

Abstract
Purpose: To report a prospective, multicenter, observational study (ClinicalTrials.gov identifier NCT01609621) of the safety and effectiveness of tibiopedal access and retrograde crossing in the treatment of infrainguinal chronic total occlusions (CTOs). Methods: Twelve sites around the world prospectively enrolled 197 patients (mean age 71±11 years, range 41-93; 129 men) from May 2012 to July 2013 who met the inclusion criterion of at least one CTO for which a retrograde crossing procedure was planned or became necessary. The population consisted of 64 (32.5%) claudicants (Rutherford categories 2/3) and 133 (67.5%) patients with critical limb ischemia (Rutherford category ≥4). A primary antegrade attempt to cross had been made prior to the tibiopedal attempt in 132 (67.0%) cases. Techniques used for access, retrograde lesion crossing, and treatment were at the operator’s discretion. Follow-up data were obtained 30 days after the procedure. Results: Technical tibiopedal access success was achieved in 184 (93.4%) of 197 patients and technical occlusion crossing success in 157 (85.3%) of the 184 successful tibial accesses. Failed access attempts were more common in women (9 of 13 failures). The rate of successful crossing was roughly equivalent between sexes [84.7% (50/59) women compared to 85.6% (107/125) men]. Technical success did not differ significantly based on a prior failed antegrade attempt: the access success rate was 92.4% (122/132) after a failed antegrade access vs 95.4% (62/65) in those with a primary tibiopedal attempt (p=0.55). Similarly, crossing success was achieved in 82.8% (101/122) after a failed antegrade access vs 90.3% (56/62) for patients with no prior antegrade attempt (p=0.19). Minor complications related to the access site occurred in 11 (5.6%) cases; no patient had access vessel thrombosis, compartment syndrome, or surgical revascularization. Conclusion: Tibiopedal access appears to be safe and can be used effectively for the crossing of infrainguinal lesions in patients with severe lower limb ischemia.
Keywords: chronic total occlusion, critical limb ischemia, peripheral artery disease, retrograde approach, tibiopedal, transpedal, vascular access
Introduction
The use of a tibiopedal access to cross infrainguinal occlusions from a retrograde approach has become a critical interventional strategy to address the growing public health threat of peripheral artery disease (PAD) and critical limb ischemia (CLI). Retrograde crossing of infrainguinal chronic total occlusions (CTOs) to facilitate recanalization was first described via cutdown by Iyer et al1 in 1990 to help avoid the morbidity, cost, and mortality associated with major limb amputation. Recently, more widespread adoption of the evolved percutaneous technique has been driven by the increased number of interventionists treating advanced PAD and the rising prevalence of CLI stemming from increased life expectancy and the global diabetes epidemic.2 These trends have fostered a growing recognition of the need to promote limb salvage in a patient population characterized by multilevel PAD and significant comorbidities.3
Many CLI patients present as unsuitable surgical candidates due to poor conduit, poor distal runoff, and high operative risk secondary to comorbidities. For these reasons, an endovascular-first approach is being utilized more frequently in treating CLI. Endovascular treatment requires navigating obstructive lesions that are commonly CTOs, but the traditional antegrade ipsilateral and contralateral femoral approaches fail to cross the lesion in roughly 20% of cases.4,5 The tibiopedal retrograde approach was developed to provide another endovascular option to cross infrainguinal lesions and allow successful interventional therapy following a failed antegrade crossing attempt, particularly in patients with poor surgical options.
Although the use of the tibiopedal approach has conventionally followed a failed antegrade attempt to promote limb salvage in CLI patients,4-14 increasing recognition of the advantages of the tibiopedal approach relative to antegrade access and crossing,15-17 combined with increasing expertise, improved tools, and the low reported risk of complications,18,19 have led some institutions to permit a more liberal use of the tibiopedal approach. This trend includes the use of a retrograde approach as a primary treatment for patients who are poor candidates for an antegrade access19 and for the treatment of PAD patients suffering from claudication (Rutherford categories 2–3) that has not yet progressed to CLI (Rutherford categories 4–6).
Despite these trends, there remains some debate7,17 over the role of tibiopedal access in the treatment of PAD, which is centered on the concern over the risk of injury or thrombotic occlusion of a pedal vessel, especially in patients with a single runoff artery to the foot. Though thrombotic occlusion from a tibiopedal approach has been reported only rarely and limb salvage has been achieved in all reported instances,4,13,14 in theory this could lead to sacrifice of a distal bypass target or loss of limb in a patient not previously at risk for amputation.
Despite these limitations, the high technical success and low complication rates documented by these reports have clearly demonstrated the vital importance of the tibiopedal access approach for limb salvage. Further adoption of the tibiopedal approach and a deeper understanding of the appropriate patient population for treatment via a tibiopedal access are currently hampered by a lack of published multicenter data. This report describes an investigation of the use of the tibiopedal approach for retrograde crossing of infrainguinal CTOs with the goal of evaluating acute access safety and the success of tibiopedal access and retrograde crossing.
Methods
Study Design
A prospective, nonrandomized, multicenter, observational study was designed to compile clinical data from a target population of 200 patients undergoing percutaneous tibiopedal access to retrogradely cross infrainguinal CTOs at 8 US and 3 European sites. The trial was registered on the National Institutes of Health website (ClinicalTrials.gov; identifier NCT01609621).
Patients were eligible for enrollment if they had an infrainguinal CTO for which a percutaneous tibiopedal access was used after a failed antegrade approach or as a primary access at institutions where tibiopedal access is a standard of care procedure. There were no specific exclusion criteria. The study was performed in accordance with the ethical principles that have their origin in the Declaration of Helsinki. Approval was obtained from each site’s institutional review board or ethics committee. All patients provided written informed consent.
Study Procedure
Devices and techniques used to gain tibiopedal access and cross the occluding lesion have been described in detail in the literature.15,17 Patients were treated according to the standard of care at each participating site by physicians possessing a range of expertise with tibiopedal access procedures. In this study, all devices and techniques were used at the investigator’s discretion, so only a general description of conventional technique is appropriate. Following preparation of the access site, light sedation, and local anesthesia, access was achieved under ultrasound or angiographic guidance. Typically, a micropuncture needle was used in conjunction with a 0.018-inch wire followed by a 2.9-F microcatheter once access had been achieved. Lesion crossing involved advancing the wire or the use of other crossing devices. Following successful crossing via the tibiopedal access, delivery of the final therapy proceeded via either the tibiopedal access or a femoral access. Throughout the procedure vasodilators and anticoagulants were delivered intra-arterially. Manual pressure was typically sufficient to achieve closure of the tibiopedal access following treatment and device removal.
Outcome Measures
Technical access success was defined as the ability to gain percutaneous entry into a tibiopedal artery in the desired location and to deliver a wire guide to facilitate introduction of a catheter. Technical crossing success referred to the ability to reach an infrainguinal CTO via a tibiopedal approach and to pass a wire through the proximal boundary of the occlusion. No limitations were placed on size of the distal vessels to be accessed, degree of calcification, length of the occluded target segment, or sheath size utilized in the procedure. Treatment success following crossing was measured, but treatment methods, treatment success, runoff status, and long-term clinical outcomes, such as limb salvage, were not specific outcomes of the study.
Data Collection and Definitions
Data collected included patient demographics and medical history, Rutherford classification, access vessel location, lesion characteristics, treatments used, and all procedure-related complications. If multilevel lesions were targeted for revascularization, the cumulative total lesion length was recorded. A 30-day telephone follow-up was conducted to record any complications and to assess the postoperative Rutherford category, which was treated as a continuous variable for comparison with the preoperative values for the population. All complications related to the access site were noted postoperatively and at follow-up, including minor events (ecchymosis, pain, non–life-threatening bleeding, and hematoma) and major events (access vessel thrombosis, compartment syndrome, or surgical revascularization). Amputations were documented (major amputations were defined as above the ankle). Adverse events related to the new onset of wounds in the study leg were recorded even though they represented CLI progression in cases of failed or insufficient revascularization.
Patient Enrollment
From May 2012 through July 2013, 197 patients (mean age 71±11 years, range 41–93; 129 men) were enrolled. Three patients were excluded: one patient was initially enrolled twice and 2 had the retrograde access site in the popliteal artery rather than a tibiopedal vessel. Baseline characteristics of the study population and the treated limb are presented in Table 1. Two-thirds of the population presented with CLI (133, 67.5%). Roughly half (101, 51.3%) of the patients had preexisting tissue loss in the study leg, the majority of which presented as ischemic ulcers. A prior minor amputation to the study leg had been performed in 21 (10.7%) patients. The mean lesion length was 17±13 cm (median 15); the majority (116, 58.9%) had lesions >10 cm long. Occlusive lesions in multiple vessels were targeted for therapy in 79 (40.1%) patients. In two-thirds (132, 67.0%) of the cases, a previous antegrade approach to cross the occlusion had failed prior to the tibiopedal attempt.
Table 1.
Baseline Characteristics for the 197 Patients and Treated Limbs.a
| Age, y | 71±11 (41–93) |
| Men | 129 (65.5) |
| Comorbidities and risk factors | |
| Hypertension | 181 (91.9) |
| Hypercholesterolemia | 153 (77.7) |
| Bleeding diathesis/coagulopathy | 2 (1.0) |
| Diabetes mellitus | 129 (65.5) |
| Chronic renal insufficiency | 57 (28.9) |
| Renal failure requiring dialysis | 16 (8.1) |
| Smoking status, current / former / never | 35 (17.8) / 96 (48.7) / 66 (33.5) |
| Target limb characteristics | |
| Previous intervention | 65 (33.0) |
| Previous intervention with tibiopedal access | 30 (15.2) |
| Previous arterial access site complication | 10 (5.1) |
| Antegrade attempt prior to tibiopedal attempt | 132 (67.0) |
| Rutherford score | |
| 2 | 9 (4.6) |
| 3 | 55 (27.9) |
| 4 | 37 (18.8) |
| 5 | 80 (40.6) |
| 6 | 16 (8.1) |
| Preexisting tissue loss | 101 (51.3) |
| Amputation | 7 (3.6) |
| Amputation/gangrene | 2 (1.0) |
| Amputation/ischemic ulcer | 7 (3.6) |
| Amputation/ischemic ulcer/gangrene | 5 (2.5) |
| Gangrene | 12 (6.1) |
| Ischemic ulcer | 55 (27.9) |
| Gangrene/ischemic ulcer | 13 (6.6) |
| Lesion locationb | |
| Iliacc | 1 (0.5) |
| Superficial femoral artery | 63 (32.0) |
| Popliteal | 74 (37.6) |
| Anterior tibial | 85 (43.1) |
| Posterior tibial | 47 (23.9) |
| Peroneal | 27 (13.7) |
| Other | 18 (9.1) |
| Arteries spanned by lesion, 1 / 2 / 3 | 118 (59.9) / 48 (24.4) / 31 (15.7) |
| Cumulative lesion length, cm | 17±13 (0.5–60.0), median 15 |
| 0–10 | 72 (36.5) |
| 11–20 | 50 (25.4) |
| 21–30 | 39 (19.8) |
| >30 | 27 (13.7) |
| Not reported | 9 (4.6) |
| Tortuosity | |
| None | 69 (35.0) |
| Mild | 69 (35.0) |
| Moderate | 43 (21.8) |
| Severe | 9 (4.6) |
| Not reported | 7 (3.6) |
Continuous data are presented as the means ± standard deviation (range), median if available; categorical data are given as the counts (percentage).
Total exceeds 100% due to lesions that spanned multiple vessels.
Treated in conjunction with infrapopliteal disease.
Statistical Analysis
Data were analyzed on an intention-to-treat basis with the exception of outcomes dependent on successful access (eg, crossing success). Continuous variables are reported as means ± standard deviations, medians, and ranges. Categorical variables are reported as frequencies and percentages. Variables were compared using the Fisher exact test, with p<0.05 as the threshold of significance. Statistical analyses were performed using SAS software (version 9.3 for Windows; SAS Inc., Cary, NC, USA).
Results
Technical access success was recorded in 184 (93.4%) patients (Table 2): 62 (96.9%) of 64 claudicants and 122 (91.7%) of the 133 CLI patients. The anterior and posterior tibial vessels followed by the dorsalis pedis were the most common access vessels (Table 2). The imaging method used to assist was angiography (66, 33.5%), ultrasound (71, 36.0%), or both (58, 29.4%). Of the 13 (6.6%) failed cases, calcification at the access site was reported as severe in 10 and moderate in 1 (2 cases unreported). The imaging mode used in the failed access cases was ultrasound in 4 or both modes in 7 (unreported in 3 cases). Failed access attempts were more common in female patients (9/13), although women represented only a third of the patient cohort; they also tended to have more severe calcification at the access site relative to the male patients.
Table 2.
Vascular Access Data.a
| Vessels accessed (n=197) | |
| Anterior tibial | 51 (25.9) |
| Posterior tibial | 69 (35.0) |
| Peroneal | 19 (9.6) |
| Dorsalis pedis | 44 (22.3) |
| Lateral plantar | 1 (0.5) |
| Technical access success | |
| All patients (n=197) | 184 (93.4) |
| Rutherford 2–3 (n=64) | 62 (96.9) |
| Rutherford 4–6 (n=133) | 122 (91.7) |
| Access unsuccessful | 13 (6.6) |
| Calcification at access site (n=197) | |
| None | 44 (22.3) |
| Mild | 57 (28.9) |
| Moderate | 49 (24.9) |
| Severe | 45 (22.8) |
| Not reported | 2 (1.0) |
| Access guidance (n=197) | |
| Angiography | 66 (33.5) |
| Angiography/ultrasound | 58 (29.4) |
| Ultrasound | 71 (36.0) |
| Not reported | 2 (1.0) |
| Access vessel diameter, mm (n=182) | 2.3±0.5 (1–4) |
Continuous data are presented as the means ± standard deviation (range); categorical data are given as the counts (percentage).
Technical retrograde crossing success (Table 3) was reported in 157 (85.3%) of the 184 successful tibiopedal access cases [52 (83.9%) of 62 claudicants and 105 (86.1%) of 122 CLI patients]. The rate of successful crossing was roughly equivalent between sexes [84.7% (50/59) of women compared to 85.6% (107/125) of men]. Multiple endovascular tools were used in most cases (99/157, 63.1%), with balloon angioplasty being the most common (90.4%, 142/157). Single tool techniques were infrequent: balloon angioplasty (30.6%, 48/157), bare metal stent (2.5%, 4/157), drug-coated balloon (1.9%, 3/157), other treatment (1.3%, 2/157), and rotational atherectomy (0.6%, 1/157). Treatment of the occlusion was deemed successful by the treating physician in 156 (99.4%) of the 157 cases in which retrograde lesion crossing was achieved.
Table 3.
Procedure and Treatment Data.
| Technical crossing success | |
| All patients (n=184) | 157 (85.3) |
| Rutherford 2–3 (n=62) | 52 (83.9) |
| Rutherford 4–6 (n=122) | 105 (86.1) |
| Crossing success by primary usage | |
| After failed antegrade (n=122) | 101 (82.8) |
| Via primary tibiopedal (n=62) | 56 (90.3) |
| Time from wire delivery to lesion crossing, min (n=157) | 19±20 (0–107), median 13 |
| Treatment method (n=157)b | |
| Bare balloon | 142 (90.4) |
| Bare metal stent | 45 (28.7) |
| Otherc | 28 (17.8) |
| Drug-eluting stent | 23 (14.6) |
| Drug-coated balloon | 20 (12.7) |
| Directional atherectomy | 17 (10.8) |
| Thrombectomy | 5 (3.2) |
| Rotational atherectomy | 3 (1.9) |
| Thrombolysis | 2 (1.3) |
| Closure method (n=197)b | |
| Manual compression | 125 (63.5) |
| Hemostatic closure band | 49 (24.9) |
| Balloon inflation | 38 (19.3) |
| Other | 17 (8.6) |
| Suture | 0 (0) |
| Treatment success (n=157) | 156 (99.4) |
Continuous data are presented as the means ± standard deviation (range), median if available; categorical data are given as the counts (percentage).
Total exceeds 100% due to cases in which multiple methods were used.
Predominantly specialty balloons.
A third of the study population (65, 33.0%) had the retrograde procedure without a prior antegrade attempt. Of that group, the majority were CLI patients (43/65, 66.2%), which closely matches the incidence of CLI in the study population (67.5%, 133/197), demonstrating that primary usage of the approach was independent of the ischemia grade. Technical success did not differ significantly based on a prior failed antegrade attempt: the access success rate was 92.4% (122/132) after a failed antegrade access vs 95.4% (62/65) in those with a primary tibiopedal attempt (p=0.55). Similarly, crossing success was achieved in 82.8% (101/122) after a failed antegrade access vs 90.3% (56/62) for patients with no prior antegrade attempt (p=0.19).
Telephone follow-up was performed 30 days after the revascularization procedure in 190 patients (2 patients were lost to follow-up and 5 died of procedurally-unrelated advanced heart disease or renal failure). Mean Rutherford scores (Figure 1) improved in 130 (68.4%) of the 190 patients contacted, while only 12 (6.3%) patients worsened. There was 1 access failure and 1 crossing failure in the latter 12 patients, while the other 10 patients had a worse score despite successful access and crossing. Most of the claudicants improved (54/64, 84.4%) compared with the CLI population (76/126, 60.3%; p<0.01). Roughly one-quarter (48/190, 25.3%) of the entire cohort had no change in Rutherford score; the majority were CLI patients (42/48, 87.5%).
Figure 1.
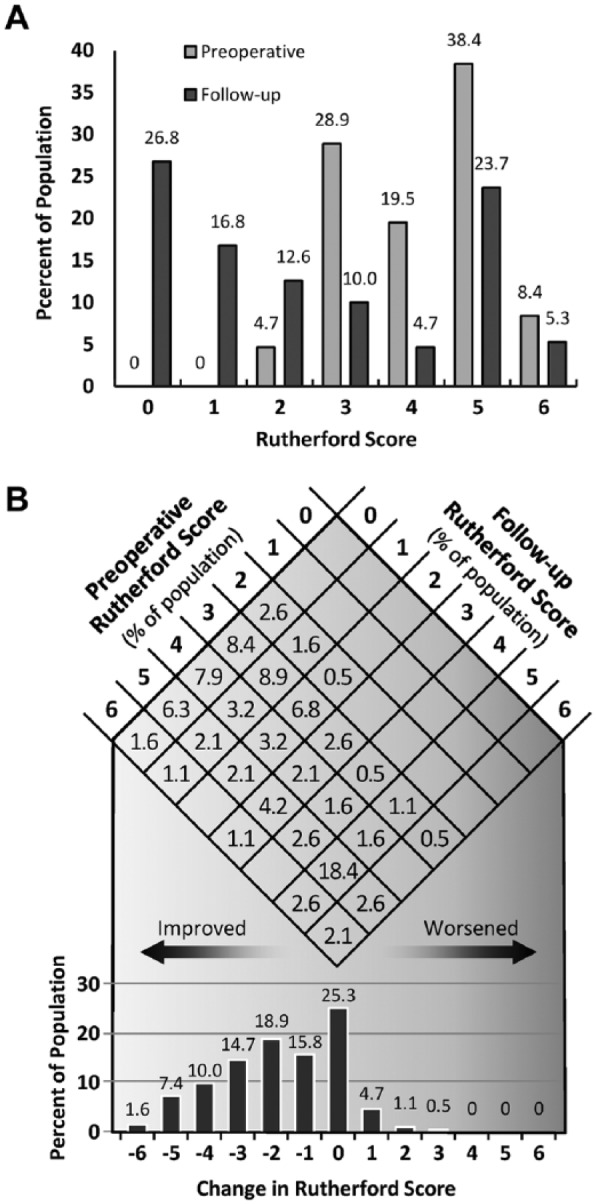
(A) Comparison of the mean preoperative and 30-day Rutherford category values. (B) The top matrix exhibits the percentage of patients that moved between specific Rutherford categories. The matrix diagonal represents patients with no change in score; to the left and right of the diagonal are improved and worsened levels, respectively. The bottom bar graph is the summed percentage of patients from the matrix who had a change in Rutherford category of a given magnitude.
All major and minor complications were recorded postoperatively and at the 30-day follow-up. Minor access site–related complications were local pain (4/197, 2.0%), infection (2/197, 1.0%), ecchymosis (2/197, 1.0%), bleeding (2/197, 1.0%), and acute vessel dissection (1/197, 0.5%). There were no major complications related to access. Nonaccess-related adverse events in the study leg included gangrene (6/197, 3.0%), ischemia (8/197, 4.1%), and ischemic ulcer (5/197, 2.5%). Six major and 6 minor amputations were required in 12 (6.1%) patients.
Discussion
The global epidemic of CLI combined with improved endovascular tools and increasing experience of interventionists continues to drive improvements in the current PAD treatment paradigm. Tibiopedal retrograde revascularization has become another critical tool for crossing lesions and promoting limb salvage, offering a number of advantages over surgical and traditional antegrade endovascular approaches. From a hypothetical standpoint, the value of the tibiopedal approach stems from the fact that the distal cap of peripheral lesions is often softer than the proximal cap, allowing engagement of “hibernating distal vessels” that can be more easily traversed.15,16 This may increase the likelihood of successful crossing following a failed antegrade attempt and may also improve the chance of remaining within the true vessel lumen, which could reduce routine use of costly CTO crossing and reentry tools.7 Other potential advantages include reduced bleeding risk, good control and pushability due to proximity of the target lesion to the access, and reductions in procedure time and time to discharge.
The single-center literature has documented these advantages as well as high success and low complication rates.4-14,18,19 However, some debate persists, primarily centering on the proper role of tibiopedal revascularization as a treatment for severe claudication.7,17 Although rare and not recorded in this clinical experience, acute and subacute thrombotic occlusion of the access vessel has been reported.4,13,14 For claudicant patients, especially those with a single runoff vessel to the foot, such a major access site complication could potentially lead to deterioration in the health of the limb and progression to CLI.
The primary objective of this study was to evaluate the safety of the tibiopedal approach and the success rates of pedal access and retrograde crossing in a multicenter, international setting with a population indicative of real-world patients and lesions. For this reason, there were no specific exclusion criteria, and the study population included patients with significant comorbidities, preexisting tissue loss, multilevel disease, and diffuse and long CTOs. Procedures were performed at 11 global sites by operators with a range of procedural experience.
The multicenter design of the study contrasts with the current literature, which consists of a limited number of case reports and retrospective series from single institutions. Among the larger studies, Montero-Baker et al4 reported 86.3% success in treating 51 patients (45 with CLI), with 1 access site–related thrombosis that required urgent surgical repair. Walker14 recently reported the results of 228 CLI patients in whom a tibiopedal approach was utilized, documenting successful access in 95% (217/228), successful crossing in 93% (199/217) of those successfully accessed, and overall treatment success in 99% (196/197) of these cases. There were no observed bleeding complications. A single pedal occlusion was encountered in a patient in whom the pedal access was deemed the only viable route for superficial femoral artery stenting via a 6-F sheath; ultimately, limb salvage was achieved.
With 2 exceptions,18,19 the previously published series4-14 used a tibiopedal approach following a failed antegrade attempt to cross, demonstrating that typical usage of the retrograde approach has been as a bailout option to avoid limb amputation. Both Mustapha et al18 and Hanna and Prout19 used a primary tibiopedal approach in cases in which body habitus, comorbidities, or complex angiographic characteristics precluded an initial antegrade attempt to cross. Both investigators reported successful arterial access and crossing in all patients, with no major complications.
The number of claudicant patients enrolled in the study and the significant use of the retrograde approach as a primary procedure with no prior antegrade attempt could indicate a trend toward more liberal use of retrograde revascularization in some institutions. Although this observational study recorded good acute safety of the retrograde approach, the published data remain insufficient to recommend such use. However, the study investigators recognize that this trend likely stems from more widespread adoption, increasing expertise with the approach, improved tools, increased incidence of CLI interventions, and growing recognition of the crossing advantages and overall safety of the tibiopedal approach. A retrograde approach also may be the only endovascular option in patients who cannot lie flat or whose body habitus or comorbidities preclude femoral access.
The most frequently accessed vessels in the study were the posterior and anterior tibial and the pedal arteries; the peroneal artery was attempted in <10% of the cases. Understandably, operators may be hesitant to access a vessel that may be more technically challenging due to its position behind the interosseus membrane. In our study, disease distribution (see Table 1) may have played a large role.
Interestingly, there does not seem to be consensus regarding the imaging method used to gain access. Approximately a third of the cases were done solely under fluoroscopy, a third under ultrasound, and a third using both. The study investigators recognize the value of angiography in securing access in complex scenarios, but ultrasound guidance can be highly effective, lowering the access-related complication rate20-22 and reducing the radiation exposure to both the patient and operator. However, effective use of ultrasound requires extensive training, and the experience may not yet be available in many institutions.
The 20% access/crossing failure rate in this study should not be viewed negatively, as it is similar to reported failure rates of traditional antegrade approaches.4,5 More important, it is critical to remember that two thirds of the population had already experienced a failed antegrade crossing attempt and had no further endovascular option to avoid amputation. Three quarters of the patients with a prior failed antegrade attempt were successfully approached from a retrograde access. Importantly, this implies that in patients amenable to both approaches, the ability to employ a retrograde approach following a failed antegrade attempt should leave only ~5% of patients with lesions that cannot be crossed.
Overall, the cohort demonstrated a low rate of access-related complications without a major event, including access-site thrombosis. Most operators will recognize that the risk of thrombotic occlusion is higher when devices that may be potentially occlusive are utilized to secure access.15,16 The study investigators support use of the smallest possible microcatheters, vasodilators, and aggressive anticoagulation as means to minimize the risk of thrombosis.
The majority of the population experienced an improvement in Rutherford score at the 30-day follow-up, and a worsened score was not indicative of procedure failure. Although half the patients had extensive preexisting tissue loss and 20% of all patients experienced access or crossing failure, only 6 major and 6 minor amputations were observed in the study. Additionally, it is important to note that a primary goal of an intervention in some patients with extensive tissue loss may be to reduce the amputation level and facilitate healing rather than avoid amputation altogether. Achieving such reductions in the level of amputation may be considered a success in some patients based on significant differences in patient mortality and quality of life between major and minor amputations.2
An important avenue of future research is further elucidation of factors that contribute to access or crossing failure. The population size and low failure rates (13 access and 27 crossing failures) in this study precluded statistical analysis of such characteristics, but by way of observation there was a moderate to high degree of calcification in the failed cases. Moreover, failures occurred predominately in female patients, who may be likely to have smaller access vessels and more diffuse disease. Neither access nor crossing failure showed any strong correlation with mean Rutherford score, and operators using both ultrasound and a combination of ultrasound and angiography experienced access failures.
Limitations
The limitations of this study are primarily those inherent in its observational design, the relatively short 30-day telephone follow-up, and the moderate size of the patient population. Future studies with a longer follow-up could compare amputation-free survival to prior studies of surgical or antegrade endovascular techniques, as well as provide additional insight into the risk of thrombotic occlusion or access site injury. In addition, as improvement in Rutherford category for a CLI patient is predicated on wound healing rates, which can vary widely,23 a follow-up period >30 days may be necessary to accurately evaluate changes in Rutherford category for patients with extensive preexisting tissue loss. Finally, future studies with larger patient populations may allow statistical analysis of factors that reduce the likelihood of tibiopedal access and crossing success and could continue to improve our understanding of the patient population most amenable to this approach.
Conclusion
This prospective, multicenter, observational study on the use of a tibiopedal access for retrograde crossing of occlusions recorded high access and lesion-crossing rates with relatively few and minor access-related complications. The study suggests increasing utilization of this approach as a primary treatment for CLI and as a treatment option for severe claudication. The rapid growth of the CLI population, combined with the morbidity and mortality associated with major limb amputation, emphasizes the critical need for additional research on the effectiveness of tibiopedal access and revascularization from a retrograde access site.
Acknowledgments
The authors thank Katrine Birch Rasmussen of Cook Medical for input into study design and critical review of the manuscript. The authors thank Anna Moseley and Alan Saunders of Cook Research, Inc. (a contract research organization and Cook Group company) for help with data analysis and statistical methods. The authors thank David Chadwick and Angela Huber of Cook Medical for critical review of the manuscript.
Footnotes
Authors’ Note: Preliminary study data were presented at New Cardiovascular Horizons 2013 (New Orleans, LA, USA; June 5–7, 2013); TCT 2013 (San Francisco, CA, USA; October 27–November 1, 2013); Amputation Prevention Symposium 2013 (Chicago, IL, USA; August 8–10, 2013); VIVA 2013 (Las Vegas, NV, USA; October 8–11, 2013); Veith 2013 (New York, NY, USA; November 19–23, 2013); Leipzig Interventional Course 2014 (Leipzig, Germany; January 28–31, 2014); and New Cardiovascular Horizons 2014 (New Orleans, LA, USA; May 28–30, 2014).
Declaration of Conflicting Interests: The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Craig Walker is a consultant and speaker for Cook Medical. Jihad Mustapha is a consultant for Cook Medical. Thomas Zeller has received study grants and speaking honoraria from Cook Medical. Andrej Schmidt is a consultant for Cook Medical. Miguel Montero-Baker is a speaker for Cook Medical. Aravinda Nanjundappa is a consultant for Cook Medical and a speaker for Jannsenn Pharmaceuticals, Astra Zeneca, and Pfizer. Marco Manzi and Mariano Palena are speakers and consultants for Cook Medical. Nelson Bernardo conducts training courses for Cook Medical. Yazan Khatib is a consultant for Cook Medical and is a board member for Bayer and Boston Scientific. Robert Beasley performs training for Abbott Vascular, Bard, BSCI, Cook Medical, Cordis, Medtronic/Covidien, CSI, Endologix, Gore, Lombard Medical, and Spectranetics. Fadi Saab is a consultant for Cook Medical. Adam Shields is a paid employee of MED Institute, Inc, a contract research organization and a Cook Group company. George Adams is a consultant and speaker for Cook Medical.
Funding: The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by Cook Medical Inc, Bloomington, IN, USA.
References
- 1. Iyer SS, Dorros G, Zaitoun R, et al. Retrograde recanalization of an occluded posterior tibial artery by using a posterior tibial cutdown: two case reports. Cathet Cardiovasc Diag. 1990;20:251–253. [DOI] [PubMed] [Google Scholar]
- 2. Allie DE, Hebert CJ, Walker CM, et al. Critical limb ischemia: a global epidemic. A critical analysis of current treatment unmasks the clinical and economic costs of CLI. EuroIntervention. 2005;1:75–84. [PubMed] [Google Scholar]
- 3. Norgren L, Hiatt WR, Dormandy JA, et al. Inter-society consensus for the management of peripheral arterial disease (TASC II). J Vasc Surg. 2007;45(suppl S):S5–S67. [DOI] [PubMed] [Google Scholar]
- 4. Montero-Baker M, Schmidt A, Bräunlich S, et al. Retrograde approach for complex popliteal and tibioperoneal occlusions. J Endovasc Ther. 2008;15:594–604. [DOI] [PubMed] [Google Scholar]
- 5. Rogers RK, Dattilo PB, Garcia JA, et al. Retrograde approach to recanalization of complex tibial disease. Catheter Cardiovasc Interv. 2011;77:915–925. [DOI] [PubMed] [Google Scholar]
- 6. Botti CF, Jr, Ansel GM, Silver MJ, et al. Percutaneous retrograde tibial access in limb salvage. J Endovasc Ther. 2003;10:614–618. [DOI] [PubMed] [Google Scholar]
- 7. Bazan HA, Le L, Donovan M, et al. Retrograde pedal access for patients with critical limb ischemia. J Vasc Surg. 2014;60:375–381. [DOI] [PubMed] [Google Scholar]
- 8. Mustapha JA, Saab F, McGoff T, et al. TAMI technique: tibiopedal arterial minimally invasive retrograde revascularization. Endovascular Today. 2013;1:39–47. [Google Scholar]
- 9. Fusaro M, Tashani A, Mollichelli N, et al. Retrograde pedal artery access for below-the-knee percutaneous revascularization. J Cardiovasc Med. 2007;8:216–218. [DOI] [PubMed] [Google Scholar]
- 10. Downer J, Uberoi R. Percutaneous retrograde tibial access in the endovascular treatment of acute limb ischaemia: a case report. Eur J Vasc Endovasc Surg. 2007;34:350–352. [DOI] [PubMed] [Google Scholar]
- 11. Kawarada O, Yokoi Y, Sekii H, et al. Retrograde crossing through the pedal arch for totally occluded tibial artery. J Interv Cardiol. 2008;21:342–346. [DOI] [PubMed] [Google Scholar]
- 12. Hansen A, Krawzcynski H, Lacher F. Retrograde transpedal recanalization of tibial artery occlusion. Vasa. 2009;38:249–253. [DOI] [PubMed] [Google Scholar]
- 13. Gür S, Oğuzkurt L, Gürel K, et al. US-guided retrograde tibial artery puncture for recanalization of complex infrainguinal arterial occlusions. Diagn Interv Radiol. 2013;19:134–140. [DOI] [PubMed] [Google Scholar]
- 14. Walker C. Pedal access in critical limb ischemia. J Cardiovasc Surg (Torino). 2014;55:225–227. [PubMed] [Google Scholar]
- 15. Walker CM. Pedal access in critical limb ischemia. In: Dieter RS, Dieter RA, Dieter RA, III, eds. Endovascular Interventions. New York, NY: Springer; 2014:805-822. [Google Scholar]
- 16. Montero-Baker M. The retrograde approach for BTK chronic total occlusions. Endovascular Today. 2014;5:55-64. [Google Scholar]
- 17. El-Sayed HF. Retrograde pedal/tibial artery access for treatment of infragenicular arterial occlusive disease. Methodist Debakey Cardiovasc J. 2013;9:73–78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Mustapha JA, Saab F, McGoff T, et al. Tibio-pedal arterial minimally invasive retrograde revascularization in patients with advanced peripheral vascular disease: the TAMI technique, original case series. Catheter Cardiovasc Interv. 2014;83:987–994. [DOI] [PubMed] [Google Scholar]
- 19. Hanna EB, Prout DL. Combined radial-pedal access strategy and radial-pedal rendezvous in the revascularization of complex total occlusions of the superficial femoral artery (the “no femoral access” strategy). J Endovasc Ther. 2016;23:321–329. [DOI] [PubMed] [Google Scholar]
- 20. Dietrich CF, Horn R, Morf S, et al. US-guided peripheral vascular interventions, comments on the EFSUMB guidelines. Med Ultrason. 2016;18:231–239. [DOI] [PubMed] [Google Scholar]
- 21. Kalish J, Eslami M, Gillespie D, et al. ; Vascular Study Group of New England. Routine use of ultrasound guidance in femoral arterial access for peripheral vascular intervention decreases groin hematoma rates. J Vasc Surg. 2015;61:1231–1238. [DOI] [PubMed] [Google Scholar]
- 22. Lo RC, Fokkema MT, Curran T, et al. Routine use of ultrasound-guided access reduces access site-related complications after lower extremity percutaneous revascularization. J Vasc Surg. 2015;61:405–412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Hoffman U, Schulte KL, Heidrich H, et al. Complete ulcer healing as primary endpoint in studies on critical limb ischemia? A critical reappraisal. Eur J Vasc Endovasc Surg. 2007;33:311–316. [DOI] [PubMed] [Google Scholar]