

Abstract
Previous studies have found evidence for gender and racial/ethnic differences in depressive symptoms in adolescence; however, the mechanisms driving this relationship are poorly understood. The goal of this study was to examine the role of individual differences in dispositional coping in the relationships between gender and depressive symptomatology, and race/ethnicity and depressive symptomatology. Surveys were administered to 905 15-17 year old adolescents (mean age 16.10, SD = .67; 54% girls, n = 485) in the spring of 2007, 2008, and 2009. Girls reported more depressive symptomatology than boys and endorsed a greater disposition for the following coping strategies in comparison to boys: emotional social support, instrumental social support, and venting emotions. When race/ethnicity was examined, African-American adolescents reported a greater tendency toward using religious coping than Caucasian and Hispanic adolescents. Dispositional coping preferences also were found to mediate the relationships between gender and depressive symptomatology. These findings indicated that a preference for venting emotions may be particularly problematic when endorsed by girls, whereas instrumental social support may be particularly helpful for girls.
Keywords: adolescence, coping, depressive symptoms, gender, race
Introduction
Adolescence is a time of dramatic growth and opportunity on the one hand (e.g., Forbes & Dahl, 2010; Spear, 2000), and a time of increased stress and vulnerability on the other hand (Costello, Erkanli, & Angold, 2006; Hollenstein & Lougheed, 2013). The ability to self-regulate under stress or to cope is a critical factor that may aid adolescents in negotiating the challenging period of adolescence (e.g., Zimmer-Gembeck & Skinner, 2011). However, previous research has demonstrated that there are gender (e.g., Eschenbeck, Kohlmann, & Lohaus, 2007) and racial/ethnic (e.g., Chapman & Mullis, 2000) differences in dispositional coping strategies as well as in the incidence of symptoms of depression during adolescence (Kouros & Garber, 2014; Li, DiGiuseppe, & Froh, 2006; Wight, Aneshensel, Botticello, & Sepúlveda, 2005). The current study postulates that differences in coping tendencies may be a mechanism that could explain gender and racial/ethnic differences in the incidence of depressive symptoms during adolescence.
Depressive Symptoms
Throughout adolescence, the incidence of dysphoria increases dramatically. Subclinical depression is common during this period and results in both functional impairment and increased risk of suicide (Balázs et al., 2013), particularly for girls and minority adolescents. Compared with boys, girls report significantly greater subclinical symptoms of depression (Li et al., 2006). Girls also appear to experience a significant increase in stressors and stressful life events during adolescence, which in turn, may contribute to vulnerability to depressive symptoms (Ge, Lorenz, Conger, Elder, & Simons, 1994; Hankin, Mermelstein, & Roesch, 2007; Telzer & Fuligni, 2013). Among minority adolescents, some studies indicate that African-American and Hispanic adolescents are more likely to experience symptoms of depression compared with Caucasian adolescents, even when controlling for other risk factors such as family structure, socioeconomic status, and community ethnic composition (e.g., Wight et al., 2005). Ethnic minority status may be inextricably linked with experiences that put adolescents at risk for depression such as discrimination or victimization. Compounding this difference, symptoms of depression are less likely to be detected and diagnosed in minority populations (e.g., Stockdale, Lagomasino, Siddique, McGuire & Miranda, 2008). Although risk factors for depression are diverse (i.e., genes, SES; Beardslee & Gladstone, 2001), dispositional coping appears to be a particularly important individual difference variable that may affect the incidence and course of depressive symptomatology during adolescence (Kort-Butler, 2009).
Coping
Coping involves effortful strategies used to regulate stress (e.g., Zimmer-Gembeck & Skinner, 2011). Coping may be conceptualized as a situational response to a stressor or as an individual difference dimension representing a dispositional style of responding to stress (Carver, Scheier, & Weintraub, 1989). Dispositional coping may represent the “structure” which shapes the way the process of coping unfolds in a given situation (Lazarus & Folkman, 1984). Indeed, dispositional coping preferences have been found to be associated with personality dimensions such as optimism, self-esteem, and hardiness, as well as with situational coping responses (Carver et al., 1989).
Coping may broadly be conceptualized based on whether the goal is to change the situation (problem-focused) or to change the way one feels (emotion-focused; Folkman & Lazarus, 1980). Alternatively, one may consider whether the strategy is oriented toward approaching the problem or avoiding it (Herman-Stahl, Stemmler, & Petersen, 1995). However, these dichotomous approaches used to assess coping often have proved to be overly simplistic (Carver et al., 1989). Factor analyses indicate that coping strategies used by adolescents rarely fall within two dimensions only (e.g. Connor-Smith, Compas, Wadsworth, Thomsen, & Saltzman, 2000). Indeed, widely published coping measures used with children have included three factors (Pain Response Inventory; Walker, Smith, Garber, & Van Slyke, 1997), four factors (Children's Coping Strategies Checklist; Ayers, Sandler, West, & Roosa, 1996), or five factors (Responses to Stress Questionnaire; Connor-Smith et al., 2000). This disagreement in number of coping factors is troubling. Furthermore, some strategies that are used to cope with stress, such as seeking emotional social support from others, may have elements of multiple factors, such as both problem-focused and emotion-focused. Finally, it is important to consider that coping dichotomies tend to be empirically derived, rather than theory-driven. In order to improve construct validity, the assessment of coping should be based on theory as well as data.
Some scholars have come to favor an approach in which individual coping strategies are assessed, as opposed to coping dimensions (e.g., Carver et al., 1989; Zimmer-Gembeck & Skinner, 2011). This individualized approach is more nuanced and allows for investigating preferences for specific coping strategies. It breaks down coping dimensions such as problem-focused coping into the strategies which comprise it (i.e. active coping, planning), allowing for a more detailed examination of coping dispositions. Furthermore, this approach eliminates the problem of some strategies, such as seeking emotional support, mapping onto multiple coping dimensions.
Coping follows a developmental trajectory with gains made over the course of adolescence due to the integration of new, age-appropriate coping strategies such as planning and cognitive distraction, which both involve cognitive control and self-awareness (Zimmer-Gembeck & Skinner, 2011). Cognitive advances during adolescence allow for more flexibility in coping; however, individual differences may affect which strategies are used and when they are used. For example, individual differences in conscientiousness, peer influence, and rule following have been found to predict dispositional use of active versus disengagement oriented coping (Nicholls, Perry, Jones, Morely, & Carson, 2013).
Of note, evidence suggests that significant gender and racial/ethnic differences in coping exist during adolescence (e.g., Eschenbeck et al., 2007; Moodley, Esterhuyse, & Beukes, 2014). When examining gender differences in coping, several patterns emerge. One of the most robust findings in the literature is that girls use social support more often than do boys (Eschenbeck et al., 2007; Moodley et al., 2014; Seiffge-Krenke, 2011). Other findings indicate that boys report using more problem-focused strategies than do girls, whereas girls report using more emotion-focused, strategies in comparison to boys (Kort-Butler, 2009; Seiffge-Krenke, 2011). Evidence also suggests that girls may use a wider, more flexible repertoire of coping strategies than do boys (Cicognani, 2011) or that girls may use coping strategies more often than boys in general (Wilson, Pritchard, & Revalee, 2005). It should be noted, however, that few studies have examined gender differences in specific coping strategies such as humor, denial, and religious coping.
The representation of minority groups is growing in the coping literature; however, only a handful of investigations have compared multiple ethnic groups within a single study. Across some studies, Caucasian adolescents have been found to report more frequent use of ventilation of emotion than African-American adolescents; whereas African-American and Hispanic adolescents have reported more frequent use of seeking social support and religious coping than Caucasian adolescents (Chapman & Mullis, 2000; Molock & Barksdale, 2013; Plucker, 1998). African-American adolescents also have been identified as more likely than Caucasian adolescents to be complex copers or to favor many varied coping strategies, including both active and passive styles (Lewis, Byrd, & Ollendick, 2012; Tolan, Gorman-Smith, Henry, Chung, & Hunt, 2002). On the other hand, in a study comparing various low-SES, minority groups, no ethnic differences in active, avoidant, or low generic coping were found (Aldridge & Roesch, 2008). Racial/ethnic differences in many other coping strategies, such as denial or humor coping, have not been examined. These strategies, particularly denial, may be especially important to examine given the perceived uncontrollability of stressors facing many minority youth, coupled with attempts to match coping strategies to the stressor (Compas, 1987).
Coping and Depressive Symptoms
Good coping skills help adolescents adapt to the developmental challenges that occur during adolescence. However, maladaptive coping responses are associated with elevated stress and psychological difficulties (Cairns, Yap, Pilkington, & Jorm, 2014). For example, active coping strategies, in which the adolescent is doing something to address or solve the problem, have been linked with reduced symptoms of adolescent depression (Dunbar, McKee, Rakow, Watson, Forehand, & Compas, 2013). Avoidance coping, on the other hand, has been linked to increased symptoms of depression (e.g., Kort-Butler, 2009), and this is especially true among adolescents with low levels of emotional intelligence (Davis & Humphrey, 2012), and those who engage specifically in behavioral disengagement (Horwitz, Hill, & King, 2011). Religious coping has been associated with a lower incidence of symptoms of depression among urban girls (e.g., Carleton, Esparza, Thaxter, & Grant, 2008); however, this finding is inconsistent. Some studies have found no association (e.g., Dew et al., 2008), and others have found that positive religious coping is only marginally protective against depression, whereas negative religious coping actually intensifies the effect of stress on depression (Carpenter, Laney, & Mezulis, 2012). Research also has indicated that humor and active coping may be associated with less dysphoria among adolescents (Freiheit, Overholser, & Lehnert, 1998), whereas denial and ventilation of emotions may be associated with increased dysphoria (Sontag & Graber, 2010). Lack of planning has been associated with increased symptoms of depression among adolescents as well (Rawana & Kohut, 2012).
Examining how specific coping strategies relate to symptoms of depression is important because of the nuanced nature of coping dimensions. As noted, some coping strategies may map onto multiple dimensions. Furthermore, there is variability among strategies within coping dimensions. For instance, within the domain of emotion-focused strategies, some strategies may be viewed as more passive (i.e., venting emotions), whereas others appear to be more active (i.e., seeking emotional support). Thus, within a dimension, some specific emotion-focused strategies may relate to depressive symptomatology differently than others. These limitations of the dimensional approach necessitate the examination of specific coping strategies in isolation.
In addition, it is important to identify mechanisms that may underlie gender and racial/ethnic differences in coping and depressive symptomatology in adolescence. As discussed, differences have been found in coping preferences and symptoms of depression based on gender and race/ethnicity, and gender or race/ethnic differences in coping may contribute to corresponding differences in symptoms of depression. For instance, girls tend to utilize their social support networks more often than boys, which may protect girls from developing increased symptoms of depression. As such, the use of social support to cope with a stressor may mediate the gender difference in depressive symptoms. Some evidence suggests that using spirituality to cope may be more common among minority adolescents in comparison to Caucasian adolescents (Molock & Barksdale, 2013; Plucker, 1998). As such, religious coping may be a mechanism that drives racial/ethnic differences in symptoms of depression. In sum, the examination of coping as a mediator in the relationship between gender and depressive symptoms during adolescence has been relatively unexplored. Moreover, the mediating role that coping may play in the relationship between race/ethnicity and symptoms of depression during adolescence has yet to be examined.
The Present Study
The present study was designed to examine gender and race/ethnicity differences in coping and depression, and their relations over time. In order to address conflicting results regarding coping, a specific strategy approach was used, rather than a dimensional approach. This approach was deemed necessary because some strategies may map onto multiple dimensions (i.e. emotional social support is both problem- and emotion-focused) and dimensions may encapsulate both adaptive and maladaptive strategies. A more nuanced and detailed approach may help to clarify gender and racial differences in coping, as well as which coping strategies are particularly related to symptoms of depression during adolescence. It is important to note that relatively few studies have examined multiple coping strategies simultaneously, which is problematic given that adolescents may be flexible and use many coping strategies (Cicognani, 2011). By examining many coping strategies at the same time, unique effects of specific coping strategies, controlling for use of other strategies, may be identified. Also of note, when racial/ethnic differences in coping and depressive symptoms have been examined, most studies have included only Caucasian and African-American adolescents, or Hispanic adolescents alone. Studying these groups in isolation makes group comparisons difficult, and may mask important differences between groups. Finally, the potential mediating role that coping may play in the relationships between gender and depressive symptomatology and race/ethnicity and depressive symptomatology has yet to be systematically examined and may shed light on the etiology of depression across different groups of youth.
Given the limitations of the current literature, the present study addressed the following research questions using a large, diverse, longitudinal sample of adolescents
Do coping strategies differ by gender and/or race/ethnicity during adolescence? We used cross-sectional comparisons of Time 1 data to attempt to replicate the findings that girls would endorse more instrumental and emotional support coping than boys, whereas boys would endorse more active coping than girls. We also anticipated that girls may be more likely to use denial and religious coping compared with boys, given the unique stressors that girls face during adolescence. We expected that boys may be more likely to use humor and planning compared with girls, given that these are “active” strategies. Regarding race/ethnic differences, based on the current literature, we anticipated that African-American and Hispanic adolescents would use social support and religious coping more often than Caucasian adolescents. We also hypothesized that African-American and Hispanic adolescents may utilize a more complex profile of coping strategies overall compared with their Caucasian counterparts.
Does depressive symptomatology differ by gender and/or race/ethnicity during adolescence? Based on the existing literature, we expected girls to have higher depressive symptomatology scores than boys, and African-American and Hispanic adolescents to have higher depressive symptomatology scores than Caucasians adolescents. We tested this hypothesis with our cross sectional data.
Does coping mediate the longitudinal relationship between gender and depressive symptomatology during adolescence? Specifically, we hypothesized that boys would be more likely than girls to use active coping and, in turn, that more active coping would be associated with lower symptoms of depression a year later. We also anticipated that girls would be more likely than boys to use social support, and that this would buffer against depressive symptoms for girls specifically. We included other, less well-studied coping strategies such as religious coping and denial, as mediators in an exploratory fashion.
Does coping mediate the longitudinal relationship between race/ethnicity and depressive symptomatology during adolescence? We hypothesized that minority adolescents would be more likely than Caucasians to use religious coping and social support seeking, and that these strategies would specifically protect these youth from developing symptoms of depression. We also speculated that minority youth may be more likely than Caucasians to use denial, and that denial would be associated with increased depressive symptoms. In addition, we examined the mediating role of other coping strategies, such as humor, in an exploratory manner.
Method
Participants
The sample for this study was drawn from a larger study, the Adolescent Adjustment Project (AAP; Ohannessian, 2009). During the spring of 2007 (Time 1), 10th and 11th grade students from public high schools in the Mid-Atlantic region of the U.S. were invited to participate in the study. The participants were followed up during the spring of 2008 (Time 2) and the spring of 2009 (Time 3).
At Time 1, the sample included 905 15-17 year old adolescents (54% girls, n = 485) enrolled in seven public high schools in Delaware, Maryland, or Pennsylvania. Two of the schools were located in urban areas, three in suburban areas, and two schools were rural. The mean age of participants was 16.10 (SD = .67). The racial/ethnic composition of the sample was 63% Caucasian (n = 571), 24% African-American (n = 219), and 13% Hispanic (n = 115). About half of adolescents reported living with both biological parents (54%, n = 488). The sample consisted mostly of working and middle class families. The majority of the adolescents' parents had completed high school only (37% of fathers, 35% of mothers). A smaller percentage of parents had completed two years of college (16% of fathers, 17% of mothers), or four years of college (20% of fathers, 23% of mothers). A minority of the parents had completed less than high school (4% of both fathers and mothers) or graduate/medical school (6% of fathers, 9% of mothers).
Measures
Participating students were administered a self-report survey. The measures included in the survey relevant to this study are described below.
Coping
Students completed the 60 item COPE Inventory (Carver et al.,1989) to assess general coping preferences. The COPE has been shown to be psychometrically sound (Carver et al., 1989) and to have good internal reliability (Phelps & Jarvis, 1994). The following scales were included in this study: Venting emotions (“I get upset and let my emotions out”), instrumental social support (“I try to get advice from someone about what to do”), active coping (“I concentrate my efforts on doing something about it”), denial (“I say to myself ‘this isn't real’”), religious coping (“I put my trust in God”), humor (“I laugh about the situation”), emotional social support (“I discuss my feelings with someone”) and planning (“I make a plan of action”). Participants responded to the items using a response scale ranging from 1 = don't do this at all to 4 = do this a lot. Cronbach's alphas for the COPE scales in our sample ranged from .75-.90.
Depressive symptoms
Depressive symptomatology was assessed using the Center for Epidemiologic Studies Depression Scale for Children (CES-DC; Weissman, Orvaschell, & Padian, 1980). The CES-DC includes 20 items rated on a 4-point Likert scale ranging from 1 = not at all to 4 = a lot, based on the past week. A sample item is “I felt sad.” A total score was created by summing all items, with higher scores indicating higher depressive symptomatology.
Previous studies have found the CES-DC to be psychometrically sound for use with adolescents (Faulstich, Carey, Ruggiero, Enyart, & Gresham, 1986; Ohannessian, Lerner, Lerner, & von Eye, 1999). The Cronbach's alpha coefficient for the CES-DC in our sample was .90.
Procedures
High schools in urban, suburban, and rural areas of Delaware, Maryland, and Pennsylvania were invited to participate in this study. The principals of seven high schools agreed to have their school participate. Consent forms were sent home to the parents of 10th and 11th grade students early in 2007. Students also were given assent forms to complete at school prior to participation in the study. Forty-five adolescents declined to participate. Only those students with both parental consent and adolescent assent participated in the study. In total, 71% percent of eligible students participated. Most of the non-participating students were absent on the day of data collection.
Prior to participation, the students were assured that all data collected were confidential, participation was voluntary, and that they could withdraw from the study at any time. In addition, the students were informed that an active Certificate of Confidentiality from the U.S. Government was in place to protect their privacy. The students were told that they were “invited to participate in a research study that will look at what kinds of things (for example, involvement in extracurricular activities, coping abilities) may protect some adolescents from developing problems (such as depression, anxiety, and alcohol/drug abuse).” Study participants completed a self-report survey administered by trained research personnel (all certified with human subjects training) during regular school hours. The survey took approximately 40 minutes to complete. Upon completion of the survey, participants were compensated with a movie pass. Those students who were absent were given the opportunity to complete the survey at home and to return it in a prepaid envelope by mail.
All students who participated at Time 1 were invited to participate again in the spring of 2008 (Time 2) and again in the spring of 2009 (Time 3). The protocol at Time 2 and Time 3 was identical to the Time 1 protocol except that at Time 3, participants who had graduated from high school completed the survey online. Twenty percent of the youth participating at Time 1 did not participate at subsequent waves. Girls were more likely than boys, and Caucasian adolescents were more likely than African-American or Hispanic adolescents, to participate in all three waves of data collection (p < .001 in each comparison). However, the longitudinal and non-longitudinal subsamples did not differ on any other variable of interest.
Results
Does Coping Differ by Gender and/or Race/Ethnicity during Adolescence?
A Multivariate Analysis of Variance (MANOVA) model was conducted to examine whether coping strategies differ by gender and/or race/ethnicity. The design factors in this model were gender and race/ethnicity and the dependent variables were coping strategies (all assessed at Time 1). Results of the MANOVA are presented in Table 1. Significant gender effects were found for emotional social support [F(1, 496) = 35.62; p < .001], instrumental social support [F(1, 496) = 16.98; p < .001], and venting emotions [F(1, 496) = 47.64; p < .001], such that girls were more likely to report the use of these coping strategies than were boys.
Table 1. Means and Confidence Intervals for the Coping Strategies and Symptoms of Depression at Time 1 by Gender and Race/Ethnicity.
| Variable | Boys | Girls | F-Ratio from ANOVA |
Significant Post- Hoc Differences |
||||
|---|---|---|---|---|---|---|---|---|
|
|
|
|||||||
| Caucasian M (95% CI) |
African-American M (95% CI) |
Hispanic M (95% CI) |
Caucasian M (95% CI) |
African-American M (95% CI) |
Hispanic M (95% CI) |
|||
| Active Coping | 8.73(8.28-9.18) | 9.63(8.53-10.73) | 8.80(7.53-10.07) | 9.63(9.24-10.04) | 9.42(8.68-10.15) | 10.03(9.05-11.01) | ||
| Denial Coping | 5.84(5.43-6.25) | 6.93(5.93-7.92) | 6.00(4.84-7.16) | 6.55(6.19-6.92) | 5.65(4.98-6.32) | 7.47(6.58-8.34) | 5.38** | Caucasian Boys<Caucasian Girls; African-American Girls<African-American Boys |
| Emotional Support Coping | 7.99(7.50-8.48) | 8.70(7.51-9.90) | 8.70(7.31-10.09) | 11.23(10.79-11.67) | 10.42(9.62-11.22) | 10.91(9.85-11.98) | 35.62*** | Boys < Girls |
| Humor Coping | 9.51(8.96-10.05) | 8.63(7.30-9.96) | 8.70(7.16-10.24) | 8.99(8.50-9.48) | 7.88(6.99-8.77) | 8.79(7.61-9.98) | ||
| Instrumental Support Coping | 8.36(7.88-8.84) | 9.15(7.98-10.31) | 9.10(7.75-10.45) | 10.95(10.52-11.37) | 9.98(9.20-10.76) | 10.50(9.46-11.54) | 16.98*** | Boys < Girls |
| Planning Coping | 9.05(8.56-9.54) | 9.70(8.52-10.89) | 8.75(7.38-10.13) | 9.47(9.04-9.91) | 9.85(9.06-10.64) | 9.71(8.65-10.76) | ||
| Religious Coping | 7.36(6.77-7.94) | 11.56(10.13-12.98) | 8.40(6.74-10.06) | 8.59(8.06-9.11) | 11.30(10.34-12.26) | 9.15(7.88-10.42) | 25.89*** | African-American > Caucasian, Hispanic |
| Venting Emotions Coping | 6.79(6.32-7.26) | 7.74(6.60-8.89) | 6.90(5.57-8.23) | 10.10(9.68-10.52) | 9.92(9.15-10.68) | 9.35(8.33-10.37) | 47.64*** | Boys < Girls |
| Depression | 33.27(31.58-34.95) | 32.46(28.64-36.27) | 34.92(30.63-39.22) | 37.44(35.92-38.96) | 36.38(33.82-38.95) | 38.71(35.01-42.42) | 9.34*** | Boys < Girls |
Note: All coping variables have a range from 4-16. Depression measured using the CES-DC ranges from 0-60. Time 1 variables are presented. The time 1 n=905.
p < .10
p < .05
p< .01
p< .001
As shown in Table 1, a significant main effect for race/ethnicity was found for religious coping [F(2, 496) = 25.89; p < .001]. Follow up testing using Tukey's Honestly Significant Difference method revealed that African-American adolescents were more likely to use religious coping than both Caucasian adolescents and Hispanic adolescents (p < .001 for both contrasts). There also was a significant gender × race/ethnicity interaction in the use of denial coping [F(2, 496) = 5.38; p < .01]. Follow up analyses indicated that Caucasian girls used more denial coping than did Caucasian boys; and African-American boys used more denial coping than African-American girls. Among Hispanic youth, there was no significant difference between girls' and boys' use of denial coping. This interaction also was evident in the racial/ethnic differences observed for boys and girls. For boys, there was a significant difference such that African-American boys reported using more denial coping than Caucasian boys. For girls, a different pattern emerged such that Hispanic girls reported engaging in significantly more denial coping than African-American girls.
Does Depressive Symptomatology Differ by Gender and/or Race/Ethnicity during Adolescence?
A factorial Analysis of Variance (ANOVA) model was conducted to examine whether depressive symptomatology differed by gender and/or race/ethnicity at baseline (Time 1). The design factors for this analysis were gender and race/ethnicity and the dependent variable was depressive symptomatology. As shown in Table 1, a significant main effect for gender was found, indicating that girls reported more symptoms of depression than boys [F(1, 910) = 13.78, p < .001]. However, no association was found between race/ethnicity and depressive symptomatology. There also was no gender × race/ethnicity interaction.
Does Coping Mediate the Relationships between Gender and Depressive Symptomatology and Race/Ethnicity and Depressive Symptomatology during Adolescence?
Path Analysis was used to examine the longitudinal relations between gender and race/ethnicity at Time 1, coping at Time 2, and depressive symptomatology at Time 3, and to test whether coping strategies mediated the relationship between gender and depressive symptomatology or race/ethnicity and depressive symptomatology. The path models included pathways between gender or race/ethnicity and depressive symptomatology, gender or race/ethnicity and all of the coping strategies, and all of the coping strategies and depressive symptomatology. Depressive symptomatology at Time 1 was included as a covariate in the model. Because results from a factorial ANOVA revealed a significant difference in the levels of parent education between the racial/ethnic groups [F(2, 746) = 37.60, p < .001], parent education (a proxy variable for SES) at Time 1 was also included as covariate in the model. In addition, the disturbance terms of the endogenous variables were allowed to correlate. These correlations were included because there is theoretical rationale to assume that the disturbance terms of coping strategies could be related to each other through an underlying coping factor. Finally, the Sobel test was used to determine whether the coping strategies significantly mediated the relationship between gender and/or race/ethnicity and depressive symptoms one year later. Of note, the Sobel test calculates whether the addition of the mediator explains a significant amount of variance in the outcome and decreases the direct path from something significant to a value of either 0 (total mediation), or a significantly lower number (partial mediation). The Sobel test works well with large samples and allows for missing data (Baron & Kenny, 1986). All of the path analyses were conducted with AMOS 22.0.
Gender and depressive symptomatology: The mediating influence of coping
The model fit the data well (X2(19) = 120.33, p <.001; NFI = .97; CFI = .97; RMSEA = .06). As shown in Figure 1, gender significantly predicted venting emotions (β = .40, p <.001), instrumental social support (β = .31, p <.001), active coping (β = .14, p <.001), religious coping (β = .17, p <.001), emotional social support (β = .37, p <.001), and planning (β = .14, p<.001), such that girls reported using these coping strategies more than boys (boys were coded as 0, girls were coded as 1). In turn, venting emotions, instrumental social support, and humor significantly predicted depressive symptomatology (βs = .16, p <.05; -.24, p <.05; and -.12, p <.05, respectively). Of the control variables included, only baseline depressive symptomatology had a significant effect on later depressive symptomatology (β = .31, p<.001).
Figure 1.
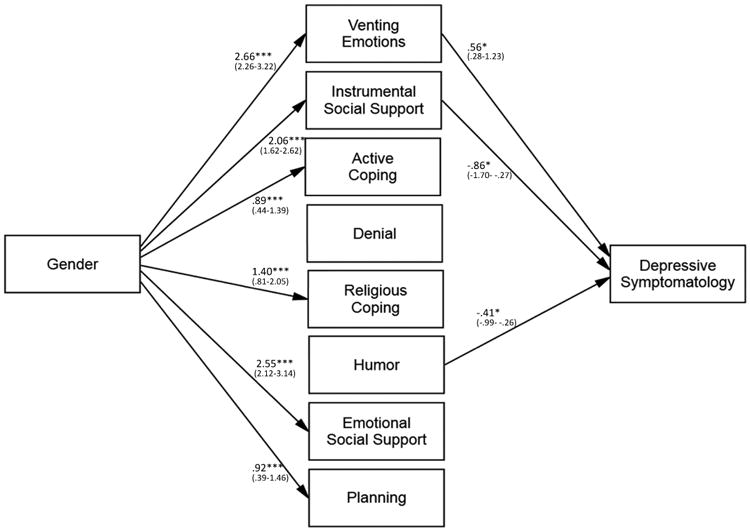
Pathways from gender at Time 1 to coping strategies at Time 2 and depressive symptomatology at Time 3. (Note. Unstandardized regression coefficients are presented with 95% confidence intervals below. For ease of interpretation, only significant paths are shown. n = 905.)
Sobel test results indicated that the relationship between gender and adolescent depressive symptomatology was significantly mediated by venting emotions (c.r. = 3.08, p<.01). This finding indicated that girls were more likely to use venting emotions than boys and, in turn, venting emotions increased depressive symptomatology. The relationship between gender and depressive symptomatology also was significantly mediated by instrumental social support (c.r. = -2.40, p<.05). These results indicated that girls were more likely to use instrumental social support than boys and that, in turn, instrumental social support was associated with decreased depressive symptomatology.
Race/ethnicity and depressive symptomatology: The mediating influence of coping
Three sets of path analysis models were conducted to examine whether coping mediates the relationship between race/ethnicity and depressive symptomatology. The first set contrasted Caucasian adolescents (coded as 0) with African-American adolescents (coded as 1), the second set contrasted Caucasian adolescents (coded as 0) with Hispanic adolescents (coded as 1), and the third set contrasted African-American adolescents (coded as 0) with Hispanic adolescents (coded as 1).
In the analyses contrasting Caucasian and African-American adolescents, the model fit the data quite well (X2(19) = 104.41, p < .001; NFI = .97; CFI = .98; RMSEA = .06). As shown in Figure 2, race/ethnicity significantly predicted venting emotions (β = .11, p<01), active coping (β = .09, p<05), denial (β = 20, p<001), religious coping (β = .36, p <.001), and planning (β = .09, p <.05), indicating that African-American adolescents were more likely to use venting emotions, active coping, denial, religious coping, and planning in comparison to Caucasian adolescents. In addition, similar to the models examining gender, venting emotions, instrumental social support, and humor significantly predicted depressive symptomatology (βs = .16, p <.05; -.24, p <.05; and -.12, p <.05, respectively). Of the control variables included, again only baseline depressive symptomatology had a significant effect on later depressive symptomatology (β = .32, p <.001). Sobel tests indicated that venting emotions was not a significant mediator between race/ethnicity and depressive symptomatology.
Figure 2.
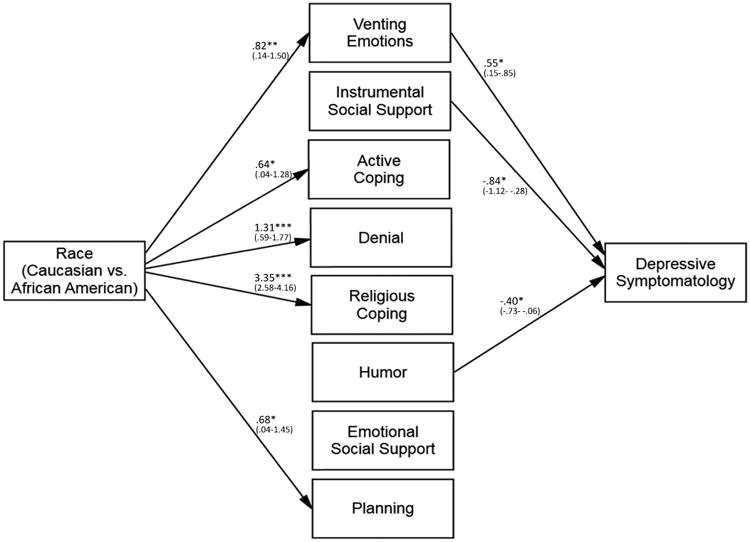
Pathways from race/ethnicity (Caucasian vs. African-American) at Time 1 to coping strategies at Time 2 and depressive symptomatology at Time 3. (Note. Unstandardized regression coefficients are presented with 95% confidence intervals below. For ease of interpretation, only significant paths are shown. n = 905.)
In the analyses contrasting Caucasian and Hispanic adolescents, the model also fit the data quite well (X2(19) = 153.17, p < .001; NFI = .96; CFI = .96; RMSEA = .07). As shown in Figure 3, race/ethnicity significantly predicted denial (β = . 12, p <.01), and humor (β = -.10, p <.05), indicating that Hispanic adolescents were more likely to use denial when coping in comparison to Caucasian adolescents, but that Caucasian adolescents were more likely to use humor when coping than were Hispanic adolescents. Similar to the prior models examining gender and race/ethnicity, venting emotions, instrumental social support, and humor significantly predicted depressive symptomatology (βs = .16, p<.05; -.24, p<.05; and -.13. p <.05, respectively). Baseline depressive symptomatology also had a significant effect on later depressive symptomatology (β = .31, p <.001). A Sobel test was conducted to examine whether humor significantly mediated the relationship between race/ethnicity and depressive symptomatology. Results indicated that humor was not a significant mediator.
Figure 3.
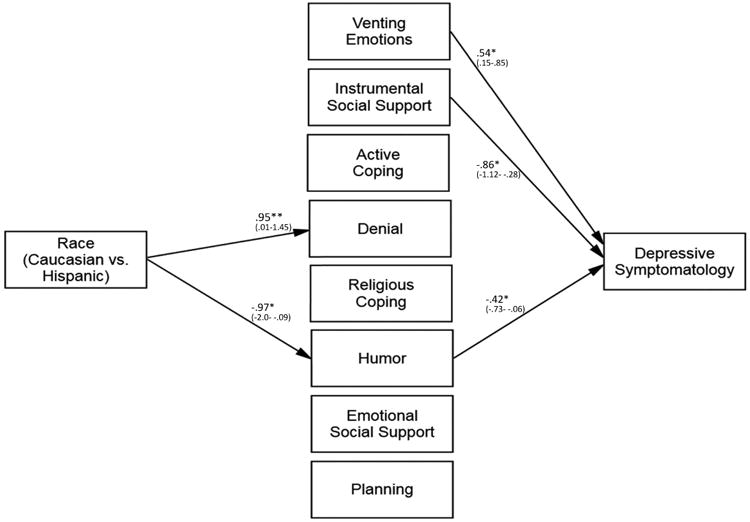
Pathways from race/ethnicity (Caucasian vs. Hispanic) at Time 1 to coping strategies at Time 2 and depressive symptomatology at Time 3. (Note. Unstandardized regression coefficients are presented with 95% confidence intervals below. For ease of interpretation, only significant paths are shown. n = 905.)
In the analyses contrasting African-American and Hispanic adolescents, the model also fit the data quite well (X2(19) = 157.24, p < .001; NFI = .96; CFI = .96; RMSEA = .07). As shown in Figure 4, race/ethnicity significantly predicted active coping (β = -.19, p <.01), religious coping (β = -.39, p <.001), humor (β = -.16, p<.05), and planning (β = -.15, p <.05), indicating that African-American adolescents were more likely to use active coping, religious coping, humor and planning than Hispanic adolescents. Similar to the prior models examining gender and race/ethnicity, venting emotions, instrumental social support, and humor significantly predicted depressive symptomatology (βs = .15, p<.05; -.23, p<.05; and -.13, p <.05, respectively). Of the control variables included, again only baseline depressive symptomatology had a significant effect on later depressive symptomatology (β = .32, p<.001). A Sobel test indicated that humor did not significantly mediate the relationship between race/ethnicity and depressive symptomatology.
Figure 4.
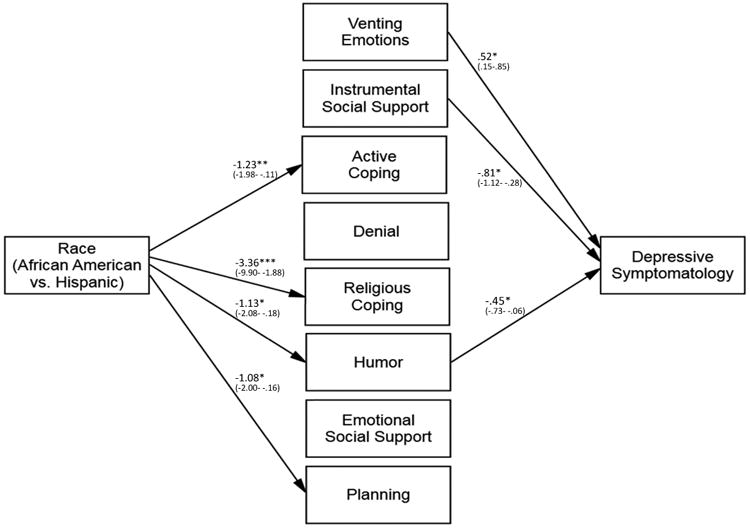
Pathways from race/ethnicity (African-American vs. Hispanic) at Time 1 to coping strategies at Time 2 and depressive symptomatology at Time 3. (Note. Unstandardized regression coefficients are presented with 95% confidence intervals below. For ease of interpretation, only significant paths are shown. n = 905.)
Discussion
Given the prevalence of depressive symptoms in adolescence (Balázs et al., 2013), it is important to study the frequency and effectiveness of coping mechanisms in this age group. Although there is a large literature on coping, there is debate about the best way to classify various coping strategies, evidenced by the many different approaches that have been used to identify factors (e.g., Ayers et al., 1996; Connor-Smith et al., 2000; Walker et al., 1997). Therefore, the current study assessed differential relations between eight coping strategies and symptoms of depression during adolescence. Differences in reported use of each of the eight coping strategies between boys and girls, and Caucasian, African-American, and Hispanic adolescents were examined first, as the literature suggests that there are both gender and racial/ethnic differences in coping during adolescence (e.g., Chapman & Mullis, 2000; Eschenbeck et al., 2007; Li et al., 2006). This approach allowed for an examination of gender and racial/ethnic differences in coping mechanisms that are less well studied in adolescence, such as humor and denial. Differences in depressive symptoms also were examined, and the current study went a step beyond that to examine how differences in the use of coping strategies may mediate the relationship between gender and depressive symptoms, and race/ethnicity and depressive symptoms.
A primary aim of the present study was to clarify how coping varies by gender and race/ethnicity during adolescence. The results from this study regarding gender differences in coping were fairly consistent with the literature. Girls endorsed more frequent use of many coping strategies in comparison to boys. More specifically, gender differences were observed for instrumental and emotional social support (e.g., Eschenbeck et al., 2007), with girls endorsing more frequent use of these strategies than boys. In contrast to the literature (e.g., Kort-Butler, 2009), in the present study, girls were found to use more venting of emotion, active coping, and planning than boys. Girls also were more likely to use religious coping in comparison to boys. Although somewhat surprising, these findings are consistent with the idea that girls endorse a broader repertoire of coping strategies than do boys and use those strategies more frequently (Cicognani, 2011). Flexibility in coping may be particularly important for girls given that girls experience more stressors than boys during adolescence, often simultaneously (Hankin, Abramson, Miller, & Haeffel, 2004).
Discrepancies in findings across studies may be due to differences in the assessment of coping. Indeed, some of the cited studies used a dimensional approach (e.g., Eschenbeck et al., 2007; Kort-Butler, 2009), whereas our study examined individual coping strategies. Furthermore, there was no standard measure of coping used across studies; a variety of measures such as the COPE (Carver et al., 1989), the A-COPE (Patterson & McCubbin, 1987), and the Adolescent Coping Scale (Frydenberg & Lewis, 1993) were used. Thus, it is difficult to rule out whether differences across studies simply are artifacts due to measurement differences.
Consistent with the literature (Chapman & Mullis, 2000; Molock & Barksdale, 2013; Plucker, 1998), when race/ethnicity differences in coping were examined, African-American adolescents were more likely to engage in religious coping compared to Caucasian and Hispanic adolescents. These findings make sense in light of the perceived uncontrollability of stressors facing many minority adolescents (e.g., discrimination), and the observation that individuals attempt to match coping strategies with the stressor (Compas, 1987). There also is literature to suggest that religiosity and spirituality are especially common in African American cultures (Cauce et al., 2002), and therefore it would be expected that African American youth would rely on religion as a coping strategy relatively more than other racial groups.
An interaction between gender and ethnicity also was observed, such that Hispanic girls engaged in denial coping significantly more than African-American girls, with Caucasian girls scoring between the two. In contrast, among boys, African-American boys reported the highest use of denial coping, significantly more than Caucasian boys, with Hispanic boys scoring between the two. It is unclear why Hispanic girls and African-American boys rely on denial coping more than their counterparts. In line with the literature cited previously, perhaps African-American boys and Hispanic girls feel the least in control of the stressors in their life and consequently resort to denial coping. Some research suggests that when social constraints are present, effective coping strategies may be limited. For example, in a study focusing on adults with cancer, conducted by Merluzzi, Philip, Zhang, and Sullivan (2014), the authors suggest that there are social constraints that limit the options in coping strategies available to African-Americans to a point where they resort to being disengaged, and use less active coping than their Caucasian counterparts. Further research is needed to systematically explore the interaction between race/ethnicity and gender on the use of denial.
In terms of depressive symptomatology, this study replicated previous findings of girls endorsing more symptoms of depression than boys (e.g., Kort-Butler, 2009). However, racial/ethnic differences in depressive symptoms were not observed. The literature has been mixed on this subject, but the results of this study are consistent with some other studies that have not found differences in depression based on race/ethnicity (e.g., Maag & Irvin, 2005). Of note, the present study extends this research by including Hispanic adolescents, as well as African-American adolescents.
Another primary goal of the present study was to examine whether coping mediates the relationship between gender and adolescent depressive symptomatology. Venting emotions and instrumental social support both significantly mediated the relationship between gender and depressive symptomatology. More specifically, girls were more likely than boys to vent emotions to cope, which in turn predicted more depressive symptoms a year later. On the other hand, girls also were more likely than boys to use instrumental social support, which in turn, predicted fewer symptoms of depression a year later. Both of these socially oriented coping strategies predicted depressive symptoms in opposite directions: venting emotions led to more symptoms, whereas instrumental social support coping led to fewer symptoms. Therefore, it appears that the context in which the person engages others in their coping is important in determining whether the strategy is adaptive or maladaptive. Seeking social support from others may help to comfort the adolescent and bolster confidence. In contrast, venting to others may actually exacerbate negative emotions by activating negative thoughts and behaviors (via cognitive neoassociation; Berkowitz, 1990).
This study also sought to examine whether coping mediates the relationship between race/ethnicity and depressive symptomatology during adolescence. In the present study, there were no instances of mediation. Nonetheless, significant indirect paths were observed. For instance, in the model comparing Caucasian adolescents to African-American adolescents, a difference was observed such that African American adolescents reported venting their emotions more than Caucasian adolescents. In turn, using venting emotions as a coping strategy was related to higher levels of depressive symptoms the following year.
From these models, it is clear that African American youth engaged in more varied coping strategies than Caucasian youth across time (for instance, venting emotion, active coping, denial, religious coping, and planning). This broader repertoire of coping strategies may be required due to the increased stressors faced by African American youth, especially those from the inner city. Of the schools that were included in this study, 85 percent of the youth attending the schools located in inner cities were minority youth. African American adolescents in this study were likely to live in the inner city and, therefore, had to deal with the accompanying stressors, such as greater exposure to poverty, crime, gangs, and access to drugs (Ohannessian, 2014). It also is important to note that while adolescence may be a stressful time for youth due to the numerous developments and changes that take place in a short amount of time (Hollenstein & Lougheed, 2013; Smetana, Campione-Barr, & Metzger, 2006), this developmental period may be especially stressful for African American youth living in inner cities, as there is evidence to suggest that the transition between childhood and adulthood is even more brief for this group because many of these youth are required to adopt adult roles relatively early (Burton, Obeidallah, & Allison, 1996; Cauce et al., 2002). Such additional responsibilities may make adolescence even more stressful for these youth, demanding the use of more varied coping strategies.
In addition, in both of the models comparing Hispanic adolescents to Caucasian adolescents and to African-American adolescents, Hispanic adolescents reported using humor as a coping strategy less often than both other groups. In turn, lower levels of humor predicted more depressive symptomatology one year later. As such, interventions targeting depression for Hispanic youth in particular should emphasize the use of humor as a potential coping strategy.
Of note, results from the present study suggest that Hispanic youth do not engage in a broader repertoire of coping strategies than the other racial/ethnic groups, despite their minority status. Perhaps the central role that the family typically plays in Hispanic cultures, referred to as familism (Parra-Cardona, Bulock, Imig, Villarruel, & Gold, 2006), protects Hispanic youth from exposure to stressors and offers additional support, allowing these youth to rely less on other coping strategies.
The present study contributes to the literature in a number of respects; however, limitations of the current study should be noted. The measures used in this study all were self-report in nature, which may have increased the likelihood of biased responding. Although adolescents are the most accurate reporters of their own behaviors (Deković et al., 2006), it would be useful to replicate these findings with other methodologies (e.g., parent and teacher reports, clinical interviews). It also is important to note that this study did not collect information about the participants' countries of origin. Future studies should aim to collect more detailed information concerning race/ethnicity, as youth who identify as minority (e.g., Hispanic) may differ from each other based on their country of origin.
Despite these limitations, the present study was unique in several ways, and strengths of the study deserve consideration. The coping measure used in this study assessed numerous coping strategies, some of which are underrepresented in the literature (i.e., humor, religion), allowing for a comprehensive analysis of coping. Moreover, the use of path analysis allowed for the examination of the influence of these coping strategies on depressive symptomatology simultaneously. The large, diverse sample also allowed us to examine the three largest racial/ethnic groups in the U.S., individually and in comparison to one another. Finally, the longitudinal nature of the study allowed for the examination of the relationship between coping and symptoms of depression over time.
In summary, the results of this study shed light on gender and racial/ethnic differences in both coping and depressive symptomatology during adolescence. We replicated results that girls experience more dysphoria than boys (e.g., Kort-Butler, 2009), but did not find support for race/ethnicity differences in symptoms of depression (e.g., Maag & Irvin, 2005). We also found support for more complexity and flexibility in girls' coping repertoires compared with boys' (Cicognani, 2011), and more religious coping in African-American youth compared with either Caucasian or Hispanic youth (Chapman & Mullis, 2000; Plucker, 1998). Importantly, our study added to the current literature by presenting evidence that coping (venting emotions and instrumental social support) also mediates the relationship between gender and depressive symptomatology during adolescence.
The present study contributes to the extant literature by examining the mediating role that coping may play in the relationships between gender and depressive symptomatology and race/ethnicity and depressive symptomatology, over time, during adolescence. Of note, although research has shown that gender and race/ethnicity are associated with depression during adolescence, few studies have examined the underlying mechanisms involved in these relationships. Moreover, only a handful of studies have examined multiple coping strategies simultaneously, and those that have typically have not considered gender or race/ethnicity. It also should be noted that when racial/ethnic differences in coping and depressive symptoms have been examined, most studies have included only Caucasian and African-American adolescents (Hispanic adolescents have been overlooked). Results from this study underscore the importance that coping strategies may play in the development of depression during adolescence. The findings also point to specific coping strategies (e.g., instrumental social support and humor) that should be targeted to prevent depression as adolescents negotiate the numerous changes and stressors inherent to this sometimes challenging developmental period.
Acknowledgments
This research was supported by grant 5K01A015059 to Christine McCauley Ohannessian from the National Institutes of Health. The involvement of all of the students who participated in the study is greatly appreciated. Special thanks go to members of the project staff, especially Magdalena Owczarska, Kelly Cheeseman, Lisa Fong, Alyson Cavanaugh, Jessica Schulz, Laura Finan, Sara Bergamo, Juliet Bradley, and Ashley Ings.
Contributor Information
Ashley M. Malooly, University of Miami
Kaitlin M. Flannery, University of Connecticut
Christine McCauley Ohannessian, Children's Center for Community Research, Connecticut Children's Medical Center, University of Connecticut School of Medicine
References
- Aldridge AA, Roesch SC. Developing coping typologies of minority adolescents: A latent profile analysis. Journal of Adolescence. 2008;31:499–517. doi: 10.1016/j.adolescence.2007.08.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ayers TS, Sandler IN, West SG, Roosa MW. A dispositional and situational assessment of children's coping: Testing alternative models of coping. Journal of Personality. 1996;64(4):923–958. doi: 10.1111/j.1467-6494.1996.tb00949.x. [DOI] [PubMed] [Google Scholar]
- Balázs J, Miklósi M, Keresztény Á, Hoven CW, Carli V, Wasserman C, et al. Wasserman D. Adolescent subthreshold-depression and anxiety: Psychopathology, functional impairment and increased suicide risk. Journal Of Child Psychology And Psychiatry. 2013;54(6):670–677. doi: 10.1111/jcpp.12016. [DOI] [PubMed] [Google Scholar]
- Baron RM, Kenny DA. The moderator-mediator variable distinction in social psychological research: Conceptual, strategic, and statistical considerations. Journal of Personality and Social Psychology. 1986;51:1173–1182. doi: 10.1037//0022-3514.51.6.1173. [DOI] [PubMed] [Google Scholar]
- Beardslee WR, Gladstone TRG. Prevention of childhood depression: Recent findings and future prospects. Biological Psychiatry. 2001;49(12):1101–1110. doi: 10.1016/s0006-3223(01)01126-x. [DOI] [PubMed] [Google Scholar]
- Berkowitz L. On the formation and regulation of anger and aggression: A cognitive-neoassociationistic analysis. American Psychologist. 1990;45(4):494–503. doi: 10.1037//0003-066x.45.4.494. [DOI] [PubMed] [Google Scholar]
- Burton LM, Obeidallah DA, Allison K. Ethnographic insights on social context and adolescent development among inner-city African-American teens. In: Jessor R, Colby A, editors. Ethnography and Human Development: Context and Meaning in Social Inquiry. Chicago, IL: The University of Chicago Press; 1996. pp. 395–418. [Google Scholar]
- Cairns KE, Yap MH, Pilkington PD, Jorm AF. Risk and protective factors for depression that adolescents can modify: A systematic review and meta-analysis of longitudinal studies. Journal of Affective Disorders. 2014;169:61–75. doi: 10.1016/j.jad.2014.08.006. [DOI] [PubMed] [Google Scholar]
- Carleton RA, Esparza P, Thaxter PJ, Grant KE. Stress, religious coping resources, and depressive symptoms in an urban adolescent sample. Journal for the Scientific Study of Religion. 2008;47(1):113–121. [Google Scholar]
- Carpenter TP, Laney T, Mezulis A. Religious coping, stress, and depressive symptoms among adolescents: A prospective study. Psychology of Religion and Spirituality. 2012;4(1):19–30. [Google Scholar]
- Carver CS, Scheier MF, Weintraub JK. Assessing coping strategies: A theoretically based approach. Journal of Personality and Social Psychology. 1989;56:267–283. doi: 10.1037//0022-3514.56.2.267. [DOI] [PubMed] [Google Scholar]
- Cauce AM, Domenech-Rodríguez M, Paradise M, Cochran BN, Shea JM, Srebnik D, Baydar N. Cultural and contextual influences in mental health help seeking: A focus on ethnic minority youth. Journal of Consulting and Clinical Psychology. 2002;70(1):44. doi: 10.1037//0022-006x.70.1.44. [DOI] [PubMed] [Google Scholar]
- Chapman PL, Mullis RL. Racial/ethnic differences in adolescent coping and self-esteem. Journal of Genetic Psychology. 2000;161(2):152–160. doi: 10.1080/00221320009596702. [DOI] [PubMed] [Google Scholar]
- Cicognani E. Coping strategies with minor stressors in adolescence: Relationships with social support, self-efficacy, and psychological well-being. Journal of Applied Social Psychology. 2011;41(3):559–578. [Google Scholar]
- Compas BE. Coping with stress during childhood and adolescence. Psychological Bulletin. 1987;101(3):393–403. [PubMed] [Google Scholar]
- Connor-Smith JK, Compas BE, Wadsworth ME, Thomsen AH, Saltzman H. Responses to stress in adolescence: Measurement of coping and involuntary stress responses. Journal of Consulting and Clinical Psychology. 2000;68(2):976–996. [PubMed] [Google Scholar]
- Costello JE, Erkanli A, Angold A. Is there an epidemic of child or adolescent depression? Journal of Child Psychology and Psychiatry. 2006;47(12):1263–1271. doi: 10.1111/j.1469-7610.2006.01682.x. [DOI] [PubMed] [Google Scholar]
- Davis SK, Humphrey N. The influence of emotional intelligence (EI) on coping and mental health in adolescence: Divergent roles for trait and ability EI. Journal of Adolescence. 2012;35(5):1369–1379. doi: 10.1016/j.adolescence.2012.05.007. [DOI] [PubMed] [Google Scholar]
- Deković M, ten Have M, Vollebergh WM, Pels T, Oosterwegel A, Wissink IB, et al. Ormel J. The cross-cultural equivalence of parental rearing measure: EMBU-C. European Journal of Psychological Assessment. 2006;22:85–91. [Google Scholar]
- Dew RE, Daniel SS, Armstrong TD, Goldston DB, Triplett MF, Koenig HG. Religion/spirituality and adolescent psychiatric symptoms: A review. Child Psychiatry & Human Development. 2008;39(4):381–398. doi: 10.1007/s10578-007-0093-2. [DOI] [PubMed] [Google Scholar]
- Dunbar JP, McKee L, Rakow A, Watson KH, Forehand R, Compas BE. Coping, negative cognitive style and depressive symptoms in children of depressed parents. Cognitive Therapy and Research. 2013;37:18–28. doi: 10.1007/s10608-012-9437-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eschenbeck H, Kohlmann C, Lohaus A. Gender differences in coping strategies in children and adolescents. Journal of Individual Differences. 2007;28(1):18–26. [Google Scholar]
- Faulstich ME, Carey MP, Ruggiero L, Enyart P, Gresham F. Assessment of depression in childhood and adolescence: An evaluation of the Center for Epidemiological Studies Depression Scale for Children (CES-DC) American Journal of Psychiatry. 1986;143(8):1024–1027. doi: 10.1176/ajp.143.8.1024. [DOI] [PubMed] [Google Scholar]
- Folkman S, Lazarus RS. An analysis of coping in a middle-aged community sample. Journal of Health and Social Behavior. 1980;21(3):219–239. [PubMed] [Google Scholar]
- Forbes EE, Dahl RE. Pubertal development and behavior: Hormonal activation of social and motivational tendencies. Brain and Cognition. 2010;72(1):66–72. doi: 10.1016/j.bandc.2009.10.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Freiheit SR, Overholser JC, Lehnert KL. The association between humor and depression in adolescent psychiatric inpatients and high school students. Journal of Adolescent Research. 1998;13(1):32–48. [Google Scholar]
- Frydenberg E, Lewis R. Adolescent Coping Scale: Administrator's manual. Melbourne, Australia: ACER (The Australian Council for Educational Research Ltd); 1993. [Google Scholar]
- Ge X, Lorenz FO, Conger RD, Elder GH, Simons RL. Trajectories of stressful life events and depressive symptoms during adolescence. Developmental Psychology. 1994;30(4):467–483. [Google Scholar]
- Hankin BL, Abramson LY, Miller N, Haeffel GJ. Cognitive vulnerability-stress theories of depression: Examining affective specificity in the prediction of depression versus anxiety in three prospective studies. Cognitive Therapy and Research. 2004;28(3):309–345. [Google Scholar]
- Hankin BL, Mermelstein R, Roesch L. Sex differences in adolescent depression: Stress exposure and reactivity. Child Development. 2007;78:279–295. doi: 10.1111/j.1467-8624.2007.00997.x. [DOI] [PubMed] [Google Scholar]
- Herman-Stahl MA, Stemmler M, Petersen AC. Approach and avoidant coping: Implications for adolescent mental health. Journal of Youth and Adolescence. 1995;24(6):649–665. [Google Scholar]
- Hollenstein T, Lougheed JP. Beyond storm and stress: Typicality, transactions, timing, and temperament to account for adolescent change. American Psychologist. 2013;68(6):444–454. doi: 10.1037/a0033586. [DOI] [PubMed] [Google Scholar]
- Horwitz AG, Hill RM, King CA. Specific coping behaviors in relation to adolescent depression and suicidal ideation. Journal of adolescence. 2011;34(5):1077–1085. doi: 10.1016/j.adolescence.2010.10.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kort-Butler LA. Coping styles and sex differences in depressive symptoms and delinquent behavior. Journal of Youth and Adolescence. 2009;38:122–136. doi: 10.1007/s10964-008-9291-x. [DOI] [PubMed] [Google Scholar]
- Kouros CD, Garber J. Trajectories of individual depressive symptoms in adolescents: Gender and family relationships as predictors. Developmental Psychology. 2014;50(12):2633–2643. doi: 10.1037/a0038190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lazarus RS, Folkman S. Stress, Appraisal, and Coping. New York, NY: Springer Publishing Company; 1984. [Google Scholar]
- Lewis KM, Byrd DA, Ollendick TH. Anxiety symptoms in African-American and Caucasian youth: Relations to negative life events, social support, and coping. Journal of Anxiety Disorders. 2012;26(1):32–39. doi: 10.1016/j.janxdis.2011.08.007. [DOI] [PubMed] [Google Scholar]
- Li CE, DiGiuseppe R, Froh J. The roles of sex, gender, and coping in adolescent depression. Adolescence. 2006;41(163):409–415. [PubMed] [Google Scholar]
- Maag JW, Irvin DM. Alcohol use and depression among African-American and Caucasian adolescents. Adolescence. 2005;40(157):87–101. [PubMed] [Google Scholar]
- Merluzzi TV, Philip EJ, Zhang Z, Sullivan C. Perceived discrimination, coping, and quality of life for African-American and Caucasian persons with cancer. Cultural Diversity and Ethnic Minority Psychology. 2014 doi: 10.1037/a0037543. Advance online publication, http://dx.doi.org/10.1037/a0037543. [DOI] [PMC free article] [PubMed]
- Molock SD, Barksdale CL. Relationship between religiosity and conduct problems among African American and Caucasian adolescents. Journal of Child and Family Studies. 2013;22:4–14. [Google Scholar]
- Moodley T, Esterhuyse K, Beukes R. The ways in which adolescents cope and their relationship to age, gender and specific religious variables. Journal of Psychology in Africa. 2014;22(1):10–20. [Google Scholar]
- Nicholls AR, Perry JL, Jones L, Morley D, Carson F. Dispositional coping, coping effectiveness, and cognitive social maturity among adolescent athletes. Journal of Sport and Exercise Psychology. 2013;35:229–238. doi: 10.1123/jsep.35.3.229. [DOI] [PubMed] [Google Scholar]
- Ohannessian CM. Media use and adolescent psychological adjustment: An examination of gender differences. Journal of Child and Family Studies. 2009;18(5):582–593. doi: 10.1007/s10826-009-9261-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ohannessian CM. Anxiety and substance use during adolescence. Substance Abuse. 2014;35(4):418–425. doi: 10.1080/08897077.2014.953663. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ohannessian CM, Lerner RM, Lerner JV, von Eye A. Does self-competence predict gender differences in adolescent depression and anxiety? Journal of Adolescence. 1999;22:397–411. doi: 10.1006/jado.1999.0231. [DOI] [PubMed] [Google Scholar]
- Parra-Cardona JR, Bulock LA, Imig DR, Villarruel FA, Gold SJ. “Trabajando duro todos los días”: Learning from the life experiences of Mexican-origin migrant families. Family Relations. 2006;55:361–375. [Google Scholar]
- Patterson JM, McCubbin HI. Adolescent coping style and behaviors: Conceptualization and treatment. Journal of Adolescence. 1987;10:163–186. doi: 10.1016/s0140-1971(87)80086-6. [DOI] [PubMed] [Google Scholar]
- Phelps SB, Jarvis PA. Coping in adolescence: Empirical evidence for a theoretically based approach to assessing coping. Journal of Youth and Adolescence. 1994;23:359–371. [Google Scholar]
- Plucker JA. Gender, race, and grade differences in gifted adolescents' coping strategies. Journal for the Education of the Gifted. 1998;21(4):423–436. [Google Scholar]
- Rawana JS, Kohut SA. Eating attitudes, coping styles, and peer victimization among adolescents with seasonal and nonseasonal depression symptoms. Cognitive Therapy and Research. 2012;36(3):199–209. [Google Scholar]
- Seiffge-Krenke I. Coping with relationship stressors: A decade review. Journal of Research on Adolescence. 2011;21(1):196–210. [Google Scholar]
- Smetana JG, Campione-Barr N, Metzger A. Adolescent development in interpersonal and societal contexts. Annual Review of Psychology. 2006;(57):255–284. doi: 10.1146/annurev.psych.57.102904.190124. [DOI] [PubMed] [Google Scholar]
- Sontag LM, Graber JA. Coping with perceived peer stress: Gender-specific and common pathways to symptoms of psychopathology. Developmental Psychology. 2010;46(6):1605–1620. doi: 10.1037/a0020617. [DOI] [PubMed] [Google Scholar]
- Spear LP. The adolescent brain and age-related behavioral manifestations. Neuroscience & Biobehavioral Reviews. 2000;24(4):417–463. doi: 10.1016/s0149-7634(00)00014-2. [DOI] [PubMed] [Google Scholar]
- Stockdale SE, Lagomasino IT, Siddique J, McGuire T, Miranda J. Racial/ethnic and ethnic disparities in detection and treatment of depression and anxiety among psychiatric and primary health care visits, 1995-2005. Medical Care. 2008;46(7):668–677. doi: 10.1097/MLR.0b013e3181789496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Telzer EH, Fuligni AJ. Positive daily family interactions eliminate gender differences in internalizing symptoms among adolescents. Journal of Youth and Adolescence. 2013;42:1498–1511. doi: 10.1007/s10964-013-9964-y. [DOI] [PubMed] [Google Scholar]
- Tolan PH, Gorman-Smith D, Henry D, Chung K, Hunt M. The relation of patterns of coping of inner-city youth to psychopathology symptoms. Journal of Research on Adolescence. 2002;12(4):423–449. [Google Scholar]
- Walker LS, Smith CA, Garber J, Van Slyke DA. Development and validation of the Pain Response Inventory for Children. Psychological Assessment. 1997;9(4):392–405. [Google Scholar]
- Weissman M, Orvaschel H, Padian N. Children's symptom and social functioning self-report scales: Comparison of mothers' and children's reports. Journal of Nervous and Mental Disorders. 1980;168(12):736–740. doi: 10.1097/00005053-198012000-00005. [DOI] [PubMed] [Google Scholar]
- Wight RG, Aneshensel CS, Botticello AL, Sepúlveda JE. A multilevel analysis of ethnic variation in depressive symptoms among adolescents in the United States. Social Science & Medicine. 2005;60(9):2073–2084. doi: 10.1016/j.socscimed.2004.08.065. [DOI] [PubMed] [Google Scholar]
- Wilson GS, Pritchard ME, Revalee B. Individual differences in adolescent health symptoms: The effects of gender and coping. Journal of Adolescence. 2005;28:369–379. doi: 10.1016/j.adolescence.2004.08.004. [DOI] [PubMed] [Google Scholar]
- Zimmer-Gembeck MJ, Skinner EA. The development of coping across childhood and adolescence: An integrative review and critique of research. International Journal of Behavioral Development. 2011;35(1):1–17. [Google Scholar]