

Abstract
An ileal pouch fistula is an uncommon complication after an ileal pouch anal anastomosis. Most patients who suffer from an ileal pouch fistula will need surgical intervention. However, the surgery can be invasive and has a high risk compared to endoscopic treatment. The over-the-scope clip (OTSC) system was initially developed for hemostasis and leakage closure in the gastrointestinal tract during flexible endoscopy. There have been many successes in using this approach to apply perforations to the upper gastrointestinal tract. However, this approach has not been used for ileal pouch fistulas until currently. In this report, we describe one patient who suffered a leak from the tip of the “J” pouch and was successfully treated with endoscopic closure via the OTSC system. A 26-year-old male patient had an intestinal fistula at the tip of the “J” pouch after an ileal pouch anal anastomosis procedure. He received endoscopic treatment via OTSC under intravenous anesthesia, and the leak was closed successfully. Endoscopic closure of a pouch fistula could be a simpler alternative to surgery and could help avoid surgery-related complications.
Keywords: Over-the-scope clip system, Endoscopic treatment, Restorative proctocolectomy, Ulcerative colitis, Ileal pouch fistula
Core tip: Leaks from the tip of the J-pouch are less likely to occur but are associated with pouch failure after ileal pouch-anal anastomosis. Salvage surgery has been commonly performed to resolve these leaks, and the surgery typically includes laparotomy with either pouch repair or pouch resection. In this report, we present a patient with a fistula on the tip of the “J” in the pouch who was successfully treated with the over-the-scope clip system. We propose that this method could be used as an alternative to surgery to avoid surgery-related complications in patients with pouch fistula.
INTRODUCTION
A leak from the tip of the J-pouch was defined as a leak from the blind limb of the J-pouch with an endoscopic finding or imaging results, including a Gastrografin enema, computed tomography scan, magnetic resonance imaging, or intraoperative diagnosis made during reoperation[1-3]. Although leaks from the tip of the J-pouch are less likely to occur than leaks from anastomosis, these leaks are known to be associated with pouch failure after ileal pouch-anal anastomosis (IPAA). Salvage surgery has been commonly used for leaks and typically includes laparotomy with either pouch repair or pouch resection[3].
Recently, interventional endoscopy has evolved into an effective alternative to salvage surgery for leakages or perforations if the patient is not in a critical septic condition[4,5]. The over-the-scope clip (OTSC) system (Ovesco Endoscopy AG, Tübingen, Germany) was initially developed for hemostasis and leakage closure in the gastrointestinal tract during flexible endoscopy. These “bear claws” apply high compression forces on the tissue and facilitate stable closure[2]. In cases of sufficient closure, surgical intervention can be avoided. For acute endoscopy-associated perforations, the mean success rate is 90%. For postoperative leaks, the success rate is 68%[6]. However, the usage of OTSC in pouch fistula has not been reported yet. Due to the success of the technique and the opportunity to avoid the considerable risks of surgery, we tested the OTSC system in this patient and achieved success.
Endoscopic management of leakage and perforation in the upper gastrointestinal tract has gained prominence because it enables minimally invasive treatment of fistulas and avoids the morbidity and mortality of surgical intervention. However, it is important that the lesion is fresh, does not have fibrotic alterations or inflammation and is usually free from foreign bodies in the leakage area[1]. In this case, we used an active washing and drainage system for 4 wk to make the lesion of the fistula clear and reduce inflammation before the endoscopic closure.
CASE REPORT
A 26-year-old male patient was admitted to our hospital due to fever and severe bloody diarrhea. Endoscopy revealed acute ulcerative colitis with a Mayo score of 12. He failed to respond to intravenous corticosteroid therapy, and toxic megacolon appeared. He underwent a total laparoscopic restorative proctocolectomy with IPAA (with a loop ileostomy). After surgery, the patient recovered without complications and was discharged 10 d after the operation. Six weeks later, he was readmitted to our department for ileostomy reversal. Prior to the operation, pouch endoscopy, antegrade Gastrografin enema, and an abdominal computed tomography scan did not reveal an abnormality. A stapled side-to-side ileostomy reversal was performed, and he was discharged 3 d after the operation. One month after the final operation, he developed a high fever again (39.9 °C) with stool leaking from the right lower abdominal trocar site. Colonoscopy and a Gastrografin enema confirmed there was a fistula on the tip of the “J” Pouch (Figures 1 and 2). He was treated with percutaneous drainage, total parenteral nutrition (TPN) and bowel rest. Signs of intra-abdominal sepsis were controlled after 4 wk of therapy. However, there was persistent feculent discharge from the fistula tract. The patient was comprehensively informed about the endoscopic procedure.
Figure 1.
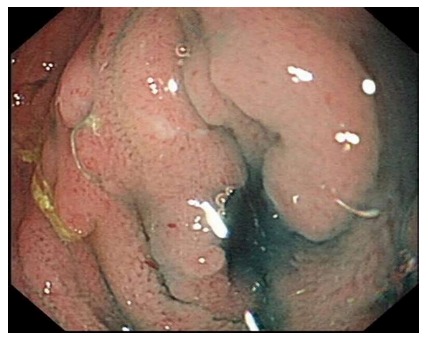
Methylene blue was injected via the trocar site and flooded the enteric cavity to reveal a leak in the pouch.
Figure 2.
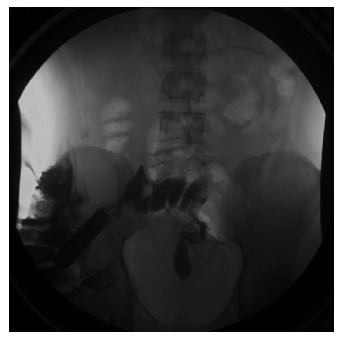
Urografin was injected via the sinus, and the pouch was visualized to confirm a fistula on the top of the “J” pouch.
DISCUSSION
Alternatives, such as surgical treatment, were also discussed with the patient, and written informed consent was obtained. The patient was informed about the possible failure of the endoscopic procedure and the eventual need for an operation that may lead to pouch repair or even pouch resection. Endoscopic evaluation and a Methylene blue injection demonstrated a pouch-cutaneous fistula on the tip of the “J” pouch. Suction was used to draw the defect into the OTSC applicator cap, and the clip (12-mm OTSC) was applied, which completely closed the fistula tract (Figure 3). The complete procedure was performed in 21 min. After the procedure, he was given TPN and bowel rest for another 2 wk to allow the fistula to heal. Then, he resumed oral feeding without signs of a fistula or leakage. He was followed up with for another 2 mo and remained asymptomatic. A Gastrografin enema later confirmed that the fistula tract had healed (Figure 4).
Figure 3.
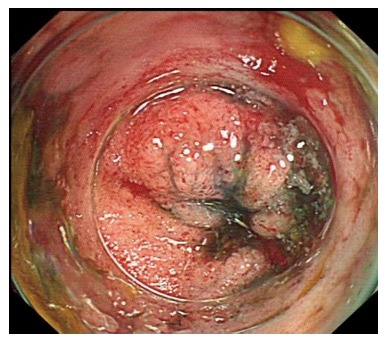
Fistula was closed by the over-the-scope clip system.
Figure 4.

Gastrografin enema confirmed the fistula was closed.
In conclusion, although the OTSC system had mostly been used for treating upper gastrointestinal perfusion and fistulas and fistulas on the top of the pouch are rare and often are cured through surgery, we still suggest attempting OTSC to treat a pouch fistula due to the easy manipulation and reduction of immediate operative intervention rates, and length of hospitalization[7,8]. Even if the endoscopic closure failed, the salvage surgery would still be feasible.
ACKNOWLEDGMENTS
We thank Zhi-Ming Wang and Yan-Qing Diao for helping with the endoscopic closure.
COMMENTS
Case characteristics
This was a young man with severe ulcerative colitis who received ileal pouch-anal anastomosis (IPAA) and developed a fistula after surgery.
Clinical diagnosis
Intestinal fistula.
Differential diagnosis
Leaks from the tip of the J-pouch, Anastomotic fistula, Crohn’s disease, abscess.
Laboratory diagnosis
The patient had a high blood white cell count and fever; thus, he was diagnosed with an intra-abdominal infection.
Imaging diagnosis
Leaks from the tip of the J-pouch.
Pathological diagnosis
He was cured with non-surgical treatment, and there was no pathological diagnosis.
Treatment
Closed the fistula with the over-the-scope clip (OTSC) system.
Related reports
A J-pouch is the most common configuration of IPAA used currently. Risk factors for pouch-related sepsis complications include steroid use, a body mass index greater than 30, a patient older than 50 years, diagnosis of inflammatory bowel disease, and surgeon inexperience. Surgical approaches have always been used for pouch-related sepsis arising from pouch fistula.
Term explanation
Fistula is a pouch-related septic complication. There are 4 main pouch sources of fistula, including the appendage, pouch reservoir, inflow limb, and pouch-rectal anastomosis. Each can fistulize to different areas, including the abdominal wall, vagina, bladder, and other loops of the small bowel.
Experience and lessons
This was a successful application of OTSC to cure a patient with a pouch fistula that could partially replace surgery and avoid surgery-related complications. However, the authors must keep the tissue around the fistula fresh so percutaneous drainage, total parenteral nutrition and bowel rest were necessary.
Peer-review
The paper is well written.
Footnotes
Manuscript source: Unsolicited manuscript
Specialty type: Gastroenterology and hepatology
Country of origin: China
Peer-review report classification
Grade A (Excellent): 0
Grade B (Very good): 0
Grade C (Good): C, C, C, C
Grade D (Fair): 0
Grade E (Poor): 0
Institutional review board statement: This case report was exempt from the Institutional Ethics Committee of Jinling Hospital.
Informed consent statement: The patient involved in this study gave his written informed consent authorizing the use and disclosure of his protected health information.
Conflict-of-interest statement: The authors declare that they have no competing interests.
Peer-review started: September 28, 2016
First decision: October 26, 2016
Article in press: December 19, 2016
P- Reviewer: Goral V, Seow-Choen F, Tang ZP, Tham CK S- Editor: Qiu S L- Editor: A E- Editor: Li D
References
- 1.Mennigen R, Senninger N, Laukoetter MG. Novel treatment options for perforations of the upper gastrointestinal tract: endoscopic vacuum therapy and over-the-scope clips. World J Gastroenterol. 2014;20:7767–7776. doi: 10.3748/wjg.v20.i24.7767. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Raju GS. Endoscopic clip closure of gastrointestinal perforations, fistulae, and leaks. Dig Endosc. 2014;26 Suppl 1:95–104. doi: 10.1111/den.12191. [DOI] [PubMed] [Google Scholar]
- 3.Kirat HT, Kiran RP, Oncel M, Shen B, Fazio VW, Remzi FH. Management of leak from the tip of the “J” in ileal pouch-anal anastomosis. Dis Colon Rectum. 2011;54:454–459. doi: 10.1007/DCR.0b013e31820481be. [DOI] [PubMed] [Google Scholar]
- 4.van Boeckel PG, Sijbring A, Vleggaar FP, Siersema PD. Systematic review: temporary stent placement for benign rupture or anastomotic leak of the oesophagus. Aliment Pharmacol Ther. 2011;33:1292–1301. doi: 10.1111/j.1365-2036.2011.04663.x. [DOI] [PubMed] [Google Scholar]
- 5.Tuebergen D, Rijcken E, Mennigen R, Hopkins AM, Senninger N, Bruewer M. Treatment of thoracic esophageal anastomotic leaks and esophageal perforations with endoluminal stents: efficacy and current limitations. J Gastrointest Surg. 2008;12:1168–1176. doi: 10.1007/s11605-008-0500-4. [DOI] [PubMed] [Google Scholar]
- 6.Mennigen R, Colombo-Benkmann M, Senninger N, Laukoetter M. Endoscopic closure of postoperative gastrointestinal leakages and fistulas with the Over-the-Scope Clip (OTSC) J Gastrointest Surg. 2013;17:1058–1065. doi: 10.1007/s11605-013-2156-y. [DOI] [PubMed] [Google Scholar]
- 7.Yang DH, Byeon JS, Lee KH, Yoon SM, Kim KJ, Ye BD, Myung SJ, Yang SK, Kim JH. Is endoscopic closure with clips effective for both diagnostic and therapeutic colonoscopy-associated bowel perforation? Surg Endosc. 2010;24:1177–1185. doi: 10.1007/s00464-009-0746-2. [DOI] [PubMed] [Google Scholar]
- 8.Kim JS, Kim BW, Kim JI, Kim JH, Kim SW, Ji JS, Lee BI, Choi H. Endoscopic clip closure versus surgery for the treatment of iatrogenic colon perforations developed during diagnostic colonoscopy: a review of 115,285 patients. Surg Endosc. 2013;27:501–504. doi: 10.1007/s00464-012-2465-3. [DOI] [PubMed] [Google Scholar]