

Abstract
Pigmented Bowen's disease is a rare subtype of Bowen's disease. Clinically it presents as a slow-growing, well-defined, hyperpigmented plaque, and should be included as a differential diagnosis of other pigmented lesions. The authors describe a challenging case of pigmented Bowen's disease with non-diagnostic dermscopy findings.
Keywords: Bowen's disease, Squamous cell carcinoma, Dermoscopy, Skin neoplasms
Pigmented Bowen's disease is a rare subtype of Bowen's disease, accounting for 2% to 5% of all cases.1,2 It manifests as a slow-growing, well-defined, hyperpigmented plaque, and should be included as a differential diagnosis of pigmented lesions. The present case stands out for the lack of dermoscopic criteria suggestive of pigmented Bowen's disease and the presence of streaks. Thus, it was not possible to set it apart from a melanocytic lesion by dermoscopy. Our patient was a 67-year old female, skin type IV, with no prior diseases, with a history of progressively growing dark lesion on her left buttock that had been present for the past five years. Clinical examination revealed a 1 cm hyperpimented (half dark brown and half light brown) macule with relatively regular borders (Figure 1). Dermoscopy showed an amorphous lightbrown areaadjacent to a dark brown area, containing irregularly distributed globules, streaks and grayished-black portions (Figure 2). Seborrheic keratosis and melanoma were the postulated as working diagnoses. An excisional showed loss of polarity, atypias in all layers of the epidermis, mitoses, dyskeratosis and dyskaryosis (Figure 3). The Fontana-Masson stain showed a heavy accumulation of melanin in the epidermis and melanophages in the upper dermis (Figure 4). Bowen's disease, or squamous cell carcinoma in situ , is an epithelial neoplasm that may rarely manifest as a pigmented disorder. It has been more frequently described in patients with high skin types and in sun-protected areas such as lower limbs and intertriginous areas.1,3 Clinically, it is a slow growing, well-defined, unevenly pigmented plaque, with a scaling, velvety, verrucous or flat surface.4-6 The differential diagnoses include - melanocytic lesions (nevi or cutaneous melanoma), solar lentigo, seborrheic keratosis, lichen planus-like keratosis, pigmented actinic keratosis and pigmented basal cell carcinoma.2,7 Since 2004, several dermoscopic findings have been described, and dermoscopy has proved to be an important diagnostic tool. Zalaudek et al. reported the following findings in a series of 10 cases: desquamative surface (90%), small brown globules grouped and irregularly distributed in the lesion (90%), glomerular vessels (80%), greyish homogeneous pigmentation, as well as pigmented network (10%), and streaks (10%).5 In the largest case series of cases thus far published Cameron et al. described the dermoscopic features of 52 cases of pigmented Bowen's disease. The most common pattern (48%) was amorphous (with no structures), followed by the association of amorphous pattern and dots (35%). Hypopigmented areas ( pink, normochromic or white) without structures were seen in 67% of the lesions. Vessels were detected in 67% of the lesions, and the glomerular vessels were the most frequent (44%). Dotted or glomerular vessels in linear arrangement were detected in 12% of the cases.2 The presence vessels and brown or gray dots in arrangened in linear fashion in the periphery of the lesion was considered by the authors to be the most suggestive, and perhaps the most specific, finding of pigmented Bowen's disease. These changes have not been described in other lesion and were present in 21% of the cases. The predominant dermoscopic finding in our case was the amorphous pattern . The presence of sreaks turned the diagnosis even more challenging since since this finding is higly suggestive of a melanocytic lesion. However, pigment network and streaks are relatively common in pigmented Bowen's disease and have already been reported with an incidence ranging from 4% to 10%.2,3,8 The differential diagnosis with other pigmented diseases continues, therefore, to be challenging. Albeit rare, pigmented Bowen's disease should be suspected especially if glomerular vessels or brownish dots are found to be linearly arranged in the lesion, or if there are no clear criteria of melanocytic lesion in the dermoscopy, given that the brownish amorphous pattern seems to be the most frequent one. Some lesions may show streaks, making it even more difficult to tell them apart from melanocytic lesions. Dermoscopy is not always diagnostic, but leads to a proper approach. In this case, surgical removal was chosen due to dermoscopic features.
Figure 1.

Irregular hyperpigmented lesion on the left buttock, with a diameter of 1 cm
Figure 2.

The dermoscopy of the lesion shows an amorphous light brown area adjacent to a dark brown area containing irregularly distributed globules, streaks and blackened gray parts
Figure 3.
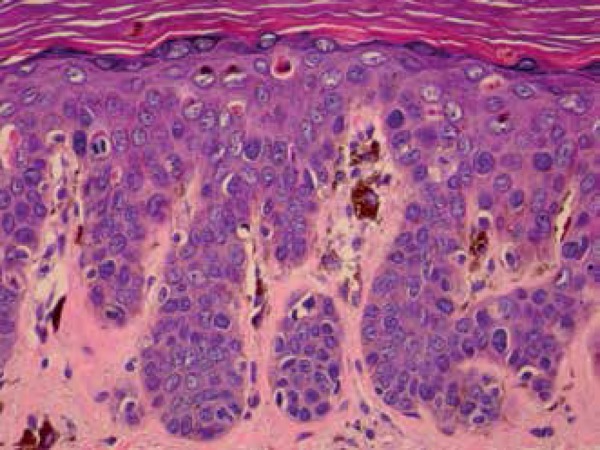
Pigmented Bowen’s disease: loss of polarity, atypias in all layers of the epidermis, mitoses, dyskeratosis and dyskaryosis. Presence of melanophages and increased pigmentation of keratinocytes (Hematoxylin & eosin x400)
Figure 4.
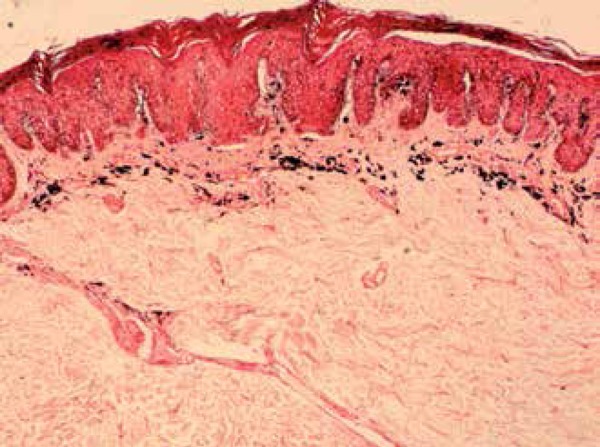
Fontana-Masson staining reveals prominent build-up of melanin in all the layers of the epidermis and melanophages in the superficial dermis (Hematoxylin & eosin x100)
Footnotes
Conflict of Interest: None
Financial Support: None
Work carried out at the Dermatology Department of the Federal University of São Paulo (Unifesp) - São Paulo (SP), Brazil.
References
- 1.Ragi G, Turner MS, Klein LE, Stoll Jr HL. Pigmented Bowen's disease and review of 420 Bowen's disease lesions. J Dermatol Surg Oncol. 1988;14:765–769. doi: 10.1111/j.1524-4725.1988.tb01161.x. [DOI] [PubMed] [Google Scholar]
- 2.Cameron A, Rosendahl C, Tschandl P, Riedl E, Kittler H. Dermatoscopy of pigmented Bowen's disease. J Am Acad Dermatol. 2010;62:597–604. doi: 10.1016/j.jaad.2009.06.008. [DOI] [PubMed] [Google Scholar]
- 3.Gutiérrez-Mendoza D, Narro-Llorente R, Karam-Orantes M, Fonte-Avalos V, Martínez-Luna E, Toussaint-Caire S, et al. Dermoscopy clues in pigmented Bowen's disease. Dermatol Res Pract. 2010 doi: 10.1155/2010/464821. 2010. pii: 464821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lee JW, Hur J, Yeo KY, Yu HJ, Kim JS. A case of pigmented Bowen's disease. Ann Dermatol. 2009;21:197–199. doi: 10.5021/ad.2009.21.2.197. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Zalaudek I, Argenziano G, Leinweber B, Citarella L, Hofmann-Wellenhof R, Malvehy J, et al. Dermoscopy of Bowen's disease. Br J Dermatol. 2004;150:1112–1116. doi: 10.1111/j.1365-2133.2004.05924.x. [DOI] [PubMed] [Google Scholar]
- 6.Öztürk Durmaz E, Dogan Ekici I, Özkan F, Sahin S. Pigmented Bowen's disease of the genitalia masquerading as malignant melanoma. Acta Dermatovenerol Croat. 2015;23:130–133. [PubMed] [Google Scholar]
- 7.Ishioka P, Yamada S, Michalany NS, Hirata SH. Dermoscopy of Bowen's disease: pigmented variant on the penis. An Bras Dermatol. 2012;87:482–484. doi: 10.1590/s0365-05962012000300023. [DOI] [PubMed] [Google Scholar]
- 8.Chung E, Marchetti MA, Pulitzer MP, Marghoob AA. Streaks in pigmented squamous cell carcinoma in situ. J Am Acad Dermatol. 2015;72:S64–S65. doi: 10.1016/j.jaad.2014.08.044. [DOI] [PubMed] [Google Scholar]