

Abstract
A 42-year-old male patient complaint with missing right eye was referred to the Department of Prosthodontics and Crown and Bridge. This patient was seeking artificial eye replacement. On careful clinical examination, a defect with a shrunken orbit and intact tissue bed was found in the patient. As the patient was economically very poor, modified stock ocular prosthesis was advised. To rehabilitate this ocular defect, “single” appointment technique with clinically available material was adopted, which is discussed in the present communication.
Keywords: Ocular defect, ocular prosthesis, rehabilitation, single appointment technique
INTRODUCTION
Eyes are generally the first features of the face to be noticed, playing a significant role in our daily lives.[1] The most grievous yet, unfortunately, the most commonly occurring loss out of all sensory organs is that of an eye, hence, not until one of them is partially or totally lost, its real value is never fully obliged. Such an adversity may have a prodigious emotional and psychological impact on the patient with loss of function.[2,3]
The loss or absence of an eye can be due to any reason as mentioned-congenital defect, irreparable trauma, tumor, a blind painful eye, the need for histological confirmation of a suspected diagnosis, the possible prevention of sympathetic ophthalmia and cosmetic reasons may necessitate surgical intervention resulting in removal of the eyeball.[1,4] Depending on the severity of the situation, there are 3 types of surgical management: Evisceration, enucleation, and exenteration. The ocular prosthesis can be given to patient who has lost ocular structures through evisceration or enucleation.[4,5] Basically, there are 3 types of acrylic resin ocular prosthesis: (i) Custom-fitted ocular prosthesis made from an impression of the socket, (ii) stock (prefabricated) ocular prosthesis and (iii) stock ocular prosthesis modified by various methods.[6,7]
In general, after completion of surgery, surgical wound is closed and a clear concave plastic conformer is placed beneath the eyelids, onto the conjunctiva, and over the orbital implant, if it is placed, which minimizes the changes in the socket size and conformation and prevents scar tissue contractures from distorting the socket bed during tissue healing.[8,9] The definitive ocular prosthesis can be initiated 10–14 days following surgery.[10,11]
Hence, removal of an eye followed by management of the anophthalmic socket may require combined efforts of the ophthalmologist and the maxillofacial prosthodontist with the aim to improve the patient's esthetics, restore and maintain the health of the remaining structures, and consequently provide physical and mental well-being.[6,12]
Various techniques for processing an ocular prosthesis have been mentioned in the past which are either time consuming, cost effective or complicated and that requires dentist good skill and time as well as patient's time. Therefore, this article explores a simplified “single” appointment technique employed for fabrication of ocular prosthesis by customizing stock ocular prosthesis, achieving ideal fit and esthetics.
CASE REPORT
A 42-year-old male patient was referred to the Department of Prosthodontics and Crown and Bridge, Mahatma Gandhi Dental College and Hospital, Sitapura, Jaipur, India. The patient complained of missing right eye which was enucleated following an accidental traumatic injury [Figure 1]. Consequent to this, patient worded dark glasses specs for almost 1 year but at the same time, he was suffering from severe emotional trauma in terms of facial esthetics and social acceptance. Hence, the patient was seeking artificial eye replacement. On examination, defect with a shrunken orbit and intact tissue bed were observed. As the patient was economically very poor, the modified stock ocular prosthesis was advised. The treatment procedure and its limitations were explained to the patient to allay apprehension and elicit cooperation.
Figure 1.

Patient with right ocular defect
Preliminary preparations
A transparent, vesseled stock eye was selected with a close resemblance of the iris of the stock ocular prosthesis with that of the natural eye using both daylight and artificial light.
An ophthalmic socket was anesthetized with topical anesthetic followed by light lubrication of same side eyebrow and eyelashes to make the procedure more comfortable.
A customized impression tray with injector was fabricated by joining hub of 10 ml syringe with perforated head of disposable plastic spoon using an adhesive. Later customizing and smoothening of corners of perforated head part according to the dimensions of anopthalmic socket of defect side was done [Figure 2].
Figure 2.
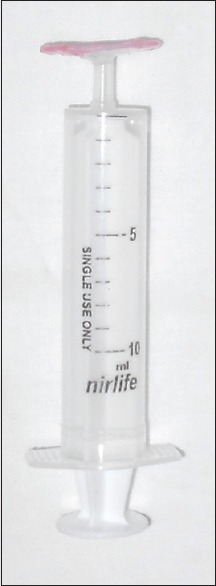
Customized impression tray with injector
Procedure
The primary impression of an ophthalmic socket was made using customized injector, by injecting the light viscosity addition elastomeric impression material (Virtual, Light body, Ivoclar Vivadent, India) slowly (to avoid any air bubbles), first into the depth below the upper eyelid and then into the lower. The patient was instructed to close his eye so that the excess material could flow out through perforations in the trays. While the material sets, instructions were given to the patient to do various eye movements in following order-moving eye laterally, followed by up and down motion and finally in a circular motion
After the impression material had set, it was carefully removed from the anophthalmic socket
The impression was checked to ensure that all the surfaces are recorded and there is no porosity present. This was followed by beading and boxing (Beading and Boxing wax, MP Sai Enterprises, India) of impression [Figure 3]. Investing with Type IV dental stone (Kalrock, Kalabhai, India) was done to obtain a primary cast
Customization of the stock ocular prosthesis was done by selectively grinding and making it 2 mm short all around the margins of primary cast
-
Border molding and secondary impression of the patient's anopthalmic socket was made by modified wax (sticky wax and utility wax in the ratio of 1:2). The objective was to obtain complete peripheral contact and proper curvature [Figures 4]
Centralization of the iris was checked by asking the patient to look straight ahead to a distant object, keeping in mind the symmetry with the iris of the adjacent unaffected left natural eye of the patient
-
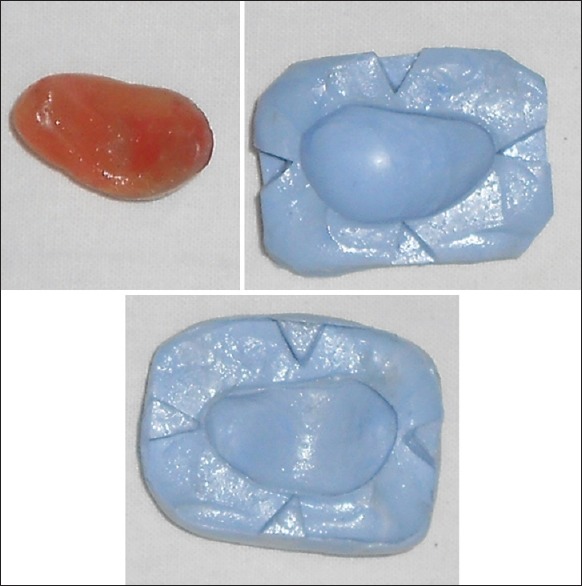
Now this wax modified stock ocular prosthesis was removed gently from the anophthalmic socket and was used to make sectional putty (Aquasil, Soft putty, Dentsply India Pvt. Ltd.) indexed mold (indexing of the first section was done so as to allow correct orientation of the second half of the mold) using putty viscosity addition elastomeric impression material [Figure 5]. This mold was used later for processing of definitive ocular prosthesis
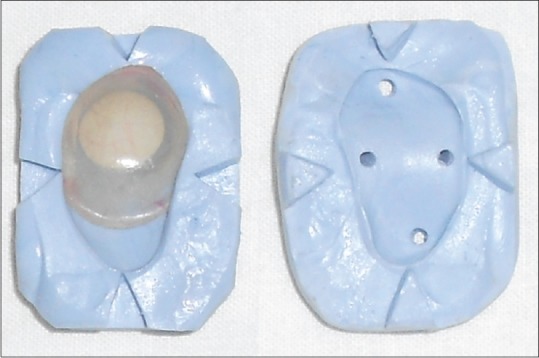
After the putty material had set, the two halves of putty mold were separated and the wax modified stock ocular prosthesis was retrieved so as to keep the mold space ready for processing of definitive ocular prosthesis [Figures 6]. Holes were made on second half of the mold to release excess resin to flow out
The Modified wax was completely removed from the wax modified stock ocular prosthesis, which was followed by placing back of same ocular prosthesis into the first half of the sectional putty indexed mold in such a manner that inner surface faces upward [Figure 7]. Proportioning of clear and tooth colored auto-polymerizing methyl methacrylate resin (Dental Product of India (DPI), self-cure tooth molding powder and liquid, India) of appropriate shade was done in such a manner that resultant mixer matches with the color of the sclera of the unaffected eye of the patient. This resultant mixer was poured over the inner surface of wax modified stock ocular prosthesis [Figure 8]. Final packing was completed by tightening of second putty mold over the first mold. Excess material flows out through holes prepared and were removed. Acrylization was done by keeping sectional putty indexed mold into pressure pot at 30 psi for 20 min for complete polymerization, preventing any excess unreacted monomer, essential to prevent any untoward irritation or sensitivity and thereby a rejection of the prosthesis by the patient. This also enables the minimization of porosities and gives a good finish to the prosthesis as the eye socket is extremely sensitive and the residual conjunctiva and related structures react to any surface roughness and irregularities
After complete acrylization, sectional putty indexed mold were opened and definitive ocular prosthesis retrieved [Figure 9]. The prosthesis was inspected for imperfections. Finishing and polishing were done to get a glass like finish to achieve maximum adaptation and overall success of the prosthesis [Figure 10]. The ocular prosthesis was washed with warm water and soap and inserted into the patient's anophthalamic socket and evaluated critically for lid drape, contour, and dimension
Figure 3.

Impression followed by beading and boxing
Figure 4.
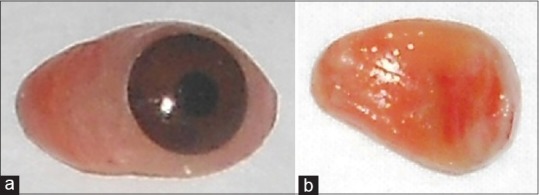
(a) Outer surface of wax modified stock ocular prosthesis. (b) Inner surface of wax modified stock ocular prosthesis
Figure 5.

Sectional putty indexed mold
Figure 6.
Retrieval of wax modified stock ocular prosthesis from sectional putty indexed mold
Figure 7.
Wax modified stock ocular prosthesis after removal of modified wax
Figure 8.

Packing of wax modified stock ocular prosthesis with resin
Figure 9.

Definitive ocular prosthesis
Figure 10.

Patient with definitive ocular prosthesis
The final outcome of the prosthesis was ascertained from the satisfied look on the face of the patient and from the follow-up a week later. Instructions regarding ocular prosthesis were given as follow:
Careful handling of the prosthesis with clean hands
Removal of the prosthesis once a day, if necessary, and to wash it under warm water with a soft clean cloth and mild soap
Cautioned to keep the eye moist by placing it in water if it's not in the anophthalmic socket, and never to allow it to come in contact with alcohol, or solvent of any kind
Examination of anophthalmic socket once in a year or instantly when there is any irritation
To improve the movement of the eyelids and the sparkle and sheen of the prosthesis, its beneficiary to use silicone base lubricant or mineral oil or safflower oil.[13,14,15]
DISCUSSION
Ocular defects constitute an important maxillofacial defect, which requires prosthetic replacement.[10,16] In the absence or loss of an eye, the prosthodontist is a person who comes into an act of providing the patient with an artificial eye to overcome the agony of losing an eye.[1,17]
One of the pioneers of the modern artificial eye was Ambroise Pare, a Frenchman (1510–1590). In 1575, Pare fabricated artificial eyes made of glass as well as porcelain. During the two world wars, the supply of glass eyes from Germany to the United States was halted, and in 1943 the United States Army and Navy both undertook research to find a substitute. Attention was concentrated on plastics, and the development of an acrylic eye resulted. By 1945, the Army had 30 installations in operation, and thousands of artificial acrylic eyes were being produced. Today the vast majority of patients all around the world wear ocular prosthesis made of acrylic.[5,18]
Although customized ocular prosthesis has proved to be the most satisfactory ocular replacement this also necessitates the service of a skilled artist for duplication of the iris and sclera and has an involved cost and time-consuming procedure. But with the advances in dentistry, the customized stock acrylic resin ocular prosthesis has presented with almost equivalent results like customized ocular prosthesis with following advantages: (1) The adaptation may be accomplished without the aid of an artist or person skilled in the art of iridal and sclera painting, (2) the prosthesis may be fabricated rapidly and positioned to serve the patient as a comfortable and esthetic prosthesis while he is waiting for his custom built ocular prosthesis, (3) the prosthesis may be constructed with materials and equipment normally found in any dental office and laboratory, with the exception of the stock eye, and (4) the prosthesis may be used as a conformer or stent immediately postoperatively to aid in the re-growth and orientation of the tissues in the surgical area.[15,18]
A stock ocular prosthesis comes in standard sizes, shapes and colors.[15] With the development of newer materials and techniques, the anophthalmic socket can be finely recorded, by which stock ocular prosthesis can be modified, and final ocular prosthesis can be fabricated with exact fit and esthetics. Hence numerous techniques for processing an ocular prosthesis exist.[4,5,6,8,9,15,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32] Mathews et al. have reviewed the literature concerning such ocular impression and fitting techniques.[4,33]
The technique for fabricating ocular prosthesis described in present case report is a combination of various techniques described in the literature, but yet it is “simple,” “safe,” requiring “single appointment.” In this technique, modified wax which was used for border molding and the secondary impression has been used as an alternative to other impression materials because of advantages of giving sufficient time for recording borders and making an impression, ease of availability, and remoldablility. This makes technique of customizing stock ocular prosthesis faster and easier. However, this material was used for the 1st time may require further study.
During processing sectional putty indexed mold (made up of putty viscosity addition silicone) and a proportionate amount of clear and tooth colored auto-polymerizing methyl methacrylate resin of appropriate shade were used because of their easy availability in a clinical setup.
Hence, the method described here is simple, undemanding and can be carried out in a very short period, providing good results from patient esthetic, acceptance, and satisfaction point of view.
Subjective errors can occur while checking for centralization of the iris of the ocular prosthesis, which is a limitation of the procedure described here; however, there may be a scope for other prosthodontists to verify the reliability of this procedure by comparing with other techniques.
CONCLUSION
Ideas and techniques have changed and experience has accumulated in the field of dentistry. It is important that the dental profession and especially those practicing maxillofacial prosthetics keep their current knowledge. The method described here is undemanding and can be carried out in a small clinical set-up, rendering better service to patient with anophthalmic socket defect. The use of modified stock ocular prosthesis has been a boon to the patients who cannot afford implant replacements or custom made ocular prosthesis. Furthermore, the esthetic and functional outcome of the prosthesis was almost similar to that of the custom ocular prosthesis, if proper shade selection of iris and sclera is done. Although the patient cannot see with this prosthesis, it will definitely restored patients self-esteem and allowed him to confidently face the world rather than hiding behind dark glasses.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Doshi PJ, Aruna B. Prosthetic management of patient with ocular defect. J Indian Prosthodont Soc. 2005;5:37–8. [Google Scholar]
- 2.Moore DJ, Ostrowski JS, King LM., Jr A quasi-integrated custom ocular prosthesis. J Prosthet Dent. 1974;32:439–42. doi: 10.1016/0022-3913(74)90355-2. [DOI] [PubMed] [Google Scholar]
- 3.Newton JT, Fiske J, Foote O, Frances C, Loh IM, Radford DR. Preliminary study of the impact of loss of part of the face and its prosthetic restoration. J Prosthet Dent. 1999;82:585–90. doi: 10.1016/s0022-3913(99)70058-2. [DOI] [PubMed] [Google Scholar]
- 4.Kale E, Mese A, Izgi AD. A technique for fabrication of an interim ocular prosthesis. J Prosthodont. 2008;17:654–61. doi: 10.1111/j.1532-849X.2008.00361.x. [DOI] [PubMed] [Google Scholar]
- 5.Beumer J, Curtis TA, Marunick MT. Maxillofacial Rehabilitation: Prosthodontic and Surgical Considerations. 2nd ed. St. Louis: Ishiyaku EuroAmerica; 1996. pp. 422–5. [Google Scholar]
- 6.Bartlett SO, Moore DJ. Ocular prosthesis: A physiologic system. J Prosthet Dent. 1973;29:450–9. doi: 10.1016/s0022-3913(73)80024-1. [DOI] [PubMed] [Google Scholar]
- 7.Moore DJ, Firtell DN. A simplified method of measuring the diameter of the anterior segment of the eye. Am J Ophthalmol. 1969;67:769–70. [PubMed] [Google Scholar]
- 8.Sykes LM, Essop AR, Veres EM. Use of custom-made conformers in the treatment of ocular defects. J Prosthet Dent. 1999;82:362–5. doi: 10.1016/s0022-3913(99)70095-8. [DOI] [PubMed] [Google Scholar]
- 9.Chin K, Margolin CB, Finger PT. Early ocular prosthesis insertion improves quality of life after enucleation. Optometry. 2006;77:71–5. doi: 10.1016/j.optm.2005.12.012. [DOI] [PubMed] [Google Scholar]
- 10.Guttal SS, Patil NP, Vernekar N, Porwal A. A simple method of positioning the iris disk on a custom-made ocular prosthesis. A clinical report. J Prosthodont. 2008;17:223–7. doi: 10.1111/j.1532-849X.2007.00272.x. [DOI] [PubMed] [Google Scholar]
- 11.Rathbun JE, Beard C, Quickert MH. Evaluation of 48 cases of orbital exenteration. Am J Ophthalmol. 1971;72:191–9. doi: 10.1016/0002-9394(71)91613-8. [DOI] [PubMed] [Google Scholar]
- 12.Hooper SM, Westcott T, Evans PL, Bocca AP, Jagger DC. Implant-supported facial prostheses provided by a maxillofacial unit in a U.K. regional hospital: Longevity and patient opinions. J Prosthodont. 2005;14:32–8. doi: 10.1111/j.1532-849X.2005.00004.x. [DOI] [PubMed] [Google Scholar]
- 13.Parr GR, Goldman BM, Rahn AO. Postinsertion care of the ocular prosthesis. J Prosthet Dent. 1983;49:220–4. doi: 10.1016/0022-3913(83)90506-1. [DOI] [PubMed] [Google Scholar]
- 14.Cain JR. Custom ocular prosthetics. J Prosthet Dent. 1982;48:690–4. doi: 10.1016/s0022-3913(82)80030-9. [DOI] [PubMed] [Google Scholar]
- 15.Welden RB, Niiranen JV. Ocular prosthesis. J Prosthet Dent. 1956;6:272–8. [Google Scholar]
- 16.Shivji AR, Bhat S, Shetty P. Prosthodontic management of an ocular defect – A case report. J Indian Prosthodont Soc. 2001;1:33–5. [Google Scholar]
- 17.Laney WR. Maxillofacial Prosthetics. 1st ed. The University of Michigan, PSG Pub. Co; 1979. pp. 279–306. [Google Scholar]
- 18.Chalian VA, Drane JB, Standish SM. Maxillofacial Prosthetics: Multidisciplinary Practice. 1st ed. Baltimore: The Williams & Wilkins Co; 1971. pp. 286–94. [Google Scholar]
- 19.Brown KE. Fabrication of an ocular prosthesis. J Prosthet Dent. 1970;24:225–35. doi: 10.1016/0022-3913(70)90149-6. [DOI] [PubMed] [Google Scholar]
- 20.Murphey PJ, Schlossberg L. Eye replacement by acrylic maxillofacial prosthesis. U S Nav Med Bull. 1944;43:1085–99. [Google Scholar]
- 21.Allen L, Webster HE. Modified impression method of artificial eye fitting. Am J Ophthalmol. 1969;67:189–218. doi: 10.1016/0002-9394(69)93148-1. [DOI] [PubMed] [Google Scholar]
- 22.Maloney BA. Development of impression fitting equipment: A new technique. J Am Soc Ocularists. 1979;9:32–3. [Google Scholar]
- 23.Engelmeier RL. Autoclavable custom-made metal impression trays to improve infection control. J Prosthet Dent. 1987;58:121–2. doi: 10.1016/s0022-3913(87)80156-7. [DOI] [PubMed] [Google Scholar]
- 24.Miller BJ. Custom ocular impression trays. J Facial Somato Prosthet. 1996;2:109–13. [Google Scholar]
- 25.Rahn AO, Boucher LJ. Maxillofacial Prosthetics: Principles and Concepts. 1st ed. Philadelphia, PA: WB Saunders Company; 1970. pp. 164–7. [Google Scholar]
- 26.Taicher S, Steinberg HM, Tubiana I, Sela M. Modified stock-eye ocular prosthesis. J Prosthet Dent. 1985;54:95–8. doi: 10.1016/s0022-3913(85)80079-2. [DOI] [PubMed] [Google Scholar]
- 27.Smith RM. Relining an ocular prosthesis: A case report. J Prosthodont. 1995;4:160–3. doi: 10.1111/j.1532-849x.1995.tb00333.x. [DOI] [PubMed] [Google Scholar]
- 28.Ow RK, Amrith S. Ocular prosthetics: Use of a tissue conditioner material to modify a stock ocular prosthesis. J Prosthet Dent. 1997;78:218–22. doi: 10.1016/s0022-3913(97)70129-x. [DOI] [PubMed] [Google Scholar]
- 29.Benson P. The fitting and fabrication of a custom resin artificial eye. J Prosthet Dent. 1977;38:532–8. doi: 10.1016/0022-3913(77)90029-4. [DOI] [PubMed] [Google Scholar]
- 30.McKinstry RE. Fundamentals of Facial Prosthetics. 1st ed. Arlington, VA: Abi Professional Pubns; 1995. pp. 107–9. [Google Scholar]
- 31.Schneider RL. Modified ocular prosthesis impression technique. J Prosthet Dent. 1986;55:482–5. doi: 10.1016/0022-3913(86)90182-4. [DOI] [PubMed] [Google Scholar]
- 32.Sykes LM. Custom made ocular prostheses: A clinical report. J Prosthet Dent. 1996;75:1–3. doi: 10.1016/s0022-3913(96)90409-6. [DOI] [PubMed] [Google Scholar]
- 33.Mathews MF, Smith RM, Sutton AJ, Hudson R. The ocular impression: A review of the literature and presentation of an alternate technique. J Prosthodont. 2000;9:210–6. doi: 10.1111/j.1532-849x.2000.00210.x. [DOI] [PubMed] [Google Scholar]