

Abstract
Background
Home visits have been shown to improve quality of care, save money, and improve outcomes. Primary care physicians are in an ideal position to provide these visits; of note, the Accreditation Council for Graduate Medical Education no longer requires home visits as a component of family medicine residency training.
Objective
To investigate changes in home visit numbers and expectations, attitudes, and approaches to training among family medicine residency program directors.
Methods
This research used the Council of Academic Family Medicine Educational Research Alliance (CERA) national survey of family medicine program directors in 2015. Questions addressed home visit practices, teaching and evaluation methods, common types of patient and visit categories, and barriers.
Results
There were 252 responses from 455 possible respondents, representing a response rate of 55%. At most programs, residents performed 2 to 5 home visits by graduation in both 2014 (69% of programs, 174 of 252) and 2015 (68%, 172 of 252). The vast majority (68%, 172 of 252) of program directors expect less than one-third of their graduates to provide home visits after graduation. Scheduling difficulties, lack of faculty time, and lack of resident time were the top 3 barriers to residents performing home visits.
Conclusions
There appeared to be no decline in resident-performed home visits in family medicine residencies 1 year after they were no longer required. Family medicine program directors may recognize the value of home visits despite a lack of few formal curricula.
What was known and gap
While home visits have many benefits, the ACGME removed a requirement for home visits for family medicine (FM) residents.
What is new
A survey of FM program directors finds little change in home visit practices after removal of the requirement.
Limitations
Response and social desirability bias; findings may be premature to detect permanent changes in home visit practices.
Bottom line
Program directors may recognize the value of home visits despite an absence of requirements and a lack of formal curricula.
Introduction
Home visits were once a major mode of health care delivery, but most physician services are now provided in clinic and hospital settings.1 Patients are growing older, more medically complex, and often experience costlier and more fragmented care. This has led to calls for change in the health care delivery system.2,3 Evidence suggests that home visits can help achieve the “Triple Aim”: decreased health care costs, improved care experience of patients, and improved health of the population.4 The Independence at Home demonstration is following providers who deliver primary care in the home to Medicare patients.5 In the first year, it has already shown cost savings of $3,070 per beneficiary, in addition to improved quality of care measures such as decreases in emergency department visits and hospital readmissions.6 Home visits have also been shown to increase patient and caregiver satisfaction.7,8 However, perceptions that home visits are time consuming, inadequately reimbursed, and lack diagnostic capabilities may cause some clinicians to shy away from this care modality.9–11
Despite these obstacles, home visits by primary care providers have been growing in number in recent years. Physician home visits to Medicare beneficiaries doubled between 2000 and 2006, and steadily rose through 2011.12,13 Advanced practitioner (physician assistants and nurses) visits have also increased, and comprised 25% of all home visits billed to Medicare patients in 2013.14 Physician-led, team-based approaches combining advanced practitioners with pharmacists, nurses, and social workers are becoming a dominant mode of health care delivery associated with improved patient outcomes.15–17
Previously, family medicine (FM) residents were required to complete at least 2 home visits during residency. In 2014, the Accreditation Council for Graduate Medical Education (ACGME) transitioned to a competency-based model, and no longer required completion of home visits.18 It is possible that without a specific requirement, home visits will recede from residency training. We suspect that the effect of the ACGME requirement change may relate to the perception by FM residency program directors of the value of home visits and current practices. There is little information on how program directors perceive home visits, and how the new competency-based requirement will be met. We aimed to investigate changes in home visit education, and to examine current FM program directors' expectations, attitudes, and approaches to training.
Methods
This survey was part of the Council of Academic Family Medicine Educational Research Alliance (CERA) national omnibus survey of FM program directors, containing questions on 4 topics (laborists, group visits, home visits, and patient-centered medical homes). The methods for data collection have been documented.19 Data were collected from June to July 2015.
The survey included questions on program director and departmental demographics, current home visit training curricula and evaluation methods, needs for improvement, common types of patients and visit categories, and barriers to home visit education. The authors developed the survey with multiple-choice, rank-the-top-3, and fill-in-the-blank responses. It was piloted for readability, flow, and relevance by a program director and revised based on feedback.
The study was approved by the American Academy of Family Physicians Institutional Review Board.
Descriptive statistics were used to characterize the data. Basic statistical measures (means, medians, and 1-way frequency distributions) were calculated to describe responses for each question. Two-way contingency tables examined associations between program type, number of home visits performed, and community size. Statistical analysis was performed using SAS version 9.0 (SAS Institute Inc, Cary, NC).
Results
The survey was sent to 455 FM program directors, with a resulting 252 responding (55% response rate). All questions were optional in the survey, and the section on home visits had the highest average response rate at 92% (232 of 252) for each item, with the other sections averaging 63%, 88%, and 85% (data not shown).
Survey Respondent Demographics
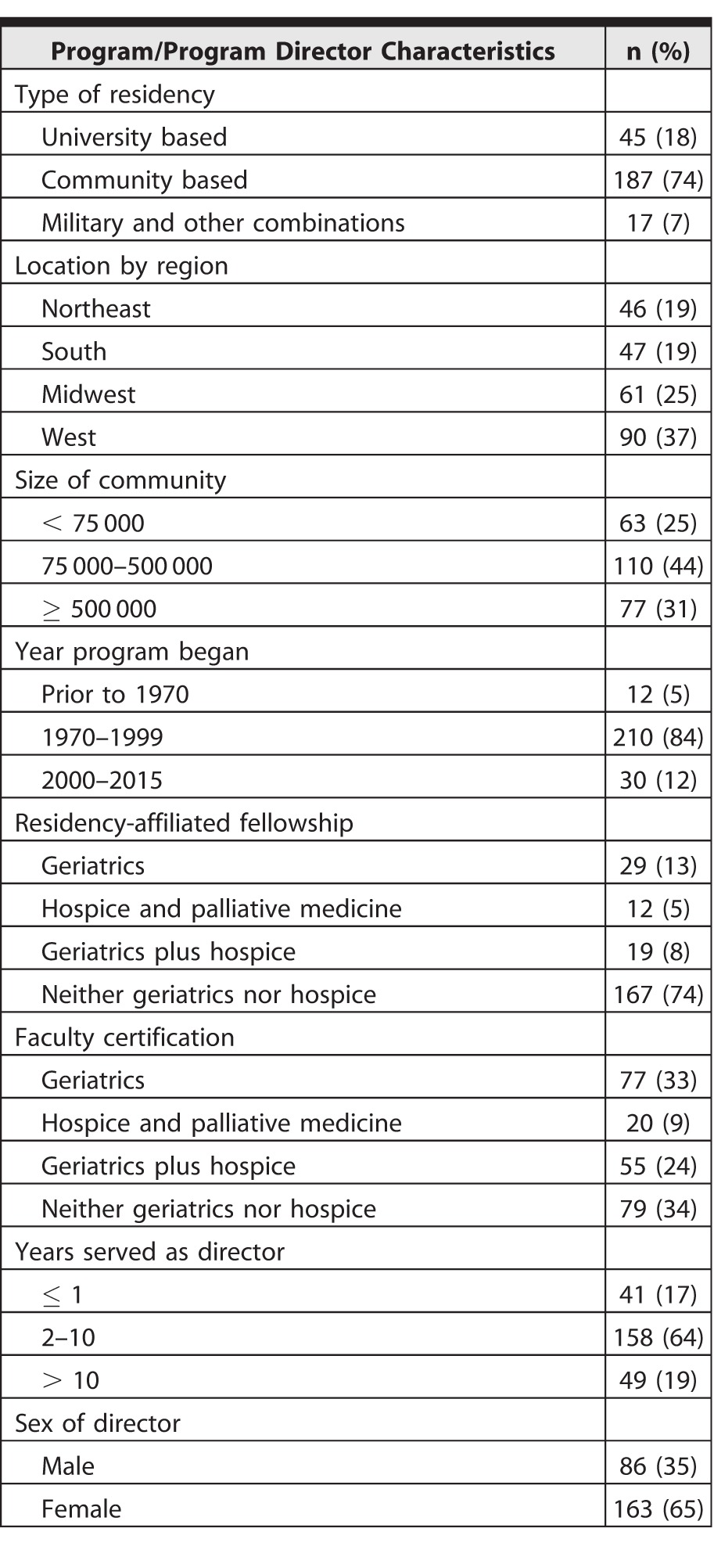
Respondents were mostly from community-based residency programs (74%, 187 of 252), followed by university-based programs (18%, 45 of 252; table 1). Although communities of 75 000 to 500 000 people were home to the most programs (44%, 110 of 252), 25% of programs (63 of 252) were in communities with less than 75 000 people. A total of 12% (29 of 252) of residencies reported having a geriatrics fellowship, 5% (12 of 252) a hospice/palliative care medicine fellowship, and 8% (19 of 252) had both.
Table 1.
Characteristics of Family Medicine Residency Programs and Program Directors (N = 252)
Current State of Home Visit Education at FM Residency Programs
Family medicine program directors reported residents performed similar numbers of home visits in 2014 and 2015 (table 2). At most programs, residents performed 2 to 5 home visits (69% [174 of 252] in 2014 and 68% [172 of 252] in 2015) by the time of graduation. At some programs, residents did not perform any home visits (3% [8 of 252] in 2014, 2% [5 of 252] in 2015), and in some programs, residents performed more than 10 home visits (7% [18 of 252] for both years). There was no statistical difference in the number of home visits, based on the program type or community size in which the program was located (data not shown).
Table 2.
State of Home Visit Education at Family Medicine Residency Programs in 2015 (N = 252)
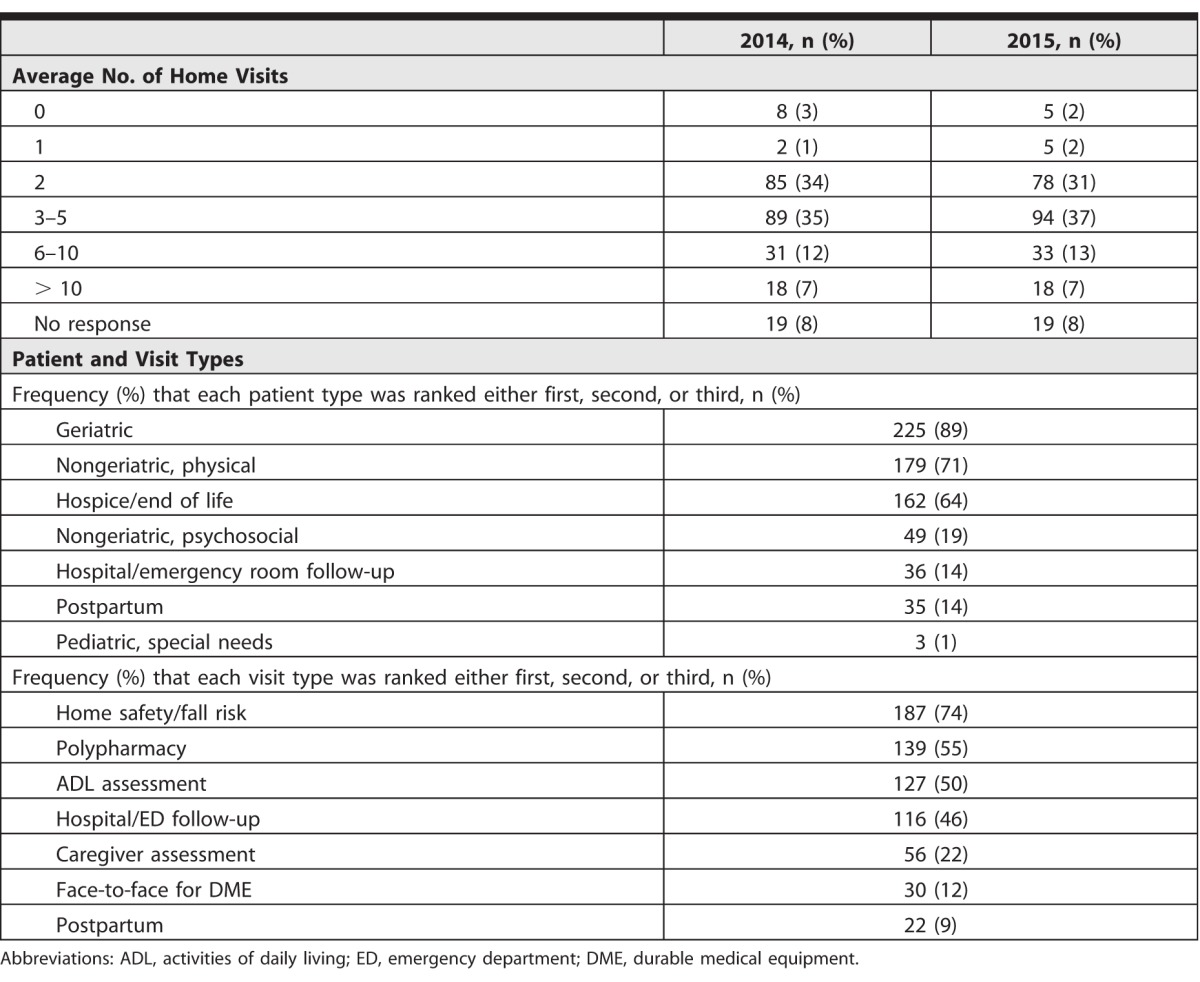
Geriatrics patients, nongeriatric patients for physical assessment, and hospice/end-of-life patients were the 3 most common types of patients seen at home. This aligned with the 3 most common reasons for performing a home visit: home safety/fall risk assessment, polypharmacy, and activities of daily living assessment (table 2), suggesting internal consistency in responses. The majority of FM program directors (68%, 172 of 252) expected less than one-third of their graduates to include home visits in their patient care practice after graduation.
Teaching and Evaluations of Home Visits
Overall, 67% (170 of 252) of respondents thought their residents performed enough home visits to achieve competence (provided as online supplemental material), and 56% (140 of 252) of home visits are performed under direct supervision of faculty. However, some programs do not evaluate residents' home visits (7%, 17 of 252), and at other programs residents simply report completion of home visits (13%, 33 of 252). While 57% (143 of 252) of programs reported that all of their faculty members are competent to supervise home visits, 16% (40 of 252) of programs stated that less than one-third of their faculty can competently supervise a home visit.
Perceptions and Attitudes of Program Directors
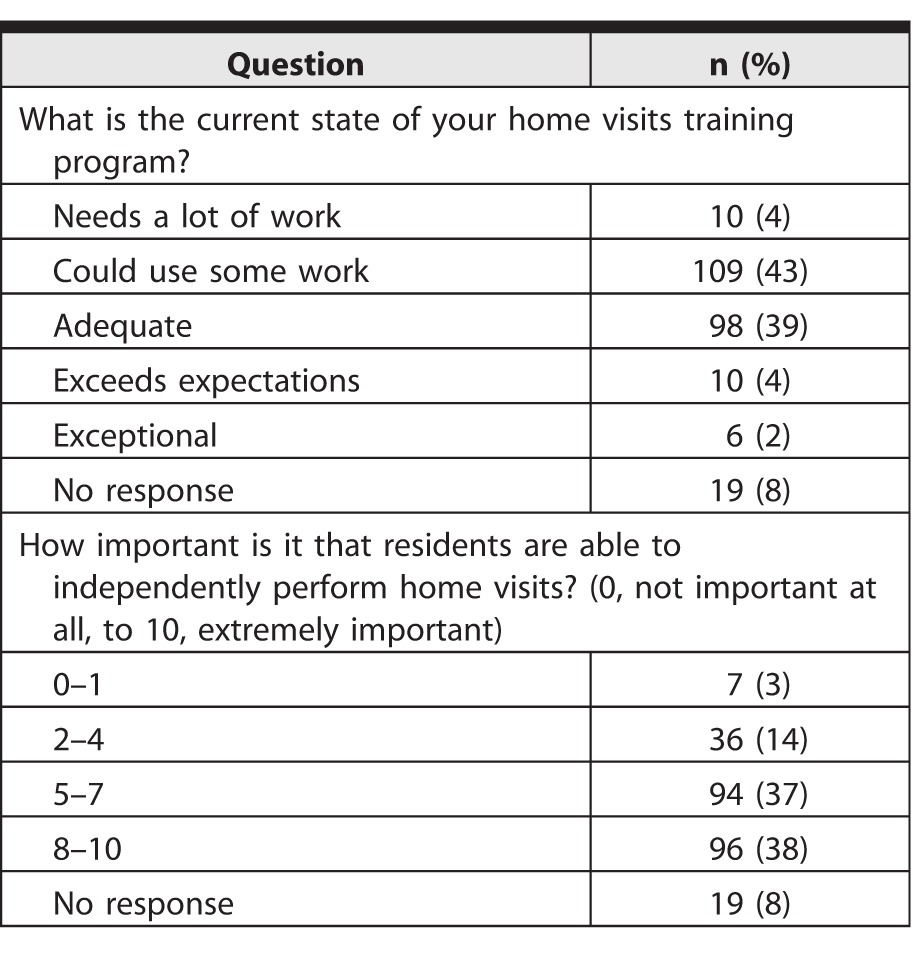
Approximately half of FM program directors reported that their home visit training programs need either some or a lot of work for improvement (table 3). On a scale from 0 to 10 (0, least important, to 10, most important), 38% (96 of 252) rated the importance that residents are able to perform home visits independently by graduation an 8 to 10.
Table 3.
Perceptions and Attitudes of Program Directors Regarding Home Visits (N = 252)
Barriers to Home Visit Education
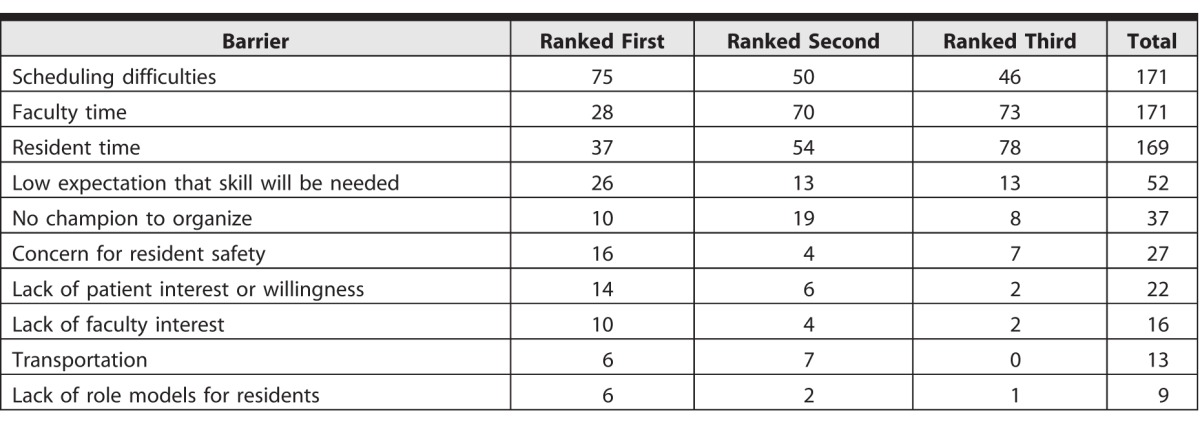
The survey collected 687 rankings for first, second, and third of 10 possible barriers to home visits for FM residents (table 4). Scheduling difficulties, faculty time, and resident time accounted for 74% (511 of 687) of the total votes.
Table 4.
Ranking of the Top 3 Barriers to Resident Home Visits
Discussion
There was little change in the number of home visits performed by FM residents by the time of graduation between 2014 and 2015, despite the removal of the ACGME requirement for home visits. This suggests that FM program leadership still value the experience provided by home visits.
Broaden the Scope: Types of Patients and Visit Types
Geriatrics patients, homebound patients, and patients at the end of life/hospice were the most common types of patients seen on home visits; however, home visits could additionally benefit other patient populations. Home visits can be used for “hot-spotting,” or identifying patients who are high utilizers of physician's offices, emergency rooms, and hospitals to improve individual health.20 Often, these patients not only have challenging health care needs, but also complex social situations. There is also the idea of “cold-spotting”: identifying communities with disintegrated social determinants of health, little community support, and poor access to primary care.21 These cold spots may be amenable to approaches that connect primary care and public health for the improvement of health in a population. Though social history can be investigated in many ways, home visits allow practitioners a more comprehensive view of the social determinants of a patient's health.22,23
Adjusting Expectations and Responding to Societal Needs
If residents are not expected to use a skill, a cascade of events may occur. A residency program is less inclined to invest time, energy, and resources into teaching, and the level of trainee competency becomes irrelevant. One-half of program directors reported that they expect only 10% or fewer of their graduates to perform home visits. This may explain why 69% of FM program directors felt that their graduates had done the “right amount” of home visits, although 35% did 2 or fewer home visits and 72% performed 5 or fewer.
We anticipate that the results of the Independence at Home demonstration will impact health policies and Medicare coverage regarding home visits.5 Given the “Quadruple Aim” (Triple Aim + provider satisfaction),24 aging demographics, and growing financial incentives, the need for practitioners who can provide home visits will likely increase. There is also resident interest; a recent report shows that 44% of FM residents intend to provide home visits after graduation.25 When residents have been trained they are more likely to engage in an activity after graduation, as demonstrated in quality improvement domains.26 This may be a good opportunity to readjust program directors' expectations and reinforce training in home visits.
Home Visits as Opportunities to Teach and Evaluate Residents
This survey found that 60% of programs provide direct faculty supervision of home visits (provided as online supplemental material). Although securing faculty time may be challenging, their presence at a home visit is worth the effort. Faculty members can be role models for residents, as being in the patient's home may present an entirely different and challenging social dynamic. Additionally, home visits can be billed for, whereas independently performed resident visits cannot, as they are not covered by the primary care exception rule. Discussions on the diversification of home visit models such as concierge, academic, and Veterans Affairs–associated practices could ensue, with discourse on how each functions in the health care system. Perhaps most importantly, home visits are a valuable chance to evaluate residents. Direct observation is recognized as the best method to evaluate clinical skills.27 Only 46% of observed residents were evaluated.
Home visits have been shown to fulfill all of the ACGME competencies,28 and relate to at least 16 of the 22 Family Medicine Milestone Project subcompetencies (patient care 1–4, medical knowledge 1–2, systems-based learning 2–4, practice-based learning and improvement 1–3, professionalism 1–3, communication 1–3).12 Direct observation aligned with these subcompetencies and milestones could greatly inform resident performance and assessment. These opportunities to intentionally teach and deliberately evaluate should not be missed.
Improving Home Visit Curricula
Almost half of programs stated that their home visit training program needs either some or a lot of improvement to prepare residents to provide home visits independently. A variety of means for improvement were mentioned, but the method of providing residents opportunity for longitudinal care of patients at home was least popular. Experiential learning has been an effective method to develop home visits skills for internal medicine residents,29 but barriers—faculty time, scheduling, and/or resident time—make it difficult to implement.
This study has several limitations, including the response rate of 55%.30 Response bias and social desirability may be present, where program directors with a more favorable attitude toward home visits were more likely to complete this portion of the survey. Another limitation is that this survey is not a direct assessment of home visit training programs, but of program directors' perceptions. Finally, the conclusion that the removal of the ACGME requirement did not change home visits as part of FM residency curriculum may be premature, as the requirement change occurred only 1 year prior to the study.
Conclusion
This study, the first to investigate current home visit training in US FM programs, did not find a change in the number of home visits performed by FM residents 1 year after removal of the ACGME home visit requirement. Scheduling difficulties, faculty time, and resident time were the main barriers reported in performing home visits. Family medicine program directors believed that a minority of residents would continue to perform home visits after graduation, in contrast to some health care trends that demonstrate increased utility of home visits for selected populations.
Supplementary Material
References
- 1. Starr P. . The Social Transformation of American Medicine. Reprint ed. New York, NY: Basic Books; 1982. [Google Scholar]
- 2. Lochner KA, Cox CS. . Prevalence of multiple chronic conditions among Medicare beneficiaries, United States, 2010. Prev Chronic Dis. 2013; 10: E61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. The National Institute for Health Care Management Foundation. Health care's 1%: the extreme concentration of US health spending. November 2014. http://www.nihcm.org/categories/chart_story/health-care-one-percent-extreme-concentration-cc. Accessed October 27, 2016. [Google Scholar]
- 4. Saultz JW, Jones SM, McDaniel SH, et al. A new foundation for the delivery and financing of American health care. Fam Med. 2015; 47 8: 612– 619. [PubMed] [Google Scholar]
- 5. Centers for Medicare & Medicaid Services. Independence at Home demonstration. http://innovation.cms.gov/initiatives/independence-at-home. Accessed October 27, 2016. [Google Scholar]
- 6. Centers for Medicare & Medicaid Services. Affordable Care Act payment model saves more than $25 million in first performance year. https://www.cms.gov/Newsroom/MediaReleaseDatabase/Press-releases/2015-Press-releases-items/2015-06-18.html. Accessed October 27, 2016. [Google Scholar]
- 7. Cryer L, Shannon SB, Van Amsterdam M, et al. Costs for “hospital at home” patients were 19 percent lower, with equal or better outcomes compared to similar inpatients. Health Aff (Millwood). 2012; 31 6: 1237– 1243. [DOI] [PubMed] [Google Scholar]
- 8. Edes T, Kinosian B, Vuckovic NH, et al. Better access, quality, and cost for clinically complex veterans with home-based primary care. J Am Geriatr Soc. 2014; 62 10: 1954– 1961. [DOI] [PubMed] [Google Scholar]
- 9. Theile G, Kruschinski C, Buck M, et al. Home visits—central to primary care, tradition or an obligation? A qualitative study. BMC Fam Pract. 2011; 12: 24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Stall N, Nowaczynski M, Sinha SK. . Back to the future: home-based primary care for older homebound Canadians: part 2: where we are going. Can Fam Physician. 2013; 59 3: 243– 245. [PMC free article] [PubMed] [Google Scholar]
- 11. Eaton B. . Why we do not make housecalls. Can Fam Physician. 2000; 46: 1945– 1947, 1957–1959. [PMC free article] [PubMed] [Google Scholar]
- 12. Peterson LE, Landers SH, Bazemore A. . Trends in physician house calls to Medicare beneficiaries. J Am Board Fam Med. 2012; 25 6: 862– 868. [DOI] [PubMed] [Google Scholar]
- 13. Sairenji T, Jetty A, Peterson LE. . Shifting patterns of physician home visits. J Prim Care Community Health. 2016; 7 2: 71– 75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. The Moran Company. Physician/supplier procedure summary (PSPS) master record file for Medicare Part B summary data, 2005–2013. https://aahcm.site-ym.com/resource/resmgr/News_Room/AAHCM_Units_Specialty_Catgr.xlsx. Accessed October 27, 2016. [Google Scholar]
- 15. Flanagan P, Virani A, Baker W, et al. Pharmacists making house calls: innovative role or overkill? Can J Hosp Pharm. 2010; 63 6: 412– 419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Beck RA, Arizmendi A, Purnell C, et al. House calls for seniors: building and sustaining a model of care for homebound seniors. J Am Geriatr Soc. 2009; 57 6: 1103– 1109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Leff B, Weston CM, Garrigues S, et al. Home-based primary care practices in the United States: current state and quality improvement approaches. J Am Geriatr Soc. 2015; 63 5: 963– 969. [DOI] [PubMed] [Google Scholar]
- 18. Accreditation Council for Graduate Medical Education. ACGME program requirements for graduate medical education in family medicine. July 2016. http://www.acgme.org/portals/0/pfassets/programrequirements/120_family_medicine_2016.pdf. Accessed October 27, 2016. [Google Scholar]
- 19. Mainous AG III, Seehusen D, Shokar N. CAFM. Educational Research Alliance (CERA) 2011 Residency Director survey: background, methods, and respondent characteristics. Fam Med. 2012; 44 10: 691– 693. [PubMed] [Google Scholar]
- 20. Gawande A. The hot spotters: can we lower medical costs by giving the neediest patients better care? New Yorker. January 2011: 40–51. [PubMed] [Google Scholar]
- 21. Westfall JM. . Cold-spotting: linking primary care and public health to create communities of solution. J Am Board Fam Med. 2013; 26 3: 239– 240. [DOI] [PubMed] [Google Scholar]
- 22. Dattalo M, Nothelle S, Tackett S, et al. Frontline account: targeting hot spotters in an internal medicine residency clinic. J Gen Intern Med. 2014; 29 9: 1305– 1307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Pimlott N. . Whither the housecall? Can Fam Physician. 2013; 59 3: 234. [PMC free article] [PubMed] [Google Scholar]
- 24. Unwin BK, Jerant AF. . The home visit. Am Fam Physician. 1999; 60 5: 1481– 1488. [PubMed] [Google Scholar]
- 25. Coutinho AJ, Cochrane A, Stelter K, et al. Comparison of intended scope of practice for family medicine residents with reported scope of practice among practicing family physicians. JAMA. 2015; 314 22: 2364– 2372. [DOI] [PubMed] [Google Scholar]
- 26. Diaz VA, Carek PJ, Johnson SP. . Impact of quality improvement training during residency on current practice. Fam Med. 2012; 44 8: 569– 573. [PubMed] [Google Scholar]
- 27. Holmboe ES. . Faculty and the observation of trainees' clinical skills: problems and opportunities. Acad Med. 2004; 79 1: 16– 22. [DOI] [PubMed] [Google Scholar]
- 28. Hayashi J, Christmas C. . House calls and the ACGME competencies. Teach Learn Med. 2009; 21 2: 140– 147. [DOI] [PubMed] [Google Scholar]
- 29. Hayashi J, Christmas C, Durso SC. . Educational outcomes from a novel house call curriculum for internal medicine residents: report of a 3-year experience. J Am Geriatr Soc. 2011; 59 7: 1340– 1349. [DOI] [PubMed] [Google Scholar]
- 30. Society of Teachers of Family Medicine. CERA data clearinghouse. http://www.stfm.org/Research/CERA/CERADataClearinghouse. Accessed October 27, 2016. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.