

Abstract
Shoulder arthroscopy is traditionally performed with the patient in either the beach chair position or the lateral decubitus position. Each position has its advantages and disadvantages. The main topics for consideration include ease of surgery, view into the surgical field, risks to the patient, and economics of the setup. In the lateral decubitus position, it is inconvenient to work through the anterior portal and it is difficult to convert to an open procedure. In the beach chair position, it is difficult to manage the airway and cerebral oxygenation and the patient's head and the beach chair frame obstruct the insertion of a scope into the superior and posterior portals. This technical note presents the supine position for shoulder arthroscopic surgery. The supine position does not have the disadvantages of the traditional positions. In addition, it is comparatively easy to set up and comfortable for the patient.
Shoulder arthroscopic surgery is traditionally performed in either the beach chair or the lateral decubitus position. Each position offers some advantages, disadvantages, and potential complications. In general, arthroscopic surgeons' preferences for patient positioning have been based on their training.
Shoulder arthroscopy was first introduced with the lateral decubitus position, which allows easier access to the glenohumeral joint space during the shoulder arthroscopic procedure. In the lateral decubitus position, the patient is stable and a static traction is applied in the directions of abduction and flexion of the shoulder. Generally, the arm to be operated is placed in the traction at approximately 25° to 45° abduction and 15° to 30° forward flexion.1, 2 This position is good for exposing the anterior, inferior, and posterior capsules. Both capsulolabral complex and superior lateral anterior posterior lesions can easily be repaired in the lateral position. The patient's head and the operating table do not obstruct access to the anterior and posterior shoulder. Arthroscopic bubbles float away from the subacromial space to the subdeltoid space and therefore do not block the surgeon's view of the operation. The lateral decubitus position has disadvantages such as the necessity to reach forwards and around for the anterior portals, the difficulty in converting to an open procedure, and patients not tolerating isolated regional anesthesia.2 This position requires a device for traction. The traction is associated with brachial plexus injury3, 4 and vascular complications.5, 6
The first report on the use of the beach chair position for arthroscopic shoulder procedures was in 1988 by Skyhar et al.7 The advantages of the beach chair position include presenting the anatomy in the anatomic upright position, minimizing disorientation, and facilitating easy conversion to an open procedure when necessary. With the patient in this position, it is possible to move the arm to be operated to a different position intraoperatively without the arm hanging in the way of the anterior portal.2, 7, 8 The disadvantages of the beach chair position include the need for an assistant or a special device to maintain the position of the arm and to provide traction to expose the subacromial and joint space. The patient's head and the beach chair frame obstruct the insertion of a scope into the superior and posterior portals. Anesthetists prefer not to operate in the sitting position because in this position it is difficult to manage the airway and cerebral oxygenation. In addition, there have been several reports of complications with the use of the beach chair position. Hypotensive and bradycardic conditions have been reported in patients undergoing shoulder arthroscopy in the beach chair position. Pohl and Cullen9 reported on 4 cases of neurovascular complications after both open and arthroscopic procedures were performed with patients in the semiupright position that resulted in the death of one patient and severe brain damage to 3 others. Cerebral ischemia,9, 10, 11, 12, 13 vision loss, and ophthalmoplegia14 have also been described.
We presents an alternative position, the supine position, for shoulder arthroscopy. This position offers the benefits of both the lateral decubitus position and the beach chair position, but it is relatively easy to set up.
Surgical Technique
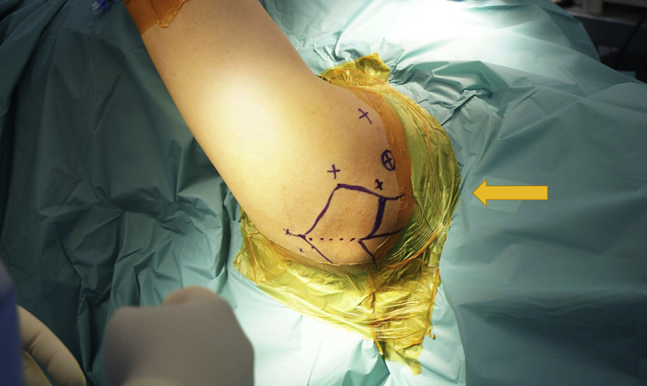
Shoulder arthroscopic surgery in the supine position is performed when the patient receives a brachial block in the interscalene region, guided by ultrasound. This is combined with a laryngeal mask airway or general anesthesia by an anesthetist. The patient is then placed supinely on an operating table (ALPHASTAR, Maquet GmbH, Rastatt, Germany) in the reverse position with the patient's head above one of the leg plates. The other leg plate on the operating side is detached to make room for the operation. The patient's head is maintained in a neutral position and stabilized with tape. The scapular must be set free from the operating table. Pressure points are padded with foam pads (Fig 1 and Video 1).
Fig 1.

Patient positioning for shoulder arthroscopic surgery in the supine position. The patient with anteroinferior capsulolabral lesion from recurrent anterior dislocation of the left shoulder is placed supinely on an operating table in the reverse position with the leg plate on the operating side detached (arrow) and the patient's head stabilized with tape.
Then the forearm of the arm to be operated is strapped by simple adhesive traction tape that is connected to a traction device. A weight of approximately 3 to 6 kg is applied to the traction device, depending on the size of the patient. The traction position should be 45° of forward flexion and 30° of abduction (Fig 2).
Fig 2.

Patient's arm positioning for shoulder arthroscopic surgery in the supine position. The arm to be operated is strapped by adhesive traction tape (arrow) that is connected to a traction device with a weight of 3 to 6 kg. The traction position should be 45° of forward flexion and 30° of abduction.
With the arm supported in suspension, a sterile waterproof drape is then applied. This arm position is suitable for a good view of both the glenohemoral joint and the subacromial space. The next step is outlining the surface anatomy with a sterile marking pen before making any skin incisions (Fig 3).
Fig 3.
Surgical area preparation for shoulder arthroscopic surgery in the supine position. A sterile waterproof drape (arrow) is applied to the patient's left shoulder. Surface anatomy is outlined by a sterile marking pen.
Arthroscopy is initiated with a posterior portal slightly lateral to the glenohumeral joint line. After the joint is entered, an anterior-superior portal and an anterior-inferior portal are established (Fig 4). The rest of the surgical procedure in the supine position, including the arthroscopic view, is the same as in the traditional positions (Fig 5).
Fig 4.
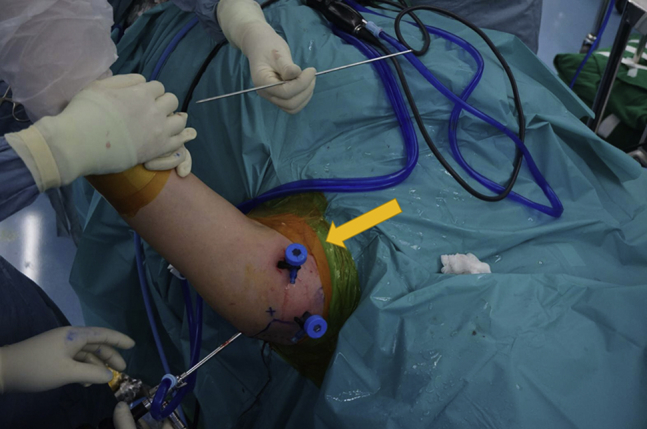
Portal insertions for shoulder arthroscopic surgery in the supine position. Arthroscopy is initiated on the patient's left shoulder with a posterior portal slightly lateral to the glenohumeral joint line. An anterior-superior portal and an anterior-inferior portal can then be established (arrow).
Fig 5.
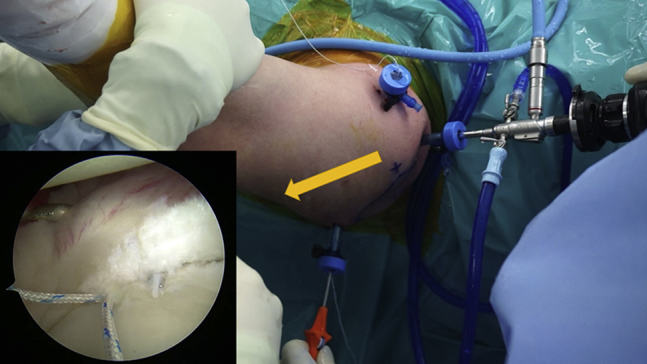
Arthroscopic view of shoulder arthroscopic surgery in the supine position from the anterior-superior portal. The view from the camera (arrow) is the same as in the lateral decubitus position and the beach chair position, however, the camera orientation is different.
Discussion
Shoulder arthroscopic surgery in the supine position is similar to surgery in the lateral decubitus position. However, in the supine position, it is easier to access the anterior portal. The patient's head and the operating table do not obstruct the surgery as in the beach chair position. Similar to the lateral decubitus position, air bubbles from electrocautery do not interfere during the procedure. It is easy to convert to an open procedure with a patient in the supine position with excellent visualization and access to the surgical site just by removing the traction device. The anesthesiologist can easily convert the laryngeal mask airway to intubation in this position when necessary. The surgery can be performed as an out-patient procedure where the patient receives only a brachial block with sedation.
There is still a possibility of neurologic complications from using the traction device, including compression of the dorsal digital nerve of thumb and peroneal nerve and traction-induced trauma to the brachial plexus.2, 15, 16, 17 However, care can be taken to avoid excessive hyperflexion or hyperabduction of the arm. The traction weights should not be more than 7 kg.16, 17 Overall, the comparison of the advantages and disadvantage of shoulder arthroscopic surgery in the lateral decubitus, the beach chair, and the supine position are shown in Table 1 and Table 2.18, 19, 20, 21
Table 1.
Comparison of the Advantages of Shoulder Arthroscopic Surgery in the Lateral Decubitus, the Beach Chair, and the Supine Position
| Advantages | Lateral Decubitus | Beach Chair | Supine |
|---|---|---|---|
| Subacromial and joint space increase from traction | x | x | |
| Provides better access to capsulolabral and bicep lesion | x | x | |
| Cautery bubbles float out of the working area | x | x | |
| Patient's head and operating table do not obstruct the superior and posterior shoulder | x | x | |
| Arm not hanging in the way of the anterior portal | x | x | |
| Easy to convert to an open procedure without repositioning or redraping | x | x |
Table 2.
Comparison of the Disadvantages of Shoulder Arthroscopic Surgery in the Lateral Decubitus, the Beach Chair, and the Supine Position
| Disadvantages | Lateral Decubitus | Beach Chair | Supine |
|---|---|---|---|
| Increased risk of cardiovascular and cerebral hypoperfusion | x | ||
| Requires an assistant or expensive equipment to maintain the arm position | x | ||
| Less visualization in posterior and inferior aspects of the joint | x | ||
| Patients need to receive general anesthesia | x | x | |
| Nonanatomic orientation | x | x | |
| Increased risk of neurapraxia to brachial plexus and peripheral nerve | x | x |
A wide spectrum of procedures can be done with a patient in the supine position, such as capsulolabral repair, rotator cuff repair, subacromial decompression, bicep tenotomy, bicep tenodesis, acromioclavicular joint resection, removal of calcific tendinitis, and release of adhesion from adhesive capsulitis. Even though the arthroscopic view in the supine position is the same as in the traditional positions, the surgeon must learn how to operate with a different camera orientation (Table 3).
Table 3.
Pearls and Pitfalls of Shoulder Arthroscopic Surgery in the Supine Position
| Pearls |
| The operating table must have an option to detach the shoulder support (or leg plate) |
| Patient's head must be strapped securely |
| Traction weight should be less than 7 kg to prevent risk of neurapraxia |
| The traction position should be 45° of forward flexion and 30° of abduction |
| Pitfall |
| Surgeon needs experience and practice to learn how to operate in this position |
In summary, the proposed supine position has been shown to have most of the advantages of both the lateral decubitus position and the beach chair position, yet it avoids some of the disadvantages of those positions. Furthermore, the supine position is comparatively easy to set up and comfortable for the patient, the assistant, the anesthetist, and the surgeon.
Footnotes
The authors report that they have no conflicts of interest in the authorship and publication of this article.
Supplementary Data
Step-by-step demonstration of shoulder arthroscopic surgery in the supine position. The video shows an example procedure on a male patient with anteroinferior capsulolabral lesion from recurrent anterior dislocation of the left shoulder. The patient is placed supinely on an operating table in the reverse position with the leg plate on the operating side detached, and the arm to be operated is strapped by adhesive traction tape that is connected to a traction device. The rest of the surgical procedure in the supine position is similar to the procedure in the traditional positions. The video includes the list of advantages of the supine position over the lateral decubitus position and the beach chair position.
References
- 1.Gross R.M., Fitzgibbons T.C. Shoulder arthroscopy: A modified approach. Arthroscopy. 1985;1:156–159. doi: 10.1016/s0749-8063(85)80002-5. [DOI] [PubMed] [Google Scholar]
- 2.Peruto C.M., Ciccotti M.G., Cohen S.B. Shoulder arthroscopy positioning: Lateral decubitus versus beach chair. Arthroscopy. 2009;25:891–896. doi: 10.1016/j.arthro.2008.10.003. [DOI] [PubMed] [Google Scholar]
- 3.Klein A.H., France J.C., Mutschler T.A., Fu F.H. Measurement of brachial plexus strain in arthroscopy of the shoulder. Arthroscopy. 1987;3:45–52. doi: 10.1016/s0749-8063(87)80009-9. [DOI] [PubMed] [Google Scholar]
- 4.Pitman M.I., Nainzadeh N., Ergas E., Springer S. The use of somatosensory evoked potentials for detection of neuropraxia during shoulder arthroscopy. Arthroscopy. 1988;4:250–255. doi: 10.1016/s0749-8063(88)80039-2. [DOI] [PubMed] [Google Scholar]
- 5.Polzhofer G.K., Petersen W., Hassenpflug J. Thromboembolic complication after arthroscopic shoulder surgery. Arthroscopy. 2003;19:E129–E132. doi: 10.1016/j.arthro.2003.09.016. [DOI] [PubMed] [Google Scholar]
- 6.Kuremsky M.A., Cain E.L., Jr., Fleischli J.E. Thromboembolic phenomena after arthroscopic shoulder surgery. Arthroscopy. 2011;27:1614–1619. doi: 10.1016/j.arthro.2011.06.026. [DOI] [PubMed] [Google Scholar]
- 7.Skyhar M.J., Altchek D.W., Warren R.F., Wickiewicz T.L., O'Brien S.J. Shoulder arthroscopy with the patient in the beach-chair position. Arthroscopy. 1988;4:256–259. doi: 10.1016/s0749-8063(88)80040-9. [DOI] [PubMed] [Google Scholar]
- 8.Hoenecke H.R., Fronek J., Hardwick M. The modified beachchair position for arthroscopic shoulder surgery: The La Jolla beachchair. Arthroscopy. 2004;20(suppl 2):113–115. doi: 10.1016/j.arthro.2004.04.017. [DOI] [PubMed] [Google Scholar]
- 9.Pohl A., Cullen D.J. Cerebral ischemia during shoulder surgery in the upright position: A case series. J Clin Anesth. 2005;17:463–469. doi: 10.1016/j.jclinane.2004.09.012. [DOI] [PubMed] [Google Scholar]
- 10.Dippmann C., Winge S., Nielsen H.B. Severe cerebral desaturation during shoulder arthroscopy in the beach-chair position. Arthroscopy. 2010;26:S148–S150. doi: 10.1016/j.arthro.2010.03.012. [DOI] [PubMed] [Google Scholar]
- 11.Murphy G.S., Szokol J.W., Marymont J.H. Cerebral oxygen desaturation events assessed by near-infrared spectroscopy during shoulder arthroscopy in the beach chair and lateral decubitus positions. Anesth Analg. 2010;111:496–505. doi: 10.1213/ANE.0b013e3181e33bd9. [DOI] [PubMed] [Google Scholar]
- 12.Salazar D., Sears B.W., Aghdasi B. Cerebral desaturation events during shoulder arthroscopy in the beach chair position: Patient risk factors and neurocognitive effects. J Shoulder Elbow Surg. 2013;22:1228–1235. doi: 10.1016/j.jse.2012.12.036. [DOI] [PubMed] [Google Scholar]
- 13.Gale T., Leslie K. Anaesthesia for neurosurgery in sitting position. J Clin Neurosci. 2004;11:693–696. doi: 10.1016/j.jocn.2004.05.007. [DOI] [PubMed] [Google Scholar]
- 14.Bhatti M.T., Enneking F.K. Visual loss and ophthalmoplegia after shoulder surgery. Anesth Analg. 2003;96:899–902. doi: 10.1213/01.ANE.0000047272.31849.F9. [DOI] [PubMed] [Google Scholar]
- 15.Rains D.D., Rooke G.A., Wahl C.J. Pathomechanisms and complications related to patient positioning and anesthesia during shoulder arthroscopy. Arthroscopy. 2011;27:532–541. doi: 10.1016/j.arthro.2010.09.008. [DOI] [PubMed] [Google Scholar]
- 16.Stanish W.D., Peterson D.C. Shoulder arthroscopy and nerve injury: Pitfalls and prevention. Arthroscopy. 1995;11:458–466. doi: 10.1016/0749-8063(95)90201-5. [DOI] [PubMed] [Google Scholar]
- 17.Weber S.C., Abrams J.S., Nottage W.M. Complications associated with arthroscopic shoulder surgery. Arthroscopy. 2002;18:88–95. doi: 10.1053/jars.2002.31801. [DOI] [PubMed] [Google Scholar]
- 18.Li X., Eichinger J.K., Hartshorn T. A comparison of the lateral decubitus and beach-chair positions for shoulder surgery: Advantages and complications. J Am Acad Orthopaed Surg. 2015;23:18–28. doi: 10.5435/JAAOS-23-01-18. [DOI] [PubMed] [Google Scholar]
- 19.Meex I., Vundelinckx J., Buyse K. Cerebral tissue oxygen saturation values in volunteers and patients in the lateral decubitus and beach chair positions: A prospective observational study. Can J Anesth. 2016;63:537–543. doi: 10.1007/s12630-016-0604-3. [DOI] [PubMed] [Google Scholar]
- 20.Laflam A., Joshi B., Brady K. Shoulder surgery in the beach chair position is associated with diminished cerebral autoregulation but no differences in postoperative cognition or brain injury biomarker levels compared with supine positioning: The anesthesia patient safety foundation beach chair study. Anesth Analg. 2015;120:176–185. doi: 10.1213/ANE.0000000000000455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Frank R.M., Saccomanno M.F., McDonald L.S. Outcomes of arthroscopic anterior shoulder instability in the beach chair versus lateral decubitus position: A systematic review and meta-regression analysis. Arthroscopy. 2014;30:1349–1365. doi: 10.1016/j.arthro.2014.05.008. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Step-by-step demonstration of shoulder arthroscopic surgery in the supine position. The video shows an example procedure on a male patient with anteroinferior capsulolabral lesion from recurrent anterior dislocation of the left shoulder. The patient is placed supinely on an operating table in the reverse position with the leg plate on the operating side detached, and the arm to be operated is strapped by adhesive traction tape that is connected to a traction device. The rest of the surgical procedure in the supine position is similar to the procedure in the traditional positions. The video includes the list of advantages of the supine position over the lateral decubitus position and the beach chair position.