

Abstract
BACKGROUND:
The abnormal conditions of life and genetic factors often play a major role in the incidence of “diabetes - diabetes”, heart disease and vascular disease, jaundice and posttraumatic stress.
AIM:
Trauma and posttraumatic stress are most common in the displaced persons, and the focus of this paper is to focus on this issue regarding cases in former Yugoslavia, and now in our country. These diseases are caused by increased beta-cell sensitivity to viruses, the development of autoimmune antibodies attacking their pancreas cells, degenerative changes in cells that result in the change of structure and of insulin production.
MATERIALS AND METHODS:
In this paper, we have taken into account the traumatic events and long-term psychosocial consequences for internally displaced persons, several years after displacement, and found a high level of PTSD symptoms.
RESULTS:
This stress is present in almost 1/3 of internally displaced persons, and every sixth person has suffered from PTSD in the past. Respondents suffer from symptoms of intrusion, but there was a large number of symptoms, such as avoidance and increased arousal. We also found that gender, age and education are related to the symptoms.
CONCLUSION:
Females, and older respondents and internally displaced persons with lower levels of education show a higher level of PTSD symptoms.
Keywords: living environment, displaced persons, jaundice, diabetes, trauma, diabetic hypertension, post-traumatic stress (PTSD)
Introduction
Diabetes mellitus or diabetes (diabetes mellitus, διαβήτης) is a chronic, incurable systemic disorder of metabolism, which manifests itself as hyperglycemia and permanently elevated level of blood glucose. It is mainly caused by hereditary factors, and it is usually the result of reduced secretion or reduced biological effects of the hormone insulin, but it could also be the result of the combination of these two factors. This deficiency impedes the exchange of carbohydrates, fats and proteins in the body (which is the common symptom of the issue), and after a longer period, it influences the structure and function of blood vessels, nerves, and other vital organs [1-5].
Jaundice denotes yellowish tissue disease, which manifests itself as a yellowing of the skin and deep tissues. The most common cause of hepatitis is a large amount of free or conjugated bilirubin in the extracellular fluids. The normal bilirubin concentration in plasma (free-form) is on average of 9 mmol/l. In the certain pathological conditions, the concentration of bilirubin can be increased to 700 mmol/l. In the case of obstructive jaundice, caused either by an obstruction of the bile ducts, or by damage to the liver cells, the creation of bilirubin is normal, but the bilirubin created cannot reach the intestine from the blood. Free bilirubin further enters liver cells wherein it conjugates in a usual manner and creates problems for the body.
Trauma and posttraumatic stress among IDPs are results of numerous wars in the previous Yugoslavia, Yugoslavia and after the secession of the former federate republics, and to this day there have been more than one million refugees in the area.
Diseases of the heart and blood vessels are also frequent complications following all forms of diabetes, and one of them is gangrene of the feet and so on. Hypertension is a major risk factor for chronic cardiovascular and cerebra-vascular diseases, which are particularly noticeable among internally displaced persons above all due to degraded living conditions [6, 7].
Diseases of Diabetic Hypertension
The word diabetes was first used by Demetrius of Apollonius around 200 BC. It is derived from the Greek word διαβανειν which mean “flow through”, corresponding to one of the main symptoms of the disease - constant fluid intake and excessive production of urine (urine).
In 1675, Thomas Willis added, to the name of the disease, the word Mellitus, which was derived from Latin and means “sweet” (this is connected to the sweet taste of urine of the affected individuals). Matthew Dobson proved in 1776 that the sweet taste comes from the presence of sugar in the blood and urine of the diabetics [8, 9].
Despite the fact that it was known about for a relatively long time, diabetes was first experimentally determined and described at the end of the nineteenth century. Discovery of the role and importance of pancreas in the development of diabetes has been attributed to the scientists Joseph von Mering and Oskar Minkowski. In 1889, they discovered that dogs with removed pancreas soon started manifesting all the signs and symptoms of diabetes, and they died shortly after that. In 1910, Sir Edward Albert Sharpey suggested that people with diabetes lack one of the substances produced by the pancreas, and he proposed to call it insulin. The name is derived from the Latin word insula, which means “island”, referring to the fact that insulin creates beta cells of the islets of Langerhans in the pancreas [10].
The endocrine role of the pancreas in the metabolism, as well as the actual discovery of insulin, were not defined until 1921 when Ser Frederick Grant Banting and Charles Best Herbert demonstrated that in dogs without the pancreas, diabetes can be prevented by administering the extract of the islets of Langerhans of healthy dogs. Banting, Best and colleagues (especially the chemist Kolip) were able to isolate insulin from the pancreas of cattle at the University of Toronto, and in 1922, its use was allowed in the treatment of diabetes. A year later, Banting and laboratory director MacLeod won the Nobel Prize for this discovery [11]. They were protected from a patent disclosure but allowed its use without compensation, which contributed to the rapid expansion of the application of insulin in the treatment of this disease worldwide [12].
The difference between type one diabetes and type two was first discovered and published by Sir Harold Percival Himsworth in January 1936 [13].
According to WHO (World Health Organization), etiological classification of diabetes includes [14]:
Type 1 diabetes - occurs when the pancreas produces too little insulin or cannot produce it any more. This disorder usually occurs suddenly in childhood or adolescence.
Type 2 diabetes - is the most common form of diabetes. In this disorder, the pancreas continues to secrete insulin, but the cells of the body become resistant to its effects. This type of diabetes affects people over the age of 40 and often affects obese people.
Gestational diabetes usually occurs after giving birth; however, women who are afflicted by it have a higher chance of developing type 2 diabetes later in life.
Experiment
Trauma and post-traumatic stress are vicious diseases among IDPs, and they are the result of numerous wars in the previous Yugoslavia, FRY as well as in the succeeding states. From 1991, until today in this area, there are over 1 million refugees, although not all of them responded to the last census. Revision of their refugee status is in progress, and it is expected that about 30% of them would lose that status due to the acquisition of citizenship, the appliance for a program of return to the former republics and now separate states or because they did not respond to the census. Experimental research will be in compliance with the Helsinki Declaration.
The bad economy and unstable political situation hamper the integration of refugees, which is the permanent solution chosen by 60% of the refugees. Inadequate housing and high unemployment are the two main problems of the refugees and displaced persons. The inability of finishing works on the residential units without help, the problem of legalization, poor infrastructure, the inability to obtain grants and loans (only about 20% of refugees have somehow solved their housing problems), the inability to be properly informed and lack of education in self-employment opportunities, failure in take part in the labor market also contribute to the issue of integration.
Risk factors for coronary disease
The term “risk factor” is often used to describe features found in healthy individuals and which have been determined by epidemiological studies to be associated with the subsequent occurrence of the disease, in this case of CHD.
In the elementary sense, the term risk factors include changeable and immutable characteristics of each. NIDDM is a significant risk factor for the development of cardio-vascular diseases (CVD) in both men and women. Data obtained from the studies indicate that the risk of cardiovascular disease is 2 to 4 times higher in NIDDM patients than in non-diabetics and that the annual rate of fatal and non-fatal cardiovascular disease occurrence in NIDDM patients is 2 to 5%.
To verify this data, and, to determine the presence and importance of risk factors for coronary heart disease in diabetics, we examined 60 insulin dependent diabetes patients treated at a health centre.
All patients had clinically proven non-insulin dependent diabetes, and according to the presence of coronary disease were divided into two groups: Group I-NIDDM patients with coronary disease; Group II-NIDDM patients without coronary disease. In addition to taking a detailed medical history, the following data were measured: body mass index (BMI) and waist/hip ratio (WHR), which were evaluated based on the criteria of European NIDDM Policy Group (1996) [15].
From biochemical parameters which are risk factors for CHD, acidum uricum and fibrinogen were determined. The level of risk assessment for coronary disease was performed according to the criteria of the European Association for atherosclerosis - EAS where the table was determined by a ten-year absolute risk assessment. Statistical analysis was performed using methods of descriptive and analytical statistics in Excel 7.0 and Windows 98 environment, and the results have been shown in the table and diagram.
The following was performed: the measurement of blood pressure; determination of fasting plasma glucose and daily glucose profile. From morning venous blood samples total cholesterol (HOL), HDL cholesterol, triglycerides (TG), and LDL cholesterol was determined.
Results
Out of a total number, 37 patients (62%) were female, and 23 (38%) were males. The average age of the patients was 57.98 ± 7.3 years, whereas there was no significant difference in age between men and women 58.8 ± 9.3 vs. 57.5 ± 7.23 years prospectively. Duration of diabetes was significantly higher in women than in men 9.2 ± 6.71 vs. 6.12 ± 7.13 years (p <0.05).
Although there were no significant differences in glycemic control, the value of daily mean blood glucose profiles (MBG), was much higher in treated patients 9.97 ± 3.29 mmol/l Waist/hip ratio (WHR) was significantly higher in male patients than 0.92 ± 0.04 vs. 0.87 ± 0.03 in females (p < 0.01), as the finding expected. The degree of obesity expressed in body mass index (BMI) showed significantly higher values in women than in men 29.75 ± 4.48 vs. 27.46 ± 2.74 kg/m2 (p < 0.01), while the average value of this parameter in the study group was 28.86 ± 3.95 kg/m2 above the WHO recommendation.
Coronary heart disease was significantly more prevalent in women than in men 21 (70 %) vs. 9 (30 %) (χ2 = 8.06, p < 0.01). The intensity of the connection between gender and the occurrence of CHD in diabetics was examined by test contingency. Test results unambiguously showed an extremely high degree of correlation between the appearance of CHD and females in diabetics (Cmax = 0.707, C = 0.61).
Basic characteristics of patients with CHD and without CHD are shown in Figure 1 the mean age of diabetic patients was 57.9 ± 7.3 years. There was no significant difference between the groups with KBS and without KBS. The diabetic length of service was 8 ± 7.1 years, and the duration of dyslipidemia 5.7 ± 4.72, whereas there was no significant difference between the groups. BMI values were significantly higher in patients with CHD compared to diabetics without CHD 29.77 ± 3.55 vs. kg/m2 27.97 ± 3.95 (p < 0.05).
Figure 1.
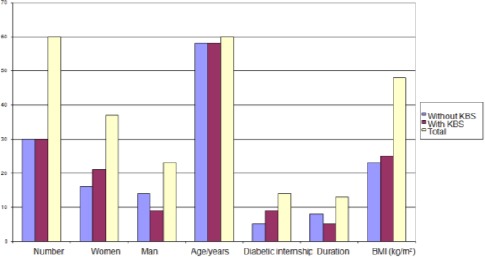
The characteristics of the studied patients
Elevated lipid risk levels (high-risk + border) for cholesterol (HOL) had 90% of patients with CHD and 76% without CHD, which proved to be statistically significant (χ2 = 6.12, p < 0.05). A significantly higher percentage of patients in the group with CHD had elevated lipid levels and risk for triglyceride (TG) 70% compared to patients without CHD, 56.5% (χ2 = 4.36, p < 0.05). Other parameters did not show significant differences in the distribution between the two groups. Representation of non-lipids risk factors for CHD is shown in Figure 4. It is evident that some non-lipid risk factors were present at high levels in the observed group of diabetes patients with CHD. Hypertension, as a risk factor was present in 60% of patients and a positive family history for the existence of a cardiovascular disease, was present in 63% of patients. Obesity is defined as BMI > 30 kg/m2 and was found in 40% of the patients. The possible existence of the improper distribution of non-lipids risk factors according to gender was investigated by Fisher’s exact test of probability. The test showed a significant difference in the occurrence of smoking regarding gender (0% women vs. 6% of men, p < 0.05) and in a positive family history (53% women vs. males 10%, p < 0.05).
Figure 2.
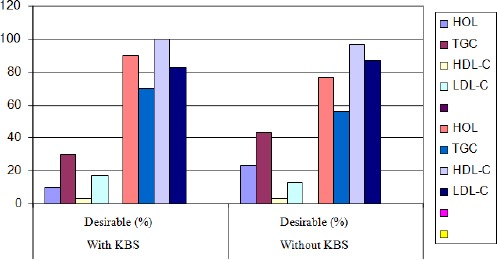
The prevalence of lipid disorders
Figure 3.
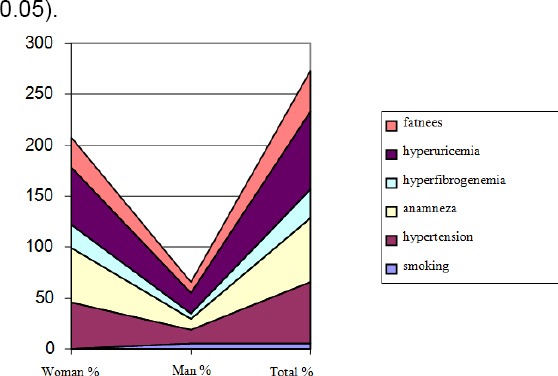
Representation of non-lipid risk factors in patients with CHD
Figure 4.
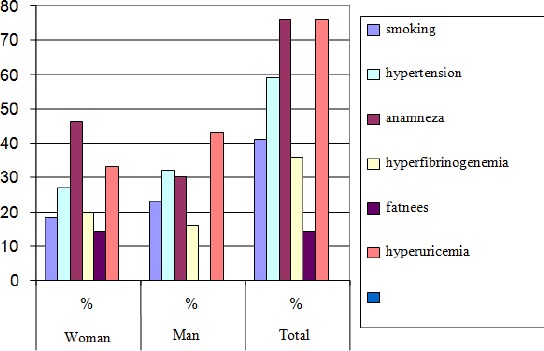
Representation of non-lipid risk factors in patients without CHD
It is evident, judging by the table, that some non-lipid risk factors were present at high levels in NIDDM diabetics without CHD. Hypertension as a risk factor is present (similar group, 60%) in 59% of patients. A family history of the cardiovascular disease was found in 76% of patients.
Obesity is defined as BMI > 30 kg/m2 and was found with a small percentage of patients: 13.6%, in contrast to the diabetes patients with CHD which was present with 40% of patients. Smoking unexpectedly exhibited a high level of incidence of 4% in one group of patients (current smokers and abstainers in less than two years).
Figure 5.
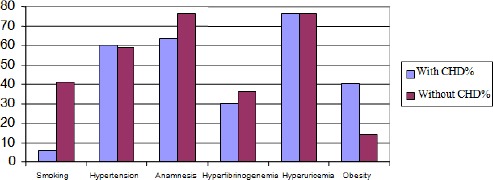
Non-lipid risk factors in diabetes patients with and without CHD
The possible existence of the improper distribution of non-lipids risk factors according to gender was investigated by Fisher’s exact probability test. The significantly higher occurrence of obesity in women has been demonstrated at the level of p = 0.05.
The existence of differences in the frequency of non-lipids risk factors in patients with CHD and diabetes patients without CHD was determined by Fisher’s exact probability test.
Table 1.
Non-Lipid Risk Factors in Patients with and without CHD
| Without CHD | With CHD | P | |
|---|---|---|---|
| WHR | 0.92 ± 0.04 | 0.90 ± 0.04 | NS |
| TA systolic (mmHg) | 156.72 ± 3.17 | 147.7 ± 22.7 | NS |
| TA diastolic (mmHg) | 96.81 ± 10.86 | 90.34 ± 14.2 | < 0.05 |
| Glycemia (mmol/l) | 7.37 ± 2.19 | 8.9 ± 2.67 | < 0.05 |
| MBG (mmol/l) | 9.34 ± 2.28 | 11.61 ± 2.7 | < 0.01 |
| Fibrinogen (g/l) | 3.66 ± 1.3 | 3.68 ± 1.4 | NS |
| Acidum urici (mmmol) | 292.08 ± 87.14 | 294 ± 102.74 | NS |
| Diabetic experience (year) | 6.4 ± 7.35 | 7.6 ± 5.84 | NS |
The percentage of smokers was much higher among the patients without CHD compared to diabetics with CHD (41% vs. 6%, p < 0.01). Obesity was relatively rare, however, with patients who did not have CHD compared to diabetes patients with CHD group (13.6% vs. 40%, p < 0.01).
The possible role of anthropometric and biochemical indicators of CHD with dyslipidemic diabetes patients was analysed statistically. Obesity expressed as the mean BMI was significantly higher in patients with CHD 29.67 + 3.31 about diabetes patients without coronary disease 3.17 ± 27.8 kg/m2. Abnormal glucose regulation was perceived as the fasting plasma glucose and daily mean glycemic profile. These disorders were more prevalent with patients with CHD; FBG 8.9 ± 2.67 vs. 7.37 ± 2.19 mmol/1 (p < 0.05) and MBG 11.61 ± 2.7 vs. 9.34 ± 2.82 mmol/l (p < 0.01). In contrast to more favourable profile values of all parameters in patients without CHD, diastolic blood pressure values were significantly higher in diabetes patients without CHD 96.81 ± 10.86 vs. 90.34 ± 14.2 mmHg than in patients with coronary artery disease.
Discussion
It is known, according to the data from the expert literature that over 60% of homeless diabetics (IDPs) had manifested dyslipidemia [8]. In this original work, elevated lipid levels of risk (high-risk + border) cholesterol (HOL) was investigated for this type of patients.
These health problems had 90% of the patients (with CHD and 76% without CHD), which proved to be statistically significant (χ2 = 6.12, p < 0.05). A higher percentage of patients in the group with CHD had elevated lipid levels and risk for triglycerides (TG) 70% compared to patients without CHD, 56.5% (χ2 = 4.36, p < 0.05). Other parameters did not show significant differences in the distribution between the two groups.
Coronary disease in a non-diabetic population is far more prevalent in men younger than 65, compared to women of the same age. However, in diabetes patients, this difference do not exist; furthermore, women with diabetes are far more vulnerable to early morbidity and mortality from CHD [10]. This was confirmed in this study, where women with diabetes were slightly younger (57.5 ± 23.7 vs. 58.8 ± 9.3) and with longer disease duration (9.2 ± 6.71. vs. 6.12 ± 7.13, p < 0.05) compared to men.
In the group of diabetes patients with dyslipidemia and coronary disease, some of the parameters of syndrome X were discovered in abundance. Hyperuricemia was found in 76% of patients, obesity in 40% and hypertension in 60% of cases. A positive family history was present in 63.3%, which supports the claims of the existence of the hereditary genetic defect in syndrome X.
Acknowledgements
Authors thank for support of the Institute of Biomedical Sciences, Faculty of Pharmacy and Health in Travnik, Bosnia and Herzegovina.
Footnotes
Funding: This research did not receive any financial support.
Competing Interests: The authors have declared that no competing interests exist.
Abbreviations: BMI = body mass index; CHD = coronary heart diseases; CVD = cardio-vascular diseases; FRY = Former Republic of Yugoslavia; MBG = mean blood glucose; PTSD = post-traumatic stress disease; WHR = waist/hip ratio.
References
- 1.Breslau N, Kessler RC, Chilcoat HD, Schultz LR, Davis GC, Andreski P. Trauma and posttraumatic stress disorder in the community: the 1996 Detroit Area Survey of Trauma. Arch Gen Psychiatry. 1998;55(7):626–32. doi: 10.1001/archpsyc.55.7.626. https://doi.org/10.1001/archpsyc.55.7.626. PMid: 9672053. [DOI] [PubMed] [Google Scholar]
- 2.Breslau N, Chilcoat HD, Kessler RC, Davis GC. Previous exposure to trauma and PTSD effects of subsequent trauma: results from the Detroit Area Survey of Trauma. Am J Psychiatry. 1999;156(6):902–7. doi: 10.1176/ajp.156.6.902. https://doi.org/10.1176/ajp.156.6.902. PMid: 10360130. [DOI] [PubMed] [Google Scholar]
- 3.Connor KM, Butterfield MI. Posttraumatic stress disorder. Focus. 2003;1(3):247–62. https://doi.org/10.1176/foc.1.3.247. [Google Scholar]
- 4.Duraković-Belko E, Powell S. Psychosocial effects of war - the results of empirical research from the territory of the former Yugoslavia. Sarajevo: UNICEF Bosnia and Herzegovina; 2002. [Google Scholar]
- 5.Karamatic S. Diabetes mellitus causes and risk factors, Medical Faculty of Tuzla, Bosnia and Herzegovina. 2009 [Google Scholar]
- 6.Savic D. Risk factors for lipid modification of their origin and in patients with coronary heart disease. Niš: Medical Faculty, Serbia; 1999. [Google Scholar]
- 7.Gu K, Cowie CC, Harris MI. Diabetes and decline in heart disease mortality in US adults. JAMA. 1999;281(14):1291–7. doi: 10.1001/jama.281.14.1291. https://doi.org/10.1001/jama.281.14.1291. PMid: 10208144. [DOI] [PubMed] [Google Scholar]
- 8.Djindjic B. Testing of dyslipidemia as risk factors for coronary heart disease in patients with insulin dependent diabetes. Niš: Faculty of Medicine, Serbia; 2000. [Google Scholar]
- 9.Dobson M. Experiments in an Heated Room. By Matthew Dobson, MD In a Letter to John Fothergill, MDFRS. Philosophical Transactions. 1775;65:463–9. https://doi.org/10.1098/rstl.1775.0046. [Google Scholar]
- 10.Maksimovic R. Clinical laboratory diagnosis. Pan-European university of Banja Luka, Bosnia and Herzegovina. 2010 [Google Scholar]
- 11. https://www.nobelprize.org/educational/medicine/insulin/discovery-insulin.html .
- 12.Cepelak I. Medical-biochemical guidance, Faculty of Medicine, Zagreb, Croatia. 2004 [Google Scholar]
- 13.Black D, Gray J. Sir Harold Percival Himsworth, K.C.B. - 19 May 1905--1 November 1993. Biogr Mem Fellows R Soc. 1995;41:199–218. https://doi.org/10.1098/rsbm.1995.0013. PMid: 11615356. [PubMed] [Google Scholar]
- 14. http://apps.who.int/iris/bitstream/10665/43588/1/9241594934_eng.pdf .
- 15.Biocanin R, Danelisen D, Amidzic B. The morbidity of the population as a result of the devastation of the environment. Banja Luka, Bosnia and Herzegovina. 2008 [Google Scholar]