

Abstract
Background
Maximum Step Length may be used to identify older adults at increased risk for falls. Since leg muscle weakness is a risk factor for falls, we tested the hypotheses that maximum knee and hip extension speed, strength, and power capacities would significantly correlate with Maximum Step Length and that the original “step out and back” Maximum Step Length would also correlate with the Maximum Step Length of its two sub-tasks: stepping “out only” and stepping “back only”. These sub-tasks will be referred to as versions of Maximum Step Length.
Methods
Unimpaired younger (N=11, age=24[3] years) and older (N=10, age=73[5] years) women performed the above three versions of Maximum Step Length. Knee and hip extension speed, strength, and power capacities were determined on a separate day and regressed on Maximum Step Length and age group. Version and practice effects were quantified and subjective impressions of test difficulty recorded. Hypotheses were tested using linear regressions, analysis of variance, and Fisher's exact test.
Findings
Maximum Step Length explained 6-22% additional variance in knee and hip extension speed, strength, and power capacities after controlling for age group. Within- and between-block and test-retest correlation values were high (>0.9) for all test versions.
Interpretation
Shorter Maximum Step Lengths are associated with reduced knee and hip extension speed, strength, and power capacities after controlling for age. A single out-and-back step of maximal length is a feasible, rapid screening measure that may provide insight into underlying functional impairment, regardless of age.
Keywords: step length, strength, moment, speed, power, dynamometer, falls
1. Introduction
Falls are a leading cause of accidental death and injury for those over the age of 65 years (CDC, 2000). Older women, especially those with balance impairments, are at a particularly high risk for fall-related injuries (Baker et al., 1992). The ability to recover from an imminent fall has been shown to be dependent on the ability to take an adequately rapid and long recovery step in the direction of the fall (Alexander, 1994; Luchies et al., 1994; Maki and McIlroy, 1999; Thelen et al., 1997).
In one measure of volitional stepping ability, Medell and colleagues (Medell and Alexander, 2000) instructed subjects to step out as far as possible and return to the original stance position in one step. This Maximum Step Length (MSL) was found to decline with age and balance-impairment and to correlate strongly with measures of balance, fall risk, mobility performance, and self-reported disability in balance-impaired older adults (Cho et al., 2004; Medell and Alexander, 2000). Compared to other gait and balance measures, an alternative version of MSL that did not require returning to the start position in one step showed the greatest decline from the third to the ninth decade of life, even when adjusted for body anthropometry (Lindemann et al., 2003). MSL test-retest reliability is satisfactory and, while MSL was originally conducted in three directions (forward, sideways, and backwards) with both right and left feet, a simplified version more appropriate for clinical settings (right foot forward only) is equally predictive of the above functional outcomes (Cho et al., 2004) and will be employed here.
MSL thus appears to be a measure of fall risk as well as other mobility-related factors. Yet, as in many clinical mobility tests, little is known about the mechanisms underlying variations in MSL. The central question addressed in the present paper is: “Does MSL tell us anything about an individual's leg speed, strength, or power capacities independent of their age?”.
Most tests of volitional stepping (Lord and Fitzpatrick, 2001; Luchies et al., 2002; Patla et al., 1993; White et al., 2002) evaluate only step timing and do not take into account step distance (Cronin et al., 2003; Lord and Fitzpatrick, 2001; Luchies et al., 2002; Luchies et al., 1999; White et al., 2002). Greater step distances likely place greater physiological demands on the hip and knee musculature. Given that strength (Brooks and Faulkner, 1994; Doherty et al., 1993; Frontera et al., 1991; Hakkinen et al., 1996; Lexell, 1995), power (Hakkinen et al., 1997; Izquierdo et al., 1999; Macaluso and De Vito, 2003; Metter et al., 1997; Smeesters et al., 2002; Whipple et al., 1987), and peak contraction velocity (Hortobagyi et al., 1995; Larsson et al., 1979; Pousson et al., 2001) decline with age, might these declines be related to the age-related decline in MSL (Cho et al., 2004; Lindemann et al., 2003; Medell and Alexander, 2000)?
Although the length and timing of perturbation-elicited steps (King et al., 2005; Wojcik et al., 1999), the timing of volitional steps (Lord and Fitzpatrick, 2001; Luchies et al., 2002), and the lower extremity strength required to recover from a forward fall (Madigan and Lloyd, 2005; Pijnappels et al., 2005; Wojcik et al., 2001) have been quantified, we are not aware of published studies relating maximal volitional step length to lower limb strength and power.
The primary goal of this study was to determine if decrements in knee and hip extensor muscle capacities correlate with shorter MSL independent of age group. We also sought to detect differences in performance on the original MSL and on its sub-tasks, i.e. stepping out only and thus omitting the return step as per (Lindemann et al., 2003), or starting in an outstretched position, after which only the return step was executed. These two subtasks will be fully explained in the Methods and will henceforth be referred to as MSL versions.
We hypothesized that the original MSL will a) explain a significant amount of variance in the knee and hip extension speed, strength, and power capacities after controlling for age group, and b) significantly correlate with both other MSL versions. We also hypothesized that c) all MSL versions would have sufficient reliability as indicated by within- and between-block intraclass correlation coefficients (ICC>0.90) to base decisions upon (Nunnally and Bernstein, 1994). Exploratory data were also collected on subjective perceptions of difficulty between the three MSL versions and within specific portions of the original MSL.
If MSL is related to knee and hip extensor capacities (hypotheses a) it might prove to be a rapid, age-independent screening measure of lower-limb function. If different MSL versions correlate with each other (hypothesis b), then the specific version used may not alter the clinical utility of the MSL. If ICC values are sufficiently high, then only a single trial may be required to obtain a valid and reliable MSL.
2. Methods
2.1. Subjects
Eleven younger (mean [SD] age 24[3.4] years) and ten older (mean age 73[5.3] years) unimpaired females participated in this study. All younger subjects completed a medical questionnaire and all older subjects were physically screened by a geriatric nurse-clinician supervised by the physician-geriatrician prior to testing. The older women had no significant abnormal neurological or musculoskeletal findings on directed history and physical. The two groups were of similar stature, but the younger women weighed less than the older women (p=0.008 for weight and p=0.003 for Body Mass Index, Table 1). All subjects wore their own athletic shoes for the MSL testing.
Table 1.
Mean (SD) subject characteristics and Maximum Step Length (MSL) for all three MSL versions
| Younger Women | Older Women | |
|---|---|---|
| Number of subjects | 11 | 10 |
| Mean age (years) * | 24 (3.4) | 73 (5.3) |
| Height (cm) | 163 (7) | 160 (5) |
| Mass (kg) † | 55.0 (5.1) | 68.4 (14.1) |
| Body Mass Index (kg / m2) † | 20.7 (3.2) | 26.7 (3.6) |
| MSL- “Out & Back” (% height) * | 78.5 (5.4) | 57.8 (9.1) |
| MSL- “Out Only” (% height) * | 84.0 (8.2) | 62.2 (10.3) |
| MSL- “Back Only” (% height) * | 75.4 (3.2) | 54.8 (9.6) |
indicates age group effect p<0.0001
indicates age group effect p<0.01
2.2. MSL instrumentation and protocol
Three versions of MSL were evaluated in this study- the original MSL and its two sub-tasks. Only the right leg was tested and trials were considered an error if more than a single step was used (due to a loss of balance), the arms were uncrossed, or the return step landed anterior to the initial lift off position. Optoelectronic markers (Optotrak 3020, Northern Digital, Inc., Waterloo, Canada) were used to measure foot position. There were no criteria for mediolateral placement of footfalls. The first MSL version was the original “Out & Back” version as published by Medell and Alexander (Medell and Alexander, 2000) in which the subject was instructed to “step out as far as possible and return to the starting position using a single step”. For the second MSL version the subject did not have to return to the starting position, but just had to briefly hold the landing position (“Out Only”) as reported by Lindemann and colleagues (Lindemann et al., 2003). The error definitions were identical with the exception of the return step placement requirement. The third MSL version began with the feet separated in the sagittal plane by a self-selected initial step length whereupon subjects had to push on their forward foot hard enough so as to regain the “feet together” position with a single step that placed the stepped foot posterior to the non-stepped foot (“Back Only”). Subjects were advised to first attempt an initial step length that was a little less than they could achieve on the “Out & Back” version. A handrail device, similar to a shortened walker, was used to assist the subject in reaching and maintaining the starting position. This device was removed prior to the start of each trial. After successful trials the subjects were encouraged to try a greater initial step length for the next trial and after unsuccessful trials the subjects were instructed to try the same or a shorter initial step length.
After a standardized warm-up consisting of stretching, walking in place, and short practice steps, five blocks of five trials each were presented in the following order to each subject: 1) “Out & Back”, 2) “Out Only”, 3) “Back Only”, 4) “Out & Back”, 5) “Out Only”. This order was chosen to present the least physically-demanding task first to lessen any risk of injury. The most demanding task (“Back Only”) was presented only once and the other two tasks were presented twice to evaluate practice effects. The approximate step length of the prior trial was given to the subject after each trial by a spotter located near the foot landing position, who also encouraged the subject to attempt to surpass this step length in the next trial. Several seconds of rest were provided between trials within each block and several minutes of rest were provided between trial blocks. Actual step distance and errors of foot placement were determined by foot marker positions.
Subjects were asked to rank the relative difficulty of the three MSL versions (“Out & Back”, “Out Only”, “Back Only”), and the phases of the “Out & Back” MSL (“Swing Leg Out”, “Stop Body Motion”, “Balance while Feet are Apart”, and “Push Back to Starting Position”).
2.3. Knee and hip extension capacity instrumentation and protocol
A custom dynamometer (Smeesters et al., 2002), developed to determine peak power generation (Biologic Engineering, Dexter, MI, USA) was used to record knee and hip extension speed, strength, and power capacities for each subject tested (Figure 1). The dynamometer apparatus was not instrumented to take measurements at the ankle. Subjects were placed on their left side with the upper body secured so that the right leg hip joint was aligned with the center of rotation of the lever arm for hip extensor tests. The right leg was secured to the lever arm at the ankle with the right knee near full extension but not locked. For knee extensor tests, the knee joint center was aligned with the center of rotation of the lever arm while the thigh was secured to the apparatus. The rotational damping of the low-inertia lever arm to movement in the horizontal plane was adjustable between negligible and infinite values. Dedicated angular position and torque sensors were sampled and recorded at 500 Hz via a 16-bit analog-to-digital converter and microprocessor. From the measurements obtained, speed and power were calculated after corrections for the dynamometer leg lever mass and inertial effects. Real-time feedback of peak power was marked on a plot of power vs. speed on a laptop computer screen in front of the subject.
Fig. 1.
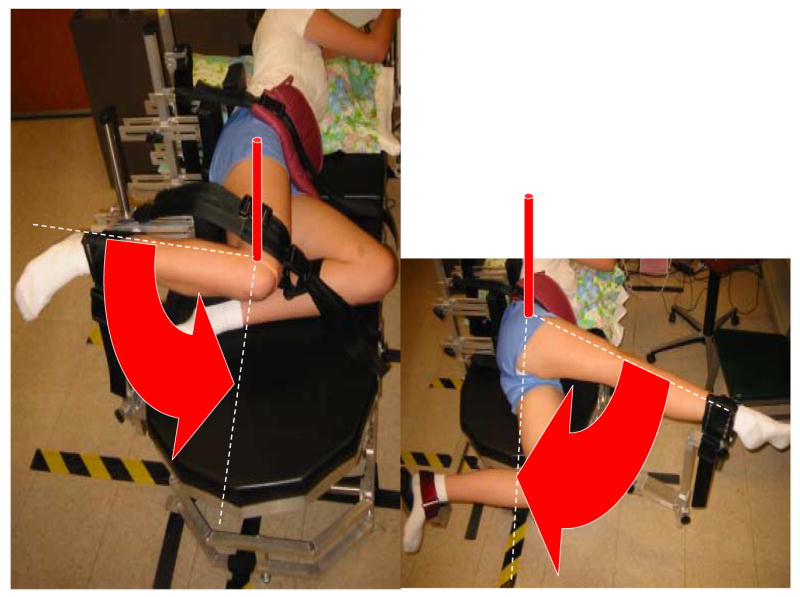
Custom dynamometer used to determine knee (left) and hip (right) extension speed, strength, and power capacities.
Knee and hip extension speed, strength, and power capacities were determined by instructing the subject to move the lever arm “as fast as possible” through a required range of motion: 60° to 0° flexion for the hip, with the knee near full extension; and 90° to 0° flexion for the knee, where 0° is the anatomical position in extension and a positive angle denotes knee extension. Five similarly-spaced damping levels ranging from negligible (maximum speed) to a large viscous damping representing near-isometric conditions (maximum strength) were tested. Note that the variable damping of this dynamometer mean that it is neither isokinetic nor isotonic. As few as two and as many as five repetitions were performed at each of the five resistance levels until two replicates within 10% of each other were identified.
Subjects were first tested at the negligible damping setting to determine their extension velocity capacity, which was the average of the two consistent (within 10%) values at this damping level. Similarly, the extension strength capacity was the average of the two consistent (within 10%) moment values at the highest damping setting tested. Power capacity was calculated as the product of moment and velocity and was defined as the peak value of an inverted parabola fitted to the consistent data on a plot of power vs. speed via a least squares approach.
Tests of the knee and hip extension speed, strength, and power capacities were performed at least one day apart from the MSL tests to minimize muscle fatigue and soreness. Both the order of the test appointments and the order of the hip and knee tests were randomized.
2.4. Data Processing & Analysis
Custom software routines in Matlab (v6.5, Natick, MA, USA) were used to process all data. Marker data were sampled at 100 Hz and filtered using a low-pass Butterworth filter with a 6 Hz cutoff frequency using forward and backwards passes to minimize initial and final time artifacts. Step length and errors were determined from foot marker data. Trials counted as errors (i.e., those with losses of balance, multiple steps, or did not return to the starting position when this was required) were excluded from subsequent analysis. The MSL was the longest valid step length for each MSL version. To facilitate inter-individual comparisons, all MSL data were normalized to subject height and knee and hip strength and power were normalized to the product of subject height and weight. Non-normalized data are available from the corresponding author.
2.5. Statistical Analyses
Unpaired t-tests were used to compare subject group differences in height, weight, body mass index. One-way analyses of variance were used to evaluate the effects of MSL version. Linear regressions were used to correlate all three MSL versions to each other.
Age group and MSL could not be simultaneously included in a single multiple linear regression model because they have previously been shown to be correlated (Cho et al., 2004; Medell and Alexander, 2000). To avoid potential distortion of results due to collinearity of the independent variables (Pedhauzer, 1997), four regression models were used to predict all six dependent variable (knee and hip extension speed, strength, and power capacities): First, two simple linear regression models were used to predict the independent effects of age group alone (model 1) and MSL alone (model 2). Then, two order-dependent multi-stage linear regression models (Pedhauzer, 1997) were employed where MSL was added to the age group model (model 3) and age group added to the MSL model (model 4). Models 1 and 2 enable the determination of the variance explained by each independent variable alone, while models 3 and 4 are multistage regressions that enable the determination the additional variance, if any, explained by the secondary variable.
Intraclass correlation coefficients (ICCs) were used to evaluate within-block (between all valid trials) and between-block (using best trials within each block) reliability. Because only the “Out & Back” and “Back Only” versions were repeated, between-block ICC values were only calculated for these versions. SPSS and SAS (SAS Institute Inc., Carey, NC, USA) were used to conduct all statistical analyses and p<0.05 was considered statistically significant.
3. Results
3.1. Effects of Age
As expected, the younger women stepped further than the older women for all MSL versions (mean[SD], 79[7]% vs. 58[10]% height, respectively; p<0.0001 for all MSL versions). Only one older subject stepped within the range of the young.
3.2. Correlations of Knee and Hip Extension Speed, Strength, and Power to Age Group and “Out & Back” MSL
The younger women were capable of greater knee and hip extension speed, strength, and power than the older women (Table 2). Since all three MSL versions were correlated with one another, only the original “Out & Back” MSL version was correlated with the knee and hip extension speed, strength, and power capacities (Fig. 2).
Table 2.
Mean (SD) of peak normalized (to height[ht] in m and weight[wt] in N) joint extension capacities as measured by custom dynamometer.
| Younger Women | Older Women | |
|---|---|---|
| Knee Speed (deg/s) | 457 (33) * | 388 (42) |
| Knee Strength (Nm/(ht*wt)) | 0.0590 (0.0096) * | 0.0366 (0.0077) |
| Knee Power (W/(ht*wt)) | 0.300 (0.043) * | 0.148 (0.038) |
| Hip Speed (deg/s) | 337 (46) † | 289 (52) |
| Hip Strength (Nm/(ht*wt)) | 0.0590 (0.0096) * | 0.0366 (0.0077) |
| Hip Power (W/(ht*wt)) | 0.300 (0.043) * | 0.148 (0.038) |
indicates age group effect p<0.0001
indicates age group effect p=0.001
Fig. 2.
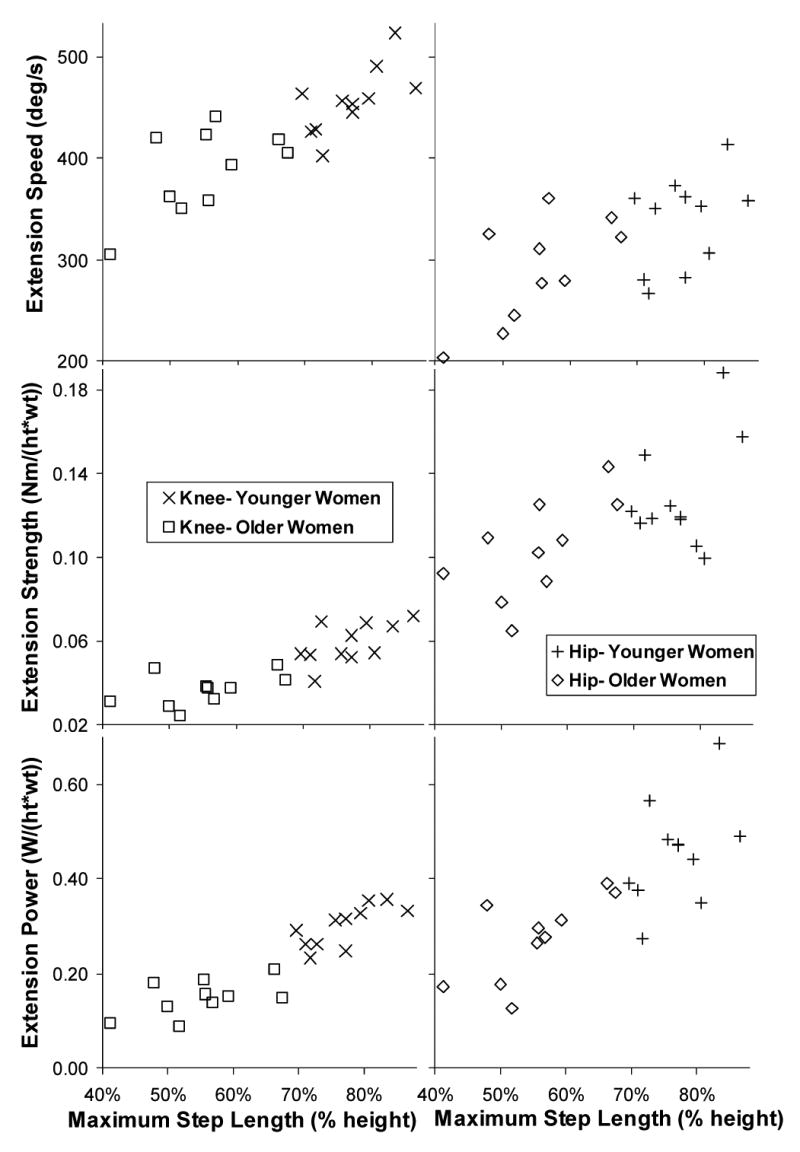
Normalized knee (left column) and hip (right column) extension speed (top row), strength (middle row), and power (bottom row) capacities plotted against normalized Maximum Step Length (MSL) by age group for “Out & Back” MSL version. “ht” refers to subject height in m and “wt” refers to subject weight in N.
As anticipated, age group and MSL were correlated with each other (p<0.0001, R2=0.69). The results of the simple linear regression models (models 1 and 2) indicate that both MSL and age group were significantly correlated with all knee and hip extension speed, strength, and power capacities. Model 3 indicated that, with the exception of knee power, MSL explained a greater percentage of the variance in all knee and hip joint extension capacities than age group and was a significant contributor to the model after accounting for age group (Fig. 2 and Table 3). Model 4 indicated that age group only explained a significant amount of additional variance in knee power after accounting for MSL.
Table 3.
Linear regressions of peak normalized knee and hip extension speed, strength, and power capacities on age group alone, original “Out & Back” Maximum Step Length (MSL) alone, and MSL after accounting for age group (younger=1 and older=2). Regression coefficients shown are for the combined model unless no additional variance was explained by including age group. Kinetics normalized to height (h) in m and weight (wt) in N.
| Age Group Alone | MSL Alone | MSL added to Age Group (Type I SS) | Regression Coefficients * | Total | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|||||||||||
| Capacity | p | R2 | p | R2 | p (Age Group) | p (MSL) | increment to R2 | Constant | Age Group | MSL | R2 |
| Knee Speed [deg/s] | 0.0005 | 0.48 | <0.0001 | 0.66 | <0.0001 | 0.0069 | 0.18 | 203. | N/A † | 321. | 0.66 |
| Knee Strength [Nm/(ht*wt)] | <0.0001 | 0.64 | <0.0001 | 0.69 | <0.0001 | 0.0265 | 0.09 | 0.0231 | −0.0103 | 0.0589 | 0.73 |
| Knee Power [W/(ht*wt)] | <0.0001 | 0.79 | <0.0001 | 0.78 | <0.0001 | 0.0105 | 0.06 | 0.1470 | −0.0884 | 0.308 | 0.86 |
| Hip Speed [deg/s] | 0.0382 | 0.21 | 0.0017 | 0.41 | 0.0198 | 0.0162 | 0.22 | 34.8 | 25.4 | 353. | 0.43 |
| Hip Strength [Nm/(ht*wt)] | 0.0314 | 0.22 | 0.0018 | 0.41 | 0.0172 | 0.0225 | 0.20 | −0.0154 | 0.0103 | 0.171 | 0.42 |
| Hip Power [W/(ht*wt)] | 0.0006 | 0.47 | <0.0001 | 0.60 | 0.0002 | 0.0206 | 0.14 | −0.0640 | −0.0352 | 0.706 | 0.61 |
Units of all coefficients are same as dependent variable (all independent variables dimensionless)
No benefit to including age group in model
3.3. Effects of MSL Version
No significant differences were found between MSL version (“Out Only”=74[14]%, “Out & Back”=69[13]%, “Back Only”=66[13]% height). All three MSL versions correlated with each other (“Out & Back” vs. “Out Only” p<0.0001, R2=0.92; “Out & Back” vs. “Back Only” p<0.0001, R2=0.86; “Out Only” vs. “Back Only” p<0.0001, R2=0.78). The “Out Only” MSL version had the fewest trials with errors (4%, p<0.0001). There was no significant difference in error rate between the “Out & Back” (23%) and “Back Only” (27%) versions.
3.4. Within and Between-Block Effects
The within-block ICC values were high for all blocks (block 1 = 0.91, block 2 = 0.93, block 3 = 0.93, block 4 = 0.95, block 5 = 0.95). When the best trials of the two repeated versions were compared the ICCs were also high (“Out & Back” = 0.91 and “Out Only” = 0.95).
3.5. Perceptions of Difficulty
None of the young and only one of the old subjects rated the “Out Only” version as most difficult while ten of the young and four of the old subjects rated the “Back Only” version as most difficult. Nine of the young and five of the old subjects rated the “Push Back to Starting Position” phase of the original MSL (i.e. the return step) as most difficult of the four MSL phases.
4. Discussion
Order-dependent multistage regressions indicated that MSL explained a significant amount of the variance in all knee (6-18% more) and hip (14-22% more) extension speed, strength, and power capacities after accounting for age group. Age group explained an additional 8% of the variation in knee extension power capacity after accounting for MSL and did not explain a significant amount of additional variation in any other capacity. All MSL versions correlated with one another and all within- and between-block ICC values were high (>0.9). As expected, younger women demonstrated greater MSL on all versions and greater knee and hip extension speed, strength, and power capacities than the older women.
Our initial hypothesis that MSL would explain a greater percentage of the variance in knee and hip extension speed, strength, and power capacities than age group was supported. However, the specific capacity parameter or combination of parameters underlying performance on the MSL test that contribute to age group-related decrements or fall risk cannot be identified without a more detailed biomechanical analysis. Such a biomechanical analyses should help provide a better understanding of the key factors (i.e., maximum leg power) contributing to clinical test performance, and ultimately, better insight into how changes in these parameters might lead to declines or improvements in mobility performance. One way to address the confound between age and MSL would be to test young and old adults stepping at similar constrained lengths.
Our hypothesis of correlation between MSL versions was supported. While not statistically tested, the subjective perceptions of difficulty led to insights about the possible differences between MSL versions. Both age groups perceived the “push back to start” phase of the “Out & Back” MSL version as the most difficult, suggesting a level of challenge that is absent from the “Out Only” version (Lindemann et al., 2003). This is The “Out Only” MSL version was best tolerated and seemed to be the easiest to explain to subjects, but the return step may require different abilities and detect different impairments that were not explored by this study. The “Back Only” MSL version required additional equipment (low handrails) to reach the starting position, seemed to be the most difficult to explain to subjects, and had the greatest percentage of trials with errors.
Clinicians may desire to predict lower extremity speed, strength, and power capacities using MSL while biomechanists may prefer to predict MSL given maximal joint speed, strength, and power capacities. Regardless of which equation is used, age group seems to be a relatively minor contributor. We caution that MSL may not correlate with leg capacities in the presence of functional asymmetries or other impairments, as synergistic movements of multiple joints are required in addition to balance control and joint capacities. While this interdependence may limit the utility of MSL as a clinical predictor of specific joint capacities, it may also increase the utility of MSL as a comprehensive screening measure for overall function, as MSL seems to be a predictor of underlying leg capacity, irrespective of age.
Our final hypothesis of high (>0.90) within- and between-block ICC values was supported. Note that while MSL was defined here and previously (Lindemann et al., 2003) as the longest valid step of five trials, it has also been defined as the mean of these five trials (Cho et al., 2004; Medell and Alexander, 2000), and it would be possible to define MSL as the first valid step. Reprocessing these data using the mean of all valid trials or the first valid trial did not alter the findings. Given the excellent consistency between definition of MSL (longest step, mean step length, or first valid step), within block ICC, and between block ICC, a single step of maximal length appears to be as predictive as the longest step or the mean step length. However, a warm-up should be used to reduce the chance of injury as was done in the present study.
It should be noted that the traction between the shoe sole and flooring material is an important factor to consider. If the flooring material is too slick then the foot may slide during the step landing, which is potentially dangerous. Providing an anti-slip (sandpaper-like) flooring surface was found to completely eliminate this slipping problem, but instead caused difficulty in executing the return step, because the stepping foot had to be completely lifted clear of the ground before it could begin its return journey. All subjects in this experiment wore athletic shoes and stepped onto the force plates. This combination proved to be an acceptable compromise of friction coefficient, but optimization of the foot-floor friction coefficient may also optimize the MSL possible for versions that include a return step. Considering that large plantarflexion moments have been shown to be required for recovery from a trip (Pijnappels et al., 2005), a limitation of the present study is that the dynamometer was not instrumented to take measurements at the ankle. Additionally, since only unimpaired females were tested, the results may not be extrapolated to males or impaired subjects without further research.
5. Conclusions
Shorter MSL correlates with reduced knee and hip extension speed, strength, and power capacities after accounting for age differences. A single valid trial seems be as predictive as the longest step or the mean step length and of the three different MSL versions tested, the “Out & Back” version is both feasible and useful in that it is likely provide more insight into underlying functional impairment.
Fig. 3.
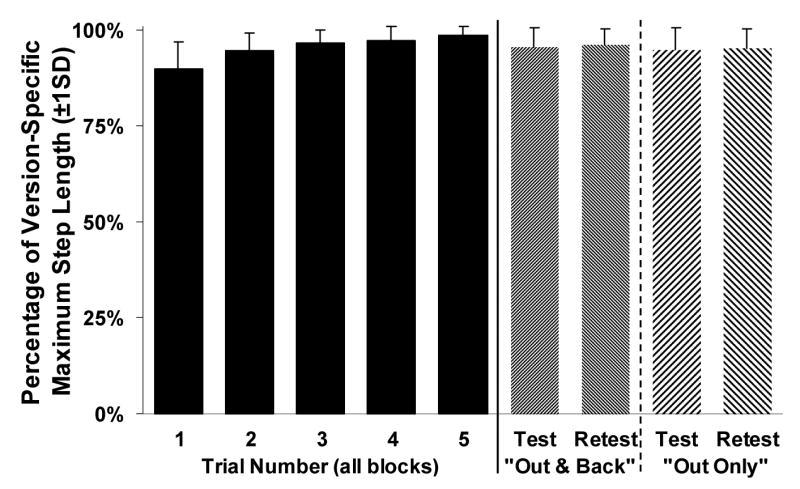
Step lengths of each trial across all blocks and step lengths of test-retest blocks. Step lengths shown as percentage of the version-specific Maximum Step Length (MSL).
Acknowledgments
We thank Eric Battjes, Adriana Figueroa, Steve Luther, and Janet Kemp for their assistance with this study. The authors wish to acknowledge the support of National Institute on Aging (NIA) Claude Pepper Older Adults Independence Center grant P60 AG08808, Institute of Gerontology Training grant 5T32 AG000114, GEM predoctoral fellowship, NIA grant P01 AG10542, and the Department of Veterans Affairs Research and Development and the VA Ann Arbor Health Care System GRECC. Dr. Alexander is also a recipient of a Mid-Career Investigator Award in Patient-Oriented Research K24 AG109675 from NIA.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Alexander NB. Postural control in older adults. J Am Geriatr Soc. 1994;42:93–108. doi: 10.1111/j.1532-5415.1994.tb06081.x. [DOI] [PubMed] [Google Scholar]
- 2.Baker SP, O'Neill B, Ginsburg MJ, Li G. The Injury Fact Book. Vol. 1. Oxford University Press; Oxford, New York: 1992. p. 344. [Google Scholar]
- 3.Brooks SV, Faulkner JA. Skeletal muscle weakness in old age: underlying mechanisms. Med Sci Sports Exerc. 1994;26:432–9. [PubMed] [Google Scholar]
- 4.CDC. National Center for Injury Prevention and Control. Vol. 2003. Centers for Disease Control and Prevention; 2000. [Google Scholar]
- 5.Cho BL, Scarpace D, Alexander NB. Tests of stepping as indicators of mobility, balance, and fall risk in balance-impaired older adults. J Am Geriatr Soc. 2004;52:1168–73. doi: 10.1111/j.1532-5415.2004.52317.x. [DOI] [PubMed] [Google Scholar]
- 6.Cronin J, McNair PJ, Marshall RN. Lunge performance and its determinants. J Sports Sci. 2003;21:49–57. doi: 10.1080/0264041031000070958. [DOI] [PubMed] [Google Scholar]
- 7.Doherty TJ, Vandervoort AA, Taylor AW, Brown WF. Effects of motor unit losses on strength in older men and women. J Appl Physiol. 1993;74:868–74. doi: 10.1152/jappl.1993.74.2.868. [DOI] [PubMed] [Google Scholar]
- 8.Frontera WR, Hughes VA, Lutz KJ, Evans WJ. A cross-sectional study of muscle strength and mass in 45- to 78-yr-old men and women. J Appl Physiol. 1991;71:644–50. doi: 10.1152/jappl.1991.71.2.644. [DOI] [PubMed] [Google Scholar]
- 9.Hakkinen K, Kraemer WJ, Kallinen M, Linnamo V, Pastinen UM, Newton RU. Bilateral and unilateral neuromuscular function and muscle cross-sectional area in middle-aged and elderly men and women. J Gerontol A Biol Sci Med Sci. 1996;51:B21–9. doi: 10.1093/gerona/51a.1.b21. [DOI] [PubMed] [Google Scholar]
- 10.Hakkinen K, Kraemer WJ, Newton RU. Muscle activation and force production during bilateral and unilateral concentric and isometric contractions of the knee extensors in men and women at different ages. Electromyogr Clin Neurophysiol. 1997;37:131–42. [PubMed] [Google Scholar]
- 11.Hortobagyi T, Zheng D, Weidner M, Lambert NJ, Westbrook S, Houmard JA. The influence of aging on muscle strength and muscle fiber characteristics with special reference to eccentric strength. J Gerontol A Biol Sci Med Sci. 1995;50:B399–406. doi: 10.1093/gerona/50a.6.b399. [DOI] [PubMed] [Google Scholar]
- 12.Izquierdo M, Ibanez J, Gorostiaga E, Garrues M, Zuniga A, Anton A, Larrion JL, Hakkinen K. Maximal strength and power characteristics in isometric and dynamic actions of the upper and lower extremities in middle-aged and older men. Acta Physiol Scand. 1999;167:57–68. doi: 10.1046/j.1365-201x.1999.00590.x. [DOI] [PubMed] [Google Scholar]
- 13.King GW, Luchies CW, Stylianou AP, Schiffman JM, Thelen DG. Effects of step length on stepping responses used to arrest a forward fall. Gait Posture. 2005;22:219–24. doi: 10.1016/j.gaitpost.2004.09.008. [DOI] [PubMed] [Google Scholar]
- 14.Larsson L, Grimby G, Karlsson J. Muscle strength and speed of movement in relation to age and muscle morphology. J Appl Physiol. 1979;46:451–6. doi: 10.1152/jappl.1979.46.3.451. [DOI] [PubMed] [Google Scholar]
- 15.Lexell J. Human aging, muscle mass, and fiber type composition. J Gerontol A Biol Sci Med Sci. 1995;50 doi: 10.1093/gerona/50a.special_issue.11. Spec No, 11-6. [DOI] [PubMed] [Google Scholar]
- 16.Lindemann U, Bauerle C, Muche R, Kikolaus T, Becker C. Age-related differences in balance, strength, and motor function. European Journal of Geriatrics. 2003;5:15–22. [Google Scholar]
- 17.Lord SR, Fitzpatrick RC. Choice stepping reaction time: a composite measure of falls risk in older people. J Gerontol A Biol Sci Med Sci. 2001;56:M627–32. doi: 10.1093/gerona/56.10.m627. [DOI] [PubMed] [Google Scholar]
- 18.Luchies CW, Alexander NB, Schultz AB, Ashton-Miller J. Stepping responses of young and old adults to postural disturbances: kinematics. J Am Geriatr Soc. 1994;42:506–12. doi: 10.1111/j.1532-5415.1994.tb04972.x. [DOI] [PubMed] [Google Scholar]
- 19.Luchies CW, Schiffman J, Richards LG, Thompson MR, Bazuin D, DeYoung AJ. Effects of age, step direction, and reaction condition on the ability to step quickly. J Gerontol A Biol Sci Med Sci. 2002;57:M246–9. doi: 10.1093/gerona/57.4.m246. [DOI] [PubMed] [Google Scholar]
- 20.Luchies CW, Wallace D, Pazdur R, Young S, DeYoung AJ. Effects of age on balance assessment using voluntary and involuntary step tasks. J Gerontol A Biol Sci Med Sci. 1999;54:M140–4. doi: 10.1093/gerona/54.3.m140. [DOI] [PubMed] [Google Scholar]
- 21.Macaluso A, De Vito G. Comparison between young and older women in explosive power output and its determinants during a single leg-press action after optimisation of load. Eur J Appl Physiol. 2003;90:458–63. doi: 10.1007/s00421-003-0866-7. [DOI] [PubMed] [Google Scholar]
- 22.Madigan ML, Lloyd EM. Age-related differences in peak joint torques during the support phase of single-step recovery from a forward fall. J Gerontol A Biol Sci Med Sci. 2005;60:910–4. doi: 10.1093/gerona/60.7.910. [DOI] [PubMed] [Google Scholar]
- 23.Maki BE, McIlroy WE. The control of foot placement during compensatory stepping reactions: does speed of response take precedence over stability? IEEE Trans Rehabil Eng. 1999;7:80–90. doi: 10.1109/86.750556. [DOI] [PubMed] [Google Scholar]
- 24.Medell JL, Alexander NB. A clinical measure of maximal and rapid stepping in older women. J Gerontol A Biol Sci Med Sci. 2000;55:M429–33. doi: 10.1093/gerona/55.8.m429. [DOI] [PubMed] [Google Scholar]
- 25.Metter EJ, Conwit R, Tobin J, Fozard JL. Age-associated loss of power and strength in the upper extremities in women and men. J Gerontol A Biol Sci Med Sci. 1997;52:B267–76. doi: 10.1093/gerona/52a.5.b267. [DOI] [PubMed] [Google Scholar]
- 26.Nunnally JC, Bernstein IH. Psychometric Theory. McGraw-Hill; New York: 1994. Chapter 7: The Assessment of Reliability; pp. 264–265. [Google Scholar]
- 27.Patla AE, Frank JS, Winter DA, Rietdyk S, Prentice S, Prasad S. Age-related changes in balance control system: initiation of stepping. Clinical Biomechanics. 1993;8:179–184. doi: 10.1016/0268-0033(93)90012-7. [DOI] [PubMed] [Google Scholar]
- 28.Pedhauzer EJ. Multiple Regression In Behavioural Research. Harcourt Brace College Publishers; Fort Worth: 1997. Multiple Regression Analysis: Explanation; pp. 294–318. [Google Scholar]
- 29.Pijnappels M, Bobbert MF, van Dieen JH. How early reactions in the support limb contribute to balance recovery after tripping. J Biomech. 2005;38:627–34. doi: 10.1016/j.jbiomech.2004.03.029. [DOI] [PubMed] [Google Scholar]
- 30.Pousson M, Lepers R, Van Hoecke J. Changes in isokinetic torque and muscular activity of elbow flexors muscles with age. Exp Gerontol. 2001;36:1687–98. doi: 10.1016/s0531-5565(01)00143-7. [DOI] [PubMed] [Google Scholar]
- 31.Smeesters C, Cole NM, Ashton-Miller J. World Congress of Biomechanics. Calgary, Alberta, Canada: 2002. Effects of age and gender on maximum hip flexion power at low and high velocities. [Google Scholar]
- 32.Thelen DG, Wojcik LA, Schultz AB, Ashton-Miller JA, Alexander NB. Age differences in using a rapid step to regain balance during a forward fall. J Gerontol A Biol Sci Med Sci. 1997;52:M8–13. doi: 10.1093/gerona/52a.1.m8. [DOI] [PubMed] [Google Scholar]
- 33.Whipple RH, Wolfson LI, Amerman PM. The relationship of knee and ankle weakness to falls in nursing home residents: an isokinetic study. J Am Geriatr Soc. 1987;35:13–20. doi: 10.1111/j.1532-5415.1987.tb01313.x. [DOI] [PubMed] [Google Scholar]
- 34.White KN, Gunter KB, Snow CM. The Quick Step: A New Test for Measuring Reaction Time and Lateral Stepping Velocity. Journal of Applied Biomechanics. 2002;18:271–277. [Google Scholar]
- 35.Wojcik LA, Thelen DG, Schultz AB, Ashton-Miller JA, Alexander NB. Age and gender differences in single-step recovery from a forward fall. J Gerontol A Biol Sci Med Sci. 1999;54:M44–50. doi: 10.1093/gerona/54.1.m44. [DOI] [PubMed] [Google Scholar]
- 36.Wojcik LA, Thelen DG, Schultz AB, Ashton-Miller JA, Alexander NB. Age and gender differences in peak lower extremity joint torques and ranges of motion used during single-step balance recovery from a forward fall. J Biomech. 2001;34:67–73. doi: 10.1016/s0021-9290(00)00152-4. [DOI] [PubMed] [Google Scholar]