 (0.99–1.46) 0.062 | 38.4 | 1.43 (1.26–1.63) <.001 | 12.9 | 1.31 (1.01–1.71) 0.044 |
Note. Missing data on non-outcome measures modeled using missing data indicators. Adjusted odds ratios for missing data indicators not shown. Unweighted n intoxication 1,755; sustained high 1,736; binge drinking 3,501; high-intensity drinking 1,739.
Ever drunk or very high from drinking in past 30 days
Usually stay drunk or high for 3 or more hours when drinking.
Having 5 or more drinks in a row on at least one occasion in the past two weeks.
Having 10 or more drinks in a row on at least one occasion in the past two weeks.
Unadjusted percentage of cases in each specified covariate category that reported the specific outcome.
AOR = Adjusted odds ratio obtained from models simultaneously including all listed covariates as well as cohort using categorical groupings of 1997–1998, 1999–2001, 2002–2004, and 2005–2007.
CI = Confidence interval.
Combined estimates for Blacks, Hispanics, and other.
Gender
No significant gender differences were observed for sustained high. In contrast, males were significantly more likely than females to report intoxication, binge drinking, and high-intensity drinking.
Race/ethnicity
White respondents were significantly more likely than Black respondents to report intoxication, sustained high, and binge drinking. Whites and Hispanics reported statistically similar rates of intoxication, sustained high, and binge drinking. Whites were more likely than respondents who did not identify as either Black or Hispanic to report intoxication and binge drinking. For high-intensity drinking, all non-White respondents were collapsed into a single group due to very low reported prevalence; Whites had greater odds of consuming 10+ drinks.
Parent education
Higher parental education was not significantly associated with sustained high, binge drinking, or high-intensity drinking, but was associated with higher odds of intoxication.
Alcohol use initiation
The odds of intoxication, sustained high, and binge drinking were statistically similar when comparing those who first used alcohol during versus prior to high school (i.e., grades 9–12 vs. 8 or below). Compared to those who first drank alcohol during high school, those who first used prior to high school had significantly higher odds of reporting high-intensity drinking. High school abstainers had significantly lower odds of all high-risk alcohol use outcomes than individuals who first used alcohol during high school.
Age 25/26 substance use
Past 12-month use of illicit drugs other than marijuana or past 30-day cigarette or marijuana use was associated with significantly higher odds of all high-risk alcohol use outcomes.
Social roles
Being married was associated with significantly lower odds of all high-risk alcohol use outcomes. Having children was associated with lower odds of all outcomes other than sustained high. Having paid work was associated only with higher odds of binge or high-intensity drinking. Having graduated from a 4-year college was associated with significantly higher odds of intoxication, binge, and high-intensity drinking.
DISCUSSION
Among US young adults undergoing the transition from the initial stages of early adulthood into building and maintaining an initial structure of adult life, alcohol use was normative. More than one-third reported intoxication and/or binge drinking, approximately one-quarter reported sustained high, and more than one in ten reported high-intensity drinking. Thus, among the three-quarters of the sample who reported past 30-day alcohol use, roughly one-half reported binge drinking in the past two weeks. Of those reporting any binge drinking, more than one-third reported engaging in high-intensity drinking. Half of all binge drinkers reported usually experiencing a sustained high whenever they drank alcohol. These results support calls for increased attention to the issue of high-intensity drinking.4, 5 The observed alcohol use prevalence rates at age 25/26 remained statistically stable across the cohorts examined, in contrast to significant decreases in several use measures observed over historical time among these respondents during late adolescence. Characteristics associated with particularly high-risk drinking included being male, White, unmarried, employed, a non-parent, and an alcohol user before finishing high school
Individuals aged 25/26 are in a unique period of young adulthood. The initial transition out of adolescence is completed, but they are not yet fully established in adulthood. Many of those pursuing post-secondary education have completed a certificate, associate’s or bachelor’s degree37, 38 but have not yet fully established employment paths. A growing number are moving toward marriage and/or parenthood (with approximately one-quarter of the current sample in at least one of those roles). By the end of adulthood, about half will marry, and about three-quarters will have children.39, 40 It is a period of significant change and transition that, based on the findings of the current study, is frequently accompanied by high-risk alcohol use behaviors that are associated with acute and long-term risks. Similar to published findings for young adults overall,30 high-risk alcohol use behaviors were especially likely for those who were not married, were not parents, had at least some paid employment, and had graduated from a 4-year college.
The prevalence levels of all alcohol use behaviors at age 25/26 were stable over the decade examined (2005–2014). Such stability is in contrast to significant declines in alcohol use observed among these same individuals when they were high school seniors. In other words, the decreasing levels of alcohol use over time observed when these respondents were age 18 (1997–2007) have not persisted to age 25/26 (2005–2014). These findings are in line with prior research showing a decreasing rate of alcohol use at age 18,9, 22, 23 followed by an acceleration in the rate of drinking (at least binge drinking) in early young adulthood.23, 24 The current study demonstrates historically stable levels of use at age of 25/26. Concerted advocacy, intervention, and policy efforts have helped lower adolescent alcohol consumption.41, 42 These reductions in alcohol use—including high-risk use—have not persisted to the second major transition in young adulthood. Historical variation in social role acquisition (delayed marriage, parenthood, and employment) has been associated with increased acceleration in alcohol use in early young adulthood.24 However, there have also been other important shifts over time, including an industry effort to reinforce drinking as a social norm and meet desires for new, innovative packaging and flavor profiles.43 There also has been dramatic growth in the exposure of young adults to alcohol marketing and other alcohol-related content on social media,44 which may affect both perceived social norms of alcohol use as well as individual use intentions.45 Both broad population-based and targeted media efforts are needed to counteract the social “culture of intoxication” that encourages high-risk alcohol use.44, 46
In the face of high-risk alcohol use that has been stable across time, the highest rates of AUD in adulthood,3 and decreases in discussing alcohol use with health professionals,25 improved screening and intervention programs for young adults in their mid-twenties also clearly are needed. Alcohol-related consequences include significant short- and long-term health risks to individual users47 as well as risks to the public including interpersonal violence, vandalism, motor vehicle crashes, and fetal alcohol syndrome.48, 49 The US Preventive Services Task Force50 recommends that clinicians screen all adults aged 18 and older for both risky or hazardous alcohol use as well as AUDs. Young adults often do not self-identify as having alcohol problems, and thus proactive screening is needed.51 Given that the Affordable Care Act now extends coverage for individuals covered under a parent’s policy until they turn 26, there may be an increased opportunity for primary care clinicians to proactively screen young adults into their mid-twenties. In addition, there is a call for clinicians to become more actively involved in screening in a range of locations, including hospital emergency rooms and workplaces.51
To help inform prevention and screening efforts among young adults in their mid-twenties, this study provides information on demographic, substance use, and adult social role characteristics associated with high-risk alcohol use. Similar to previous research on gender differences in alcohol use,10, 27, 28, 52 men were more likely to report most high-risk alcohol use behaviors. However, we did not find significant differences between men and women on sustained high. Observed racial/ethnic differences in age 25/26 alcohol use were similar to research reporting on binge drinking among adults overall,26–28 in that Whites and Hispanics had similar rates of most alcohol use outcomes, while Blacks reported significantly lower rates for most outcomes. In prior studies, parental education showed a complex relationship with high-risk drinking behaviors. Among high school seniors, associations with higher parental education moved from significantly higher odds of binge drinking, to no association with high-intensity drinking, to lower odds of having 15+ drinks in a row.21 Among early young adults, higher parental education was found to be associated with significantly higher odds of binge drinking on 12 or more occasions per year in bivariate models, but after including covariates, only those with the highest levels of parental education (postgraduate studies) continued to have higher odds.53 In the current study, higher parental education was significantly associated only with increased odds of intoxication at age 25/26. Thus, parental education does not appear to be a consistent predictor of a range of high-risk drinking behaviors during the mid-twenties, but some associations do persist.
The current study’s findings related to alcohol initiation and other substance use also are important. Initiating alcohol use prior to high school (vs. during) was associated with increased risk for high-intensity drinking, as shown in previous research.31 Yet, initiation during high school (vs. being a high school abstainer) was also associated with increased risk for all alcohol outcomes examined. Delaying alcohol use initiation until after high school may be protective against all forms of alcohol use, including high-risk use behaviors, at age 25/26. The current study’s findings extend prior research among college students9, 32, 33 indicating that the risk of high-risk alcohol use behaviors at age 25/26 is higher for individuals reporting concurrent use of cigarettes, marijuana, or illicit drugs.
Limitations
These findings must be considered within their limitations. The sample was based on 12th-grade students; as a result, high school drop-outs were not included (those who drop out of high school may have a lower prevalence of high-risk drinking behaviors, but a higher frequency of participation if any use is reported26–28). In addition, attrition between ages 18 and 25/26 raises the possibility of bias in prevalence estimates of age 25/26 high-risk alcohol use. Sensitivity analyses (not shown) examined baseline characteristics associated with attrition. Respondents lost to follow-up were more likely to be male; Black or Hispanic (vs. White); in a home where no parent had a college education; to have initiated alcohol use prior to finishing high school; and to have been members of more recent cohorts. Given that the current study found few differences in high-risk alcohol use by either parental education or cohort, attrition associated with these characteristics is not likely to substantively affect the reported results. Greater attrition among Blacks (with lower alcohol use rates compared to Whites) may somewhat increase prevalence estimates. However, greater attrition among males and those initiating alcohol use prior to finishing high school (groups with high alcohol use) and Hispanics (with alcohol use rates equivalent to Whites) may lead to under-estimates of overall age 25/26 high-risk drinking. While use of attrition weights resulted in recapturing baseline sample distributions, the actual prevalence of high-risk drinking among age 25/26 young adults may be underestimated to some degree. A further limitation is that binge and high-intensity drinking were assessed with the same items for men and women, rather than gender-specific cut-offs that help to account for differences in body size and alcohol metabolism. There is also a need for future research examining associations between high-risk alcohol use among this population and comorbidities (such as ADHD and other mental health issues) and additional social roles (such as military personnel). These limitations notwithstanding, the current analyses provide previously missing data on a range of high-risk alcohol behaviors in a national sample of young adults undergoing the second major transition in young adulthood.
Conclusions
Among US young adults aged 25/26, alcohol use was normative and included significant participation in high-risk drinking. The decreasing levels of alcohol use observed among this sample at age 18 did not persist when these same individuals entered their mid-twenties. Intervention approaches developed specifically to reach young adults in their mid-twenties clearly are needed that counteract social norms encouraging intoxication, as well as efforts to increase proactive screening by clinicians to identify individuals engaged in high-risk drinking behaviors.
Supplementary Material
Acknowledgments
Development of this manuscript was supported by research grant R01AA023504 (to M. Patrick) from the National Institute on Alcohol Abuse and Alcoholism. Data collection was supported by research grants R01DA001411 and R01DA016575 (to L. Johnston) from the National Institute on Drug Abuse. The study sponsors had no role in the study design, collection, analysis or interpretation of the data, writing of the manuscript, or the decision to submit the paper for publication. The content is solely the responsibility of the authors and does not necessarily represent the official views of the study sponsor.
Footnotes
The authors declare that they have no conflicts of interest.
AUTHOR CONTRIBUTIONS
Ms. Terry-McElrath and Dr. Patrick contributed equally to this manuscript with respect to concept, interpretation of data, and the write-up of results. Ms. Terry-McElrath conducted the analysis.
REFERENCES
- 1.Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2224–2260. doi: 10.1016/S0140-6736(12)61766-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Alcohol and Public Health: Alcohol-Related Disease Impact. [Accessed September 12, 2015];Centers for Disease Control and Prevention (CDC) website. http://nccd.cdc.gov/DPH_ARDI/default/default.aspx.
- 3.Grant BF, Goldstein RB, Saha TD, et al. Epidemiology of DSM-5 alcohol use disorder: results from the National Epidemiologic Survey on Alcohol and Related Conditions III. JAMA Psychiatry. 2015;72(8):757–766. doi: 10.1001/jamapsychiatry.2015.0584. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Patrick ME. A call for research on high-intensity alcohol use. Alcohol Clin Exp Res. 2016;40(2):256–259. doi: 10.1111/acer.12945. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Hingson RW, White A. Trends in extreme binge drinking among US high school seniors. JAMA Pediatr. 2013;167(11):996–998. doi: 10.1001/jamapediatrics.2013.3083. [DOI] [PubMed] [Google Scholar]
- 6.Naimi TS, Nelson DE, Brewer RD. The intensity of binge alcohol consumption among US adults. Am J Prev Med. 2010;38(2):201–207. doi: 10.1016/j.amepre.2009.09.039. [DOI] [PubMed] [Google Scholar]
- 7.Chen K, Kandel DB. The natural history of drug use from adolescence to the mid-thirties in a general population sample. Am J Public Health. 1995;85(1):41–47. doi: 10.2105/ajph.85.1.41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Johnston LD, O'Malley PM, Bachman JG, Schulenberg JE, Miech RA. Monitoring the Future National Survey Results on Drug Use, 1975–2014: Volume II, College Students and Adults Ages 19–55. Ann Arbor: Institute for Social Research, The University of Michigan; 2015. [Accessed September 11, 2015]. http://www.monitoringthefuture.org/pubs/monographs/mtf-vol2_2014.pdf. [Google Scholar]
- 9.Substance Abuse and Mental Health Services Administration. Results from the 2013 National Survey on Drug Use and Health: Summary of National Findings, NSDUH Series H-48, HHS Publication No. (SMA) 14-4863. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2014. [Accessed September 12, 2015]. http://www.samhsa.gov/data/sites/default/files/NSDUHresultsPDFWHTML2013/Web/NSDUHresults2013.htm#3.1.9. [Google Scholar]
- 10.Esser MB, Hedden SL, Kanny D, Brewer RD, Gfroerer JC, Naimi TS. Prevalence of alcohol dependence among US adult drinkers, 2009–2011. Prev Chronic Dis. 2014;11(E206):1–11. doi: 10.5888/pcd11.140329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Wechsler H, Dowdall GW, Davenport A, Castillo S. Correlates of college student binge drinking. Am J Public Health. 1995;85(7):921–926. doi: 10.2105/ajph.85.7.921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Wechsler H, Nelson TF. What we have learned from the Harvard School of Public Health College Alcohol Study: focusing attention on college student alcohol consumption and the environmental conditions that promote it. J Stud Alcohol Drugs. 2008;69(4):481–490. doi: 10.15288/jsad.2008.69.481. [DOI] [PubMed] [Google Scholar]
- 13.Hingson RW, Heeren T, Zakocs RC, Kipstein A, Wechsler H. Magnitude of alcohol-related mortality and morbidity among US college students ages 18–24. J Stud Alcohol. 2002;63(2):136–144. doi: 10.15288/jsa.2002.63.136. [DOI] [PubMed] [Google Scholar]
- 14.Perkins HW. Surveying the damage: a review of research on consequences of alcohol misuse in college populations. J Stud Alcohol. 2002;S14:91–100. doi: 10.15288/jsas.2002.s14.91. [DOI] [PubMed] [Google Scholar]
- 15.Levinson DJ. A conception of adult development. Am Psychol. 1986;41(1):3–13. [Google Scholar]
- 16.Levinson DJ. The Seasons of a Man’s Life. New York: Ballantine Books; 1978. [Google Scholar]
- 17.Erikson EH. Childhood and Society. New York: W.W. Norton & Company, Inc.; 1950, 1963. [Google Scholar]
- 18.AMA Council on Science and Public Health. [Accessed February 10, 2016];Summary: Report 11 of the Council on Scientific Affairs (A-03): Effects of Alcohol on the Brains of Underage Drinkers; 2003. file:///Z:/exbinge/age2526/lit/a03csa11-summary.pdf.
- 19.Sowell ER, Thompson PM, Holmes CJ, Jernigan TL, Toga AW. In vivo evidence for post-adolescent brain maturation in frontal and striatal regions. Nat Neurosci. 1999;2(10):859–861. doi: 10.1038/13154. [DOI] [PubMed] [Google Scholar]
- 20.Sowell ER, Peterson BS, Thompson PM, Welcome SE, Henkenius AL, Toga AW. Mapping cortical change across the human life span. Nat Neurosci. 2003;6(3):309–315. doi: 10.1038/nn1008. [DOI] [PubMed] [Google Scholar]
- 21.Patrick ME, Schulenberg JE, Martz ME, Maggs JL, O'Malley PM, Johnston LD. Extreme binge drinking among 12th-grade students in the United States: prevalence and predictors. JAMA Pediatr. 2013;167(11):1019–1025. doi: 10.1001/jamapediatrics.2013.2392. (2013) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Miech RA, Johnston LD, O'Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future National Survey Results on Drug Use 1975–2014: Volume I, Secondary School Students. Ann Arbor: Institute for Social Research, The University of Michigan; 2015. [Accessed September 11, 2015]. http://www.monitoringthefuture.org/pubs/monographs/mtf-vol1_2014.pdf. [Google Scholar]
- 23.Jager J, Schulenberg JE, O’Malley PM, Bachman JG. Historical variation in drug use trajectories across the transition to adulthood: the trend toward lower intercepts and steeper, ascending slopes. Dev Psychopathol. 2013;25:527–543. doi: 10.1017/S0954579412001228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Jager J, Keyes KM, Schulenberg JE. Historical variation in young adult binge drinking trajectories and its link to historical variation in social roles and minimum legal drinking age. Dev Psychol. 2015;51(7):962–974. doi: 10.1037/dev0000022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.McKnight-Eily LR, Liu Y, Brewer RD, et al. Vital signs: communication between health professionals and their patients about alcohol use—44 states and the District of Columbia, 2011. Morb Mortal Wkly Rep. 2014;63(1):16–22. [PMC free article] [PubMed] [Google Scholar]
- 26.Naimi TS, Brewer RD, Mokdad A, Denny C, Serdula MK, Marks JS. Binge drinking among US adults. JAMA. 2003;289(1):70–75. doi: 10.1001/jama.289.1.70. [DOI] [PubMed] [Google Scholar]
- 27.Kanny D, Liu Y, Brewer RD, Garvin WE, Balluz L. Vital signs: binge drinking prevalence, frequency, and intensity among adults—United States, 2010. Morb Mortal Wkly Rep. 2012;61(1):14–19. [PubMed] [Google Scholar]
- 28.Kanny D, Liu Y, Brewer RD, Lu H. Binge drinking—United States, 2011. Morb Mortal Wkly Rep. 2013;62(3):77–80. [PubMed] [Google Scholar]
- 29.Marchetta CM, Denny CH, Floyd RL, Cheal NE, Sniezek JE, McKnight_Eily LR . Alcohol use and binge drinking among women of childbearing age—United States, 2006–2010. Morb Mortal Wkly Rep. 2012;61(28):534–538. [PubMed] [Google Scholar]
- 30.Bachman JG, Wadsworth KN, O’Malley PM, Johnston LD, Schulenberg JE. Smoking, Drinking, and Drug Use in Young Adulthood: The Impact of New Freedoms and New Responsibilities. Mahwah, NJ: Lawrence Erlbaum; 1997. [Google Scholar]
- 31.Grant B, Dawson DA. Age of alcohol onset and its association with DSM-IV alcohol abuse and dependence: results from the National Longitudinal Alcohol Epidemiologic Survey. J Subst Abuse. 1997;9:103–110. doi: 10.1016/s0899-3289(97)90009-2. [DOI] [PubMed] [Google Scholar]
- 32.Keith DR, Hart CL, McNeil MP, Silver R, Goodwin RD. Frequent marijuana use, binge drinking and mental health problems among undergraduates. Am J Addict. 2015;24(6):499–506. doi: 10.1111/ajad.12201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Weitzman ER, Chen Y-Y. The co-occurrence of smoking and drinking among young adults in college: national survey results from the United States. Drug Alcohol Depend. 2005;80(3):377–386. doi: 10.1016/j.drugalcdep.2005.05.008. [DOI] [PubMed] [Google Scholar]
- 34.Bachman JG, Johnston LD, O'Malley PM, Schulenberg JE, Miech RA. The Monitoring the Future Project after Four Decades: Design and Procedures (Monitoring the Future Occasional Paper No. 82) Ann Arbor, MI: Institute for Social Research, University of Michigan; 2015. [Accessed September 11, 2015]. (2015). http://www.monitoringthefuture.org/pubs/occpapers/mtf-occ82.pdf. [Google Scholar]
- 35.Kim HJ, Fay MP, Feuer EJ, Midthune DN. Permutation tests for joinpoint regression with applications to cancer rates. Stat Med. 2000;19(3):335–351. doi: 10.1002/(sici)1097-0258(20000215)19:3<335::aid-sim336>3.0.co;2-z. (correction: 2001;20(4):655) [DOI] [PubMed] [Google Scholar]
- 36.National Cancer Institute (NCI) Joinpoint Regression Program, Version 4.0.1. Bethesda: Statistical Research and Applications Branch, National Cancer Institute; 2013. [Google Scholar]
- 37.Cataldi EF, Green C, Henke R, et al. 2008–09 Baccalaureate and Beyond Longitudinal Study (B&B:08/09): first look (NCES 2011-236) Washington, DC: US Department of Education, National Center for Education Statistics; 2011. [Accessed September 10, 2015]. http://nces.ed.gov/pubsearch. [Google Scholar]
- 38.Characteristics of Certificate Completers with Their Time to Certificate and Labor Market Outcomes. [Accessed September 10, 2015];US Department of Education website. http://nces.ed.gov/pubs2013/2013157.pdf.
- 39.Cohn D, Passel JS, Wang W, Livingston G. [Accessed September 10, 2015];Barely Half of US Adults are Married—A Record Low. Pew Research Center website. http://www.pewsocialtrends.org/2011/12/14/barely-half-of-u-s-adults-are-married-a-record-low/
- 40.Newport F, Wilke J. Desire for Children Still Norm in US: US Birthrate Down, but Attitudes Toward Having Children Unchanged. [Accessed September 11, 2015];GALLUP Politics website. http://www.gallup.com/poll/164618/desire-children-norm.aspx.
- 41.Bonnie RJ, O’Connell ME, editors. Reducing Underage Drinking: A Collective Responsibility. Washington, DC: The National Academies Press; 2004. [PubMed] [Google Scholar]
- 42.National Institute on Alcohol Abuse and Alcoholism. Underage drinking: why do adolescents drink, what are the risks, and how can underage drinking be prevented? Alcohol Alert. 2006;67:1–7. [Google Scholar]
- 43.Fromm J, Swartz L. Five marketing lessons for brands in the adult beverage category. [Accessed November 3, 2015];Forbes. 2014 Oct 28; http://www.forbes.com/sites/jefffromm/2014/10/28/five-marketing-lessons-for-brands-in-the-adult-beverage-category/ [Google Scholar]
- 44.Moreno MA, Whitehill JM. Influence of social media on alcohol use in adolescents and young adults. Alcohol Res-Curr Rev. 2014;36(1):91–100. [PMC free article] [PubMed] [Google Scholar]
- 45.Alhabash S, McAlister AR, Quilliam ET, Richards JI, Lou C. Alcohol’s getting a bit more social: when alcohol marketing messages on Facebook increase young adults’ intentions to imbibe. Mass Commun Soc. 2015;18(3):350–375. [Google Scholar]
- 46.Szmigin I, Bengry-Howell A, Griffin C, Hackley C, Mistral W. Social marketing, individual responsibility and the “culture of intoxication”. Eur J Marketing. 2011;45(5):759–779. [Google Scholar]
- 47. [Accessed September 11, 2015];Fact Sheets: Alcohol Use and Your Health. Centers for Disease Control and Prevention (CDC) website. http://www.cdc.gov/alcohol/fact-sheets/alcohol-use.htm.
- 48.Town M, Naimi TS, Mokdad AH, Brewer RD. Health care access among US adults who drink alcohol excessively: missed opportunities for prevention. Prev Chronic Dis. 2006;3(2):1–8. [PMC free article] [PubMed] [Google Scholar]
- 49.Wechsler H, Lee JE, Hall J, Wagenaar AC, Lee H. Secondhand effects of student alcohol use reported by neighbors of colleges: the role of alcohol outlets. Soc Sci Med. 2002;55(3):425–435. doi: 10.1016/s0277-9536(01)00259-3. [DOI] [PubMed] [Google Scholar]
- 50. [Accessed September 10, 2015];Final Recommendation Statement -- Alcohol Misuse: Screening and Behavioral Counseling Interventions in Primary Care, May 2013. US Preventive Services Task Force website. doi: 10.7326/0003-4819-159-3-201308060-00652. http://www.uspreventiveservicestaskforce.org/Page/Document/RecommendationStatementFinal/alcohol-misuse-screening-and-behavioral-counseling-interventions-in-primary-care. [DOI] [PubMed]
- 51.Monti PM, O’Leary Tevyaw T, Borsari B. Drinking among young adults: screening, brief intervention, and outcome. Alcohol Res Health. 2004/2005;28(4):236–244. [Google Scholar]
- 52.Wilsnack RW, Wilsnack SC. International gender and alcohol research: Recent findings and future directions. Alcohol Res Health. 2002;26(4):245–250. [PMC free article] [PubMed] [Google Scholar]
- 53.Patrick ME, Wightman P, Schoeni RF, Schulenberg JE. Socioeconomic status and substance use among young adults: a comparison across constructs and drugs. J Stud Alcohol Drugs. 2012;73(5):772–782. doi: 10.15288/jsad.2012.73.772. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.