

Abstract
Pulmonary hypertension significantly changes biventricular anatomy and physiology, frequently evolving to clinical deterioration and right ventricular failure. The case of a woman developing atrial arrhythmias complicating dipyridamole stress in concomitance with scintigraphic “D-shaped” left ventricle is briefly reported. Although rare, our finding may suggest that nonselective vasodilators should be used with caution in this clinical setting.
Keywords: Arrhythmias, “D shaped”, pulmonary hypertension
Introduction
Pulmonary hypertension (PH) determines dramatic biventricular remodeling and several physiological modifications of right ventricular function.[1] In atrial septal defect (ASD), moderate/severe PH frequently marks an elevated risk of supraventricular tachyarrhythmias as atrial flutter, atrial fibrillation, and atrioventricular nodal reentry tachycardia.[2] The development of these arrhythmias is frequently accompanied by clinical deterioration and right ventricular failure.[3]
We describe the development of unusual fast supraventricular arrhythmias complicating vasodilator stress in concomitance of scintigraphic “D-shaped” left ventricle (LV), highlighting that dipyridamole should be used with special caution in this clinical context.
Case Report
A 77-year-old hypertensive woman with noncorrected ASD (ostium secundum) and moderate PH was referred to vasodilator stress Tc-99m sestamibi gated-single-photon emission computed tomography (SPECT) (2 days stress/rest protocol) due to nonanginal chest pain superimposed to class III dyspnea. She was under aspirin, losartan, and atenolol after previous nonembolic recurrent episodes of atrial flutter. Atenolol was discontinued 48 h before stress. Laboratory tests were normal.
After dipyridamole infusion (0.56 mg/kg), the patient installed tachycardia-dependent left bundle branch block followed by atrial flutter at 175 bpm (A) and atrial fibrillation 2 min after aminophylline administration [Figure 1]. Standard loading dose of amiodarone was then required. Poststress nongated SPECT images revealed marked right ventricle enlargement and “D-shaped” LV [Figure 2]. LV perfusion was normal.
Figure 1.

Atrial arrhythmias during vasodilator stress. Electrocardiogram tracings obtained at baseline (panel a), during atrial flutter (b), and fast atrial fibrillation (2 min after aminophylline, c). Left bundle branch block morphology with no R-wave progression through chest leads denoted counterclockwise rotation of the heart in horizontal plane
Figure 2.
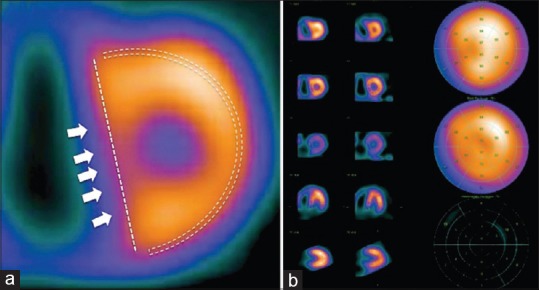
Scintigraphic “D-shaped” sign. (a) “D-shaped” left ventricle morphology (dotted-line contour) with flattening and stretching of interventricular septum (white arrows) and slightly decreased septal uptake. (b) No perfusion defects
Discussion
“D-shaped” remodeling of LV has been extensively described in acute or chronic right ventricle overload,[4] although data refer almost exclusively to echocardiographic examination.[5,6] In fact, most information about this anatomical finding in myocardial scintigraphy is limited to isolated reports and small case series.[7,8] In an observational retrospective report, Movahed et al. found that “D-shaped” LV in SPECT imaging correlated well with right ventricle overload; a history of ASD was found in 38% of this sample.[9]
It is difficult to find a plausible mechanism explaining electrical complications induced by dipyridamole in the clinical setting we described. In fact, an increase in intracellular adenosine levels is more likely to reduce the occurrence of atrial arrhythmias instead of precipitating it, there were no ionic or metabolic disorders, and perfusion imaging tended to exclude important potential ischemia as a precipitating event. However, we cannot exclude the possibility that beta-blockers discontinuation could have played an important role in the development of arrhythmias.
As phenotypic predisposition to electrical complications during vasodilator stress in patients exhibiting scintigraphic “D-shaped” LV is still unknown, inverted (rest-stress) protocol could not be systematically indicated in all patients with PH derived to SPECT. Safety profiles of dipyridamole, adenosine, and new selective A2A-receptor agonists (e.g., regadenoson) should be compared in patients with PH derived to myocardial perfusion imaging.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Hopkins WE. Right ventricular performance in congenital heart disease: A physiologic and pathophysiologic perspective. Cardiol Clin. 2012;30:205–18. doi: 10.1016/j.ccl.2012.03.006. [DOI] [PubMed] [Google Scholar]
- 2.Olsson KM, Nickel NP, Tongers J, Hoeper MM. Atrial flutter and fibrillation in patients with pulmonary hypertension. Int J Cardiol. 2013;167:2300–5. doi: 10.1016/j.ijcard.2012.06.024. [DOI] [PubMed] [Google Scholar]
- 3.Perloff JK. Survival patterns without cardiac surgery or interventional catheterization: A narrowing base. In: Perloff JK, Childs JS, editors. Congenital Heart Disease in Adults. 2nd ed. Philadelphia: W.B. Saunders; 1998. pp. 15–53. [Google Scholar]
- 4.Mitoff PR, Beauchesne L, Dick AJ, Chow BJ, Beanlands RS, Haddad H, et al. Imaging the failing right ventricle. Curr Opin Cardiol. 2012;27:148–53. doi: 10.1097/HCO.0b013e32834fec4e. [DOI] [PubMed] [Google Scholar]
- 5.Moceri P, Baudouy D, Chiche O, Cerboni P, Bouvier P, Chaussade C, et al. Imaging in pulmonary hypertension: Focus on the role of echocardiography. Arch Cardiovasc Dis. 2014;107:261–71. doi: 10.1016/j.acvd.2014.02.005. [DOI] [PubMed] [Google Scholar]
- 6.Mazurek JA, Forfia PR. Enhancing the accuracy of echocardiography in the diagnosis of pulmonary arterial hypertension: Looking at the heart to learn about the lungs. Curr Opin Pulm Med. 2013;19:437–45. doi: 10.1097/MCP.0b013e3283645966. [DOI] [PubMed] [Google Scholar]
- 7.Shih WJ, Kousa K, Mitchell B, Huang WS. Permanently increased brightness of right ventricle (D-shaped left ventricle) on myocardial perfusion imaging in a patient with chronic cor pulmonale: An autopsy correlation. J Nucl Cardiol. 2006;13:294–6. doi: 10.1007/BF02971253. [DOI] [PubMed] [Google Scholar]
- 8.Murarka S, Movahed MR. Review of Movahed's sign (D shaped left ventricle seen on gated SPECT) suggestive of right ventricular overload. Int J Cardiovasc Imaging. 2010;26:553–7. doi: 10.1007/s10554-010-9600-9. [DOI] [PubMed] [Google Scholar]
- 9.Movahed MR, Hepner A, Lizotte P, Milne N. Flattening of the interventricular septum (D-shaped left ventricle) in addition to high right ventricular tracer uptake and increased right ventricular volume found on gated SPECT studies strongly correlates with right ventricular overload. J Nucl Cardiol. 2005;12:428–34. doi: 10.1016/j.nuclcard.2005.04.004. [DOI] [PubMed] [Google Scholar]