

Abstract
Purpose
Little is known about different ways of assessing risk of distant recurrence following cancer treatment (e.g., numeric or descriptive). We sought to evaluate the association between overestimation of risk of distant recurrence of breast cancer and key patient reported outcomes, including quality of life and worry.
Methods
We surveyed a weighted random sample of newly diagnosed patients with early-stage breast cancer identified through SEER registries of Los Angeles & Georgia (2013-14) ∼2 months after surgery (N=2578, RR=71%). Actual 10-year risk of distant recurrence after treatment was based on clinical factors for women with DCIS & low risk invasive cancer (Stg 1A, ER+HER2-, Gr 1-2). Women reported perceptions of their risk numerically (0 – 100%), with values ≥10% for DCIS & ≥20% for invasive considered overestimates. Perceptions of “moderate, high or very high” risk were considered descriptive overestimates. In our analytic sample (N=927), we assessed factors correlated with both types of overestimation and report multivariable associations between overestimation and QoL (PROMIS physical & mental health) and frequent worry.
Results
30.4% of women substantially overestimated their risk of distant recurrence numerically and 14.7% descriptively. Few factors other than family history were significantly associated with either type of overestimation. Both types of overestimation were significantly associated with frequent worry, and lower QoL.
Conclusions
Ensuring understanding of systemic recurrence risk, particularly among patients with favorable prognosis, is important. Better risk communication by clinicians may translate to better risk comprehension among patients and to improvements in QoL.
Keywords: breast cancer, risk, perception, quality of life
Introduction
The long-term prognosis for women with a new diagnosis of ductal carcinoma in situ (DCIS, or stage 0) or early stage invasive breast cancer with favorable biology is generally excellent.[1,2] Studies have shown that initial management translates into a high likelihood of cure.[2] Only a small proportion of patients experience systemic recurrence of their cancer, which can lead to mortality from the disease. The likelihood of systemic recurrence after treatment for women with node negative, estrogen receptor positive (ER) invasive breast cancer and favorable tumor biology 5 year metastases free survival rates is less than 2%; for those with DCIS, there is almost no chance of systemic recurrence.[2-4] Yet, understanding and interpreting risk, is challenging, and studies have found that many women with breast cancer significantly overestimate their risk of distant recurrence after treatment.[5-8]
Importantly, overestimation of perceived risk of recurrence and associated fear of recurrence, may negatively contribute to long-term outcomes that are important for cancer survivors, such as quality of life (QoL) and ongoing worry. It may also motivate patients to prefer more extensive treatment and follow up care.[9,10] Prior work has identified an important link between overestimation of risk and lower scores on physical health assessments (5) and on fear of recurrence after treatment.7 It may also motivate patients to prefer more extensive treatment and follow up care.[9,10]
Furthermore, despite a rich literature in risk communication documenting different types of risk measurement, no studies have explicitly assessed whether it matters more if patients have an accurate numeric understanding of their risk or a more general descriptive comprehension (i.e. “gist”[11]) of their own risk of cancer spreading. While previous studies lend an important perspective on this issue from clinical samples, there have not been large population-based studies among racially/ethnically diverse samples on this issue.
Our study had two objectives. First, to evaluate correlates of overestimation of distant recurrence, measured both numerically and descriptively, in a diverse, contemporary, population-based sample of breast cancer patients with DCIS and early stage invasive breast cancer. Second, to determine the association between overestimation of risk using two methods (numeric and descriptive) and the patient-reported outcomes of QoL and worry about recurrence.
Methods
Study Population
The iCanCare Study, a large, diverse, population-based survey study of women with favorable prognosis breast cancer, accrued women ages 20-79 with newly diagnosed breast cancer (DCIS and stages I-II) as identified by rapid reporting systems from the Surveillance Epidemiology and End Results (SEER) registries of Georgia and Los Angeles County in 2013-2014. Black, Asian, and Hispanic women were oversampled in Los Angeles.[12] We selected 3,880 of whom 249 women were later deemed ineligible due to having a prior cancer diagnosis or stage III or IV disease; residing outside the SEER registry area; being deceased, too ill or unable to complete a survey in Spanish or English. Of 3,631 eligible women remaining, 1,053 did not return mailed surveys, refused to participate or were lost to follow up. Non-respondents did not differ significantly from respondents on key variables, including stage and race/ethnicity. Of 2,578 patients who responded (71%), for this analysis the following exclusions were made: 1388 because their actual risk of recurrence was higher than that for DCIS or our low risk invasive cases, 165 because they did not have sufficient data to calculate actual risk, and 98 because they had bilateral disease. The resulting analytic sample was 927 women.
Data Collection
Patients were sent surveys approximately 2 months after surgery. We provided a $20 cash incentive and used a modified Dillman method for patient recruitment, as done in prior work.[12,13] All materials were sent in English and Spanish to those with Spanish surnames.[12] Survey responses were then merged with clinical data from SEER. The study was approved by the Institutional Review Boards of the University of Michigan, University of Southern California and Emory University and the Committee for the Protection of Human Subjects and the California Cancer Registry.
Questionnaire Design and Content
Patient questionnaire content was guided by a conceptual framework, research questions, and hypotheses. We chose established measures when available and developed new measures, when necessary, drawing from the literature and our prior research.[14-16] We used standard techniques to assess content validity, including review by survey design experts, cognitive pre-testing with patients, and pilot studies in selected clinic populations.
Measures
Actual Risk of Distant Recurrence
We first created our analytic sample with highly favorable prognosis, and thus very low actual risk of distant recurrence, using stage, histology and biology. Using SEER data, women were classified as having DCIS (stage 0) (with almost no risk of distant recurrence) or low risk invasive breast cancer (with <10% actual risk of distant recurrence); stage 1A, ER+, HER2-, tumor grade 1-2, and either having a 21-gene assay test result of 0-10, or the result was not indicated.[2,3] Actual risk was assessed following treatment (surgery, radiation, chemotherapy).
Overestimation of Risk of Distant Recurrence
We assessed overestimation by using both a numeric and descriptive method. In the survey, women were asked “After receiving all the planned treatments, what do you think is the chance that your cancer will spread to other parts of your body in 10 years?” and asked (1) to provide a numeric estimate on a scale from 0 to 100% and (2) to choose a descriptive risk category (very low, low, moderate, high, very high). For women with DCIS, we considered them to have overestimated risk numerically if they perceived a chance of distant recurrence of 10% or higher; for women with invasive cancer, overestimation was considered 20% or higher. These percent cutoffs were chosen by clinical experts to represent “substantial overestimation of risk of recurrence” as they are more than twice/double the percent of “actual risk of systemic recurrence” expected following treatment for these patients with highly favorable prognosis.[2,3] For all women, if they indicated that their systemic risk of recurrence was moderate, high or very high we considered them to have overestimated their risk descriptively.
To understand the independent and combined effects of numeric and descriptive discordant risk perception, we additionally combined the two risk measures into one 4-level categorical risk summary measure: (1) correct on both numeric and descriptive measure (N+, D+), (2) correct on numeric but overestimated descriptive (N+, D-), (3) correct on descriptive and overestimated on numeric (N-, D+), and (4) overestimated on both numeric and descriptive measures (N-, D-).
Quality of Life
Quality of life (QoL) was measured with the Patient Reported Outcomes Measurement Information System (PROMIS) measure, providing Global Mental Health (GMH) and Global Physical Health (GPH) subscales. The PROMIS scales are validated QoL measures that have been widely used to assess patient reported QoL in cancer.[17,18] The 10-item scale is scored and standardized into the GMH and GPH. PROMIS scores are normalized to a mean of 50 with a standard deviation of 10. A score of < 40 is considered a clinically meaningful decline/reduction in QoL. Following this scoring recommendation, for our analysis, scores of ≤ 40 for GPH and GMH were used to indicate low (worse) mental and physical health.[17]
Frequent Worry about Recurrence
We asked women to indicate on a 5-point scale how often they worried about the cancer coming back in the past month (not at all, a little, sometimes, a lot, almost always). For these analyses, those who indicated they worried at least sometimes were considered to have frequent worry.
Covariates
Covariates used in this analysis included patient demographics and clinical factors. We included age, race/ethnicity (White, Black, Latina, Asian, Other/Unknown), educational attainment (high school graduate or less, some college or more), marital status (married/partnered vs. not), employment (employed; retired; unemployed), number of comorbid health conditions (none vs. 1 or more), and family history of breast cancer (none vs. 1 or more first degree relatives). Breast cancer treatment, including surgical treatment type (lumpectomy; unilateral mastectomy; bilateral mastectomy) and receipt of chemotherapy (yes/no), was also collected via survey. We controlled for patient factors that could confound QoL and worry by including patient report of being bothered by treatment side effects (yes/no) at the time of the survey and a measure of decisional anxiety. We further controlled for treatment (surgery type, radiation and chemotherapy receipt).
Statistical Analyses
We first calculated the proportion of women who overestimated their risk of distant recurrence using both the numeric and descriptive measures, as a whole and separately for women with DCIS and invasive cancer. Multivariable, weighted logistic regression was used to explore correlates of overestimation and to estimate the association between overestimation using both numeric and descriptive forms and each PROMIS measure (physical and mental health) and frequency of worry, after adjustment for all covariates above. We further assessed the association between the combined overestimation measure and QoL. Survey and SEER item non-response was low (<5%) for all covariates; however, to correct for the potential of bias due to missing data, values for missing items were imputed using sequential regression multiple imputation (SRMI).[19] Five multiply imputed datasets were analyzed and model estimates were combined to account for additional uncertainty due to imputation. Results were compared between SRMI analyses and complete-case analyses for any meaningful differences. Odds ratios (OR) with 95% confidence intervals (CI) are reported for models, with p-values ≤0.05 considered significant. All statistical analyses incorporated weights to account for differential probabilities of sample selection and non-response. All analyses were performed using SAS version 9.4 (Cary, NC).
Results
Patient Characteristics
The characteristics of the analytic sample (N=927) are provided in Table 1. The mean age of patients was 63 (range: 31-82). The diversity of the sample reflected the population-based sampling approach: 57.7% white, 17.7% black, 14.4% Latina, 7.5% Asian and 2.7% other. Most reported being married (61.4%) and having some college or more education (71.6%). About two-thirds of patients were treated with lumpectomy (68.3%), and a minority (3.6%) reported having received chemotherapy at the time of the survey.
Table 1. Demographic and Clinical Characteristics among Patients with Favorable Prognosis Breast Cancer (N=927).
| Characteristic | N or Mean | Percent or Minimum – Maximum | Weighted Percent or Weighted Mean |
|---|---|---|---|
| SEER Site | |||
| Los Angeles County | 491 | 53.0 | 51.8 |
| Georgia | 436 | 47.0 | 48.2 |
| Age at survey administration | 63.3 | 31.2 – 82.4 | 62.8 |
| Race/Ethnicity | |||
| Non-Hispanic White | 478 | 51.6 | 57.7 |
| Non-Hispanic Black | 168 | 18.1 | 17.7 |
| Hispanic | 175 | 18.9 | 14.4 |
| Asian | 81 | 8.7 | 7.5 |
| Missing | 25 | 2.7 | 2.7 |
| Education | |||
| High school or less | 273 | 29.4 | 27.4 |
| At least some college | 645 | 69.6 | 71.6 |
| Missing | 9 | 1.0 | 1.0 |
| Marital Status | |||
| Married/partnered | 566 | 61.1 | 61.4 |
| Not partnered | 349 | 37.7 | 37.0 |
| Missing | 12 | 1.3 | 1.5 |
| Employment status | |||
| Employed | 363 | 39.2 | 40.8 |
| Retired | 329 | 35.5 | 34.7 |
| Unemployed | 212 | 22.9 | 22.1 |
| Missing | 23 | 2.5 | 2.3 |
| Breast cancer stage | |||
| DCIS (0) | 429 | 46.3 | 45.0 |
| Low risk invasive | 498 | 53.7 | 55.0 |
| Comorbidities | |||
| None | 644 | 69.5 | 70.0 |
| One or more | 279 | 30.1 | 29.7 |
| Missing | 4 | 0.4 | 0.3 |
| Family history of breast cancer | |||
| No | 702 | 75.7 | 74.3 |
| Yes | 225 | 24.3 | 25.7 |
| Surgical Treatment | |||
| Breast Conserving Surgery | 634 | 68.4 | 68.3 |
| Unilateral Mastectomy | 170 | 17.0 | 17.0 |
| Bilateral Mastectomy | 131 | 14.1 | 14.4 |
| Missing | 4 | 0.4 | 0.4 |
| Chemotherapy at time of survey | |||
| No | 884 | 95.4 | 95.9 |
| Yes | 33 | 3.6 | 3.0 |
| Missing | 10 | 1.1 | 1.1 |
| Current symptom bother | |||
| No | 665 | 71.7 | 72.8 |
| Yes | 243 | 26.2 | 24.9 |
| Missing | 19 | 2.1 | 2.4 |
| Decisional axiety scale | 2.5 | 1 - 5 | 2.5 |
| Missing | 18 | 1.9 | 1.9 |
Overall, 30.4% of women with highly favorable prognosis substantially overestimated their risk of distant recurrence numerically, 14.7% descriptively, and 12.1% overestimated using both definitions. Among women with DCIS, 35.1% overestimated numerically, and 13.1% descriptively, while 24.3% of women with invasive cancer overestimated numerically and 16.7% descriptively (Fig.1a).
Fig. 1a. Overestimation of Risk of Distant Recurrence (Numeric, Descriptive, and Both) in Women with Favorable Prognosis Breast Cancer (Weighted)†.
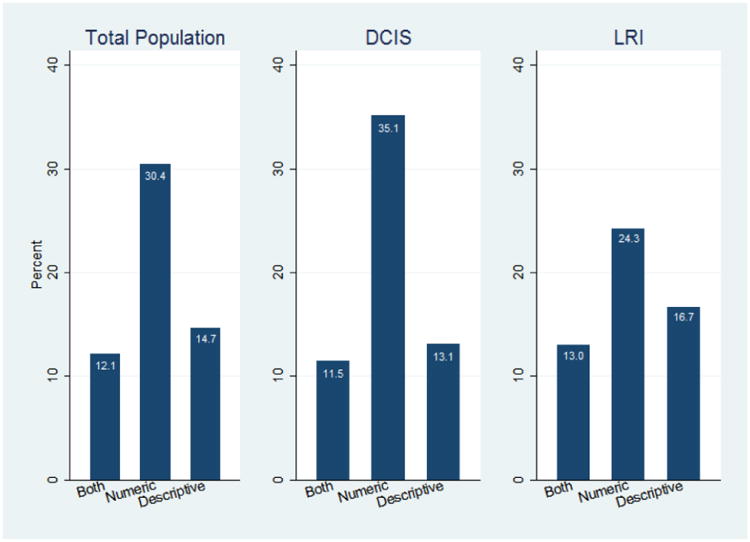
†The denominator population is those answering the risk perception questions. Description: Describes the proportion of patients who overestimated using descriptive, numeric and both types of measurement of risk in the population.
About 10% of patients reported poor mental health and 18.2% poor physical health using PROMIS measures. About a third (30.8%) of women indicated that they worried about the cancer coming back “at least sometimes.” (Fig. 1b).
Fig. 1b. Distribution of Low General Mental Health (GMH), General Physical Health (GPH), and Frequent Worry about Recurrence in Women with Favorable Prognosis Breast Cancer (Weighted)†.
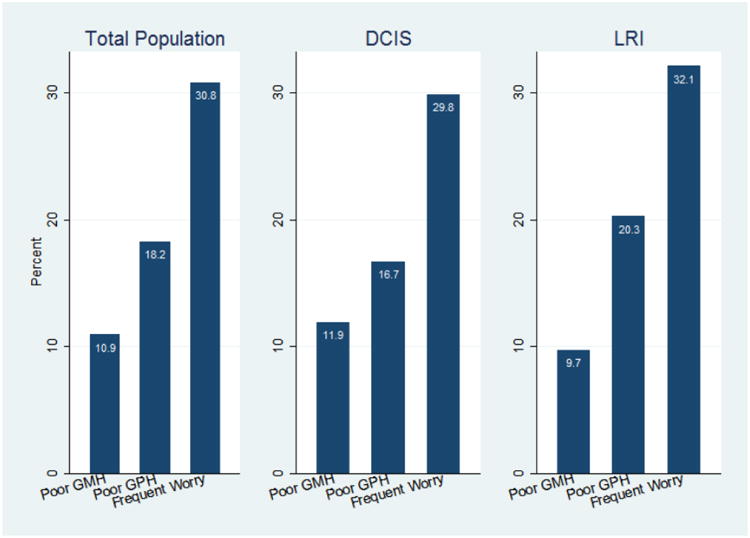
†The denominator population is those answering the QoL questions. Description: Describes the proportion of patients with qol scores of low general mental health, general physical health, and frequent worry about recurrence.
Few demographic or clinical factors were consistently associated with overestimating risk both numerically and descriptively. Black (vs. white) patients were less likely to overestimate numerically (OR: 0.47; 95% CI 0.29-0.76) but not descriptively. Those with more education more often overestimated numerically (OR: 1.46; 95% CI 1.02-2.09). Women with a family history of breast cancer were more likely to overestimate both numerically (OR: 1.45; 95% CI 1.03-2.04) and descriptively (OR: 1.79; 95% CI 1.18-2.69). Finally, women who received bilateral mastectomy (vs. breast conservation) were significantly less likely to overestimate their risk of recurrence numerically (OR: 0.46; 95% CI 0.28-0.76). (Data not shown).
Controlling for all covariates, patients who overestimated their risk numerically had higher odds of reporting frequent worry (OR 2.87; 95% CI 1.90-4.33) than those who did not overestimate. These women were also more likely to report poor physical health (OR: 1.90; 95% CI 1.11-3.26). Women who overestimated their risk descriptively more often reported frequent worry (OR: 3.16; 95% CI 1.87-5.35) and lower mental health (OR: 2.52; 95% CI 1.24-5.08), but were no more likely to report worse physical health. The covariates significantly (p<0.05) associated with poor physical health, poor mental health and more frequent worry are included in Table 2.
Table 2. Multipvariable adjusted logistic regression odds ratios for Poor Mental Health, Poor Physical Health and Frequent Worry.
| Characteristic | Odds Ratio, weighted, with 95% confidence interval | ||
|---|---|---|---|
| Poor Mental Health | Poor Physical Health | Frequent Worry | |
| Age | 0.99 (0.96 - 1.02) | 1.01 (0.99 - 1.04) | 0.97 (0.95 - 0.99) ** |
| + 1 year increase | |||
| Race/ethnicity: | |||
| Non-Hispanic White | REF | REF | REF |
| Non-Hispanic Black (vs Non-Hispanic White) | 0.60 (0.31 - 1.15) | 1.78 (1.01 - 3.15) * | 1.09 (0.66 - 1.80) |
| Hispanic (vs Non-Hispanic White) | 1.33 (0.59 - 3.00) | 1.48 (0.77 - 2.84) | 0.75 (0.44 - 1.27) |
| Asian (vs Non-Hispanic White) | 1.22 (0.44 - 3.37) | 2.60 (1.14 - 5.92)* | 1.09 (0.61 - 1.94) |
| Education: | |||
| Some college or more vs High school or less | 1.76 (0.95 - 3.26) | 3.18 (1.99 - 5.09)˄ | 1.34 (0.88 - 2.06) |
| Employment status: | |||
| Retired vs Employed | 2.31 (1.21 - 4.43)* | 2.38 (1.32 - 4.31)** | 1.32 (0.84 - 2.06) |
| Unemployed vs Employed | 2.49 (1.20 - 5.17)* | 2.04 (1.16 - 3.61)* | 0.82 (0.50 - 1.34) |
| Marital Status: | |||
| Not married/partnered vs Married/partnered | 2.44 (1.41 - 4.20)** | 1.18 (0.75 - 1.86) | 0.95 (0.66 - 1.35) |
| Breast cancer stage: | |||
| Low risk invasive vs DCIS | 0.67 (0.37 - 1.22) | 1.06 (0.69 - 1.65) | 1.57 (1.10 - 2.25)* |
| Family history of breast cancer: | |||
| Yes vs. No | 0.52 (0.28 - 0.97)* | 1.12 (0.72 - 1.74) | 1.05 (0.69 - 1.61) |
| Comorbidities: | |||
| 1 or more vs None | 3.42 (2.02 - 5.81)˄ | 2.90 (1.89 - 4.44)˄ | 1.00 (0.66 - 1.50) |
| Current symptom bother: | |||
| Yes vs No | 2.36 (1.44 - 3.87)˄ | 6.04 (3.98 - 9.18)˄ | 1.30 (0.89 - 1.90) |
| Decisional anxiety scale: | |||
| +1 point increase | 2.14 (1.54 - 2.97)˄ | 1.14 (0.88 - 1.46) | 1.70 (1.37 - 2.11)˄ |
| Descriptive Overestimation: | |||
| Yes vs No | 2.52 (1.24 - 5.08)* | 1.56 (0.84 - 2.91) | 3.16 (1.87 - 5.35)˄ |
| Numeric Overestimation: | |||
| Yes vs No | 1.36 (0.72 - 2.56) | 1.90 (1.11 - 3.26)* | 2.87 (1.90 - 4.33)˄ |
p<0.05,
p<0.01,
p<0.001
Controlling for: site, surgical treatment, chemotherapy receipt
The point estimates and 95% confidence intervals for the association between the 4-category risk perception measure described above and frequent worry are presented in Fig 2. As is apparent from the figure, in adjusted analysis, there is a nearly linear association between risk perception and frequent worry. Compared to women who correctly reported both numeric and descriptive risk (N+, D+), N-, D+ women were 3.2 times as likely to have frequent worry, N+, D- women were 6.2 times as likely, and those who overestimated on both measures (N-, D-) were 8.4 times as likely to have frequent worry.
Fig. 2. Association between Combined Risk Perception Measure and Frequent Worry†.
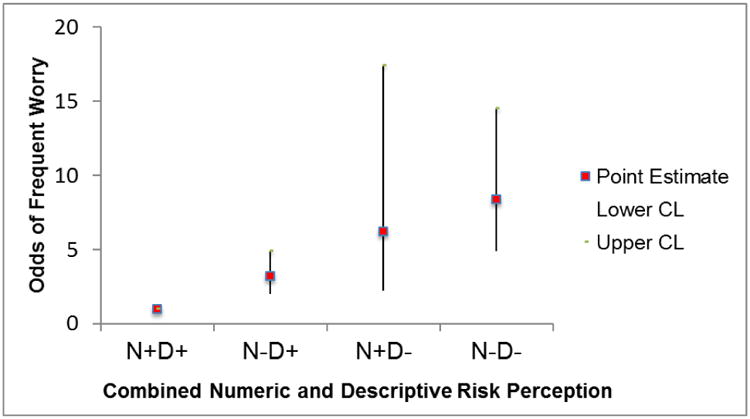
†Controlling for all covariates. (-) indicates overestimation of risk N: numeric, D: descriptive; +: correct (did not overestimate), -: incorrect (did overestimate). Description: Describes the odds ratios for the association between the combined numeric/descriptive measure on frequent worry.
Discussion
In this large, diverse, population-based sample of newly diagnosed and treated breast cancer patients with favorable prognosis, we found that nearly a third (30.4%) overestimated the numeric risk of systemic recurrence to be more than twice their actual risk. A unique finding relative to prior work was that numeric overestimation was more common than descriptive or “gist” overestimation (14.7%). Particularly striking was that almost a third of women with DCIS, who have almost no chance of systemic recurrence, believed their risk to be at 10% or higher.
This study confirms prior research showing that many women diagnosed with breast cancer, including DCIS, do not have an accurate understanding of the likelihood of their cancer spreading systemically.[5-8] However, our study substantially extends this literature to a diverse, population-based sample and by assessing patients' understanding of two different measures of risk perception; a numeric (number-based) and a descriptive (word-based) measure. While we did not find a consistent set of demographic or clinical factors associated with a tendency to overestimate risk using either measure, one factor, having a family history of breast cancer, was associated with both types of overestimation. We conclude that no assumptions should be made about the ability of patients to comprehend their risk, but that patient understanding of their familiar risk may contribute to their assessment of their own risk. Our findings reflect the difficulty of communicating complex risk information (e.g., distant metastatic recurrence versus new primary) in a situation that is emotionally charged and affectively driven.[20]
Our study revealed associations between overestimation and reduced physical and mental health, using validated PROMIS QoL measures, and more frequent patient self-reported worry about recurrence. Our results are consistent with other work showing an association between overestimation and reduced physical health.[5] However, our study further suggests that how overestimation is expressed may influence outcomes. For example, while we found that numeric overestimation was more common, descriptive overestimation had an independent influence on outcomes. While others have found that providing numbers is important for risk comprehension,[21] our study suggests that having a “gist” understanding is also very important. As a whole, these results underscore the need to ensure that women accurately understand their risk of systemic recurrence following treatment, in a general way, as well as numerically.
Importantly, our analysis included a unique assessment of patient report of their personality as it relates to “general anxiety” when making decisions (not specific to breast cancer treatment). This trait was significantly and independently associated with QoL and frequent worry, supporting the concept that patients who are more naturally anxious may also be more likely to overestimate recurrence risk and worry. These findings suggest that ideally patient provider communication would include the assessment and management of underlying anxiety related to decisions as well as communication of risk information using gist and numeric approaches. It is important to note that even when controlling for decisional anxiety, overestimation remained independently associated with frequent worry.
Little is known about underlying reasons why women have difficulty understanding this recurrence risk. In prior work by our team, over 80% of surgeons and oncologists reported that they do discuss risk of recurrence with breast cancer patients – most often using descriptive terms.[22] The current study suggests that despite prior clinician reports, not all patients comprehend risk of recurrence. Several factors may contribute, including low patient numeracy, or clinicians more focused on discussing risk among patients presenting with higher recurrence risk. Importantly, prior work also showed that despite discussing risk, many oncologists and surgeons reported lack of confidence in identifying women who are frequent worriers and in managing worry about recurrence with their patients.[23] Our results suggest that clinicians should consider both as important avenues for intervention. Efforts to educate providers about how to effectively convey risk information to their patients using principles of patient centered communication across patients of diverse backgrounds and literacy levels are needed.[24,25] In fact, research suggests effective communication of uncertainty, including risk information, translates into higher decision satisfaction on the part of patients.[26] Effective patient-provider communication around risk of recurrence would benefit from further studies examining the dimensions of the communication process most closely aligned with patient understanding.
Strengths of this study include a large, diverse sample, clinical information to determine actual recurrence risk, a high participation rate, and use of weighting and multiple imputation methodology. However, the study has some limitations. Patients lived in two geographic regions, so may not represent all U.S. breast cancer patients. Although we had detailed clinical information from SEER to determine actual risk, it is possible that patients perceived additional factors influencing their risk that were not assessed. Finally, associations observed in the study are not necessarily causal.
Implications
Our results suggest strategies to improve patient experiences and outcomes. First, in addition to providing numbers, clinicians could focus attention on describing risk in general verbal terms as well as in numeric terms; doing both may prove easier than conveying specific numeric risk estimates particularly to patients with lower numeracy skills. Second, assessing anxiety and worry across the care trajectory, from diagnosis through the survivorship period, may help identify women who would benefit from support services to manage worry. There is a clear need to improve approaches to conveying risk information to patients as well as assess and manage patient anxiety about the cancer diagnosis and its treatment. Areas for intervention include clinician skill-building in risk communication and patient decision tools that present risk information in comprehensible ways practice. These types of interventions are needed to improve risk comprehension among patients and, if effective, may translate into better quality of life for patients with breast cancer.
Acknowledgments
Research Support: This work was funded by grant P01CA163233 to the University of Michigan from the National Cancer Institute.
The collection of Los Angeles County cancer incidence data used in this study was supported by the California Department of Public Health pursuant to California Health and Safety Code Section 103885; Centers for Disease Control and Prevention's (CDC) National Program of Cancer Registries, under cooperative agreement 5NU58DP003862-04/DP003862; the National Cancer Institute's Surveillance, Epidemiology and End Results Program under contract HHSN261201000140C awarded to the Cancer Prevention Institute of California, contract HHSN261201000035C awarded to the University of Southern California, and contract HHSN261201000034C awarded to the Public Health Institute. The ideas and opinions expressed herein are those of the author(s) and endorsement by the State of California, Department of Public Health, the National Cancer Institute, and the CDC or their Contractors and Subcontractors is not intended nor should be inferred. The collection of cancer incidence data in Georgia was supported by contract HHSN261201300015I, Task Order HHSN26100006 from the NCI and cooperative agreement 5NU58DP003875-04-00 from the CDC. The ideas and opinions expressed herein are those of the author(s) and endorsement by the States of California and Georgia, Department of Public Health the National Cancer Institute, and the Centers for Disease Control and Prevention or their Contractors and Subcontractors is not intended nor should be inferred.
We acknowledge the outstanding work of our project staff (Mackenzie Crawford, M.P.H. and Kiyana Perrino, M.P.H. from the Georgia Cancer Registry; Jennifer Zelaya, Pamela Lee, Maria Gaeta, Virginia Parker, B.A., and Renee Bickerstaff-Magee from USC; Rebecca Morrison, M.P.H., Rachel Tocco, M.A., Alexandra Jeanpierre, M.P.H., Stefanie Goodell, B.S., and Rose Juhasz, Ph.D. from the University of Michigan). We acknowledge with gratitude the breast cancer patients who responded to our survey.
Dr. Kurian has received research funding for work performed outside of the present study from Myriad Genetics, Invitae, Ambry Genetics, GeneDx, and Genomic Health. Dr. Jagsi has done consulting, received funding, as well as provided support for work outside of the current study; she is on the Medical Advisory Board for Eviti, has grants and pending grants from the NIH (R01 and P01), American Cancer Society, National Comprehensive Cancer Network Foundation, and the Translational Breast Cancer Research Consortium, and supports for drug only for a Phase I trial from Abbvie Pharmaceuticals (provides drugs and distribution only for an investigator-initiated trial).
Footnotes
Conflict of interest: All the other authors have no conflict to disclose.
Ethical Standards: This study complies with the current laws in the United States
References
- 1.Narod SA, Iqbal J, Giannakeas V, Sopik V, Sun P. Breast Cancer Mortality After a Diagnosis of Ductal Carcinoma In Situ. JAMA oncology. 2015;1(7):888–896. doi: 10.1001/jamaoncol.2015.2510. [DOI] [PubMed] [Google Scholar]
- 2.Sparano JA, Gray RJ, Makower DF, Pritchard KI, Albain KS, Hayes DF, Geyer CE, Jr, Dees EC, Perez EA, Olson JA, Jr, Zujewski J, Lively T, Badve SS, Saphner TJ, Wagner LI, Whelan TJ, Ellis MJ, Paik S, Wood WC, Ravdin P, Keane MM, Gomez Moreno HL, Reddy PS, Goggins TF, Mayer IA, Brufsky AM, Toppmeyer DL, Kaklamani VG, Atkins JN, Berenberg JL, Sledge GW. Prospective Validation of a 21-Gene Expression Assay in Breast Cancer. The New England journal of medicine. 2015;373(21):2005–2014. doi: 10.1056/NEJMoa1510764. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Vaz-Luis I, Ottesen RA, Hughes ME, Mamet R, Burstein HJ, Edge SB, Gonzalez-Angulo AM, Moy B, Rugo HS, Theriault RL, Weeks JC, Winer EP, Lin NU. Outcomes by tumor subtype and treatment pattern in women with small, node-negative breast cancer: a multi-institutional study. J Clin Oncol. 2014;32(20):2142–2150. doi: 10.1200/jco.2013.53.1608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Worni M, Akushevich I, Greenup R, Sarma D, Ryser MD, Myers ER, Hwang ES. Trends in Treatment Patterns and Outcomes for Ductal Carcinoma In Situ. Journal of the National Cancer Institute. 2015;107(12):djv263. doi: 10.1093/jnci/djv263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ruddy KJ, Meyer ME, Giobbie-Hurder A, Emmons KM, Weeks JC, Winer EP, Partridge AH. Long-term risk perceptions of women with ductal carcinoma in situ. The oncologist. 2013;18(4):362–368. doi: 10.1634/theoncologist.2012-0376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Partridge A, Adloff K, Blood E, Dees EC, Kaelin C, Golshan M, Ligibel J, de Moor JS, Weeks J, Emmons K, Winer E. Risk perceptions and psychosocial outcomes of women with ductal carcinoma in situ: longitudinal results from a cohort study. Journal of the National Cancer Institute. 2008;100(4):243–251. doi: 10.1093/jnci/djn010. [DOI] [PubMed] [Google Scholar]
- 7.Haas JS, Kaplan CP, Des Jarlais G, Gildengoin V, Perez-Stable EJ, Kerlikowske K. Perceived risk of breast cancer among women at average and increased risk. Journal of women's health (2002) 2005;14(9):845–851. doi: 10.1089/jwh.2005.14.845. [DOI] [PubMed] [Google Scholar]
- 8.Liu Y, Perez M, Aft RL, Massman K, Robinson E, Myles S, Schootman M, Gillanders WE, Jeffe DB. Accuracy of perceived risk of recurrence among patients with early-stage breast cancer. Cancer epidemiology, biomarkers & prevention : a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology. 2010;19(3):675–680. doi: 10.1158/1055-9965.epi-09-1051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Fisher CS, Martin-Dunlap T, Ruppel MB, Gao F, Atkins J, Margenthaler JA. Fear of recurrence and perceived survival benefit are primary motivators for choosing mastectomy over breast-conservation therapy regardless of age. Annals of surgical oncology. 2012;19(10):3246–3250. doi: 10.1245/s10434-012-2525-x. [DOI] [PubMed] [Google Scholar]
- 10.Hawley S, J R, Morrow M, Janz NK, Hamilton A, Graff JJ, Katz SJ. Social and clinical determinants of contralateral prophylactic mastectomy. JAMA surgery. 2014 doi: 10.1001/jamasurg.2013.5689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hawley ST, Zikmund-Fisher B, Ubel P, Jancovic A, Lucas T, Fagerlin A. The impact of the format of graphical presentation on health-related knowledge and treatment choices. Patient education and counseling. 2008;73(3):448–455. doi: 10.1016/j.pec.2008.07.023. [DOI] [PubMed] [Google Scholar]
- 12.Hamilton AS, Hofer TP, Hawley ST, Morrell D, Leventhal M, Deapen D, Salem B, Katz SJ. Latinas and breast cancer outcomes: population-based sampling, ethnic identity, and acculturation assessment. Cancer epidemiology, biomarkers & prevention : a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology. 2009;18(7):2022–2029. doi: 10.1158/1055-9965.epi-09-0238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Dillman D, Smyth J, Christian L. Internet, Mail, and Mixed-Mode Surveys: The Tailored Design Method. 3rd. John Wiley & Sons; Hoboken, NY: 2009. [Google Scholar]
- 14.Jagsi R, Griffith KA, Kurian AW, Morrow M, Hamilton AS, Graff JJ, Katz SJ, Hawley ST. Concerns about cancer risk and experiences with genetic testing in a diverse population of patients with breast cancer. J Clin Oncol. 2015;33(14):1584–1591. doi: 10.1200/jco.2014.58.5885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Janz NK, Hawley ST, Mujahid MS, Griggs JJ, Alderman A, Hamilton AS, Graff JJ, Jagsi R, Katz SJ. Correlates of worry about recurrence in a multiethnic population-based sample of women with breast cancer. Cancer. 2011;117(9):1827–1836. doi: 10.1002/cncr.25740. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hawley ST, Griggs JJ, Hamilton AS, Graff JJ, Janz NK, Morrow M, Jagsi R, Salem B, Katz SJ. Decision involvement and receipt of mastectomy among racially and ethnically diverse breast cancer patients. Journal of the National Cancer Institute. 2009;101(19):1337–1347. doi: 10.1093/jnci/djp271. doi:djp271[pii]10.1093/jnci/djp271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.PROMIS Patient-Reported Outcomes Measurement Information System: Dynamic tools to Measure Health Outcomes From the Patient Perspective. [Accessed June 24, 2016]; http://www.nihpromis.org.
- 18.Weaver KE, Forsythe LP, Reeve BB, Alfano CM, Rodriguez JL, Sabatino SA, Hawkins NA, Rowland JH. Mental and physical health-related quality of life among U.S. cancer survivors: population estimates from the 2010 National Health Interview Survey. Cancer epidemiology, biomarkers & prevention : a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology. 2012;21(11):2108–2117. doi: 10.1158/1055-9965.epi-12-0740. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Raghunathan TE, Lepkowski JM, Van Hoewyk J, Solenberger P. A Multivariate Technique for Multiply Imputing Missing Values Using a Sequence of Regression Models. Survey Methodology. 2001;27(1):85–96. [Google Scholar]
- 20.Keller C, Siegrist M, Gutscher H. The role of the affect and availability heuristics in risk communication. Risk analysis : an official publication of the Society for Risk Analysis. 2006;26(3):631–639. doi: 10.1111/j.1539-6924.2006.00773.x. [DOI] [PubMed] [Google Scholar]
- 21.Peters E, Hart PS, Tusler M, Fraenkel L. Numbers matter to informed patient choices: a randomized design across age and numeracy levels. Medical decision making : an international journal of the Society for Medical Decision Making. 2014;34(4):430–442. doi: 10.1177/0272989x13511705. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Zikmund-Fisher BJ, Janz NK, Hawley ST, Griffith KA, Sabolch A, Jagsi R. Communication of Recurrence Risk Estimates to Patients Diagnosed With Breast Cancer. JAMA oncology. 2016 doi: 10.1001/jamaoncol.2015.6416. [DOI] [PubMed] [Google Scholar]
- 23.Janz NK, Leinberger RL, Zikmund-Fisher BJ, Hawley ST, Griffith K, Jagsi R. Provider perspectives on presenting risk information and managing worry about recurrence among breast cancer survivors. Psycho-oncology. 2015;24(5):592–600. doi: 10.1002/pon.3625. [DOI] [PubMed] [Google Scholar]
- 24.Commission TJ. What Did the Doctor Say?: Improving Health Literacy to Protect Patient Safety 2007 [Google Scholar]
- 25.Fagerlin A, Zikmund-Fisher BJ, Ubel PA. Helping patients decide: ten steps to better risk communication. Journal of the National Cancer Institute. 2011;103(19):1436–1443. doi: 10.1093/jnci/djr318. doi:djr318[pii]10.1093/jnci/djr318. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Politi MC, Clark MA, Ombao H, Dizon D, Elwyn G. Communicating uncertainty can lead to less decision satisfaction: a necessary cost of involving patients in shared decision making? Health expectations : an international journal of public participation in health care and health policy. 2011;14(1):84–91. doi: 10.1111/j.1369-7625.2010.00626.x. [DOI] [PMC free article] [PubMed] [Google Scholar]