

Abstract
Background & objectives:
The age at which menopause naturally occurs may reflect nutritional and environmental circumstances as well as genetic factors. In this study we examined natural menopause as a marker of women's health at the population level in India and in some major States.
Methods:
Data from the Indian District Level Household Survey (DLHS) carried out during 2007-2008 covering 643,944 ever-married women aged 15-49 yr were used; women of older ages were not included in this survey. Since not all women in this age group had achieved natural menopause at the time of survey, Cox proportional hazard regression models were employed to obtain the median age of women reporting a natural menopause, excluding those who underwent hysterectomy. Hazard ratios (HRs) were estimated for key socio-economic and reproductive variables that could potentially affect the age at natural menopause <40 yr.
Results:
Overall, menopause prior to age 40 was reported by approximately 1.5 per cent of women. In the national data set, significant associations with age at natural menopause were identified with marriage breakdown or widowhood, poverty, Muslim religious affiliation, ‘scheduled caste’ status, not having received schooling, rural residence, having never used contraceptive pills, not been sterilized or had an abortion, low parity and residence in the western region. Within data from five selected States examined separately, the strength of these associations varied.
Interpretation & conclusions:
Associations of natural menopause with sociocultural, family planning and demographic variables were noted. Most importantly, there was an association with poverty that would require further investigation as to causality. The proportion of women experiencing early menopause may represent a useful overall indicator of women's health. The data are reassuring with regard to possible late effects of sterilization on ovarian function.
Keywords: DLHS, female sterilization, India, natural menopause, natural premature menopause, oral pill
The World Health Organization defines natural menopause as the permanent cessation of menstruation resulting from the loss of ovarian follicular activity without an obvious intervening cause and is confirmed only after 12 consecutive months of amenorrhoea. In general, the natural menopause occurs between 45 and 55 yr of age1. In India, the range of mean age at menopause reported in different studies appears to be rather young, between 41.9 and 49.42. With regard to menopause, according to the Indian National Family Health Survey (NFHS-3)3 carried out during 2005-2006, about 18 per cent of currently married women in the age group of 30-49 yr had reached menopause; a very similar finding of 17.7 per cent was reported in an earlier survey round (NFHS-2, 1998-99)4.
Concern has been expressed that rates of premature menopause (before age 40 yr1) are high in India and may be increasing in certain sections of the population5. For example, NFHS-24 showed that 3.1 per cent of women in the age group of 30-34 yr and 8.0 per cent among 35-39 yr age groups were in menopause. It further showed that 22.1 per cent of the women in the age group of 35-39 yr in Andhra Pradesh were in menopause, a potentially significant observation as this State has a high prevalence of female sterilization at a young age5. However, these data included both natural menopause and hysterectomy (surgical removal of the uterus) in the numerator so are likely to be an overestimate of natural menopause, as the number of hysterectomies in some settings in India is relatively high, for example, 9.8 per cent of rural women participating in a health insurance scheme6. Hysterectomy may be less prevalent at national level; however, a population-based survey in India reported that about two per cent of the women in the age group of 15-49 yr had undergone hysterectomy (12,888 from a sample of 643,934 women)7.
Age at menopause is associated with a number of factors such as, smoking8,9, educational attainment10, marital status, employment status11, family history12, parity2,13, diet13, age at menarche14, abortion15 and body mass index11. However, there is no consistent association between the above factors and the onset of menopause. Previous research using NFHS-2 data showed significant influences of educational attainment, standard of living, number of children, age at first and last birth, use of contraception, body mass index and anaemia5. However, as the sample included women who had undergone hysterectomy, the findings could not be attributed to natural menopause.
In the Indian context, decline in fertility and early adoption of sterilization are the two distinct features influencing women's reproductive span. According to the NFHS-3, about 37 per cent of currently married women were sterilized, and the median age at sterilization was very young at 25 yr. Further, sterilization method accounted for about 66 per cent of contraceptive use in India in 2005-20063. Higher uptake of female sterilization at younger ages is reflected in declining total fertility rates from 3.4 in 1992-199316 to 2.7 in 2005-20063. Thus, the potential influence of these widespread reproductive behavioural changes on age at menopause is of interest.
The proportion and absolute number of Indian women at age 45 yr and above is likely to increase substantially in the next few decades. According to the 2011 census of India, there were about 96 million women aged 45 yr and above and this number is expected to increase to 401 million in 202617. As the life expectancy at age 45 is 30 yr, women in India, on average, could spend approximately 30 yr in post-menopausal stage of life. As the post-menopausal years are associated with health risks such as hypertension, heart disease, osteoporosis and decline in the overall quality of life18,19, this group will present profound future challenges to public healthcare provision.
The objectives of this study were first to estimate the prevalence of natural menopause in India and its major States and second, to examine factors associated with natural menopause in India and selected States.
Material & Methods
The District Level Household Survey (DLHS) third round7 data were used for this study primarily because it allowed separation of natural menopausal women from women who had undergone hysterectomy. This survey covered 611 districts from 34 States and union territories of India. The DLHS-3 was designed to provide information on family planning, maternal and child health, the reproductive health of ever-married women (age 15-49 yr) and unmarried women (age 15-24 yr), as well as the utilization of maternal and child healthcare services at the district level. In this survey, data were not collected from women aged 50 yr or more. The DLHS-3 used a multistage stratified systematic sampling design to select the Primary Sampling Units (PSU) and the required number of households for interviews. In each district, 50 PSUs (census villages in rural areas and wards in urban areas) were selected in the first stage by systematic Probability Proportional to Size sampling. The PSUs were allocated to rural and urban areas of each district proportionally to the actual rural–urban population ratio. In rural areas, households were systematically drawn from the selected PSUs after house listing at the second stage, whereas in urban areas, the second stage of sampling included the selection of Census Enumeration Blocks followed by selection of households in the third stage of sampling. The survey covered 720,320 households and interviewed 643,944 ever-married women7.
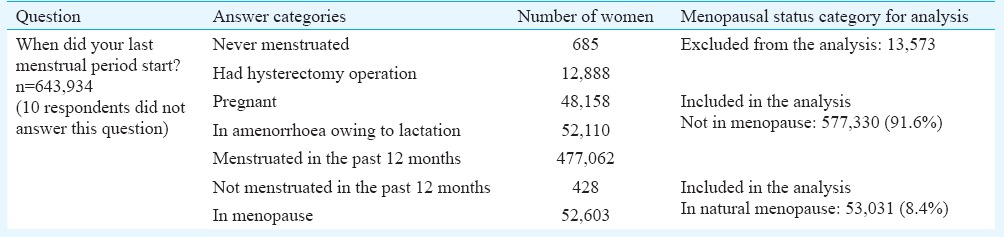
Identifying ‘naturally menopausal’ women: As part of the ever-married women's questionnaire, all respondents in the age group of 15-49 yr were asked ‘When did your last menstrual period start?’. Table I provides responses and frequencies for this question. Those who answered ‘never menstruated’ or ‘had hysterectomy operation’ (n = 13,573) were excluded from the analysis. In the data set, it was not possible to identify whether hysterectomy was done before or after menopause. Those who reported that they were pregnant, in post-partum amenorrhoea or had been menstruating in the past 12 months (n = 577,330) were considered as ‘not in menopause’. Finally, those who reported that they were in menopause and those who had not menstruated in the past 12 months were considered as ‘in natural menopause’. This group contained 53,031 women. Thus, 630,361 (577,330 + 53,031) women were included in the national-level analysis. For the selected States, these numbers were: 86,426 (Uttar Pradesh), 27,667 (Odisha), 33,947 (Maharashtra), 26,857 (Karnataka) and 12,048 (Kerala). These States were selected to obtain insights about factors associated with natural menopause in regions that these States represent, in addition to representing States with highest and lowest prevalence of natural menopause. As it was not possible to establish age at natural menopause, our analysis was based on the current age of women reporting menopause. If a woman aged 45 yr reported in the survey that she was ‘in menopause’, 45 was taken as her age at menopause although theoretically she could experience menopause any time before that age. However, since the objective of the study was not to establish accurate age at menopause but to examine its prevalence among women below 50 yr age, there was no bias in the results. This is, however, a limitation of the data as it prevents complete presentation of age at menopause and associated factors.
Table I.
Steps involved in identifying natural menopausal women from the survey question
Selection of explanatory variables: The selection of explanatory variables for this analysis was based on known associations with age at menopause from the literature, considered in the light of variables available in the DLHS-3. The explanatory variables included in the analysis were broadly grouped as socio-economic variables: educational attainment of women, wealth index quintiles (based on the ownership of household assets), religion (Hindu, Muslim, Others), caste (scheduled castes - the social group belongs to the lower strata of the traditional caste system), scheduled tribes (indigenous population), type of locality (rural/urban) and region of residence (North, Central, East, North-East, West, South - to account for the regional variations). Family planning variables were use of contraceptive pills, adoption of female sterilization and abortion. Demographic variables included marital status and parity.
Statistical analysis: Descriptive statistics were used to generate the proportion of women in natural menopause for major States and categories of explanatory variables. Cox proportional hazard regression models were used to obtain estimates of the hazard ratio (HR) for the explanatory variables that are likely to affect menopausal status. In the survival analysis, median age (median survival time) was the time beyond which 50 per cent of the women were expected to remain not in menopause. A survival method was preferred over other models such as logit analysis since it takes into account the duration to the event of interest, the age at menopause and adequately deals with censored observations which are a feature of this data set. The censored data were from women who were still premenopausal by the time of the interview as menopause is equated to an event that is yet to occur for many women in the study population. To reduce bias in the estimates of HRs, the assumption of proportional hazards was checked both by inspection of plots of the Schoenfeld residuals and by the use of time-dependent covariates. To accommodate tied observations (several women attaining menopause at the same age), adjustments were made in calculating the Cox partial likelihood using Efron method20. Bivariate models provided the unadjusted HRs and 95 per cent confidence intervals (CIs) for the association between each variable and menopausal status. The associations were re-examined in multivariable survival models after adjusting for all the other variables. Since we did not have any prior knowledge of specific interactions, all covariates were evaluated for potential interaction effect by using first-order interaction terms between the covariates. A significant (P<0.05) change in the maximum likelihood with Chi-square value following removal of the interaction term from the model indicated statistical interaction. All the analyses were performed using Stata version 1121.
Results
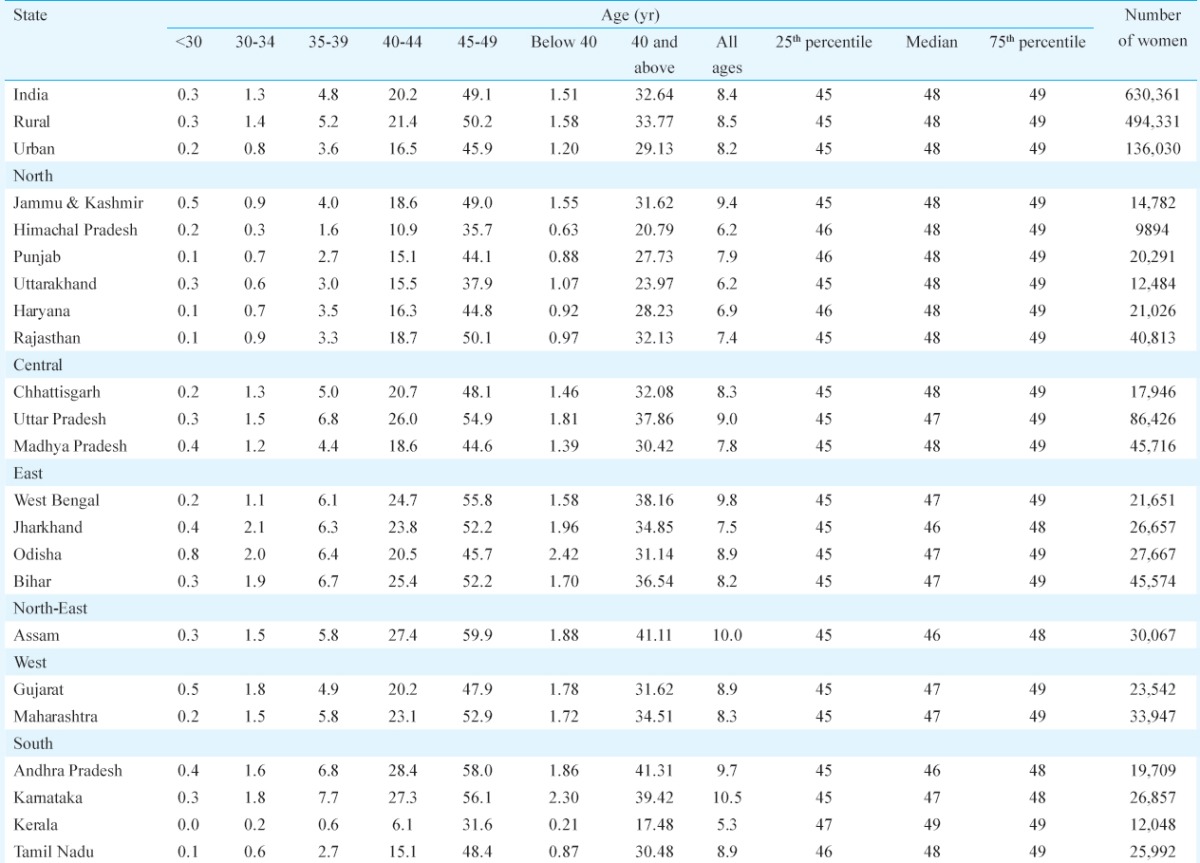
Table II provides the proportion of women in natural menopause according to various age groups and major States. Overall, about 8.4 per cent of women in the age group of 15-49 yr were in natural menopause – the highest proportion being in Karnataka (10.5%) and lowest in Kerala (5.3%). Below age 30 yr, 0.3 per cent of the women were in natural menopause compared to 1.3 per cent in the age group of 30-34 yr; 4.8 per cent in the age group of 35-39 yr; 20.2 per cent in the age group of 40-44 yr and 49.1 per cent in the age group of 45-49 yr. Overall, the percentage of women with natural premature menopause (below 40 yr) was about 1.5 per cent with the lowest rate in Kerala (0.2%) and highest in Odisha (2.4%).
Table II.
Proportion (in %) of women in natural menopause and median age of women reporting natural menopause according to major States, India, 2007-2008
Descriptive statistics: Table III provides an analysis of the number of women and percentage of women in natural menopause according to categories of explanatory variables.
Table III.
Number and proportion of women reporting natural menopause according to explanatory variables, India, 2007-2008
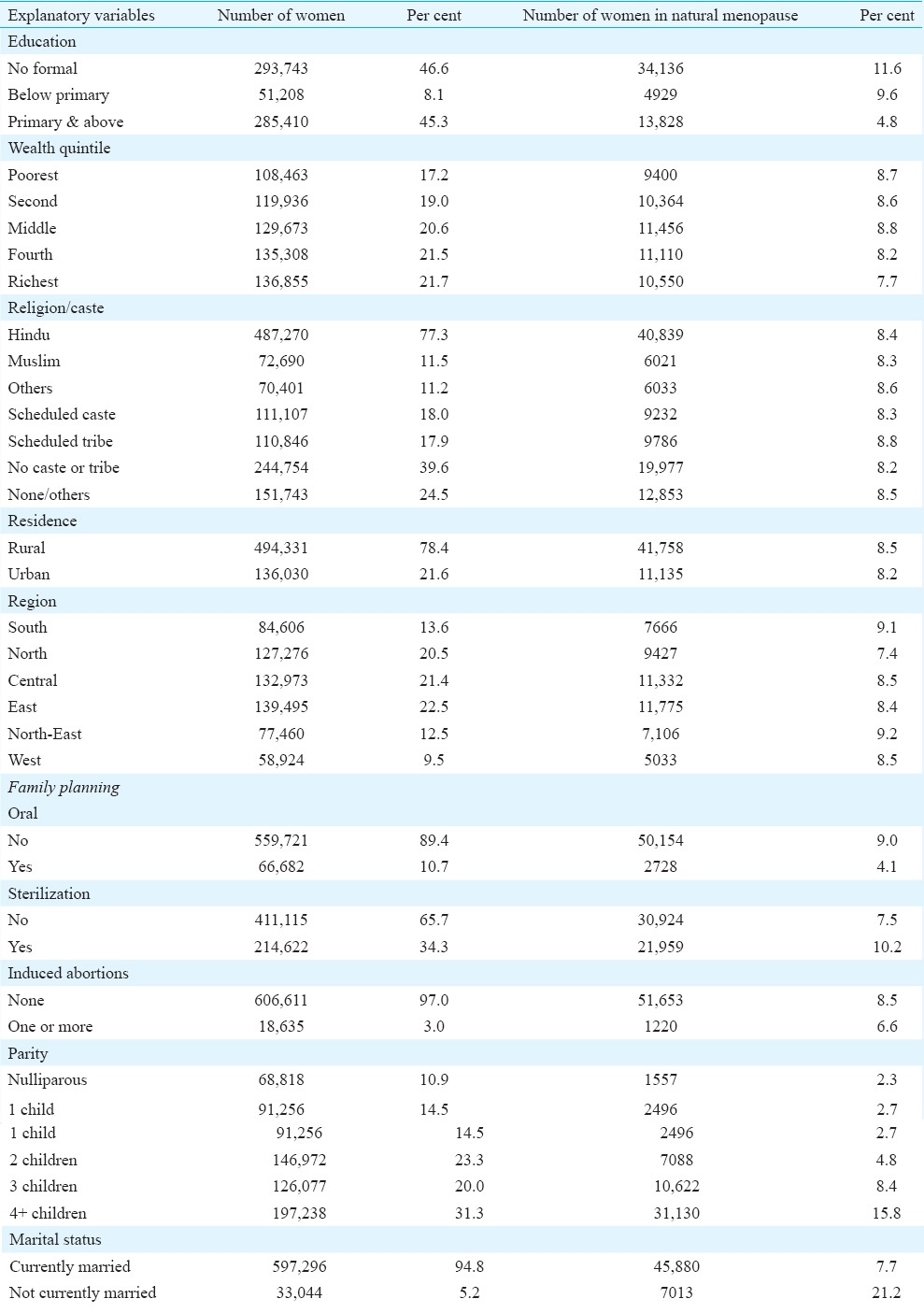
Socio-economic factors: Among women with no formal education, 11.6 per cent were in natural menopause compared to 4.8 per cent among those with ‘primary and above’ education. The proportion of women reporting natural menopause was highest among the poorest (8.7%) compared to the richest (7.7%) income quintile. There was little variation among the religious (8.3 vs 8.6%) and caste (8.2 vs 8.8%) groups. A slightly higher proportion of women in the rural areas were in natural menopause (8.5%) compared to their urban counterparts (8.2%). There were regional differences with the North 7.4 per cent and North-East 9.2 per cent.
Family planning use: The proportion of women in natural menopause among women who have never used contraceptive pills was substantially higher (9.0%) as compared to those who have ever used pills (4.1%). Among women who had been sterilized, the proportion of women in natural menopause was 10.2 per cent compared to 7.5 per cent among those who were not sterilized. Further, those who had reported at least one abortion, 8.5 per cent were in natural menopause compared to 6.6 per cent among those who did not report any abortion.
Demographic factors: Among currently married women, 7.7 per cent were in natural menopause compared to 21.2 per cent in the divorced/widowed/separated group. The proportion of women in natural menopause among women having more than four children was higher (15.8%) compared to women having no children (2.3%).
Results from survival model: Table IV provides both unadjusted and adjusted HRs along with 95 per cent CI and significance levels for all-India data. All factors included in the analysis were significantly associated with natural menopause in both unadjusted and multivariate models. The following section describes the adjusted estimates.
Table IV.
Unadjusted and adjusted hazard ratios for association of covariates with age of women reporting natural menopause, India, 2007-2008
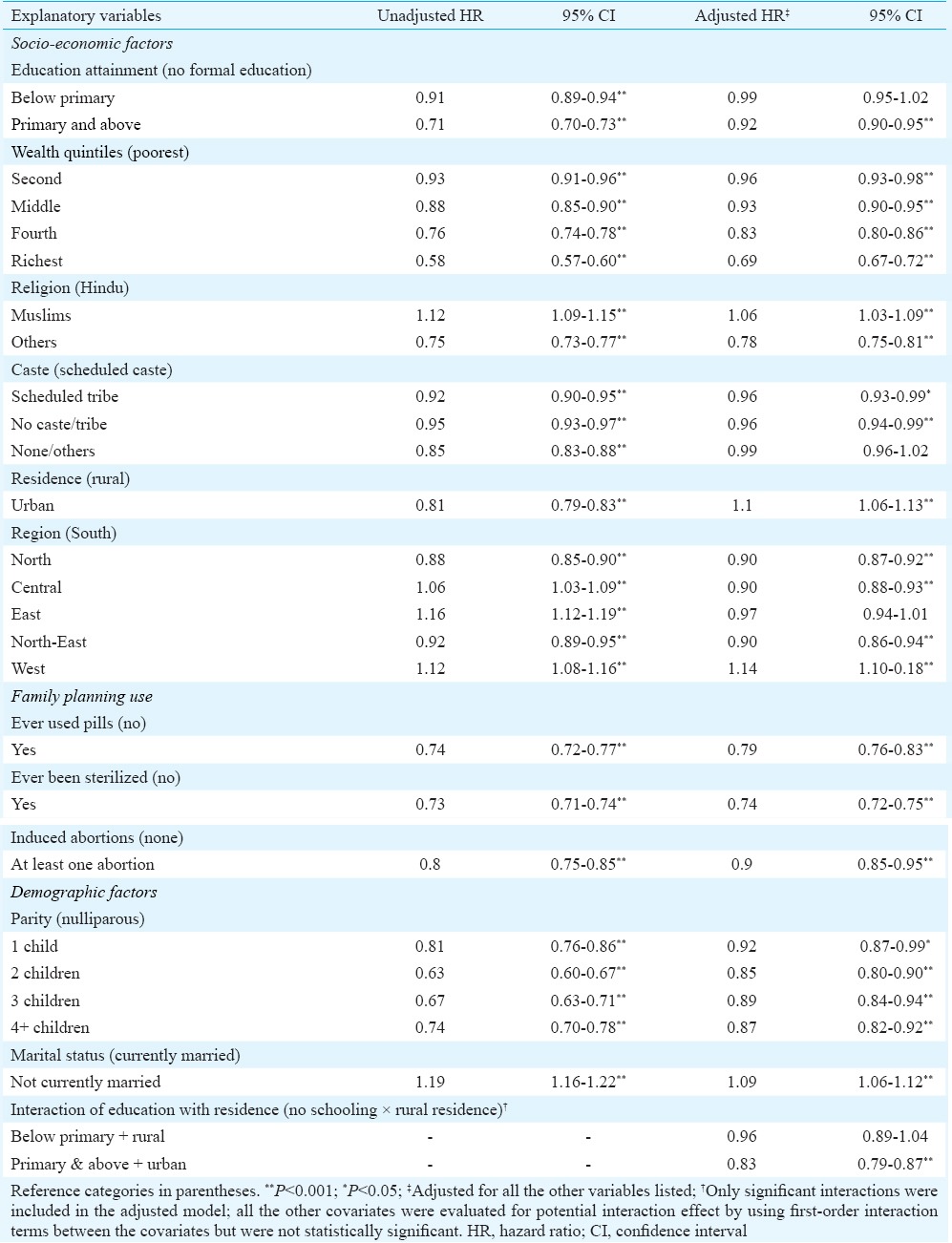
Socio-economic factors: Women who lived in urban areas with above primary level education had lower risk of natural menopause (HR = 0.83, 95% CI: 0.79-0.87) compared to women who lived in rural areas and had no schooling. There is a clear association between economic status and the risk of natural menopause: the richest women had a significantly (P<0.001) lower risk of natural menopause (HR = 0.69, 95% CI: 0.67-0.72) compared to the poorest. Compared to Hindus, Muslims had higher risk of menopause (HR = 1.06, 95% CI: 1.03-1.09); and ‘other’ religious groups had lower risk of natural menopause (HR = 0.78, 95% CI: 0.75-0.81). Scheduled tribes had lower risk of natural menopause (HR = 0.96, 95% CI: 0.93-0.99) compared to scheduled castes. Relative to the South, women from the North (HR = 0.90, 95% CI: 0.87-0.92), Central (HR = 0.90, 95% CI: 0.88-0.93) and North-East (HR = 0.90, 95% CI: 0.86-0.94) had lower risk while those from West (HR = 1.14, 95% CI: 1.10-1.10) had a higher risk of natural menopause.
Family planning use: In contrast to the initial analysis, sterilized women had a lower risk of natural menopause (HR = 0.74, 95% CI: 0.72-0.75) compared to non-sterilized women following adjustment for other variables. Women who had ever used the oral contraceptive pill also had a lower risk of natural menopause (HR = 0.79, 95% CI: 0.76-0.83) compared to women who had never done so. Experience of at least one abortion resulted in a lower risk of natural menopause (HR = 0.90, 95% CI: 0.85-0.95) compared to women who did not report any abortion.
Demographic factors: Women who had four or more children had lower risk of natural menopause (HR = 0.87, 95% CI: 0.82-0.92) compared to women who did not have any children. Divorced, separated and widowed women had a higher risk of natural menopause (HR = 1.09, 95% CI: 1.06-1.12) compared to currently married women.
Results from the survival model for selected States: Table V presents estimated HRs and 95 per cent CIs for the factors associated with natural menopause in the selected States.
Table V.
Adjusted hazard ratios for association of covariates with age of women reporting natural menopause, selected States, India, 2007-2008
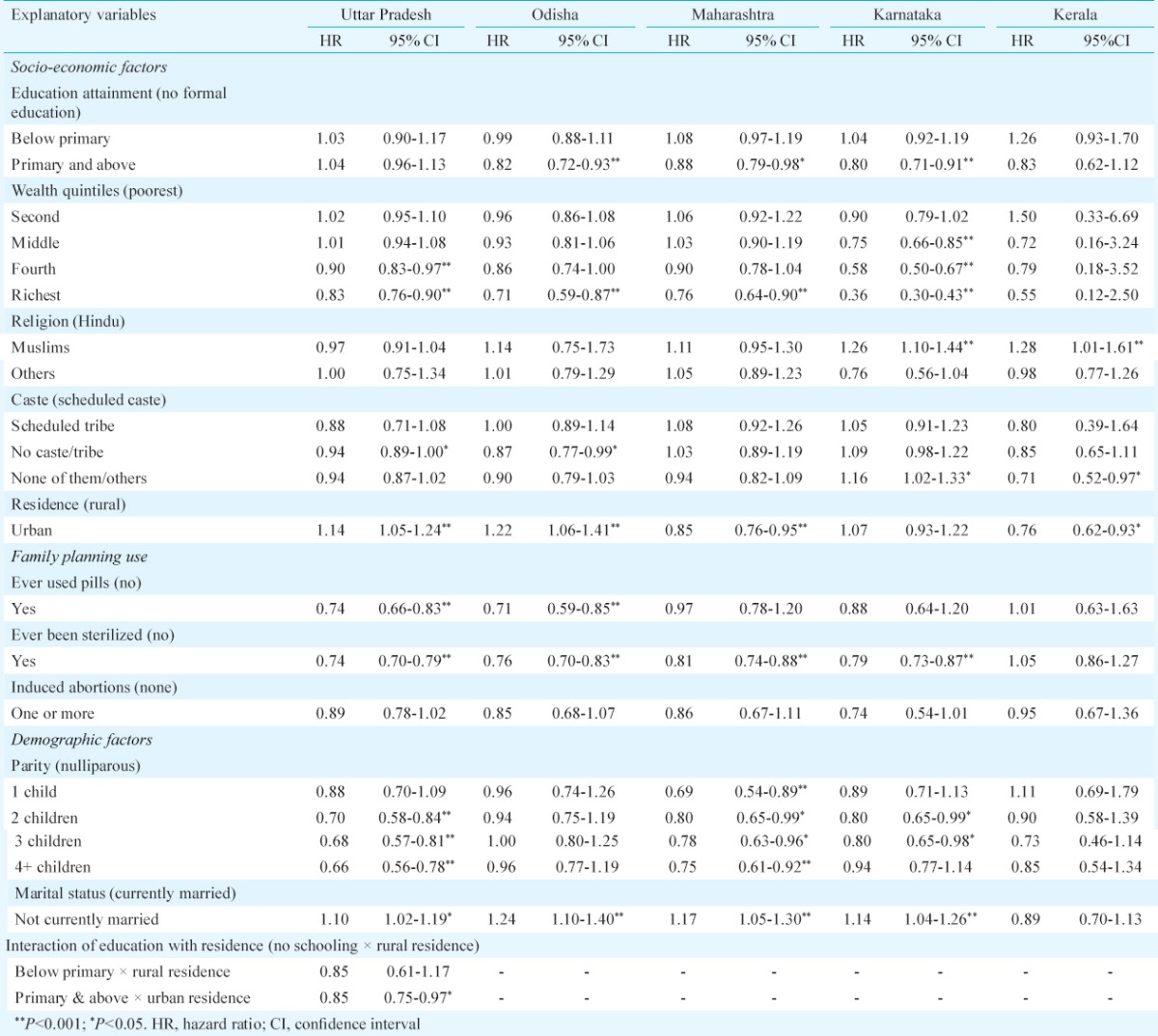
Socio-economic factors: Women with primary schooling and above had lower risk of natural menopause compared to women with no education in Odisha (HR = 0.82, 95% CI: 0.72-0.93), Maharashtra (HR = 0.88, 95% CI: 0.79-0.98) and Karnataka (HR = 0.80, 95% CI: 0.71-0.91), but not in Kerala. In Uttar Pradesh, women with schooling above primary level and living in urban areas had a lower risk of natural menopause compared to rural women with no formal schooling (HR = 0.85, 95% CI: 0.75-0.97). The richest women had a lower risk of natural menopause in Uttar Pradesh (HR = 0.83, 95% CI: 0.76-0.90), Odisha (HR = 0.71, 95% CI: 0.59-0.87), Maharashtra (HR = 0.76, 95% CI: 0.64-0.90) and Karnataka (HR = 0.36, 95% CI: 0.30-0.43), but not in Kerala. Muslims in Kerala (HR = 1.28; 95% CI: 1.01-1.61) and Karnataka (HR = 1.26, 95% CI: 1.01-1.61) had a higher risk of menopause compared to Hindus. Caste affiliation was a significant variable in the models for all States except Maharashtra. In Uttar Pradesh (HR = 0.94, 95% CI: 0.89-1.00) and Odisha (HR = 0.87, 95% CI: 0.77-0.99), women from ‘no tribe/no caste’ had a lower risk of menopause compared to those categorized as from a scheduled caste. In Karnataka, women from ‘none of them/other’ group had a greater risk of natural menopause compared to those categorized as from a scheduled caste (HR = 1.16, 95% CI: 1.02-1.33). In Kerala, the ‘none of them/other’ group had a lower risk of natural menopause compared to women categorized as from a scheduled caste (HR = 0.71, 95% CI: 0.52-0.97). While urban women in Odisha (HR = 1.22, 95% CI: 1.06-1.41) had a higher risk of natural menopause, urban women in Maharashtra (HR = 0.85, 95% CI: 0.76-0.95) and Kerala (0.76, 95% CI = 0.62-0.93) had a lower risk of menopause compared to their rural counterparts. No difference was noted in Karnataka.
Family planning use: Women who have ever used the contraceptive pills had a lower risk of menopause compared to those who did not use pills in Uttar Pradesh (HR = 0.74, 95% CI: 0.66-0.83) and Odisha (HR = 0.71, 95% CI: 0.59-0.85), but not in Kerala, Karnataka and Maharashtra. Except in Kerala, sterilized women had a lower risk of menopause compared to non-sterilized women (Uttar Pradesh: HR = 0.74, 95% CI: 0.70-0.79; Odisha: HR = 0.76, 95% CI: 0.70-0.83; Maharashtra: HR = 0.81, 95% CI: 0.74-0.88 and Karnataka: HR = 0.79, 95% CI: 0.73-0.87). In these State-level analyses, a history of abortion was not associated with natural menopause.
Demographic factors: Parity was negatively associated with menopause in Uttar Pradesh, Maharashtra and Karnataka, but not in Odisha and Kerala. Women having four or more children had a lower risk of natural menopause compared to women with no children in Uttar Pradesh (HR = 0.66, 95% CI: 0.56-0.78) and Maharashtra (HR = 0.75, 95% CI: 0.61-0.92) but not in Karnataka. In Karnataka, women who had three children had a lower risk of natural menopause compared to women who had no children (HR = 0.80, 95% CI: 0.65-0.98). Divorced/widowed/separated women in all States, except Kerala (Uttar Pradesh: HR = 1.10; 95% CI: 1.02-1.19; Odisha: HR = 1.24, 95% CI: 1.10-1.40; Maharashtra: HR = 1.17, 95% CI: 1.05-1.30 and Karnataka: HR = 1.14, 95% CI: 1.04-1.26) had higher risks of natural menopause compared to currently married women.
Discussion
In this study, an analysis of natural menopause and associated factors was done using nationally representative large-scale population-based survey data. Previous population-based research on menopause included women who had undergone both natural menopause and hysterectomy5. Our study avoided the possible overestimation of rates of early and premature natural menopause and underestimation of the true age at menopause that could have confounded previous studies; this is especially important given the large number of hysterectomies undertaken in India6,7.
It was observed that about 1.5 per cent of women below the age of 40 yr were in menopause; consistent with the 1-2 per cent range reported internationally22. We found no evidence of any increase in natural premature menopause as reported in a previous study5. Our findings were also consistent with the age at menopause reported in another study from India2. Important interstate variations in the median age of women reporting natural menopause were noted. The reason for these variations is not clear but may reflect the different nutritional and socio-economic conditions prevailing in different parts of the country.
Overall, socio-economic, family planning and demographic variables included in the study were significantly associated with natural menopause. Wealth index was the most important factor associated with lower risk of natural menopause and together with previous research carried out in India and elsewhere suggests a possible poverty-nutrition link10,13. As early menopause is linked with osteoporosis and other health risks, it is important that poor women are assured access to appropriate nutrition and health interventions19. Further work is needed to understand associations between general undernutrition arising from poverty and specific micronutrient deficiencies that might affect ovarian reserve such as vitamin D23. In our study, marital breakdown or widowhood was associated with a higher risk of natural menopause compared to currently married women. This finding was consistent with other studies; causality might lie in relative socio-economic deprivation among this group11. A lower risk of menopause for parous women might have been expected, reflecting the biological association between fertility and ovarian reserve. One study24 carried out in India did not show this association while another was consistent with our findings2. These discrepancies might have resulted from incomplete consideration of confounding variables.
An interesting finding in this study was the negative association of natural menopause with prior surgical sterilization. This contrasts with a hospital-based report from India24 and is of public health importance noting that female sterilization is the predominant family planning method in India. More research is needed to refute a possible link, but based on our analysis any substantial effect would seem to be unlikely. Another important finding was the association of lower risk of natural menopause among women who had ever used contraceptive pills. This finding was consistent with some studies25,26 but in contrast with findings from a study that used duration of pill use27. Taken together, these data did not indicate any substantial effect on ovarian reserve arising from pill use. Women who reported at least one abortion tended to have a reduced risk of natural menopause. This was in contrast with another study15. An underlying mechanism may be preservation of ovarian reserve through ovarian suppression with oral contraception; further substantiation of this would require survey methods incorporating a suitable biomarker of ovarian reserve such as anti-Müllerian hormone28.
As both the absolute number and the proportion of post-menopausal women are increasing in India, it is important to re-frame public reproductive healthcare services to include appropriate services for them. An obvious limitation of the present study was that it used data from women aged 15-49 yr. To overcome this limitation, survival models were used in our analysis which were best suited for ‘time to event data’ and for data having censored cases. Owing to data limitations, it was not possible to estimate age at menopause. Instead, the current menopause status of the women and current age were used in the analysis. Another limitations of the study included not knowing the smoking status of women. Smoking is a strong known predictor for early menopause; women who smoke are likely to undergo natural menopause one year earlier than those who do not28. While cigarette smoking remains less prevalent among Indian women than in some other countries, it is not possible to exclude the effect of this or other forms of tobacco consumption such as ‘bidi’ and chewing tobacco. Future surveys should endeavour to capture the range of ‘modern’ and traditional drugs consumed by women including the different forms of tobacco.
Acknowledgment
This study was supported by the British Council Newton Institutional Link Award (ID: 172600309).
Footnotes
Conflicts of Interest: None.
References
- 1.Research on the menopause in the 1990s. Geneva: WHO; 1996. World Health Organization. [Google Scholar]
- 2.Kriplani A, Banerjee K. An overview of age of onset of menopause in Northern India. Maturitas. 2005;52:199–204. doi: 10.1016/j.maturitas.2005.02.001. [DOI] [PubMed] [Google Scholar]
- 3.National Family Health Survey (NFHS-3), 2005-2006: India. I. Mumbai: IIPS; 2007. International Institute for Population Sciences (IIPS) and Macro International. [Google Scholar]
- 4.National Family Health Survey (NFHS-2), 1998-1999: India. Mumbai: IIPS; 2000. International Institute for Population Sciences (IIPS) and ORC Macro. [Google Scholar]
- 5.Syamala T, Sivakami M. Menopause: an emerging issue in India. Econ Polit Wkly. 2005;40:19–25. [Google Scholar]
- 6.Desai S, Sinha T, Mahal A. Prevalence of hysterectomy among rural and urban women with and without insurance in Gujarat, India. Reprod Health Matters. 2011;19:42–51. doi: 10.1016/S0968-8080(11)37553-2. [DOI] [PubMed] [Google Scholar]
- 7.District Level Household Survey 2007-2008. Mumbai: IIPS; 2010. International Institute for Population Sciences (IIPS) [Google Scholar]
- 8.Remez L. Multiple factors, including genetic and environmental components, influence when menopause begins. Fam Plan Perspect. 2001;33:236. [Google Scholar]
- 9.Hardy R, Kuh D, Wadsworth M. Smoking, body mass index, socioeconomic status and the menopausal transition in a British national cohort. Int J Epidemiol. 2000;29:845–51. doi: 10.1093/ije/29.5.845. [DOI] [PubMed] [Google Scholar]
- 10.Sievert ML. Menopause: a biocultural perspective. New Brunswick: Rutgers University Press; 2006. [Google Scholar]
- 11.Gold EB, Bromberger J, Crawford S, Samuels S, Greendale GA, Harlow SD, et al. Factors associated with age at natural menopause in a multiethnic sample of midlife women. Am J Epidemiol. 2001;153:865–74. doi: 10.1093/aje/153.9.865. [DOI] [PubMed] [Google Scholar]
- 12.Murabito JM, Yang Q, Fox C, Wilson PW, Cupples LA. Heritability of age at natural menopause in the Framingham Heart Study. J Clin Endocrinol Metab. 2005;90:3427–30. doi: 10.1210/jc.2005-0181. [DOI] [PubMed] [Google Scholar]
- 13.Hidayet NM, Sharaf SA, Aref SR, Tawfik TA, Moubarak II. Correlates of age at natural menopause: a community-based study in Alexandria. East Mediterr Health J. 1999;5:307–19. [PubMed] [Google Scholar]
- 14.Harlow BL, Signorello LB. Factors associated with early menopause. Maturitas. 2000;35:3–9. doi: 10.1016/s0378-5122(00)00092-x. [DOI] [PubMed] [Google Scholar]
- 15.Shelling AN. Premature ovarian failure. Reproduction. 2010;140:633–41. doi: 10.1530/REP-09-0567. [DOI] [PubMed] [Google Scholar]
- 16.National Family Health Survey (MCH and family planning), India 1992-1993. Bombay: IIPS; 1995. International Institute for Population Sciences (IIPS) [Google Scholar]
- 17.Population Projections for India and States 2001-2026. New Delhi: Government of India; 2006. Office of the Registrar General and Census Commissioner. [Google Scholar]
- 18.Aaron R, Muliyil J, Abraham S. Medico-social dimensions of menopause: a cross-sectional study from rural South India. Natl Med J India. 2002;15:14–7. [PubMed] [Google Scholar]
- 19.Nagata C, Takatsuka N, Inaba S, Kawakami N, Shimizu H. Association of diet and other lifestyle with onset of menopause in Japanese women. Maturitas. 1998;29:105–13. doi: 10.1016/s0378-5122(98)00012-7. [DOI] [PubMed] [Google Scholar]
- 20.Efron B. The efficiency of Cox's likelihood function for censored data. J Am Stat Assoc. 1977;72:557–65. [Google Scholar]
- 21.Stata statistical software: release 11. College Station, TX: Stata Corp LP; 2009. StataCorp. [Google Scholar]
- 22.Shuster LT, Rhodes DJ, Gostout BS, Grossardt BR, Rocca WA. Premature menopause or early menopause: long-term health consequences. Maturitas. 2010;65:161–6. doi: 10.1016/j.maturitas.2009.08.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Merhi ZO, Seifer DB, Weedon J, Adeyemi O, Holman S, Anastos K, et al. Circulating Vitamin D correlates with serum antimüllerian hormone levels in late-reproductive-aged women: women's interagency HIV study. Fertil Steril. 2012;98:228–34. doi: 10.1016/j.fertnstert.2012.03.029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bhardwaj J, Kendurkar S, Vaidya P. The age at menopause in the women of Himachal Pradesh and factors affecting the menopause. Indian J Public Health. 1987;31:40–4. [PubMed] [Google Scholar]
- 25.van Noord PA, Dubas JS, Dorland M, Boersma H, te Velde ER. Age at natural menopause in a population-based screening cohort: the role of menarche, fecundity, and lifestyle factors. Fertil Steril. 1997;68:95–102. doi: 10.1016/s0015-0282(97)81482-3. [DOI] [PubMed] [Google Scholar]
- 26.OlaOlorun F, Lawoyin T. Age at menopause and factors associated with attainment of menopause in an urban community in Ibadan, Nigeria. Climacteric. 2009;12:352–63. doi: 10.1080/13697130802521282. [DOI] [PubMed] [Google Scholar]
- 27.de Vries E, den Tonkelaar I, van Noord PA, van der Schouw YT, te Velde ER, Peeters PH. Oral contraceptive use in relation to age at menopause in the DOM cohort. Hum Reprod. 2001;16:1657–62. doi: 10.1093/humrep/16.8.1657. [DOI] [PubMed] [Google Scholar]
- 28.Bromberger JT, Matthews KA, Kuller LH, Wing RR, Meilahn EN, Plantinga P. Prospective study of the determinants of age at menopause. Am J Epidemiol. 1997;145:124–33. doi: 10.1093/oxfordjournals.aje.a009083. [DOI] [PubMed] [Google Scholar]