

Abstract
Aim
To report a study protocol that examines the impact of adding salient cues within a virtual reality simulation of a senior residential building on wayfinding for older adults with and without Alzheimer’s disease.
Background
An early symptom of Alzheimer’s disease is the inability to find one’s way (wayfinding). Senior residential environments are especially difficult for wayfinding. Salient cues may be able to help persons with Alzheimer’s disease find their way more effectively so they can maintain independence.
Design
. A repeated measures, within and between subjects design.
Methods
This study was funded by the National Institutes of Health (August 2012). Older adults (n=40) with normal cognition and older adults with early stage Alzheimer’s disease/mild cognitive impairment (n=40) will try to find their way to a location repeatedly within a virtual reality simulation of senior residence. There are two environments: standard (no cues) and salient (multiple cues). Outcome measures include how often and how quickly participants find the target location in each cue condition.
Discussion
The results of this study have the potential to provide evidence for ways to make the environment more supportive for wayfinding for older adults with Alzheimer’s disease. This study is registered at Trialmatch.alz.org (Identifier 260425-5).
Keywords: Alzheimer’s disease, mild cognitive impairment, wayfinding, aging, virtual reality, eye tracking, repeated measures, environment, nursing, repeated measures
INTRODUCTION
Alzheimer’s disease (AD) affects one in three older adults, and is one of the top 10 causes of death (Alzheimer’s Association, 2015). The disease begins with cognitive difficulties including memory loss, and progresses over a period of time to complete loss of mental and physical abilities. One of the most distressing symptoms of the disease is the problem of getting lost. In order to keep from getting lost, people must be able to successfully navigate from one place to another; an ability known as wayfinding (Passini et al. 2000). Up to 55% of persons with early stage AD have difficulties wayfinding (Chiu et al. 2004, deIpolyi et al. 2007, Rowe 2003) with up to 30% of those individuals having such problems getting lost that they cannot drive or live independently. Problems wayfinding can cause distress and fear (Chiu et al. 2004; Tu & Pai 2006) and may lead to severe injury or death if individuals leave their homes and cannot find their way safely back (Rowe 2003). In AD, getting lost is a serious problem because those with this condition may lack the cognitive resources to figure out what to do once they become lost (Chiu et al. 2004, Pai et al. 2012, Tu & Pai 2006).
Built environments that are frequented by older adults, such as senior residential environments and hospitals, are often poorly designed for wayfinding, with nondescript hallways and confusing or inadequate environmental information (Passini et al. 2000, Passini et al. 1998). In fact, persons with AD who live in assisted living have been shown to have problems finding their room, the bathroom, activity areas, and the dining room (Caspi, 2014), which are key to meeting the fundamental need of sleep, food, and socialization. Thus, problems with wayfinding can affect comfort, function, and quality of life.
Background
Wayfinding problems in AD have been linked to changes within the hippocampus and related structures, including senile plaques, neurofibrillary tangles and neuron loss. These changes have been found to be related to wayfinding deficits that commonly occur even in the earliest stages of AD (Yew et al. 2013). Persons with AD have been shown to have deficits in many functions essential to wayfinding, such as learning routes (Rainville et al. 2001), recalling landmarks, and in remembering the sequence of landmarks in a route (Jheng & Pai 2009, Kalová et al. 2005, Kavcic & Duffy 2003, Kavcic et al. 2006). People with early stage AD have also demonstrated difficulty in learning and wayfinding in new environments (Chiu et al. 2004, Cushman et al. 2008, Monacelli et al. 2003).
Cues, or pieces of sensory information in the environment, are necessary for effective wayfinding as they help to distinguish one place from another and provide a reference point to remember one’s location (Caduff & Timpf 2008). In sighted people, visual cues have been shown to overwhelmingly predominate in importance (Gunther et al. 2004). Since learning every visual element in the environment would be a costly and inefficient use of memory, only certain cues are attended to and used in wayfinding tasks (Ohm et al. 2014). Visual cues have properties such as size, stability, number, and appearance that enable them to be perceived and selected in place learning. These factors can affect how well people pay attention to cues, and how well they can encode them into a cognitive map or routes. Salience, or the ability of a cue to attract an individual’s attention, refers to the distinctiveness of the cue (Caduff & Timpf 2008). In the natural world, a wide variety of salient visual cues are present to help people in wayfinding tasks. Achieving salience in built environments is a difficult task due to the architectural design, limited viewing range, and similarity of design features most often seen. In senior living environments such as assisted living residences and skilled nursing facilities, a lack of salient features is common and contributes to wayfinding problems (Passini et al. 1998).
Studies using cues to enhance wayfinding in persons with AD have been done in institutional settings focusing on people in the moderate to severe stages of the disease. Two studies have shown that adding familiar items such as personal photographs or memorabilia outside of the residents’ rooms can enhance room recognition in people with AD (Namazi et al. 1991, Nolan et al. 2002). Other studies have shown that bright, high contrast color can enhance object recognition and recall of objects (Cernin et al. 2003, Wood et al. 1997). Color has also been identified in one study as being a primary cue to help people with dementia recognize their location (Gibson et al. 2004, Cooper 1985). These studies suggest that salient cues may be able to help individuals with AD find their way in the built environment.
Theoretical Framework
Lawton and Nahemow’s (1973) Environmental Press model proposes that behavior is a result of an interaction between individual competence, which is the capability to perform a desired activity, and environmental press, or the demands of the environment. When environmental press exceeds competence in a given area, individuals can become overwhelmed and not function to their fullest ability. If the environment can be made more supportive of the abilities of the user, function can be enhanced.
In this research study, older individuals, especially those with AD, have a decreased competence in wayfinding ability due to changes in place learning ability and visual attention (Figure 1). The environment in senior living facilities often has increased environmental press, due to long confusing hallways and lack of salient cues. The physical environment can be enhanced by adding salient cues, which would then lead to decreased press and increased competence in wayfinding. Thus, modifying the environment to better match the abilities of the individuals who are older and have cognitive impairment can improve wayfinding. The effect of environmental modifications – specifically the addition of salient environmental cues – is to support wayfinding in those with decreased competence due to AD.
Figure 1. An Adaptation of The Environmental Press Model for Wayfinding Performance.
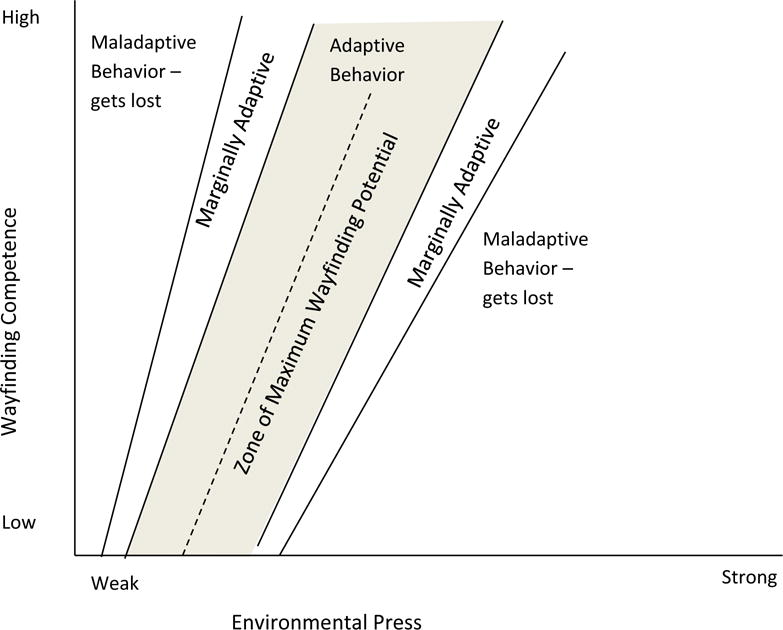
Note: Adapted with permission from Lawton M., & Nahemow L. (1973). Ecology and the aging process. In C. Eisdorfer & M. P. Lawton (Eds.), Psychology of Adult Development and Aging (pp. 619–674). Washington D.C.: American Psychological Association. In this model, environmental press is the complexity or demands of the environment, which is on a continuum from weak to strong. Persons with AD/MCI often have decreased wayfinding competence. By adding cues we propose to enhance wayfinding competence by decreasing environmental press. Environmental press can be seen as too weak; which may decrease engagement; or too strong or complex, which may be overwhelming for a person with decreased competence.
Another theory that influenced how we determined to make the environment more supportive of wayfinding is Caduff and Timpf’s (2008) Cue Salience theory. They propose that in order for individuals to use wayfinding cues, they must first visually attend to the cue after selecting it from other environmental information, focus on it, and store its attributes into memory (Caduff & Timpf 2008). People must allocate mental resources to specific environmental features – using selective attention as they are unable to attend to all information in the environment (Kirasic et al. 1992). Selective attention can be influenced by the color, form, or location of objects (exogenous guidance); or by an individual’s current goals or a priori experience (endogenous guidance) (Caduff & Timpf 2008). Eye movements are controlled by either exogenous or endogenous guided attention processes, and include saccades and eye fixations. During saccades, the eyes scan the environment. When visual fixation occurs, the eyes focus on specific environmental information which can then be processed. In complex environments, the environmental information must be sorted through or visually searched in order to locate informative cues. When selective attention is focused on a particular part of the environment, other less important environmental information is suppressed, involving inhibitory processes. The attention resources of the individual and the complexity of the environment determine the demand of the task (Caduff & Timpf 2008). Our previous studies have supported Caduff & Timpf’s theory, in that cues that are colorful and familiar (easily identified) are salient for older adults in wayfinding tasks (Davis et al. 2008, 2009, Davis & Therrien 2012). To date, there have been no known studies that have examined the effect of cue salience on wayfinding in persons with AD.
THE STUDY
Aims
The aims and hypotheses of the study include the following.
Aim 1: To examine the effect of salient visual cues on wayfinding performance initially and over time in older adults with and without AD.
Aim 2: To describe the visual tracking of cues and self-reported wayfinding strategies used by older adults with AD compared to those with normal cognition; and determine how these relate to wayfinding performance.
Hypotheses
We hypothesize that:
Salient visual cues will be supportive of improved wayfinding performance when compared with standard cues in a virtual reality environment.
Participants with early stage AD will have impaired wayfinding performance under standard and salient cue conditions when compared to those without early stage AD.
The magnitude of difference in wayfinding performance between the salient versus standard cue conditions will be greater in participants with early stage AD than those with normal cognition.
Design/Methodology
This study (funded August 2012) will use a within and between participants experimental design. Wayfinding performance will be compared between two wayfinding tasks in a virtual reality environment called the Virtual Senior Living (VSL). Participants will be tested in two cue conditions; CC1 (no cues) and CC2 (salient cues). Wayfinding performance will be compared among participant groups (control and AD) and cue conditions. The participants will wear eye tracking glasses during the VSL task that will record their eye gaze. They will be tested repeatedly over 5 learning trials in each cue condition for 2 consecutive days so environmental learning over time can be measured. In addition, they will complete several other quantitative tests for cognitive ability (working memory and general cognition) and scales that assess self-reported wayfinding strategies and wayfinding anxiety.
Participants
The convenience sample will be comprised of two groups (1) 40 adults aged ≥ 62 who have normal cognition (Control group); and (2) 40 adults aged ≥ 62 who have early stage AD or mild cognitive impairment (MCI) due to AD (AD/MCI group). A power analysis from a previous study (Davis & Therrien 2012) informed the sample size. Subjects will be recruited from memory clinics, senior residential facilities, senior groups, the Alzheimer’s Association, and an existing database of older adults who wish to participate in research. Inclusion and exclusion criteria are listed in Table 1. Initially, we were intending only to include individuals only with early stage AD; however in 2011, recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease added a category of the disease indicating very early AD (MCI due to AD) (Albert et al. 2011). Since wayfinding problems have been shown to occur early in the disease, we included this category which also has the benefit of broadening our recruiting pool.
Table 1.
Inclusion and Exclusion Criteria
| Inclusion Criteria |
|---|
|
|
Exclusion Criteria |
|
Data Collection and Study Procedures
For an overview of the study procedures, see Figure 2. A nurse will meet with the potential participants and their significant other and explain the study. The National Institutes of Health (NIH; 2009) recommends formally assessing consent capacity in persons with diminished or questionable cognitive abilities. Consent capacity is defined as “an adult’s ability to understand information relevant to making an informed, voluntary decision to participate in research” (NIH 2009, section Scope, para. 1).
Figure 2. Overview of Study Protocol.
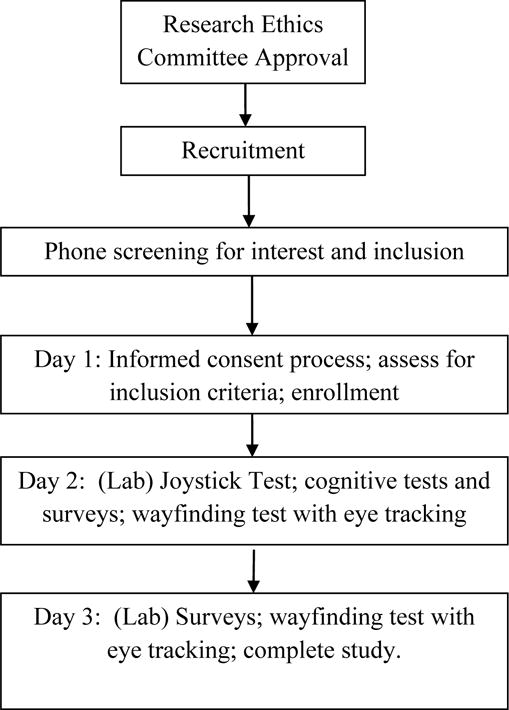
Note: Days 2 and 3 will be consecutive and will occur within 2 weeks of day 1.
In this study, since prior research has indicated that 40% of persons with early stage AD/MCI may not have consent capacity (Kim et al. 2001), the Evaluation to Sign Consent Measure (ESC; Resnick et al. 2007) will be used to assess persons with AD/MCI’s consent capacity (Table 2). The ESC was designed as a five question interview to determine if potential subjects have a sufficient factual understanding of requirements of participation in a proposed study in order to give informed consent. One question in the ESC relates to how the groups or randomization occurs; since our study does not have randomization this question will not be asked. Capacity to give consent is defined as the ability of the subject to correctly answer all four items of the ESC correctly. If the participants answer the questions appropriately, they will be determined as having sufficient understanding of the study to give consent, and they will be asked to sign the consent form. If the participants are unable to answer all of the questions from the ESC correctly, they will be identified as possibly lacking sufficient understanding of the study to give consent (Resnick et al. 2007). They will then be asked if they wish to participate (assent), and if they agree, the research assistant will explain the study fully to the legal guardian or closest relative (if no formal legal guardian has been appointed), and ask if he or she would be willing to sign a consent form. Based on this evaluation, the participant will either give informed consent or assent; or a decision maker for the participant will give consent for the subject to participate if needed.
Table 2.
Evaluation to Sign Consent Measure
| Question | Acceptable Response |
|---|---|
| 1. What are two potential risks? | Getting tired (fatigue), dizzy, nauseated, frustrated, anxious |
| 2. What is expected from you in this study? | Answering questions, computer, finding my way, doing my best, use joystick |
| 3. What if you don’t want to continue? | Ask to stop, tell someone |
| 4. What if you experience discomfort? | Tell someone, ask to stop, say something |
Note: The researcher will explain the study to the research participant and ask each question. Participants who are unable to answer any question will not demonstrate sufficient understanding of the study to give consent (Resnick et al.2007).
Then, the screening tests will be administered to determine if the participants meet the inclusion criteria (Table 1). In addition, for those in the AD/MCI group, a HIPAA release form will be given in order to obtain confirmation of their diagnosis by their treating health care provider. Then, an appointment will be set up with the participant within the next two weeks for the wayfinding portion of the study.
On day 2 of the study, participants will report to the laboratory at the university. After completing several cognitive tests and surveys, the participants will move on to the wayfinding portion of the study. They will be fitted with eye tracking goggles and the goggles will be calibrated. Then, after training them on the use of a joystick, they will take a timed joystick test in which the participant must demonstrate proficiency to continue in the study. Finally, they will then be asked to find their in a virtual reality simulation called the Virtual Senior Residence (VSL). After completing this part of the testing, they are done for the day.
The next day (day 3) participants will report to the same location as day 2, and complete some additional brief surveys and repeat the eye tracking and wayfinding portion of the study. After this, participation in the study is completed. Participants in the study will receive a $20 gift card for each day or partial day of participation (a total of $60 if they complete all 3 days).
Instruments and Measures
See Table 3 for an overview of the study variables and measures. Computer experience will be assessed using the Computer Use Survey (Moffat et al. 2001). This survey asks participants to rate their experience using a computer, playing computer games, and playing computer games that involve virtual reality technology. Each item is rated on a 0 – 7 scale for a possible total score of 0 – 21 points. Our previous analysis of the tool showed a Cronbach’s alpha for the instrument of .70. Working memory will be assessed using the Digit Span tests (Weschler 1987). In the Digit Span Forward test, participants are asked to repeat an increasingly larger series of numbers. In the Digit Span Backward test, participants repeat the numbers in reverse order. Normal scores for the DSF test are > 5 and > 4 for DSB. Test-retest reliability of the digit span tests range from .66–.89 (Lezak 1995). Cognitive status will be further assessed using the Montreal Cognitive Assessment (MoCA). The MoCA is a 10 minute, 30 point instrument that tests short term memory recall, visual-spatial abilities, executive functioning, attention, concentration and working memory, language, and orientation. The measure has good reported internal consistency (α =.83) and excellent sensitivity for identifying MCI and early dementia (Nasreddine et al. 2005, Smith et al. 2007).
Table 3.
Summary of Measures
| Dependent Variables | Measure/Indicator | Data | Schedule |
|---|---|---|---|
| Wayfinding performance | Virtual Senior Living data |
|
Day 2, 3 |
| Wayfinding Strategies | Wayfinding strategy scale | Score | Day 1 and 3* |
| Independent Variables | |||
| Presence of early stage AD | HCP report, Clinical Dementia Rating Scale |
|
Day 1 |
| Cue Condition | VSL |
|
Day 2, 3 |
| Visual Attention to cues | Eye Tracker Data/Fixations |
|
Day 2, 3 |
| Influencing Variables | |||
| Demographics | Demographic survey |
|
Day 1 |
| Working memory | Digit Span Test | Score of Digit Span Forwards and Backwards | Day 1 |
| Computer Experience | Computer Use Survey |
|
Day 1 |
| Wayfinding Anxiety | Lawton’s Spatial Anxiety Scale |
|
Day 1* |
| Cognition | Montreal Cognitive Assessment |
|
Day 2 |
Note: Since the Wayfinding Strategies Scale and The Spatial Anxiety Scale have not been tested in persons with dementia, we will test participants on day 1 and 3 to determine test – retest reliability.
Anxiety about wayfinding will be measured using Lawton’s Spatial Anxiety Scale. This scale lists eight wayfinding tasks that may produce anxiety in some individuals, such as finding their way in a new place for the first time (Lawton & Kallai 2002). Participants rate their anxiety on a 5-point Likert type scale ranging from “not at all anxious” to “very anxious” which are summed for a total wayfinding anxiety score. Principal components analysis of the items showed that all factors loaded on one factor (alpha coefficient .87) (Lawton & Kallai 2002).
The Virtual Senior Living (VSL) is a recently developed, computerized, 3-dimensional computer simulation of a continuing care retirement home which is comprised of multiple corridors and choice points. The VSL is displayed by a computer and projected on a 12 foot rectangular screen. Participants can virtually move about the VSL using a joystick, so that they have complete ability to move in any direction within the computerized environment. The size of the screen adds depth and dimension to the display. This method of VR was chosen to minimize side effects that are seen in more immersive VR such as head mounted displays which can induce simulation sickness and discomfort from wearing the equipment. In addition, this method of VR provides a life like rendition of the environment by increasing size, surround, and presence (Sherman & Craig 2003).
The VSL was modeled after an existing continuing care retirement home for this study by the University of Michigan 3-D laboratory. The VSL has 2 environmental tasks – standard and salient. Both routes are the same length from the start points, and have the same number of decision points (potential turns to other hallways). Participants will be tested for 5 consecutive trials in each condition for 2 days in a row which will be alternated between participants to reduce the effect of testing. The cue conditions have the following features: 1) the standard condition (CC1) is depicted as the typical senior living facility with few salient cues (Figure 3) and 2) the salient condition (CC2) which is similar environment, yet has 10 high contrast, large, and colorful cues placed at key decision points along the route (Figure 4). The cues are familiar objects, such as a flag, picture of children, bright balloons, flower wall hanging, and cardinal wall hanging. Participants will find their way to a dining room in CC1; and doors which lead outside in CC2. The order of testing (CC1 and CC2) reversed for each subject on the next day of testing.
Figure 3.

Standard Cue Condition in the Virtual Senior Living
Figure 4. Salient Cue Condition in the Virtual Senior Living.

Note: The pictures in the VSL are bright and colorful; the cardinal is bright red; and the lion yellow and black
The output from the VSL allows for several different measures of wayfinding performance. This includes: 1) the length of time in seconds it takes the subject to get from the starting point to the goal location (as people learn the environment, they should arrive at the goal location quicker); 2) wayfinding errors, which occur when the individual makes a wrong turn or misses a turn in the route; and 3) the length of the path taken in VSL units (a longer path length means that the subject took a longer or less direct route to find the goal location). These measures are typical measures of wayfinding ability (Moffat & Resnick 2002).
The Wayfinding Strategy scale (Lawton 1994, Lawton & Kallai 2002) is a 17 item scale that asks participants to rate their use of specific strategies while finding their way in a city, town or building, such as keeping track of direction, using the sun, using reference points such as landmarks, or relying on signage. Participants rate their responses for each item on a 5 item Likert scale. Identified questions are summed to give scores for both orientation (spatial strategies using cues whereby the individual remains oriented to the spatial environment) and route wayfinding strategies (use of maps or signage, whereby the person uses point-by-point aids). This tool has been designed for use across cultures and has been tested in an American and Hungarian samples, with alpha coefficients for the orientation items of .79; and .70 for the route items (Lawton & Kallai 2002).
Visual attention to cues will be measured by the use of eye tracking glasses, which are lightweight glasses that contain a small video camera and an optical device that tracks eye movements using pupil-corneal reflection, with visual range of 50 degrees horizontal and 40 degrees vertical. The eye tracker can be worn over existing eye glasses, is not restrictive to head movement, and weighs less than 3 ounces. The output from the eye tracker is a video recording of the visual scene, superimposed with the eye gaze (cross hairs) so that the exact movement of the eyes during the virtual navigation is recorded (Applied Science Laboratory, n.d.). For this study, visual attention will be defined as 1) the amount of time in 1/100 seconds spent gazing at each visual cue in both the standard and salient conditions; and 2) the number of visual gazes to each cue versus other environmental features. Fixations will be defined as the eye tracker cross hairs on the cue for at least 0.5 second or 15 frames.
Data Analysis
The data will be de-identified and coded to provide anonymity. It will be entered into a statistical program, cleaned, and assessed for missing data. Participant attrition and side effects will be monitored during testing. Participants who withdraw will be compared to those who do not. Data analysis will be done using the Statistical Package for Social Sciences (SPSS) version 20.
The main focus of our analysis will be to determine how wayfinding competency is affected by the presence of environmental cues (environmental press). For Specific Aim 1, the dependent variables of wayfinding performance (or competence), including how fast and how often subjects find the goal locations, and wayfinding errors, will be analyzed using linear mixed modeling (LMM). This type of analysis models the fixed effects of both within-subject factors (time) and between-subject factors (group) in a repeated measures data set along with other variables such as age, computer experience, etc. This allows for estimation of unexplained between-subject variance that is not accounted for by between-subject factors via the inclusion of random subject effects. Also, it allows for the modeling of nonlinear changes in the dependent variables (Krueger & Tian 2004). Most importantly, LMM emphasizes individual differences, which is appropriate for this study. LMM can be thought of as linear regression modeling, with the additional flexibility of modeling between-subject variance via the inclusion of random subject effects. Main effects and two and three-way interactions between the independent variables will be estimated and tested for significance in each model. In addition, possible non-linear (i.e., quadratic and cubic) trends in the dependent variables as a function of day of testing will be investigated, based on initial exploratory analyses of the results. Based on the overall significance (F-test) of each term in the model, selected terms will be removed one at a time, starting with the higher-order interactions, until the most parsimonious model with all terms significant is achieved. Significance of fixed effects and the model as a whole is set at p < .05.
For the eye tracking analysis (Specific Aim 2), descriptive data regarding the number and length of times spent fixating on each identified cue in both cue conditions will be calculated for each subject. T-tests will be used to compare differences between individuals with AD and the control group to determine differences in fixations between the groups on each cue. In addition, total fixation time on cues will be compared with total time in each trial to determine if time spent fixating on any cues is the same between groups. The eye tracking data will give important information about the usefulness of the cues for persons with and without AD/MCI in decreasing environmental press. Cue fixation time that correlates with improved wayfinding performance will give important information about the types, placement, and frequency of cues that improves wayfinding.
A part of Specific Aim 2 was to determine if wayfinding strategies differ between the groups. To meet this aim, the mean scores on the Wayfinding Strategy Scale will be compared among groups using the Mann-Whitney U test. This will help us determine if persons with AD/MCI use different types of strategies than those without this disease.
Ethical Considerations
This study was approved in August 2011 by the university research ethics committee (12–13-H) and hospital research ethics committee (SM11-0720-02). The research staff will explain the study to all participants and significant others, and obtain signed informed consent and verbal assent (if consent capacity is not present). Participants will be informed that they can withdraw from the study at any time, that their data will be de-identified and only presented in aggregate form, and that their data will be kept secure. Since the study involves research participants who are vulnerable due to cognitive impairment, the researchers have clear protocols and are trained to assess for any signs that the participant may want to withdraw. In addition, assent will be confirmed with the participant each day of the study since the participants may not recall the informed consent process. Although this is a low risk study, any problems or adverse events will be reported to the principle investigator. If necessary, the IRB’s will be notified and the protocols will be revised to reduce any risks.
Validity and Reliability
All study staff will receive extensive training in data collection. Interrater reliability will be attained on scoring tests such as the CDR and MoCA. Detailed data collection protocols have been developed and will be practiced by all data collectors. The study protocol will be monitored by the project director for study fidelity. All data will be reviewed by the project director immediately after data collection to review it and make sure it is collected according to procedures, with any variance in procedures addressed.
The use of VR simulated environments has been validated as a way to measure wayfinding for all ages and in people with cognitive disorders. For example, wayfinding ability in virtual reality environments has been shown to translate into knowledge and wayfinding performance of the same environment in the real world (Blackman et al., 2007; Foreman et al., 2000). VR wayfinding tasks are shown to be sensitive to age related changes, with older adults showing impaired performance when compared to younger adults as seen in real world wayfinding tests (Foreman et al. 2005; Moffat et al. 2001; Thomas et al. 2001). VR environments are beginning to be used successfully to test wayfinding in people with varying stages of dementia (Blackman et al. 2007; Flynn et al. 2003, Zakzanis et al. 2009). Our research team’s previous work has used VR environments successfully as a novel way to test the effects of different qualities of cues in spatial learning of environments in older adults (Davis et al. 2008, 2009, Davis & Therrien 2012).
The use of VR has several advantages over the real world. Real world environments change depending upon the lighting and distractions such as people, noise, and human manipulation. VR environments allow each subject to be tested in exactly the same condition. In VR environments, the researchers can isolate, as much as possible, the effect of the independent variables on the dependent variables of interest, with less influence from extraneous factors. VR environments allow older adults to participate even if they have mobility problems, without fear of exertion or injury. The VR methodology is a logical method to use as a precursor to real world intervention studies.
DISCUSSION
Although wayfinding problems are identified as a hallmark sign of AD even early in the disease (Jheng & Pai 2008, Uc et al. 2004), there is little known about ways to address this problem. Most of the current studies are small case studies, involving later stage dementia (Passini et al. 2000). These studies have shown an improvement in certain aspects of wayfinding, such as recognizing one’s own room, when cues such as pictures of the resident are placed outside of the room (Nolan et al. 2002). Unfortunately, in order for these interventions to be helpful individuals must have a general idea of where their room is located. This study seeks to investigate ways to improve environments for wayfinding, such that individuals know where they are and can more easily find their way to desired locations. This study is significant because the current status of most senior residential environments is not supportive of wayfinding, with long, non-distinctive hallways and equally spaced doors, and insufficient environmental information to distinguish one area from another. Improving environments for wayfinding has the potential to decrease anxiety and improve comfort and quality of life in persons with dementia.
VR is an ideal and innovative medium to test our hypotheses. The VSL mimics real world wayfinding tasks because participants can move about the environment, change speed, see 360 degrees around them, and alter perceptual perspective as if in a real environment. At the same time, VR allows older adults with mobility and endurance problems to be tested safely and repeatedly. The proposed study provides a true experimental environment in which we can test the impact of salient environmental cues on wayfinding in a virtual reality environment. Thus, this study proposes to use two novel methods – VR and eye tracking - that will give important information about how older adults with and without AD use cues to find their way in environments. This study provides the basis for further studies, systematically building evidence for specific environmental interventions to improve wayfinding.
Limitations
One limitation of this study is that it is being conducted in VR, which is different than the real world. Even though VR tests have been established as a valid measure, it will be important to replicate the findings in a real world environment to assure their usefulness as an intervention.
CONCLUSION
The results of this study can inform practice and research. In the practice arena, the use of salient environmental cues has the potential to help older adults with AD find their way more effectively. If the environment can be made to be more supportive of persons for wayfinding, it may be possible to improve their interaction with the environment and engagement. In addition, this study will provide new understanding of how persons with AD use environmental cues and how visual attention to cues is different in persons with AD when compared to those without the disease, which can inform interventions and future research.
Summary Statement.
Why is this study needed?
Persons with Alzheimer’s disease often have problems wayfinding.
There is little evidence for ways in which to enhance the design of built environments.
The use of salient visual cues may help older adults with and without Alzheimer’s disease to find their way more effectively.
Acknowledgments
Research reported in this publication was supported by the National Institute On Aging of the National Institutes of Health under Award Number R15AG037946. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Additional funding was received by Grand Valley State University and Sigma Theta Tau (Kappa Epsilon Chapter).
Footnotes
Conflict of Interest Statement: No conflict of interest has been declared by the authors.
Contributor Information
Rebecca DAVIS, Professor, Kirkhof College of Nursing, Grand Valley State University.
Jennifer OHMAN, DNP Student, Kirkhof College of Nursing, Grand Valley State University.
References
- Albert M, DeKosky T, Dickson D, Dubois B, Feldman H, Fox C, Gamst A, Holtzman D, Jagust W, Petersen R, Snyder P, Carrillo M, Thies B, Phelps CH. The diagnosis of mild cognitive impairment due to Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimer’s & Dementia. 2011;7(3):270–279. doi: 10.1016/j.jalz.2011.03.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Applied Science Laboratory (ASL) Choosing an eye tracking system. n.d. Retreived from http://delarosaresearch.com/uploads/ASL_Choosing_an_Eye_Tracking_System_brochure_10.08_1_.pdf.
- Blackman T, Van Schaik P, Martyr A. Outdoor environments for people with dementia: An exploratory study using virtual reality. Ageing and Society. 2007;27(06):811–825. doi: 10.1017/s0144686x07006253. [DOI] [Google Scholar]
- Caduff D, Timpf S. On the assessment of landmark salience for human navigation. Cognitive Processing. 2008;9(4):249–267. doi: 10.1007/s10339-007-0199-2. [DOI] [PubMed] [Google Scholar]
- Caspi E. Wayfinding difficulties among elders with dementia in an assisted living residence. Dementia-International Journal of Social Research and Practice. 2014;13(4):429–450. doi: 10.1177/1471301214535134. [DOI] [PubMed] [Google Scholar]
- Cernin P, Keller B, Stoner J. Color vision in Alzheimer’s patients: Can we improve object recognition with color cues? Aging, Neuropsychology, and Cognition. 2003;10(4):255–267. doi: 10.1076/anec.10.4.255.28971. [DOI] [Google Scholar]
- Chiu Y, Algase D, Whall A, Liang J, Liu H, Lin K, Wang P. Getting lost: Directed attention and executive functions in early Alzheimer’s disease patients. Dementia and geriatric Cognitive Disorders. 2004;17(3):174–180. doi: 10.1159/000076353. [DOI] [PubMed] [Google Scholar]
- Cushman LA, Stein K, Duffy CJ. Detecting navigational deficits in cognitive aging and Alzheimer disease using virtual reality. Neurology. 2008;71(12):888. doi: 10.1212/01.wnl.0000326262.67613.fe. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davis RL, Therrien B, West B. Cue conditions and wayfinding in older and younger women. Research in Gerontological Nursing. 2008;9(4):252–263. doi: 10.3928/19404921-20081001-06. [DOI] [PubMed] [Google Scholar]
- Davis RL, Therrien B, West B. Working memory, cues and wayfinding in older women. Journal of Applied Gerontology. 2009;28(6):743–767. doi: 10.1177/0733464809332785. [DOI] [Google Scholar]
- Davis RL, Therrien B. Cue color and familiarity in place learning for older adults. Research in Gerontological Nursing. 2012;5(2):138–148. doi: 10.3928/19404921-20111004-01. [DOI] [PubMed] [Google Scholar]
- deIpolyi AR, Rankin KP, Mucke L, Miller BL, Gorno-Tempini ML. Spatial cognition and the human navigation network in AD and MCI. Neurology. 2007;69(10):986–997. doi: 10.1212/01.wnl.0000271376.19515.c6. [DOI] [PubMed] [Google Scholar]
- Flynn D, Van Schaik P, Blackman T, Femcott C, Hobbs B, Calderon C. Developing a virtual reality-based methodology for people with dementia: A feasibility study. CyberPsychology & Behavior. 2003;6(6):591–611. doi: 10.1089/109493103322725379. [DOI] [PubMed] [Google Scholar]
- Foreman N, Stirk J, Pohl J, Mandelkow L, Lehnung M, Herzog A, Leplow B. Spatial information transfer from virtual to real versions of the Kiel locomotor maze. Behavioural Brain Research. 2000;112(1–2):53–61. doi: 10.1016/s0166-4328(00)00159-5. [DOI] [PubMed] [Google Scholar]
- Foreman N, Wilson P, Duffy H, Parnell R. Transfer of spatial knowledge to a two-level shopping mall in older people, following virtual exploration. Environment and Behavior. 2005;37(2):275–292. doi: 10.1177/0013916504269649. [DOI] [Google Scholar]
- Gunther R, Kazman R, MacGregor C. Using 3D sound as a navigational aid in virtual environments. Behaviour & Information Technology. 2004;23(6):435–446. doi: 10.1080/01449290410001723364. [DOI] [Google Scholar]
- Hardy L. The Ishihara test as a means of detecting and analyzing defective color vision. Journal of General Psychology. 1947;36:79–105. doi: 10.1080/00221309.1947.9918108. [DOI] [PubMed] [Google Scholar]
- Jacobs J, Laurance H, Thomas K. Place learning in virtual space I: Acquisition, overshadowing, and transfer. Learning and Motivation. 1997;28:521–541. doi: 10.1006/lmot.1997.0977. [DOI] [Google Scholar]
- Jheng SS, Pai MC. Cognitive map in patients with mild Alzheimer’s disease: a computer-generated arena study. Behavioural Brain Research. 2009;200(1):42–47. doi: 10.1016/j.bbr.2008.12.029. [DOI] [PubMed] [Google Scholar]
- Kalová E, Vlcek K, Jarolímová E, Bureš J. Allothetic orientation and sequential ordering of places is impaired in early stages of Alzheimer’s disease: corresponding results in real space tests and computer tests. Behavioural Brain Research. 2005;159(2):175–186. doi: 10.1016/j.bbr.2004.10.016. [DOI] [PubMed] [Google Scholar]
- Kavcic V, Duffy C. Attentional dynamics and visual perception: Mechanisms of spatial disorientation in Alzheimer’s disease. Brain. 2003;126:1173–1181. doi: 10.1093/brain/awg105. [DOI] [PubMed] [Google Scholar]
- Kavcic V, Fernandez R, Logan D, Duffy C. Neurological and perceptual correlates of navigational impairment in Alzheimer’s disease. Brain. 2006;129:736–746. doi: 10.1093/brain/awh727. [DOI] [PubMed] [Google Scholar]
- Kim SYH, Caine ED, Currier GW, Leibovici A, Ryan JM. Assessing the competence of persons with Alzheimer’s disease in providing informed consent for participation in research. American Journal of Psychiatry. 2001;158(5):712–717. doi: 10.1176/appi.ajp.158.5.712. [DOI] [PubMed] [Google Scholar]
- Kirasic KC, Allen GL, Haggerty D. Age-related differences in adults’ macrospatial cognitive processes. Experimental Aging Research. 1992;18(1–2):33–39. doi: 10.1080/03610739208253908. [DOI] [PubMed] [Google Scholar]
- Krueger C, Tian L. A comparison of the general linear mixed model and repeated measures ANOVA using a dataset with multiple missing data points. Biological Research for Nursing. 2004;6(2):151–157. doi: 10.1177/109980040426768. [DOI] [PubMed] [Google Scholar]
- Lawton C. Gender differences in way-finding strategies: Relationship to spatial ability and spatial anxiety. Sex Roles. 1994;30(11):765–779. doi: 10.1007/bf01544230. [DOI] [Google Scholar]
- Lawton C, Kallai J. Gender differences in wayfinding strategies and anxiety about wayfinding: A cross-cultural comparison. Sex Roles. 2002;47(9):389–401. doi: 10.1023/a:1021668724970. [DOI] [Google Scholar]
- Lawton M, Nahemow L. Ecology and the aging process. In: Eisdorfer C, Lawton MP, editors. Psychology of Adult Development and Aging. Washington D.C.: American Psychological Association; 1973. pp. 619–674. [Google Scholar]
- Lezak M. Neuropsychological Assessment. 3rd. New York: Oxford University Press; 1995. [Google Scholar]
- McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM. Clinical diagnosis of Alzheimer’s disease Report of the NINCDS-ADRDA Work Group* under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology. 1984;34(7):939–939. doi: 10.1212/wnl.34.7.939. [DOI] [PubMed] [Google Scholar]
- Moffat S, Resnick S. Effects of age on virtual environment place navigation and allocentric cognitive mapping. Behavioral Neuroscience. 2002;116(5):851–859. doi: 10.1037/0735-7044.116.5.851. [DOI] [PubMed] [Google Scholar]
- Moffat S, Zonderman A, Resnick S. Age differences in spatial memory in a virtual environment navigation task. Neurobiology of Aging. 2001;22(5):787–796. doi: 10.1016/s0197-4580(01)00251-2. [DOI] [PubMed] [Google Scholar]
- Monacelli AM, Cushman LA, Kavcic V, Duffy CJ. Spatial disorientation in Alzheimer’s disease: The remembrance of things passed. Neurology. 2003;61(11):1491–1497. doi: 10.1212/WNL.61.11.1491. [DOI] [PubMed] [Google Scholar]
- Namazi KH, Rosner TT, Rechlin L. Long-term memory cuing to reduce visuo-spatial disorientation in Alzheimer’s disease patients in a special care unit. American Journal of Alzheimer’s Disease and Other Dementias. 1991;6(6):10–15. doi: 10.1177/153331759100600603. [DOI] [Google Scholar]
- Nasreddine ZS, Phillips NA, Bedirian V, Charbonneau S, Whitehead V, Collin I, Chertkow H. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. Journal of the American Geriatrics Society. 2005;53(4):695–699. doi: 10.1111/j.1532-5415.2005.53221.x. [DOI] [PubMed] [Google Scholar]
- National Institutes of Health. Research Involving Individuals with Questionable Capacity to Consent: Points to consider. 2009 Nov; Retreived from http://grants.nih.gov/grants/policy/questionablecapacity.htm.
- Nolan B, Mathews R, Truesdell-Todd G, VanDorp A. Evaluation of the effect of orientation cues on wayfinding in persons with dementia. Alzheimer’s Care Today. 2002;3(1):46–49. doi: http://journals.lww.com/actjournalonline/pages/currenttoc.aspx. [Google Scholar]
- Ohm C, Muller M, Lugwig B, Bienk S. Where is the landmark? Eye tracking studies in large-scale indoor environments. 2nd International Workshop on Eye Tracking for Spatial Research. 2014:47–51. Retreived from http://epub.uni-regensburg.de/31436/1/paper10.pdf.
- Pai MC, Jacobs WJ. Topographical disorientation in community-residing patients with Alzheimer’s disease. International Journal of Geriatric Psychiatry. 2004;19(3):250–255. doi: 10.1002/gps.1081. [DOI] [PubMed] [Google Scholar]
- Pai MC, Lee CC, Yang YC, Lee YT, Chen KC, Lin SH, Jheng S, Sun P, Cheng PJ. Development of a Questionnaire on Everyday Navigational Ability to Assess Topographical Disorientation in Alzheimer’s Disease. American Journal of Alzheimers Disease and Other Dementias. 2012;27(1):65–72. doi: 10.1177/1533317512436805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Passini R, Pigot H, Rainville C, Tetreault M. Wayfinding in a nursing home for advanced dementia of the Alzheimer’s type. Environment and Behavior. 2000;32(5):684–710. doi: 10.1177/00139160021972748. [DOI] [Google Scholar]
- Passini R, Rainville C, Marchand N. Wayfinding and dementia: Some research findings and a new look at design. Journal of Architectural and Planning Research. 1998;15(2):133–151. doi: 10.1080/01688639508402431. [DOI] [Google Scholar]
- Rainville C, Passini R, Marchand N. A multiple case study of wayfinding in dementia of the alzheimertype: Decision making. Aging, Neuropsychology & Cognition. 2001;8(1):54. doi: 10.1076/anec.8.1.54.846. [DOI] [Google Scholar]
- Resnick B, Gruber-Baldini AL, Pretzer-Aboff I, Galik E, Buie VC, Russ K, Zimmerman S. Reliability and validity of the evaluation to sign consent measure. Gerontologist. 2007;47(1):69–77. doi: 10.1093/geront/47.1.69. [DOI] [PubMed] [Google Scholar]
- Rowe M. Persons with dementia who became lost in the community: Preventing injuries and death. American Journal of Nursing. 2003;103(7):32–40. doi: 10.1097/00000446-200307000-00016. [DOI] [PubMed] [Google Scholar]
- Sherman W, Craig A. Understanding Virtual Reality. San Francisco: Elsevier Science; 2003. [Google Scholar]
- Smith T, Gildeh N, Holmes C. The Montreal Cognitive Assessment: validity and utility in a memory clinic setting. Can J Psychiatry. 2007;52(5):329–332. doi: 10.1016/j.jalz.2011.05.451. [DOI] [PubMed] [Google Scholar]
- Thomas K, Hsu M, Laurance H, Nadel L, Jacobs W. Place learning in virtual space III: Investigation of spatial navigation training procedures and their application to fMRI and clinical neuropsychology. Behavior Research Methods, Instruments & Computers. 2001;33(1):21–37. doi: 10.3758/BF03195344. [DOI] [PubMed] [Google Scholar]
- Tu MC, Pai MC. Getting lost for the first time in patients with Alzheimer’s disease. International Psychogeriatrics. 2006;18(03):567–570. doi: 10.1017/S1041610206224025. [DOI] [PubMed] [Google Scholar]
- Uc EY, Rizzo M, Anderson SW, Shi Q, Dawson JD. Driver route-following and safety errors in early Alzheimer disease. Neurology. 2004;63(5):832–837. doi: 10.1017/S1041610206224025. [DOI] [PubMed] [Google Scholar]
- Weschler D. Weschler Memory Scale - revised manual. New York: The Psychological Corporation; 1987. [Google Scholar]
- Wood S, Mortel KF, Hiscock M, Breitmeyer BG, Caroselli JS. Adaptive and maladaptive utilization of color cues by patients with mild to moderate Alzheimer’s Disease. Archives of Clinical Neuropsychology. 1997;12(5):483–489. doi: 10.1093/arclin/12.5.483. [DOI] [PubMed] [Google Scholar]
- Yew B, Alladi S, Shailaja M, Hodges JR, Hornberger M. Lost and forgotten? Orientation versus memory in Alzheimer’s disease and frontotemporal dementia. Journal of Alzheimers Disease. 2013;33(2):473–481. doi: 10.3233/JAD-2012-120769. [DOI] [PubMed] [Google Scholar]
- Zakzanis KK, Quintin G, Graham SJ, Mraz R. Age and dementia related differences in spatial navigation within an immersive virtual environment. Medical science monitor: international medical journal of experimental and clinical research. 2009;15(4):CR140–CR150. Retreived from http://www.medscimonit.com/ [PubMed] [Google Scholar]