

Abstract
Background
Long-term clinical observations have shown that anxiety disorders influence the etiopathogenesis of ischemic heart disease (IHD) in women. The aim of this study was to determine the characteristics of the structure of overt and covert anxiety, and to examine the impact of the severity of anxiety on five personality traits as described Costa and McCrae.
Material/Methods
The study involved 50 women aged 37 to 74 years, who were treated because of IHD that was confirmed by angiographic examination of the coronary vessels. Psychological studies were conducted using the IPAT Anxiety Scale (Cattell) and NEO-FFI Personality Inventory (Costa and McCrae).
Results
From among the 50 women with IHD included in the study, 28 had higher overt anxiety scores than covert anxiety scores. Women with high overt anxiety were more emotionally changeable (C−), became impatient more easily, and expressed disappointment with life. They also worried about life problems more frequently. They had considerable suspiciousness (L+) and less trust towards the environment. They had a much stronger tendency to blame themselves (O+) and had intense internal, neurotic tension (Q4+). Women with high levels of overt anxiety had more neurotic traits (NEU), and lower openness to experience (OPE) scores.
Conclusions
Women with IHD were characterized by a high level of unease and anxiety. This may have resulted from lack of personality harmony, lack of personality integrity, or experienced value crises. Internal tension, auto-aggression, lowered emotional stability, and a sense of threat dominate the structure of unease and anxiety.
MeSH Keywords: Anxiety, Myocardial Ischemia, Personality, Women
Background
Ischemic heart disease (IHD) is currently the most frequent cause of deaths in highly developed countries both in men and in women. The main risk factors for cardiovascular disease are hypercholesterolemia, diabetes, arterial hypertension, cigarette smoking, obesity, and personality, as well as stress, age, sex, and heredity [1]. These risk factors have been studied in men, but have only been studied in women in the last 20 years [1]. Epidemiological studies reveal that in young people below the age of 50, a considerably higher (three to six times higher) cardiovascular disease incidence rate and death rate has been observed in men compared to women. Whereas after the age of 50, the disease incidence rate is much higher in women than in men, while around the age of 70, the incidence rate and death rate becomes similar in both groups [2].
The American Heart Association reported that cardiovascular disease in women was a “silent epidemic” [2]. In women, the clinical symptoms, disease course, and treatment and rehabilitation for IHD are different than in men. Compared with men, women’s ischemic symptoms are more often precipitated by mental or emotional stress and less frequently by physical exertion [3].
The increase in the incidence of cardiovascular disease and associated death in women has been linked to the rapid development of civilization and a sudden change in women’s lifestyle. Women have adopted a male lifestyle model and adopted male roles in professional and social environments. They perform jobs that require long work hours. They frequently work in difficult conditions and carrying roles with high level of responsibilities. Smoking has become popular among women as well as consuming other unhealthy substances, irregular diet, shorter sleep time, and reduced time for relaxation. Many women live in a constant state of hurry and are under the pressure of time, and overburdened with excessive responsibilities. They strive to achieve more and more but at the same time they have the sense of not fulfilling many important tasks. Such a style of life causes more and more women before the age of menopause to fall ill with cardiovascular disease, including IHD [4,5].
Epidemiological studies have shown that the first symptoms of the IHD in men occur around the age of forty-five, whereas in women they occur 10 years later, at about the age of fifty-five, of even sixty. Chest pain is frequently more atypical in women than in men. Frequently when a woman feels chest pain she thinks it is indigestion, muscle overexertion or spasms. She doesn’t think or realize she may have a heart infarct. IHD detection in women is less frequent and more difficult than in men. Women may not be aware of the negative effects of commonly known male risk factors on their own health state [6].
Psychological issues may be more specific in women with IHD. It should be pointed out that among factors predisposing to IHD, psychological factors play an important part, mainly personality and emotional factors such as anxiety, unease, decreased mood (depression), living in constant anxiety, suppressed aggression and anger, neurotic tension, excessive striving for success, domination, dogged determination in achieving a goal, love for excessive order, rigor and accurate planning of all undertakings, as well as living under pressure of time [7,8].
Depression symptoms that occur in women are twice as severe as in men. Women manifest lower resistance to stressful events and much more frequently reveal anxiety tension [9]. Anxiety is one of the earliest and most intense, emotional responses to pain caused by myocardial ischemia.
In studies of patients with myocardial infarction, an increased level of anxiety was reported by more than two-thirds of patients. In more than one-fourth of patients, it was as high as in people with mental health conditions [10]. In the general population of patients after myocardial infarct, anxiety tensions occurred more often in women than in men [11].
The influence of psychological factors on the etiopathogenesis, treatment, and rehabilitation of the IHD is unquestionable. However we don’t know which of the numerous psychological factors has a direct influence or has the greatest (most essential) influence on the development of the IHD. Therefore, this problem requires multidirectional studies and a thorough analysis of the obtained results [12,13].
Long-term observational studies and clinical trials have shown that anxiety disorders have a considerable influence on the etiopathogenesis of IHD. Anxiety has also been linked to known IHD risk factors. High cholesterol level, a known IHD risk factor, has been reported in patients with anxiety disorders [14]. Anxiety has also been hypothesized to be a risk factor for hypertension in women [15]. Nesse et al. found that patients with panic disorders had an increased adrenergic function (elevated resting heart rate, elevated levels of plasma epinephrine, cortisol and growth hormone, and mildly elevated plasma norepinephrine levels) even in the absence of panic attacks [16]. Increased plasma concentrations of adrenaline and serotonin (5-HT), which have been reported in depressed patients, may contribute to altered platelet function [17]. A meta-analysis suggested that anxiety was also a risk factor for heart attacks and other heart-related events [18]. A significant emotional or physical stressor, or neurologic injury typically precedes the development of the tako-tsubo syndrome, known also as tako-tsubo cardiomyopathy [19]. It can be precipitated by emotional stress, neurologic injury, and numerous other stress states. The most commonly discussed possible mechanism for tako-tsubo cardiomyopathy is stress-induced catecholamine release, with toxicity to and subsequent stunning of the myocardium. Stress-induced cardiomyopathy occurs most commonly in postmenopausal women. Diseases of the heart muscle in their acute stage usually increase symptoms of unease. However, currently, there are few studies that have evaluated this relationship [20].
Conducting studies on the role of anxiety in the etiopathogenesis, treatment and rehabilitation of the IHD may provide an explanation for the possible role of psychological functioning in people with the IHD. Therefore, every approach to the problem may provide significant information.
The aim of this study was to determine the characteristics of both overt and covert anxiety and to examine the impact of the severity of anxiety on five personality traits in women with IHD.
Material and Methods
This study was conducted in the Department of Cardiology of the Medical University in Lublin. The investigated group included 50 women aged 37 to 74 years old, with the mean age of 56.6 years, who had been treated from two months to three years because of IHD. They were admitted to the Department of Cardiology to have angiographic examination and coronary arteries evaluation performed. The qualified patients didn’t have any additional diseases and consented to psychological examinations. Among the study group 29% women had higher education, 52% secondary education, 14% vocational education, and 5% elementary education
Before each examination, a thorough psychological interview was conducted with patients and focused on somatic complaints, neurotic symptoms, mood, family, professional, financial situation, as well as the possibility of treatment.
The level of anxiety was examined using Cattell’s IPAT Anxiety Inventory Personality Scale and Costa and McCrae’s Personality Inventory. The IPAT Anxiety Scale consists of 40 questions. The test describes the level of anxiety using five factors: personal integrity (Q3−), emotional stability (C−), distrustfulness (L+), auto-aggression (O+) and neurotic tension (Q4+). The characteristic features of anxiety as understood by Cattell were connected with personality traits and were manifested as anxiety in stressful situations [21].
The Costa and McCrae NEO-FFI Personality Inventory consists of 60 questions and allows for the evaluation of five aspects of personality: neuroticism (NEU), extraversion (EXT), openness (OPE), agreeableness (AGR), and conscientiousness (CON). It is a five factor model, the so called “Big Five” [22,23].
The study group was divided into two subgroups of women: women with high overt anxiety (hAo) and women with low overt anxiety (lAo). The cut-off value used Ao average value calculated for the entire study group, which was 19.35±7.07.
Bioethics committee approval and informed consent for study participation
Approval for the study was obtained from the Bioethics Committee of the University of Lublin. Informed consent was obtained from each patient and the study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki.
Statistical analysis
Statistical analysis was carried out on an IBM PC using of a standard statistical package (SPSS for Windows Version 12.0; SPSS Inc., Chicago, IL, USA). Results were tested for normality. Data were expressed as mean ±SD (parametrically distributed continuous variables) and percentage (categorical variables). The statistical significance of the differences between subgroups of women with high (hAo) and low (lAo) overt anxiety were compared by unpaired Student’s t-test or the Mann-Whitney test. Probability values of p<0.05 were accepted as significant.
Results
The angiographic evaluation of the coronary vessels allowed determining that the narrowing within one coronary vessel occurred in 24 (48%) patients, in two vessels 13 (26%) patients, and in three vessels in 6 (12%) patients. No changes were stated in 7 (14%) women.
The analyses of the obtained results (based on IPAT Anxiety Scale) are shown in Table 1, which provides information about the structure and intensity of unease and anxiety in women with IHD.
Table 1.
The IPAT Anxiety Scale by R.B. Cattell.
| Factors | X | SD |
|---|---|---|
| Q3− | 4.76 | 1.93 |
| C− | 6.26 | 2.27 |
| L+ | 7.11 | 1.55 |
| O+ | 7.85 | 2.05 |
| Q4+ | 8.38 | 1.84 |
| Ac | 16.38 | 5.57 |
| Ao | 19.35 | 7.07 |
| AN | 7.23 | 1.58 |
Mean values and standard deviations in women with IHD (N=50). Q3− – personality integration; C− – emotional stability; L+ – personal security; O+ – apprehension; Q4+ – psychological tension; Ac – covert anxiety; Ao – overt anxiety; AN – generalized anxiety.
Test results indicated that women with IHD were characterized by a proper level of internal integration, namely personality integration (Q3−). The examined women had no problems with lack of integration and did not experience value crisis. The women with IHD revealed tendencies toward lower emotional stability (C−). They experienced intense feelings of threat and lacked the sense of personal security (L+). High scores in (O+) factor showed that the patients had a strong tendency to blame themselves and they punished themselves with the feeling of guilt for their failures.
The dominating factor in the structure of anxiety and unease was intense psychological tension (Q4+). The patients had a high level of tension associated with the so called “state of frustration”, which is described as the conflict between superego and the impulsive sphere. They had susceptibility to frequent unease and to critical self-esteem. A high level of aspiration and a great sensitivity to all types of failures were also characteristic of these patients.
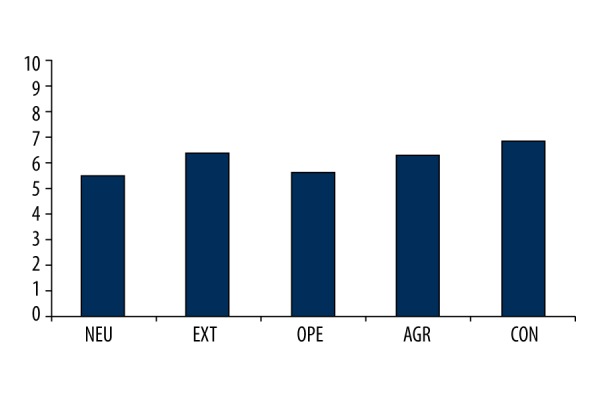
Generalized anxiety and unease (AN) expressed by the patients was a characterological anxiety according to Cattell’s concept, and is associated with personal experiences, internal conflicts, or personal problems. It may also be an expression of a high level of aspirations and high intellectual demands. The women with IHD in our study reported overt anxiety (Ao) when facing direct or alleged threat, which was characteristically higher than patients with covert anxiety (Ac). Table 2 shows the Personality Inventory study results. Women with IHD had moderate results in neuroticism (NEU) and openness factors (OPE). Extroversion (EXT), agreeableness (AGR), and conscientiousness (CON) turned to be dominant factors and above average.
Table 2.
Personality Inventory by P.T. Costa and R.R. McCrae.
| Factors | X | SD |
|---|---|---|
| NEU | 5.45 | 1.62 |
| EXT | 6.33 | 1.64 |
| OPE | 5.57 | 1.87 |
| AGR | 6.23 | 1.57 |
| CON | 6.80 | 1.82 |
Mean values and standard deviations in women with IHD (N=50). NEU – neuroticism; EXT – extroversion; OPE – openness factors; AGR – agreeableness; CON – conscientiousness.
This presentation of factors allows us to characterize the group of women with IHD as generally quiet and balanced persons; although generally experiencing sadness and a sense of guilt (NEU). Activities directed toward their environment revealed an openness and friendly attitude. In social relations they tend to seek stimulation. They try to be warmhearted, sociable, and to live active lives (EXT). They respect traditional values and prefer generally accepted ways of behavior. Their interests are pragmatic (OPE).
Results above the average in the agreeableness factor (AGR) suggested that the women with IHD were prone to offering help to other people. They try to be straightforward, altruistic, sincere, modest, and emotional in their relations to other people. They were characterized by a high level of conscientiousness and strong will, as well as a tendency to maintain order and a striving for perfectionism. Such a presentation of traits motivates patients to be responsible, as well as have persistent and scrupulous actions (CON).
From among the 50 women with IHD, a group of 28 were identified who had overt anxiety (Ao) much higher than covert anxiety (Ac). Comparative analysis (t-test) of these two subgroups of women is shown in Table 3 and Figure 1, and show that the structure of unrest and anxiety in both groups of women with IHD presented a significant diversity.
Table 3.
The IPAT R.B. Cattell’s Anxiety Scale.
| Factors | hAo | lAo | t | p | ||
|---|---|---|---|---|---|---|
| X | SD | X | SD | |||
| Q3− | 5.72 | 1.63 | 3.70 | 1.68 | 1.06 | 0.88 |
| C− | 7.13 | 1.95 | 5.30 | 2.24 | 1.31 | 0.54 |
| L+ | 7.43 | 1.71 | 6.77 | 1.31 | 1.70 | 0.24 |
| O+ | 9.04 | 1.32 | 6.55 | 1.93 | 2.12 | 0.09 |
| Q4+ | 9.63 | 0.72 | 7.00 | 1.71 | 5.58 | 0.000 |
| AN | 8.22 | 1.02 | 6.15 | 1.38 | 1.84 | 0.17 |
Mean values and standard deviation t – values and p – levels in the groups of women with high (hAo, N=28) and low (lAo, N=22) overt anxiety. Q3− – personality integration; C− – emotional stability; L+ – personal security; O+ – apprehension; Q4+ – psychological tension; AN – generalized anxiety.
Figure 1.
The IPAT Anxiety Scale by R.B. Cattell. Profiles of women with IHD (N=50).
Women with a low level of overt unease and anxiety definitely presented with less problems and more coherent personality integration. Women with high overt anxiety were more emotionally changeable (C−), and thus may become impatient more easily and show their disappointment with life. They also were found to worry about life problems more frequently. They had considerable suspiciousness (L+) and less trust towards the environment. They had much stronger tendencies to blame themselves (O+) and intense internal, neurotic tension (Q4+).
Similar study results were obtained using the NEO-FFI Personality Inventory. Table 4 and Figure 2 show obvious diversity in the comparison of women with IHD in the three dimensions (factors) of personality.
Table 4.
Personality Inventory by P.T. Costa and R.R. McCrae.
| Factors | hAo | lAo | t | p | ||
|---|---|---|---|---|---|---|
| X | SD | X | SD | |||
| NEU | 6.22 | 1.44 | 4.60 | 1.39 | 1.07 | 0.87 |
| EXT | 5.81 | 1.56 | 6.90 | 1.58 | 1.03 | 0.94 |
| OPE | 4.68 | 1.86 | 6.55 | 1.35 | 1.88 | 1.17 |
| AGR | 6.09 | 1.23 | 6.40 | 1.90 | 2.38 | 0.05 |
| CON | 6.68 | 1.67 | 6.95 | 2.01 | 1.44 | 0.41 |
Mean values and standard deviation, t – values and p – levels in the groups of women with high (hAo, N=28) and low (lAo, N=22) overt anxiety. NEU – neuroticism; EXT – extroversion; OPE – openness factors; AGR – agreeableness; CON – conscientiousness.
Figure 2.
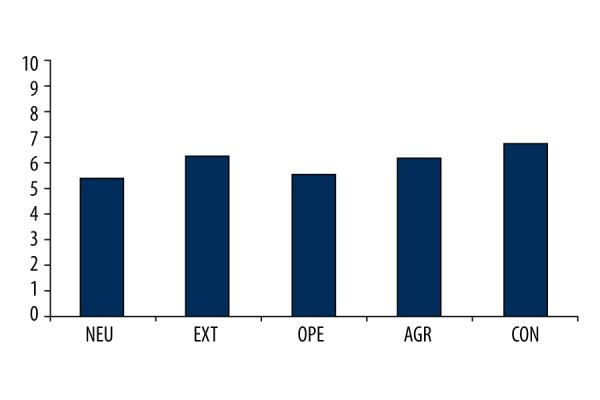
Personality Inventory NEO-FFI by P.T. Costa and R.R. McCrae. Mean values in women with IHD (N=50).
The group of women with a high level of overt anxiety had more neurotic traits (NEU), namely a stronger tendency to react with unease, worry oneself, and experience a nervous breakdown in difficult situations. Thus they establish social relations with more reserve and distance, preferring cautious behavior. Smaller openness to experience (OPE) and more self-concentration was found in this group of women which is connected with pragmatic interests and socially accepted ways of action.
These results informed the next subsequent stage of the study, to define the correlation between unease and anxiety versus personality structure in the group of women with IHD. The results are shown in Table 5. Correlation analyses revealed essential relations between the results obtained by women with IHD in the IPAT Anxiety Scale and NEO-FFI Personality Inventory. They results were most distinct between neuroticism (NEU) and personality integration (Q3−), sense of threat and mistrust (L+), tendency to blame oneself (O+), neurotic tension (Q4+), covert (Ac) and overt anxiety and unease (Ao), and generalized anxiety (AN).
Table 5.
Correlation coefficients (r Pearson’s) between Personality Inventory NEO-FFI by P.T. Costa and R.R. McCrae and The IPAT by R.B. Cattell’s Anxiety Scale.
| NEU | EXT | OPE | AGR | CON | |
|---|---|---|---|---|---|
| Q3− | r=0.48 | r=−0.05 | r=−0.43 | r=−0.42 | r=−0.19 |
| p=0.001 | p=0.7 | p=0.004 | p=0.005 | p=0.2 | |
|
| |||||
| C− | r=0.26 | r=−0.01 | r=0.08 | r=−0.12 | r=−0.18 |
| p=0.09 | p=0.9 | p=0.5 | p=0.4 | p=0.2 | |
|
| |||||
| L+ | r=0.30 | r=0.18 | r=−0.12 | r=−0.11 | r=0.15 |
| p=0.05 | p=0.2 | p=0.4 | p=0.4 | p=0.3 | |
|
| |||||
| O+ | r=0.38 | r=0.13 | r=−0.41 | r=0.07 | r=−0.09 |
| p=0.01 | p=0.3 | p=0.006 | p=0.6 | p=0.5 | |
|
| |||||
| Q4+ | r=0.45 | r=−0.24 | r=−0.18 | r=−0.19 | r=−0.13 |
| p=0.003 | p=0.1 | p=0.2 | p=0.2 | p=0.38 | |
|
| |||||
| Ac | r=0.34 | r=0.10 | r=−0.15 | r=−0.34 | r=−0.18 |
| p=0.02 | p=0.4 | p=0.3 | p=0.02 | p=0.2 | |
|
| |||||
| Ao | r=0.58 | r=−0.10 | r=−0.35 | r=−0.007 | r=−0.14 |
| p=0.000 | p=0.4 | p=0.02 | p=0.9 | p=0.3 | |
|
| |||||
| AN | r=0.52 | r=0.09 | r=−0.30 | r=−0.25 | r=−0.13 |
| p=0.000 | p=0.5 | p=0.05 | p=0.10 | p=0.3 | |
NEU – neuroticism; EXT – extroversion; OPE – openness factors; AGR – agreeableness; CON – conscientiousness; Q3− – personality integration; C− – emotional stability; L+ – personal security; O+ – apprehension; Q4+ – psychological tension; Ac – covert anxiety; Ao – overt anxiety; AN – generalized anxiety.
Interdependence occurred between the openness factor (OPE) and personality integration (Q3−), tendency for self-blaming (O+), overt anxiety (Ao), and general unease (AN). Negative interdependence occurred between agreeableness (AGR) and personality integration (Q3−).
With a moderate level of neuroticism and proper personality integration, patients likely do not experience value crisis and this probably helps them cope with everyday life.
The IHD women did not have a sense of safety. They had a tendency to auto-aggressive reactions and remain in a state of increased emotional tension. These traits support the experience of unease; and 58% of patients expressed this unease in an overt way.
Preserved personality integration likely positively influences agreeableness and openness traits in relation to the environment and surroundings. We found that the women with IHD presented (adopted) agreeable attitudes in relation to social environment.
Discussion
In the 1990s, there was a reported increase in cardiovascular disease, including IHD, in women. Numerous studies and epidemiological reports conducted formerly among men with IHD are now employed in a similar way among women. Because women have in the past were considered a minority of IHD patients, the main methods and standards of conduct in the treatment of IHD focused on men [24].
At the end of the 1970s, scientific studies revealed diversities concerning epidemiology, diagnosing, pathomechanism, disease course, and prognoses in women’s heart disease, including IHD. Attention was drawn to “feminine” factors, such as the risk of myocardial infarct being twice as high in women smoking cigarettes in comparison to men. Particular significance began to be ascribed to two risk factors: cigarette smoking and the use of oral contraceptives by young women.
The lack of family support and solitude has been reported to be one of the main factors related to myocardial infarct and sudden cardiac death [1]. Studies have drawn attention to depression as an influencer on the development and course of the IHD both in women and men. A study conducted among young women who had a heart attack revealed that they suffered from depression, and that the increase of depression symptoms was much higher than reported in men [25]. Depression is closely related to endothelial dysfunction. Endothelial dysfunction is a critical step in the development of cardiovascular disease, such as hypertension, atherosclerosis, and thrombosis. The improvement of depression is synchronous with the improvement of endothelial function [26].
Anxiety disorders among patients with cardiovascular disease have not been studied or described as thoroughly as depression. They are currently the subject of studies in numerous scientific research centers both in American and European countries. Anxiety itself is the first and most dominant emotional reaction to the manifestation of coronary disorders.
Research conducted by Frasure-Smith et al. among patients treated because of myocardial infarction found increased levels of anxiety in two-thirds of patients and intensification of anxiety disorders in one-fourth of patients with mental illnesses [10]. In the general population of people with cardiovascular disease, anxiety disorders occur more often in women than in men [11].
An international prospective studies conducted by Moser et al. among women from Australia, England, Japan, South Korea, and the USA found that women after myocardial infarct showed higher levels of anxiety than men; and a high level of anxiety in women was maintained despite providing them with social support and psychological help [27].
A 20-year prospective observational study initially conducted among healthy women by Eaker et al. as part of the Framingham study found a relationship between co-existence of anxiety disorders and myocardial infarct; a correlation was found between the occurrence of anxiety attacks and sudden cardiac deaths [28]. Anxiety, therefore, was treated as an independent factor predisposing to ischemic heart disease.
Stress plays a major role in various pathophysiological processes associated with the circulatory system [29]. In recent years, much attention has been devoted to neurotic changes in IHD. It has been confirmed that neurotic changes co-exist with IHD clinical symptoms but they are not always related to the presence of atheromatous changes in the coronary vessels.
Costa et al. conducted studies among patients with ischemic heart disease are widely known. These authors have presented personality structure in five dimensions: neuroticism, extroversion, openness, agreeableness, and conscientiousness. Neuroticism, one of the five personality dimensions, includes six specific personality traits: anxiety, hostility, depression, shyness, impulsiveness, and susceptibility to traumas. Their study tried to answer the question of whether increased levels of neurotic changes may lead to the development of ischemic heart disease. These studies conducted among patients with IHD revealed that stenocardiac complaints co-exist with the increased level of neurotic changes. Some neurotic traits, such as hostility and lowered mood-depression, were thought to be IHD risk factors. However, no explicit answer to the question of whether neuroticism may be regarded as an IHD risk factor was obtained; however, their study results showed that there was a close correlation between neuroticism and IHD [30,31].
Results of our study allowed us to characterize unease and anxiety in a group of 50 women with IHD. The women had a high level of unease and generalized anxiety. In more than half of patients, their anxiety adopted an apparent form. The dominant anxiety factor structure was: internal tension (neurotic), auto-aggression syndrome, and lowered emotional stability. Women with IHD showed a low tolerance to problems and stress, neurotic fatigability, as well as mistrust and the lack of safety. The women, who were characterized by a high anxiety level, internal tension, and openness, had a tendency to overload themselves with responsibilities and to feel extremely responsible. It is possible that a high level of anxiety may also be a reaction to the fact of being ill.
Our study results demand further continuation among larger population of women with ischemic heart disease.
Conclusions
In our study, women with IHD were found to have a high level of unease and anxiety. This may be an emotional reaction to a direct threat or the expected threat (anticipated). In this group of women, personality integration was preserved. We concluded that a high level of unease and anxiety could result from lack of personality harmony, lack of personality integrity, or experienced value crises. Internal tension, auto-aggression, lowered emotional stability, and a sense of threat dominated the structure of unease and anxiety. The structure of unease and anxiety presented by women with IHD was thus related to Cattell’s conception of psychosomatic anxiety.
Footnotes
Source of support: Departmental sources
References
- 1.Mosca L, Banka CL, Benjamin EJ, et al. Evidence-based guidelines for cardiovascular disease prevention in women: 2007 update. J Am Coll Cardiol. 2007;49:1230–50. doi: 10.1016/j.jacc.2007.02.020. [DOI] [PubMed] [Google Scholar]
- 2.Silent Epidemic (The Truth About Women and Heart Disease) Dallas, Tex: American Heart Association; 1989. Publication no. 64–9571. [Google Scholar]
- 3.Mieres JH, Gulati M, Bairey Merz N, et al. American Heart Association Cardiac Imaging Committee of the Council on Clinical Cardiology; Cardiovascular Imaging and Intervention Committee of the Council on Cardiovascular Radiology and Intervention. Role of noninvasive testing in the clinical evaluation of women with suspected ischemic heart disease: A consensus statement from the American Heart Association. Circulation. 2014;130:350–79. doi: 10.1161/CIR.0000000000000061. [DOI] [PubMed] [Google Scholar]
- 4.Karnowska A. Anxiety and coronary heart disease. Pol Merkuriusz Lek. 2008;24:481–83. [PubMed] [Google Scholar]
- 5.Doyle F, McGee H, Conroy R, et al. Systematic review and individual patent data meta-analysis of sex differences in depression and prognosis in persons with myocardial infraction: A MINDMAPS Study. Psychosom Med. 2015;77:419–28. doi: 10.1097/PSY.0000000000000174. [DOI] [PubMed] [Google Scholar]
- 6.Watkins LI, Blumenthal S, Davidson IR, et al. Phobic anxiety, depression and risk of ventricular arrhythmias in patients with coronary heart disease. Psychosom Med. 2006;68:651–57. doi: 10.1097/01.psy.0000228342.53606.b3. [DOI] [PubMed] [Google Scholar]
- 7.Jacobs S, Sherwood J. The cardiac psychology of women and heart disease. In: Allan R, Scheidt S, editors. Heart and mind. American Psychiatric Association; Washington, D.C.: 1996. [Google Scholar]
- 8.Kannel W. Silent myocardial ischemia and infarction: insights from the Framingham study. Cardiology Clinics. 1986;4(4):583–91. [PubMed] [Google Scholar]
- 9.Kowman M, Sobów T, Kłoszewska I. Anxiety and anxiety disorders in heart disease. Wiad Psych. 2007;10(2):109–15. [Google Scholar]
- 10.Frasure-Smith N. Hospital symptoms of psychological stress as predictors of long-term outcome after acute myocardial infarction in men. Am J Cardiol. 1991;67:121–27. doi: 10.1016/0002-9149(91)90432-k. [DOI] [PubMed] [Google Scholar]
- 11.Fleet R, Lavoie K, Beitman BD. Is panic disorder associated with coronary artery disease? A critical review of the literature. J Psychosom Res. 2000;48:347–56. doi: 10.1016/s0022-3999(99)00101-4. [DOI] [PubMed] [Google Scholar]
- 12.Frasure-Smith N, Lesperance F, Talajic M. The impact of negative emotions on prognosis following myocardial infarction is it more than depression? Health Psychology. 1995;14:388–98. doi: 10.1037//0278-6133.14.5.388. [DOI] [PubMed] [Google Scholar]
- 13.Kothawade K, Bairey Merz CN. Microvascular coronary dysfunction in women: Pathophysiology, diagnosis and management. Curr Probl Cardiol. 2011;36:291–318. doi: 10.1016/j.cpcardiol.2011.05.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Bajwa WK, Asnis GM, Sanderson WC, et al. High cholesterol levels in patients with panic disorder. Am J Psychiatry. 1992;149:376–78. doi: 10.1176/ajp.149.3.376. [DOI] [PubMed] [Google Scholar]
- 15.Markovitz JH, Matthews KA, Wing RR, et al. Psychological, biological and health behavior predictors of blood pressure changes in middle-aged women. J Hypertens. 1991;9:399–400. doi: 10.1097/00004872-199105000-00003. [DOI] [PubMed] [Google Scholar]
- 16.Nesse RM, Cameron OG, Curtis GC, et al. Adrenergic function in patients with panic anxiety. Arch Gen Psychiatry. 1984;41:771–76. doi: 10.1001/archpsyc.1984.01790190045005. [DOI] [PubMed] [Google Scholar]
- 17.Larrson PT, Hjemdahl P, Olsson G, et al. Altered platelet function during mental stress and adrenaline infusion in humans: Evidence for an increased aggregability in vivo as measured by filtragometry. Clin Sci. 1989;76:369–76. doi: 10.1042/cs0760369. [DOI] [PubMed] [Google Scholar]
- 18.Roest AM, Martens EJ, de Jonge P, Denollet J. Anxiety and risk of incident coronary heart disease. A meta-analysis. J Am Coll Cardiol. 2010;56:38–46. doi: 10.1016/j.jacc.2010.03.034. [DOI] [PubMed] [Google Scholar]
- 19.Boland TA, Lee VH, Bleck TP. Stress-induced cardiomyopathy. Crit Care Med. 2015;43:686–93. doi: 10.1097/CCM.0000000000000851. [DOI] [PubMed] [Google Scholar]
- 20.Kubzansky LD, Kawachi I. Anxiety and coronary heart disease a synthesis of epidemiological, psychological and experimental evidence. Ann Behav Med. 1998;20(2):47–58. doi: 10.1007/BF02884448. [DOI] [PubMed] [Google Scholar]
- 21.Cattell RB, Scheier IH. Handbook the IPAT Anxiety Scale Questionire. Institute for Personality and Ability Testing; Illinois: 1967. [Google Scholar]
- 22.Costa PT, Jr, McCrae RR. Profesional manual. Odessa, Fl: Psychological Assessment Resources; 1992. Revised NEO Personalisty Inventory (NEO-PI-R) and NEO Five-Factor Inventory (NEO-FFI) [Google Scholar]
- 23.McCrae RR, Costa PT., Jr A contemplated revision of the NEO Five-Factor Inventory. Personality and Individual Differences. 2004;36:587–96. [Google Scholar]
- 24.American Heart Association. Heart and Stroke Facts: 1996 Statistical Supplement. Dallas, Tex: American Heart Association; 1996. p. 1. [Google Scholar]
- 25.Fraure-Smith N, Lesperance F, Juneau M, et al. Gender, depression and one-year prognosis after myocardial infarction. Psychosom Med. 1993;61(1):26–37. doi: 10.1097/00006842-199901000-00006. [DOI] [PubMed] [Google Scholar]
- 26.Shi H, Feng G, Wang Z, et al. Relationships between depressive symptoms and endothelial function among outpatients of a general hospital in China. Med Sci Monit. 2015;21:1812–19. doi: 10.12659/MSM.893531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Moser DK, Dracup K, McKinley S, et al. An international prospective on gender differences in anxiety early after acute myocardial infarction. Psychosom Med. 2003;65:511–16. doi: 10.1097/01.psy.0000041543.74028.10. [DOI] [PubMed] [Google Scholar]
- 28.Eaker ED, Pinsky J, Castelli WP. Myocardial infarction and coronary death among women psychosocial predictors from a 20-year follow-up of women in the Framingham Study. Amer J Epid. 1992;135(8):854–64. doi: 10.1093/oxfordjournals.aje.a116381. [DOI] [PubMed] [Google Scholar]
- 29.Esch T, Stefano GB, Fricchione GL, Benson H. Stress in cardiovascular diseases. Med Sci Monit. 2002;8(5):RA93–101. [PubMed] [Google Scholar]
- 30.Costa PT, Zonderman AB, Engel BT, et al. The relation of chest pains symptoms to angiographic findings of coronary artery stenosis and neurotcism. Psychosom Med. 1985;47(3):285–93. doi: 10.1097/00006842-198505000-00006. [DOI] [PubMed] [Google Scholar]
- 31.Costa PT. Influence of the normal personality dimension of neuroticism on chest pain symptoms and coronary artery disease. Am J Cardiol. 1987;60:250–61. doi: 10.1016/0002-9149(87)90679-5. [DOI] [PubMed] [Google Scholar]