

The accuracy of simultaneous staging of synchronous malignancies with F-18-Fluorodeoxyglucose (FDG) positron emission tomography/computed tomography (PET/CT) has not been well-described previously.[1,2] The present report describes a case of diffuse large B-cell lymphoma (DLBCL) and gastric adenocarcinoma coexisting in the same patient. DLBCL accounts for approximately 40% of lymphomas in adults and can involve the whole lymphatic system, including the lymph nodes, spleen, thymus, and bone marrow[3,4] and usually exhibits high degree of metabolism. Conversely, primary gastric adenocarcinoma shows only a modest degree of hypermetabolism. The purpose of this report is to describe the usefulness of FDG PET/CT scan for successful staging of concomitant DLBCL and gastric adenocarcinoma and providing accurate staging of these two malignancies.
This is a case of 75-year-old male with history of several hospitalizations for gastrointestinal bleeding requiring transfusions during each admission. Endoscopy with biopsy in September 2015 revealed gastric cancer. Abdominal CT in October 2015 demonstrated thickened gastric body, a 1.5 cm celiac lymph node and multiple nonspecific mesenteric root lymph nodes. Subsequently, the patient developed cervical adenopathy in December 2015 with core needle biopsy of the germinal center revealing DLBCL. The patient was then referred for F-18 FDG PET/CT imaging for the purpose of initial staging of the newly diagnosed synchronous gastric cancer and DLBCL. One hour following intravenous injection of 17.4 mCi of F-18 FDG PET images from the base of the skull to mid-thighs were obtained combined with a low-dose noncontrast CT scan of the same region for the purpose of attenuation correction and anatomic coregistration. The obtained images demonstrated low to intermediate level of FDG uptake within the superior aspect of mid stomach with standardized uptake value (SUV) max of 7.7 in addition to diffuse probable physiologic stomach activity [Figure 1]. A repeat image of the stomach region was performed at 2 h postinjection after distention with water and showed persistent activity in the mid stomach wall with increasing SUV max at 9.8 and interval clearance of the rest of the physiologic stomach activity, which is consistent with the known gastric adenocarcinoma [Figure 2]. A 0.8 cm mildly FDG avid gastrohepatic lymph node was also identified with SUV max 4.6 at 1 h postinjection, which increased to SUV max 7.4 on the repeat images 2 h postinjection, compatible with a metastatic node from the gastric cancer. In addition, markedly hypermetabolic lymphadenopathy above and below diaphragm were noted including bilateral retrocrural (SUV max 36.5, measuring up to 1.6 cm) and retroperitoneal (SUV max 27.3, measuring up to 1.7 cm) lymph nodes [Figure 1]. Bone marrow in axial and appendicular skeleton showed diffuse and markedly increased FDG uptake with SUV max up to 25.9 without corresponding CT correlate, most consistent with bone marrow involvement by the lymphoma, and compatible with stage IV lymphoma given the known biopsy proven DLBCL.
Figure 1.
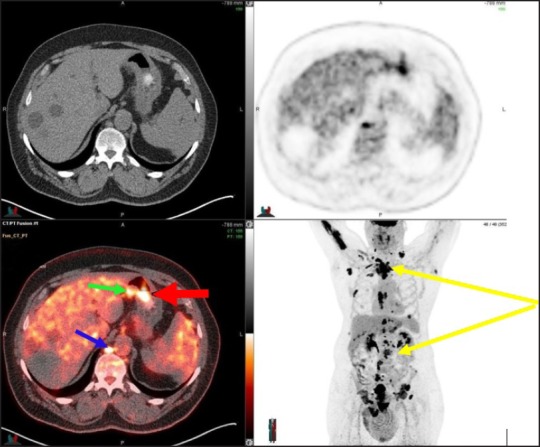
FDG PET/CT at 60 min: An intense focus of uptake in the retrocrural lymph node (SUV max 36.5, blue arrow) consistent with the known DLBCL as wells as a mildly hypermetabolic gastrohepatic small lymph node (SUV max 4.6, green arrow) suspicious for metastatic node from the second known gastric cancer. A focus of uptake at the region of the stomach body (SUV max 7.7, red arrow), not clearly localized to the stomach due to the partial stomach collapse, probably represents the second known gastric cancer; Foci of intense uptake above and below diaphragm (yellow arrow) compatible with the known DLBCL
Figure 2.
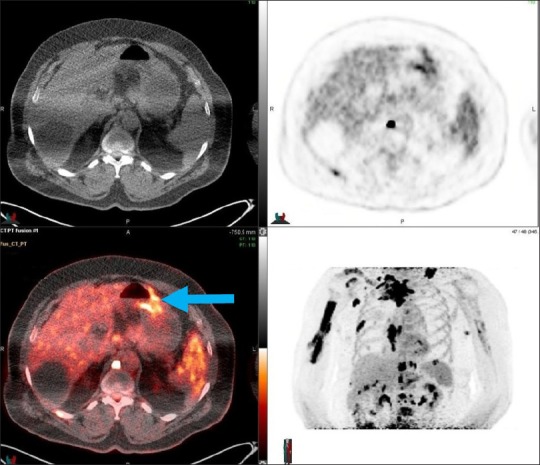
Delayed limited F-18-FDG PET acquired at 120 min after somewhat stomach distention with water: Fused transaxial PET/CT illustrates a persistent activity in the mid stomach (SUV max 9.8, blue arrow) associated with wall thickening compatible with the patient's known gastric cancer
In this case, the significant difference in the level of metabolic activity between the gastric cancer and DLBCL led to a successful staging of these malignancies. This case highlights the utility of FDG-PET/CT as a whole-body screening tool for synchronous malignancies that exhibit different degree of metabolism such as gastric cancer and DLBCL and adds to the current limited literature[12] on staging concurrent malignancies by F-18 FDG PET/CT imaging.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Yap J, Huang YT, Lin M. Detection of synchronous gastric schwannoma on FDG PET/CT aided by discordant metabolic response. Clin Nucl Med. 2015;40:e287–9. doi: 10.1097/RLU.0000000000000724. [DOI] [PubMed] [Google Scholar]
- 2.Farghaly HRS, Sayed MHM, Nasr HA, Maklad AMA. Dual time point fluorodeoxyglucose positron emission tomography/computed tomography in differentiation between malignant and benign lesions in cancer patients. Does it always work? Indian J Nucl Med. 2015;30:314–9. doi: 10.4103/0972-3919.159693. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Muzammil S, Kreze OD. Ophthalmoplegia with diffuse large B cell lymphoma: vital differential diagnosis. J Int Med Res. 2007;35:930–2. doi: 10.1177/147323000703500625. [DOI] [PubMed] [Google Scholar]
- 4.Naz E, Mirza T, Aziz S, Danish F, Siddiqui ST, Ali A. Frequency and clinicopathologic correlation of different types of non Hodgkin's lymphoma according to WHO classification. J Pak Med Assoc. 2011;61:260–3. [PubMed] [Google Scholar]