

Abstract
At the wrist, kinematic coupling (the relationship between flexion-extension and radial-ulnar deviation) facilitates function. Although the midcarpal joint is critical for kinematic coupling, many surgeries, such as four-corner fusion (4CF) and scaphoid-excision four-corner fusion (SE4CF), modify the midcarpal joint. This study examines how 4CF and SE4CF influence kinematic coupling by quantifying wrist axes of rotation. Wrist axes of rotation were quantified in eight cadaveric specimens using an optimization algorithm, which fit a two-revolute joint model to experimental data. In each specimen, data measuring the motion of the third metacarpal relative to the radius was collected for three conditions (nonimpaired, 4CF, SE4CF). The calculated axes of rotation were compared using spherical statistics. The angle between the axes of rotation was used to assess coupling, as the nonimpaired wrist has skew axes (i.e., angle between axes approximately 60°). Following 4CF and SE4CF, the axes are closer to orthogonal than those of the nonimpaired wrist. The mean angle (±95 percent confidence interval) between the axes was 92.6° ± 25.2° and 99.8° ± 22.0° for 4CF and SE4CF, respectively. The axes of rotation defined in this study can be used to define joint models, which will facilitate more accurate computational and experimental studies of these procedures.
Keywords: axes of rotation, kinematics, motion analysis, scaphoid-excision four-corner fusion, wrist
INTRODUCTION
Many surgical interventions, including arthrodesis and arthroplasty, permanently constrain the wrist by altering the geometry of the radiocarpal and midcarpal joints. For example, four-corner fusion (4CF) is a common surgical procedure used to relieve osteoarthritic wrist pain. During 4CF, a portion of the midcarpal joint is immobilized when the lunate and triquetrum (in the proximal row) are fused to the capitate and hamate (in the distal row). Frequently, 4CF is combined with scaphoid excision (SE4CF) to completely immobilize the midcarpal joint. During SE4CF, excising the scaphoid removes the linkage between the proximal row and the trapezoid and trapezium in the distal row, which are not fused. Thus, SE4CF alters the wrist such that the majority of carpal motion occurs at a modified radiocarpal joint, which is defined by the articulation between the radius and lunate. Surgically constraining the wrist through either 4CF or SE4CF reduces osteoarthritic pain, but has the unintended consequence of long-term functional impairments (e.g., decreased wrist range of motion and decreased grip strength) at both the wrist and hand.1
By definition, joint fusions markedly change wrist joint kinematics. The kinematics of the nonimpaired wrist joint involve skew axes of rotation. That is, the axes of rotation specific to the joint itself are neither aligned with the anatomical planes of the forearm nor orthogonal to each other.2–4 Importantly, an isolated rotation about a skew axis has components in multiple anatomical planes simultaneously. For example, an in vivo imaging study examining the midcarpal joint demonstrated that the capitate moves in an oblique plane, aligned with the dart thrower’s motion.5 Because of the skew orientation of the wrist joint’s axes of rotation, there is an intrinsic relationship between flexion-extension (movement of the hand relative to the forearm in the sagittal plane) and radial-ulnar deviation (movement of the hand relative to the forearm in the medial-lateral plane). More specifically, motion capture experiments, which describe wrist and hand movements relative to orthogonal anatomical planes, demonstrate that functional tasks involve a linear combination of flexion-extension and radial-ulnar deviation.6, 7 This kinematic coupling is essential for performing activities of daily living and facilitates nonimpaired wrist and hand function.6, 8
Despite the dramatic changes to wrist joint kinematics imposed by surgery, the axes of rotation specific to surgically altered joints are rarely examined. To our knowledge, joint axes of rotation following 4CF and SE4CF have not been previously quantified. This lack of data describing joint kinematics is problematic because both experimental and computational methods typically require accurate joint models. Lacking the data necessary to describe joint kinematics following surgery, previous research studies have made incompatible assumptions. For example, motion capture experiments have assumed that constraining wrist motion of nonimpaired subjects by splints is similar to post-operative wrist motion in patients with carpal fusions.6, 9 Alternatively, simulation studies of SE4CF have separately assumed that midcarpal fusion results in wrist motion consistent with either the axes of rotation of only the nonimpaired proximal row10 or those of only the nonimpaired distal row.11 Thus, quantitative studies describing joint axes of rotation following these wrist surgeries are needed.
The goal of this study was to quantify joint axes of rotation in wrists that have undergone 4CF and SE4CF. Given that midcarpal joint motion is known to facilitate coupled motion,5 we hypothesized that the severe reduction of carpal motion at the midcarpal joint associated with both 4CF and SE4CF would significantly alter kinematic coupling at the wrist, as assessed by the relative orientation of the wrist joint’s axes of rotation.
METHODS
The joint axes of rotation of 4CF and SE4CF wrists were examined using eight unmatched, fresh-frozen cadaver upper extremities (three male; five female) that were amputated at the mid-humeral level. The average age (± standard deviation) of the donors at time of death was 61.1 ± 9.1 years (range, forty-four to seventy-three). Radiographs were used to exclude specimens with evidence of degeneration or disease. Seven specimens were simultaneously included in a muscle moment arm experiment.12
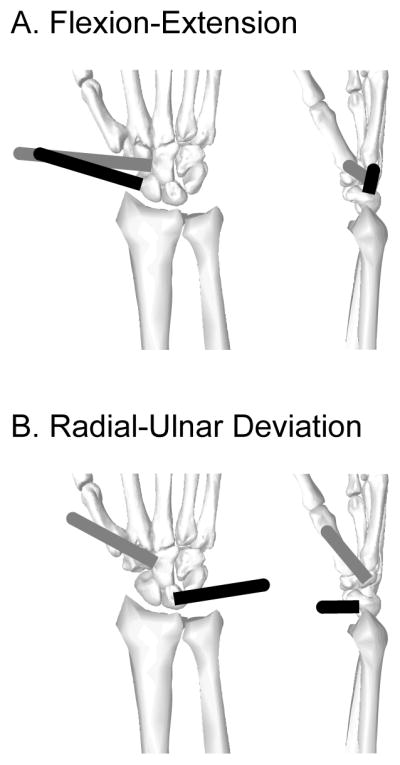
Based on a technique developed by Sommer and Miller,4 we adopted a kinematic model of the wrist joint that assumes the motion of the hand relative to the forearm can be represented by a universal joint with skew-oblique revolutes. This two-revolute joint model is similar to kinematic models implemented in motion capture experiments of the hand and wrist;13, 14 the two axes of rotation for the assumed model are fixed in space and each axis has a distinct origin (Fig. 1A). In our study, the location and orientation of both of these axes were computed for individual cadaveric specimens under a range of conditions based on the position of the third metacarpal relative to the radius during passive motion. The position of the third metacarpal and radius were determined from the measured position of two infrared targets, one attached to each bone (Fig. 1B). The infrared targets are analogous to marker clusters. Each target contained six infrared sensors, and the position of each infrared sensor was measured using an optoelectronic motion measurement system (Optotrak Certus, Northern Digital Inc.), which has an accuracy of 0.1 mm and a positional resolution of 0.0 1 mm.
Figure 1.

(A) The two-revolute joint model used to quantify the orientation and location of wrist joint axes of rotation. Nomenclature defining the assumed joint model is adopted from Sommer and Miller.4 In this model, wrist movement is described by two rotations, first about the flexion-extension axis, and second about the radial-ulnar deviation axis. Refer to the Appendix for a mathematical description of the model. (B) Experimental setup utilized infrared targets to measure the motion of the third metacarpal relative to the radius.
Specimen Preparation
Each specimen was thawed at room temperature and prepped twenty-four hours prior to testing. Preparation involved the placement of a steel rod that was used to passively move the wrist and three infrared targets that were used to define local, global, and anatomical reference frames. External fixators were used to rigidly secure the rod and targets (Fig. 1B). The rod was secured to the second metacarpal. Two infrared targets were secured to the third metacarpal and radius. A third infrared target, attached to the base of the experimental set-up, defined a global reference frame.
Surgical Conditions
In all specimens, three conditions were evaluated sequentially: nonimpaired, 4CF, and SE4CF. The nonimpaired condition represents the native, intact wrist. To simulate 4CF, the midcarpal joint was fused by pinning the lunate, capitate, hamate, and triquetrum with two 1.59 mm Kirschner wires. Accurate placement of the Kirschner wires and neutral alignment of the lunate and capitate was verified using fluoroscopy. To simulate SE4CF, the Kirschner wires remained untouched and the scaphoid was excised. The scaphoid was excised through a small dorsal incision; care was taken to not sever the palmar ligaments. Complete excision of the scaphoid was verified using fluoroscopy. This sequential technique means that the only difference between the 4CF and SE4CF conditions was the removal of the scaphoid; the bone fusion remained constant.
Experimental Testing
All experimental data for a given specimen were collected in a single day, with the specimen at room temperature. Immediately prior to testing, the specimen was secured to a custom jig using two 4.76 mm threaded steel rods that were drilled through the radius and ulna (Fig. 1B). The forearm was fixed in neutral pronation-supination. The wrist was unconstrained. The primary wrist muscles (flexor carpi radialis, flexor carpi ulnaris, extensor carpi radialis brevis, extensor carpi radialis longus, and extensor carpi ulnaris) were each loaded with 250 g weights to simulate passive muscle tension, similar to Sobczak et al.15
For each specimen and condition, position data for the infrared targets were collected during slow, passive wrist motion in order to measure the global motion of the hand relative to the radius (Fig. 2A). Five motion trials were collected for each specimen and condition. All motion trials were performed by the same experimenter, who freely moved the wrist by manipulating the steel rod connected to the second metatarsal; care was taken to ensure the lunate contacted the radius during all movements. During each motion trial, the wrist was moved through its full range of motion (Table 1) by executing the following continuous movements: flexion-extension, radial-ulnar deviation, circumduction, the dart thrower’s motion (motion from radial-extension to ulnar-flexion), and the reverse dart thrower’s motion (motion from ulnar-extension to radial-flexion) (cf., Fig. 2A, sample data trace). In a single trial, all five directions of movement were executed twice. Including this comprehensive and diverse set of movements, distributed throughout the wrist’s functional workspace, was intended to ensure that the computed axes of rotation represented the wrist joint’s full kinematic capabilities. Each motion trial took approximately 1 minute. Position data were sampled at 30 Hz and recorded relative to the global reference frame.
Figure 2.

Determining wrist axes of rotation involved (A) experimental testing followed by (B) implementation of the optimization algorithm. In (A), the representative data trace (black) is raw experimental data from one nonimpaired trial; the bone geometry traces (blue) are a graphical representation depicting the recorded anatomical data. In (B), the bounding volume included rectangular prisms surrounding the translational initial guess space and a set of axes representing the orientation initial guess space; the bounding volume was defined such that initial guesses for flexion-extension axis (green) and the radial-ulnar deviation axis (purple) encompassed different space.
Table 1.
Average Range of Motion During Motion Trials*
| Maximum Angle (in degrees)* | |||
|---|---|---|---|
| Direction | Nonimpaired | 4CF | SE4CF |
| Flexion | 70.0° ± 15.4° | 56.3° ± 18.8° | 62.9° ± 13.0° |
| Extension | 70.6° ± 9.4° | 58.4° ± 10.3° | 62.8° ± 8.6° |
| Radial Deviation | 32.2° ± 15.6° | 23.7° ± 23.1° | 36.3° ± 22.9° |
| Ulnar Deviation | 36.2° ± 12.5° | 28.9° ± 15.4° | 39.9° ± 13.5° |
Reported angles are the mean maximum angle (± standard deviation) across all specimens. The decrease in flexion-extension motion following 4CF and SE4CF is consistent with post-operative impairments following these surgeries.1 The difference in radial-ulnar deviation motion across the three conditions is related to whether the scaphoid is present to constrain motion. Refer to Figure 2 for a sample motion trace from a single specimen and trial, which demonstrates the variability in movement for a single motion trial.
To facilitate transformation of the data from the global reference frame to an anatomical reference frame, reference frames were defined based on the bone geometry of the radius and third metatarsal. Following data collection for all conditions, these bones were dissected out and measurements of their geometry were recorded using an infrared probe. Bone reference frames were established such that positive x, y, and z respectively defined radial, proximal, and dorsal. To define the radius reference frame, data describing the perimeters of the proximal radial head, the lunate fossa, and the scaphoid fossa were collected. The centers of the proximal head, lunate fossa, and scaphoid fossa were then defined as the centers of the circles that best fit the data describing their perimeters. Using these data, the origin of the radius reference frame was defined as the center of the proximal head; the y-axis was defined as the line from the center of the proximal head to the midpoint between the centers of the lunate and scaphoid fossa; the x-axis was defined as perpendicular to the y-axis and in the plane defined by the centers of the lunate fossa, scaphoid fossa, and proximal head; the z-axis was defined as the cross product of the x-axis and y-axis. To define the third metacarpal reference frame, data describing the perimeters of the proximal head, the distal head, and the shaft were collected, and best fit circles were calculated to determine the centers of each region. Using these data, the origin of the third metacarpal reference frame was defined as the midpoint between the centers of the proximal and distal heads; the y-axis was defined as the line from the center of the proximal head to the center of the distal head; the x-axis was defined as perpendicular to the y-axis and normal to the best fit plane created by four points on the dorsal side of the third metacarpal; the z-axis was defined as the cross product of the x-axis and y-axis.
Data Processing
The position data of the infrared targets were processed to determine homogeneous transformation matrices relating the anatomical reference frame of the third metacarpal to the anatomical reference frame of the radius for each measured frame of data. Data for the two left arm specimens were reflected to be processed and analyzed as right arms.
For each specimen, the data for each motion trial were resampled to eliminate nearly identical, sequential data points, as data evenly distributed in space (instead of time) improved the efficiency of the optimization algorithm, described below. During resampling, a data point was retained only if it was at least 2 mm away from neighboring data points. This resulted in data sets that contained approximately 500 data points.
Optimization Algorithm
A two-tiered optimization algorithm adapted from Sommer and Miller4 was used define the two-revolute joint model by calculating the wrist axes of rotation for each specimen and condition. Adopting the nomenclature of Sommer and Miller,4 the first axis is referred to as the flexion-extension axis of the wrist joint, while the second axis is referred to as the radial-ulnar deviation axis of the wrist joint. Please note that, despite this nomenclature, the joint axes that result from our analysis are distinct from the medial-lateral and dorsal-palmar axes of the forearm. In other words, the optimization can result in skew joint axes of rotation.
The optimization algorithm has been described in detail previously.4, 16 Briefly, the algorithm calculates the two axes of rotation for the assumed joint model by minimizing the difference between two homogenous transformation matrices that describe (i) the measured position of the third metacarpal relative to the radius and (ii) a two-revolute joint model of the wrist (Fig. 1B). The algorithm can be represented as
| (1) |
where m is the number of data frames, and ti and αi are respectively the Cartesian translations and roll-pitch-yaw angles of the decomposed homogenous transformation matrices for the experimentally measured values (primed terms) and the two-revolute joint model (unprimed terms). Note, the input to the algorithm is experimentally measured motion data and the output is a set of parameters defining the three-dimensional location and orientation the two axes that define the assumed joint model and best fit the measured data (see Appendix). A Levenberg-Marquardt algorithm17, 18 was implemented for both the outer and inner optimization (lsqnonlin, Matlab 7.6).
Iterative Search to Identify Wrist Axes of Rotation
The two joint axes of rotation were calculated for each specimen and condition (nonimpaired, 4CF, and SE4CF) through a three-phase process that involved (i) an exploratory phase, (ii) a constrained search phase, and (iii) a solution phase (Fig. 2B). This approach made it possible to systematically search the large possible solution space encompassing all possible joint axis orientations and locations. All three phases were completed using a high performance, computing cluster. The final axes of rotation include an orientation (reported as a unit vector) and an origin (reported as a Cartesian coordinate location).
The exploratory phase was used to identify the best initial guess space. In this phase, the measured data from a single motion trial were input into the optimization algorithm and 50 initial guesses were utilized. The first initial guess was similar to previously reported wrist axes of rotation;19, 20 the subsequent initial guesses added 15 percent random noise (corresponds to an approximately 20 degree range on angular parameters and 0.3 cm range on translational parameters) to the first initial guess. From the output solutions, three sets of parameters defining the three best sets of axes were identified and defined as the best initial guess space. The best solutions were defined as the solutions with the minimum squared norm of the residuals (resnorm, Matlab 7.6). In this phase, solutions were identified for 22 out of 24 cases (i.e., 8 specimens times 3 conditions), as 2 cases (corresponding to different specimens and conditions) did not converge (convergence defined as resnorm ≤ 1 ).
The constrained search phase was used to systematically search the identified initial guess space. Specifically, a bounding volume enclosing the identified initial guess space was defined (Fig 2B). This bounding volume was searched by inputting the measured data from a single motion trial into the optimization algorithm and utilizing 250 initial guesses that were equally distributed throughout the volumes. From the output solutions, the parameters defining one best set of axes were identified using the same criteria as described in the exploratory phase. This output solution, which was based on a single motion trial, defined the initial guess space to be subsequently examined across all motion trials.
The solution phase was used to determine the optimal set of axes for each specimen and condition. In this phase, the measured data for each of the five motion trials were separately input into the optimization algorithm utilizing 10 new initial guesses. The first initial guess was equal to the parameters identified in the constrained search phase. The other nine initial guesses were defined by adding random noise to the first initial guess; the magnitude of noise was equivalent to that added in the exploratory phase. In all cases, the final solution was insensitive to the added noise and the motion trial selected for input in the previous phases. The optimal axes of rotation for each specimen and condition were defined as the vector average of the axes of rotation across the five motion trials.
Data Analysis
To evaluate whether 4CF and SE4CF affect the coupled kinematics of the wrist, the angle between the flexion-extension and radial-ulnar deviation axes of rotation were calculated. This angle is a measure of axis skew; 90° represents orthogonal axes of rotation (i.e., no skew), 0° represents parallel axes of rotation (i.e., maximal skew). Using this definition, results we analyzed from previous studies3, 4, 7, 19–22 suggest that the angle between the axes of rotation describing nonimpaired wrist motion is approximately 60° (Table 2).
Table 2.
Orientation of Wrist Axes of Rotation Reported in the Literature
| Study | Description of Study | Calculation of Axes of Rotation and Skew Angle* | Skew Angle (degrees) |
|---|---|---|---|
| Sommer and Miller (1980) | in vivo experiment measuring global wrist motion (n = 5) | axes of rotation calculated using two-revolute joint model; skew angle for a representative subject reported in Table 1 of study | 60.3 |
| Palmer et al. (1985) | in vivo experiment measuring wrist range of motion during activities of daily living (n = 10) | axes of rotation assumed to be normal to regression lines fit to the flexion-extension and radial-ulnar deviation motions reported in Fig. 3 of study | 55.0 |
| Ruby et al. (1988) | cadaveric experiment measuring carpal kinematics (n = 5) | axes of rotation derived from motion of the capitate relative to the radius as described in Nichols et al. (2013) | 58.9 |
| Kobayashi et al. (1997) | cadaveric experiment measuring carpal kinematics (n = 22) | similar to the Ruby et al. (1988) study; axes of rotation derived from motion of the capitate relative to the radius | 78.2 |
| Neu et al. (2001) | in vivo experiment measuring motion of the capitate (n = 20) | axes are reported separately for flexion, extension, radial deviation, and ulnar deviation in Table 1 of study; axes of rotation for all subjects regardless of gender were used; the calculated angle is the average of each axis combination (flexion-radial, flexion-ulnar, extension-radial, extension-ulnar) | 56.5 |
| Li et al. (2005) | in vivo experiment measuring wrist coupling during flexion-extension, radial-ulnar deviation, and circumduction (n = 10) | axes of rotation assumed to be normal to the regression lines reported for the flexion-extension and radial-ulnar deviation motions in Fig. 3 of study | 40.5 |
| Blankenhorn et al. (2007) | cadaveric experiment measuring carpal kinematics (n = 8) | axes of rotation derived from Euler angles describing total wrist motion reported in Table 2 and 3 of study | 77.9 |
| Average skew angle from Previous Literature (mean ± 95% confidence interval): | 61.0 (9.9) | ||
| Average skew angle from this Study ( mean ± 95% confidence interval): | 77.5 (28.0) | ||
Skew angle defined as the angle between the single flexion-extension and single radial-ulnar deviation axes of rotation that describe global wrist motion (i.e., motion of the hand relative to the forearm). For studies measuring individual carpal kinematics, motion of the capitate relative to the radius was assumed to be representative of global wrist motion, as studies have demonstrated that the capitate and third metacarpal move together as a rigid body (e.g., Neu et al., 2001)
To understand specific changes in the wrist axes of rotation, all axes were compared using spherical statistics.23 Comparisons were conducted between each set of conditions (nonimpaired, 4CF, SE4CF), and included separate analyses examining the orientations and the origins of the wrist axes of rotation. For all comparisons, median orientations and origins were examined due to the uneven distribution of the computed axes of rotation. A significance level of p<0.05 with a Bonferonni correction for multiple comparisons was used for all tests (corrected p<0.0167).
RESULTS
The optimization routine was able to accurately quantify the position of the hand in space. With the exception of two separate specimens that did not reach convergence for the nonimpaired and SE4CF conditions, the optimization routine converged for all specimens and conditions to a solution with mean translation residuals less than 0.1 mm and mean angle residuals less than 1.4° (Table 3). The magnitude of error was similar across all types of wrist motion, with the largest magnitude of error occurring for circumduction (Fig. 3).
Table 3.
Mean Absolute Error of the Two-Revolute Joint Model*
| Nonimpaired | 4CF | SE4CF | |
|---|---|---|---|
| X Translation (mm) | 0.01 ± 0.007 | 0.01 ± 0.006 | 0.01 ± 0.008 |
| Y Translation (mm) | 0.01 ± 0.006 | 0.01 ± 0.006 | 0.01 ± 0.004 |
| Z Translation (mm) | 0.02 ± 0.014 | 0.01 ± 0.007 | 0.00 ± 0.006 |
| φAngle (degrees) | 0.7 ± 1.0 | 0.7 ± 2.5 | 0.6 ± 0.3 |
| ΘAngle (degrees) | 1.1 ± 2.2 | 1.0 ± 2.5 | 1.3 ± 0.6 |
| Ψ Angle (degrees) | 0.8 ± 2.6 | 0.8 ± 3.5 | 0.6 ± 0.4 |
Reported values are mean absolute error ± standard deviation across all trials and specimens. Mean absolute error is defined as the magnitude of difference between the angles and translations calculated using the model and those measured experimentally. Positive x, y, and z translations respectively correspond to movement in the radial, proximal, and dorsal directions. φ, Θ, and Ψ respectively correspond rotations about the x, y, and z axes.
Figure 3.
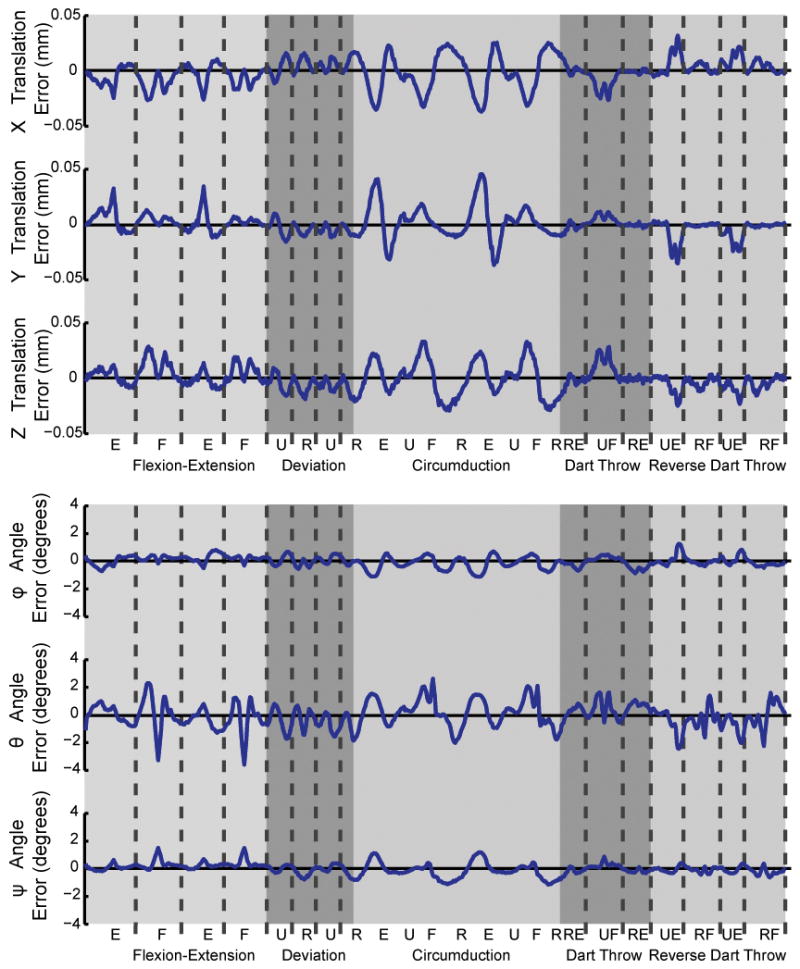
Translation errors (top) and Euler angle errors (bottom) versus wrist motion for a representative specimen and condition. Errors are reported as the difference between the optimized model and the experimental data. Wrist motion was continuous. Dotted lines represent points where the wrist passed through neutral; letters correspond to extremes of motion (F – flexion, E – extension, U – ulnar deviation, R – radial deviation, RE – radial/extension, UF – ulnar/flexion, RF – radial/flexion, UE – ulnar/extension).
Despite the small within specimen error, the optimization solutions for the orientations of the radial-ulnar deviation axes of rotation in the two-revolute joint model (Fig. 1B) were highly variable across the nonimpaired specimens. Notably, this variability in axis orientation was more than 8.4 times larger than that of the orientation of the same axis in the 4CF and SE4CF wrist models (c.f., Fig. 4A compared to Fig. 4B&C). The variability in the orientation for the flexion-extension axes for the nonimpaired wrist was comparable to that of the 4CF and SE4CF wrists (c.f., Fig. 5A compared to Fig. 5B&C).
Figure 4.

Median orientation of the radial-ulnar deviation axes of rotation for the (A) nonimpaired, (B) 4CF, and (C) SE4CF wrists. To allow comparison, the origins of all axes are centered in the same location relative to the radius. Ellipsoid cones represent 95 percent confidence region.
Figure 5.

Median orientation of the flexion-extension axes of rotation for the (A) nonimpaired, (B) 4CF, and (C) SE4CF wrists. To allow comparison, the origins of all axes are centered in the same location relative to the radius. Ellipsoid cones represent 95 percent confidence region.
Following 4CF and SE4CF, the optimization solutions for the wrist axes of rotation in the two-revolute joint model are less skewed than those of previously reported for the nonimpaired wrist (Table 2). Specifically, the mean angle (± 95 percent confidence interval) between the flexion-extension and radial-ulnar deviation axes of rotation were 92.6° ± 25.2° and 99.8° ± 22.0° for the 4CF and SE4CF conditions, respectively. Note that 90° falls within both confidence intervals.
The near orthogonality of the modeled wrist axes of rotation following 4CF and SE4CF was dictated by the orientation of the radial-ulnar deviation axis, as no significant differences were found between the orientations of the flexion-extension axes of rotation across the three conditions (Fig. 5). Importantly, the orientation of the radial-ulnar deviation axis of rotation following 4CF was significantly different (p<0.05) than that following SE4CF. The median angle between the radial-ulnar deviation axis in the 4CF and SE4CF wrists is 13.0°, with the orientation of the radial-ulnar deviation axis following SE4CF being directed more ulnarly than that following 4CF (cf., Table 4, x component of radial-ulnar deviation axis is negative and increases in magnitude).
Table 4.
Median Orientation of Axes of Rotation*
| Condition | Flexion-Extension Axis | Radial-Ulnar Deviation Axis | ||||
|---|---|---|---|---|---|---|
| median | 25th percentile | 75th percentile | median | 25th percentile | 75th percentile | |
| Nonimpaired | [0.979, 0.193, −0.067] | [0.959, 0.046, −0.279] | [0.936, 0.322, 0.146] | [0.097, 0.580, 0.809] | [−0.620, 0.266, 0.738] | [0.382, 0.628, 0.678] |
| 4CF | [0.982, 0.187, 0.032] | [0.961, 0.016, −0.277] | [0.899, 0.323, 0.295] | [−0.356, 0.522, 0.775] | [−0.598, 0.448, 0.664] | [−0.137, 0.549, 0.824] |
| SE4CF | [0.995, 0.093, −0.037] | [0.946, −0.237, −0.221] | [0.916, 0.381, 0.127] | [−0.499, 0.375, 0.781] | [−0.672, 0.299, 0.704] | [−0.334, 0.487, 0.807] |
Orientation of axes of rotation reported as unit vectors [x, y, z] in the radius reference frame. Positive values represent the radial, proximal, and dorsal directions. The median, 25th percentile, and 75th percentile were calculated using spherical statistics (Fisher et al., 1987). An illustration of these axis orientations are provided in Figure 4 and Figure 5.
The origin of the flexion-extension axes following 4CF and SE4CF shifted significantly (p<0.05) in the dorsal and proximal directions (Fig. 6, filled circles), when compared to the nonimpaired wrist. Specifically, following 4CF, the median origin of the flexion-extension axis shifted proximally by 0.62 cm and dorsally by 1.00 cm (Table 5). But, following SE4CF, the median location of the origin changed by less than 0.28 cm in the ulnar, proximal, and palmar directions when compared to 4CF. Thus, the axis location changed significantly following fusion of the midcarpal joint, but not following scaphoid removal. No significant differences were found between the origins of the radial-ulnar deviation axes of rotation (Fig. 6, open circles).
Figure 6.

Median location of origin for flexion-extension axis (proximal, filled circles) and radial-ulnar deviation axis (distal, open circles). Lines represent interquartile range.
Table 5.
Median Location of Axes of Rotation (in cm)*
| Condition | Flexion-Extension Axis | Radial-Ulnar Deviation Axis | ||||
|---|---|---|---|---|---|---|
| x | y | z | x | y | z | |
| Nonimpaired | 2.62 [2.25, 2.89] | −24.34 [−24.51, −24.29] | 2.31 [2.17, 2.48] | 3.12 [2.92, 4.87] | −24.55 [−26.37, −24.36] | 1.37 [−1.10, 2.83] |
| 4CF | 2.69 [2.14, 3.03] | −23.74 [−23.83, −23.40] | 3.10 [2.58, 3.71] | 2.97 [2.74, 3.98] | −24.38 [−25.82, −23.95] | 1.72 [0.84, 2.50] |
| SE4CF | 1.79 [1.35, 2.89] | −23.64 [−23.94, −23.31] | 2.88 [2.52, 3.23] | 2.99 [2.08, 3.40] | −25.17 [−26.34, −23.95] | 1.57 [0.63, 2.50] |
Axes are reported in the radius reference frame. Positive values represent the radial, proximal, and dorsal directions. Bracketed values represent 25th and 75th percentile. An illustration of these axis locations are provided in Figure 6.
DISCUSSION
This study demonstrates that both 4CF and SE4CF alter the kinematic coupling of the wrist by imposing axes of rotation that are less skew than those reported for the nonimpaired wrist. Notably, our data suggest this is due to a progressive ulnar shift in the orientation of the radial-ulnar deviation axis of rotation from the 4CF to the SE4CF conditions (Fig 4B&C). Altering the orientation of one axis of rotation without an equivalent alteration to the other axis of rotation may have implications for wrist function, which is known to be limited following SE4CF.
The results of this study will directly benefit investigators interested in examining 4CF and SE4CF and evaluating how surgically altering kinematic coupling at the wrist influences function. For example, our results provide a mechanism to assess the accuracy of previously implemented modeling assumptions,10 such as those prescribing motion following SE4CF using the kinematics of either the proximal or distal carpal row(Fig. 7). Our experimental results suggest that neither of these assumptions fully captures the kinematic changes imposed by SE4CF. Regardless of whether the scaphoid was (SE4CF) or was not excised (4CF), the orientation of the deviation axis of rotation following midcarpal fusion did not match the orientation of either the nonimpaired proximal or distal row identified in previous studies of carpal motion (Fig. 7B compared with Fig. 4B&C). This indicates that the data provided by this study can be used to improve the currently available biomechanical models of 4CF and SE4CF.
Figure 7.
(A) Flexion-extension and (B) radial-ulnar deviation axes of rotation for the nonimpaired proximal (black) and distal row (gray) as previously reported by Nichols et al. 10 These axes were derived from the motion of the lunate (proximal row) and capitate (distal row) reported by Ruby et al.20 For more information on this representation of wrist motion, refer to Nichols et al.10
Our study also affirms that the two-revolute joint model can accurately quantify the position of the hand in space (i.e., global wrist motion, defined as the motion of the hand relative to the forearm), as this model was able to replicate all the tested wrist motions with minimal error (Fig. 3). We interpret this accurate positional tracking of the hand to indicate that a two-revolute joint model of the wrist is adequate for motion capture studies examining gross upper limb movements. This interpretation is consistent with studies validating motion capture marker sets for the upper limb that have demonstrated excellent agreement between wrist joint angles calculated using the two-revolute joint model and measured with a goniometer.13, 14
However, the two-revolute joint model is not a robust model for explicitly identifying axes of rotation in the nonimpaired wrist. Notably, the orientations of the nonimpaired radial-ulnar deviation axes of rotation were highly variable across specimens (Fig 4A), the origins of the nonimpaired axes (Fig 6A) was not consistent with previous studies,4, 24, 25 and one nonimpaired specimen did not reach convergence. The nonimpaired specimen that did not reach convergence may indicate that the optimization routine had difficulty selecting the optimal solution from a group of multiple reasonable solutions; this interpretation is similar to that described by Lewis et al.16 for the ankle joint. We interpret the difficulty achieving convergence in combination with the high across specimen variability and inconsistency of axis origins to indicate that a more complicated model is required to accurately characterize axes of rotation in nonimpaired wrists. For example, a model that incorporates a moving joint center may be more appropriate when explicitly studying nonimpaired wrist motion. This conclusion is consistent with experimental studies that have demonstrated that nonimpaired wrist motion is effectively described using helical axes of rotation.24, 25
Given the high variability of our nonimpaired results, our conclusions that 4CF and SE4CF impose axes of rotation that are closer to orthogonal than those of the nonimpaired wrist are based on comparisons with previous literature.3, 4, 7, 19–22 Regardless of which previous study is used, our conclusions regarding the 4CF and SE4CF wrist are supported. For all studies, the skew orientation of the nonimpaired axes is farther from orthogonal than 92.6° and 99.8°, the skew orientations reported for 4CF and SE4CF, respectively (Table 2). A recent in vivo study by Wolff et al.26 also demonstrates that when compared to healthy controls, kinematic coupling is significantly reduced in SE4CF patients. This conclusion is congruent with the results of this study; a reduction in kinematic coupling is consistent with a reduction in the skew orientation of the axes of rotation.
In this study, we provide evidence that a two-revolute joint model can effectively quantify wrist axes of rotation in surgically altered wrists. Quantifying axes of rotation is fundamental to studying nonimpaired and surgically altered movement. By quantifying the axes of rotation following 4CF and SE4CF, we provide key data necessary for future computational and experimental studies examining these surgeries.
Acknowledgments
Funding: This work was funded by The Searle Funds of the Chicago Community Trust and the National Institutes of Health (NIH T32 HD007418 and NIH F31 AG041627). We thank Medcure for donation of the cadaveric specimens.
We thank Stephen Piazza, PhD for helpful discussions regarding implementation of the optimization routine; Pascal Paschos PhD, for assistance with Northwestern University’s computer cluster; Ajay Balaram, MD and Hilton Gottschalk, MD for assistance with specimen preparation; and Vikram Darbhe, MS and Andrew Lee, BS for building the experimental set-up and assisting with experimental testing, performed at the Musculoskeletal Biomechanics Laboratory at the Edward Hines Jr. VA Hospital.
Footnotes
Conflict of Interest Disclosure: The authors have no conflicts of interest to disclose.
References
- 1.Bain GI, Watts AC. The outcome of scaphoid excision and four-corner arthrodesis for advanced carpal collapse at a minimum of ten years. J Hand Surg Am. 2010;35(5):719–25. doi: 10.1016/j.jhsa.2010.01.025. [DOI] [PubMed] [Google Scholar]
- 2.Crisco JJ, Heard WM, Rich RR, Paller DJ, Wolfe SW. The mechanical axes of the wrist are oriented obliquely to the anatomical axes. J Bone Joint Surg Am. 2011;93(2):169–77. doi: 10.2106/JBJS.I.01222. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Neu CP, Crisco JJ, Wolfe SW. In vivo kinematic behavior of the radio-capitate joint during wrist flexion-extension and radio-ulnar deviation. J Biomech. 2001;34(11):1429–38. doi: 10.1016/s0021-9290(01)00117-8. [DOI] [PubMed] [Google Scholar]
- 4.Sommer HJ, 3rd, Miller NR. A technique for kinematic modeling of anatomical joints. J Biomech Eng. 1980;102(4):311–7. doi: 10.1115/1.3138228. [DOI] [PubMed] [Google Scholar]
- 5.Moritomo H, Murase T, Goto A, Oka K, Sugamoto K, Yoshikawa H. Capitate-based kinematics of the midcarpal joint during wrist radioulnar deviation: An in vivo three-dimensional motion analysis. J Hand Surg Am. 2004;29(4):668–75. doi: 10.1016/j.jhsa.2004.04.010. [DOI] [PubMed] [Google Scholar]
- 6.Garg R, Kraszewski AP, Stoecklein HH, et al. Wrist kinematic coupling and performance during functional tasks: Effects of constrained motion. J Hand Surg Am. 2014;39(4):634–42. e1. doi: 10.1016/j.jhsa.2013.12.031. [DOI] [PubMed] [Google Scholar]
- 7.Li ZM, Kuxhaus L, Fisk JA, Christophel TH. Coupling between wrist flexion-extension and radial-ulnar deviation. Clin Biomech (Bristol, Avon) 2005;20(2):177–83. doi: 10.1016/j.clinbiomech.2004.10.002. [DOI] [PubMed] [Google Scholar]
- 8.Brigstocke GH, Hearnden A, Holt C, Whatling G. In-vivo confirmation of the use of the dart thrower’s motion during activities of daily living. J Hand Surg Eur Vol. 2014;39(4):373–8. doi: 10.1177/1753193412460149. [DOI] [PubMed] [Google Scholar]
- 9.Bland MD, Beebe JA, Hardwick DD, Lang CE. Restricted active range of motion at the elbow, forearm, wrist, or fingers decreases hand function. Journal of hand therapy : official journal of the American Society of Hand Therapists. 2008;21(3):268–74. doi: 10.1197/j.jht.2008.01.003. quiz 75. [DOI] [PubMed] [Google Scholar]
- 10.Nichols JA, Bednar MS, Murray WM. Orientations of wrist axes of rotation influence torque required to hold the hand against gravity: A simulation study of the nonimpaired and surgically salvaged wrist. J Biomech. 2013;46(1):192–6. doi: 10.1016/j.jbiomech.2012.10.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Dvinskikh NA, Blankevoort L, Strackee SD, Grimbergen CA, Streekstra GJ. The effect of lunate position on range of motion after a four-corner arthrodesis: A biomechanical simulation study. J Biomech. 2011;44(7):1387–92. doi: 10.1016/j.jbiomech.2010.12.025. [DOI] [PubMed] [Google Scholar]
- 12.Nichols JA, Bednar MS, Havey RM, Murray WM. Wrist salvage procedures alter moment arms of the primary wrist muscles. Clin Biomech. 2015;30(5):424–30. doi: 10.1016/j.clinbiomech.2015.03.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hillstrom HJ, Garg R, Kraszewski A, et al. Development of an anatomical wrist joint coordinate system to quantify motion during functional tasks. Journal of applied biomechanics. 2014;30(4):586–93. doi: 10.1123/jab.2011-0094. [DOI] [PubMed] [Google Scholar]
- 14.Metcalf CD, Notley SV, Chappell PH, Burridge JH, Yule VT. Validation and application of a computational model for wrist and hand movements using surface markers. IEEE transactions on bio-medical engineering. 2008;55(3):1199–210. doi: 10.1109/TBME.2007.908087. [DOI] [PubMed] [Google Scholar]
- 15.Sobczak S, Rotsaert P, Vancabeke M, Van Sint Jan S, Salvia P, Feipel V. Effects of proximal row carpectomy on wrist biomechanics: A cadaveric study. Clin Biomech (Bristol, Avon) 2011;26(7):718–24. doi: 10.1016/j.clinbiomech.2011.03.002. [DOI] [PubMed] [Google Scholar]
- 16.Lewis GS, Piazza SJ, Sommer IHJ. In vitro assessment of a motion-based optimization method for locating the talocrural and subtalar joint axes. Journal of Biomechanical Engineering. 2006;128(4):596–603. doi: 10.1115/1.2205866. [DOI] [PubMed] [Google Scholar]
- 17.Levenberg K. A method for the solution of certain problems in least-squares. Quarterly Applied Math. 1944;2:164–8. [Google Scholar]
- 18.Marquardt D. An algorithm for least-squares estimation of nonlinear parameters. SIAM Journal Applied Math. 1963;11:431–441. [Google Scholar]
- 19.Kobayashi M, Berger RA, Nagy L, et al. Normal kinematics of carpal bones: A three-dimensional analysis of carpal bone motion relative to the radius. J Biomech. 1997;30(8):787–93. doi: 10.1016/s0021-9290(97)00026-2. [DOI] [PubMed] [Google Scholar]
- 20.Ruby LK, Cooney WP, 3rd, An KN, Linscheid RL, Chao EY. Relative motion of selected carpal bones: A kinematic analysis of the normal wrist. J Hand Surg Am. 1988;13(1):1–10. doi: 10.1016/0363-5023(88)90189-x. [DOI] [PubMed] [Google Scholar]
- 21.Blankenhorn BD, Pfaeffle HJ, Tang P, Robertson D, Imbriglia J, Goitz RJ. Carpal kinematics after proximal row carpectomy. J Hand Surg Am. 2007;32(1):37–46. doi: 10.1016/j.jhsa.2006.10.014. [DOI] [PubMed] [Google Scholar]
- 22.Palmer AK, Werner FW, Murphy D, Glisson R. Functional wrist motion: A biomechanical study. J Hand Surg Am. 1985;10(1):39–46. doi: 10.1016/s0363-5023(85)80246-x. [DOI] [PubMed] [Google Scholar]
- 23.Fisher NI, Lewis TL, Embleton BJJ. Statistical analysis of spherical data. Press Syndicate of the University of Cambridge; Cambridge: 1987. Analysis of two or more samples of vectoral or axial data; pp. 194–229. [Google Scholar]
- 24.Patterson RM, Nicodemus CL, Viegas SF, Elder KW, Rosenblatt J. High-speed, three-dimensional kinematic analysis of the normal wrist. J Hand Surg Am. 1998;23(3):446–53. doi: 10.1016/S0363-5023(05)80462-9. [DOI] [PubMed] [Google Scholar]
- 25.Salvia P, Woestyn L, David JH, et al. Analysis of helical axes, pivot and envelope in active wrist circumduction. Clinical biomechanics (Bristol, Avon) 2000;15(2):103–11. doi: 10.1016/s0268-0033(99)00055-8. [DOI] [PubMed] [Google Scholar]
- 26.Wolff AL, Garg R, Kraszewski AP, et al. Surgical treatments for scapholunate advanced collapse wrist: Kinematics and functional performance. J Hand Surg Am. 2015 doi: 10.1016/j.jhsa.2015.04.035. [DOI] [PubMed] [Google Scholar]