

Abstract
Glandular Odontogenic Cyst is a relatively rare cyst of odontogenic origin, which shows glandular or salivary features that are thought to indicate the pluripotentiality of odontogenic epithelium. It is seen in middle-aged adults, and commonly involves the anterior region of the jaws, especially the mandible. It shows non-specific clinico-radiographic findings which may resemble other lesions, but has characteristic histopathologic features which help in its diagnosis. This paper reports an unusual presentation of a glandular odontogenic cyst which was diagnosed in a 64-year old female in the posterior maxilla, along with a literature review of this cyst, especially the cases reported in India in the past.
Keywords: Jaw, maxilla, odontogenic cyst
Introduction
The Glandular Odontogenic Cyst (GOC) is a rare developmental cyst of the jaws. It was initially described by Padayachee and van Wyk in 1987, who called it ‘Sialo-Odontogenic Cyst’ due to the presence of mucous cells and pools of mucin in the epithelial lining, and the fact that mucous pools are often lined by eosinophilic cuboidal cells which resemble salivary gland ducts [1]. Gardner et al in 1988 suggested the name ‘Glandular Odontogenic Cyst’ because the cyst wall epithelium was odontogenic and contained mucin elements with absence of salivary tissue [2]. In 1992, GOC was included in the WHO typing of tumors under the term GOC or sialo-odontogenic cyst [3]. An important feature of this cyst is that its recognition on the basis of clinical and radiographic features is practically impossible, and only histopathological examination allows for a certain diagnosis [4]. This case report describes a case of glandular odontogenic cyst in a 64-year old female which was diagnosed and treated in our institution.
Patient and observation
A 64-year-old female patient reported to our out-patient department with a chief complaint of swelling over the left side of the face since two months. History revealed that the swelling was initially small in size and had gradually increased to its present size. On extra-oral examination, a diffuse swelling was seen over the left cheek region, extending from the left nasolabial fold area, posteriorly to the malar region and supero-inferiorly from 2 cms below the infra-orbital margin to 1 cm away from the left angle of mouth, measuring around 3 x 2.5 cms. The overlying skin was normal with no evidence of any discharge. On palpation, the swelling was firm in consistency, tender, non-pulsatile and non-compressible, with no local rise in temperature. Intra-oral examination revealed a diffuse swelling in the left maxilla and buccal vestibule, extending from 23 till the 26 region (Figure 1). The swelling was firm in consistency with a smooth surface and tender on palpation. On examination of the teeth, 23 were restored, while 24 and 25 were missing. No tenderness or mobility of the teeth in the area was noted. An intra-oral periapical radiograph showed a large unilocular radiolucency with a well-defined thin corticated border extending from the distal aspect of 23, upto the 26 region. A maxillary true occlusal view showed a unilocular radiolucent lesion in the 23, 24, 25, 26 region causing expansion of the buccal cortical plate in the affected area (Figure 2). Panoramic radiography showed a well-defined oval-shaped unilocular radiolucency with thin corticated borders extending from the mesial aspect of 23 up to the 26 region, superiorly involving the maxillary sinus and inferiorly the maxillary alveolar crest. The internal structure was completely radiolucent. There was no evidence of root resorption or displacement of 23 or 26 (Figure 3).
Figure 1.

Pre-operative intra-oral view
Figure 2.
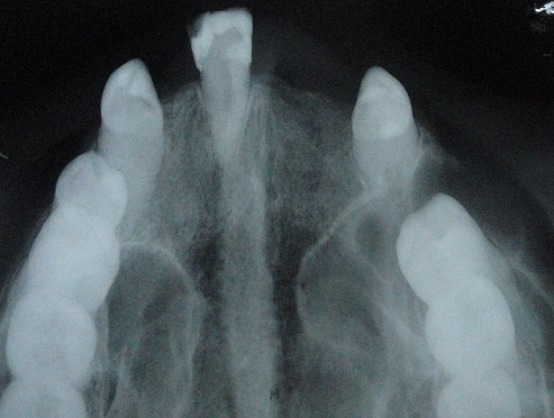
Maxillary true occlusal radiograph showing expansion of buccal cortical plate in region of 23, 24, 25 and 26
Figure 3.

Panoramic radiograph showing an oval-shaped unilocular radiolucency with thin corticated borders extending from 23 to 26 regions
Based on the history, clinical and radiographic findings, a provisional diagnosis of a residual cyst was made, with a differential diagnosis of an odontogenic cyst or tumor. The lesion was treated conservatively with careful enucleation and curettage. Histopathological examination showed a cystic lining with a pseudoglandular pattern in some areas, with other areas showing a pseudostratified columnar ciliated epithelium with goblet cells, some mucous pools / crypts (Figure 4). The connective tissue showed presence of collagen fibers, fibroblasts, blood vessels, areas of osteoid formation, and a mild chronic inflammatory cell infiltrate. Thus, based on the histopathology of the enucleated tissue, a final diagnosis of a glandular odontogenic cyst was made. Post-operative healing was uneventful. The patient has been under regular follow-up for the last 2 years, during which time no recurrence has been noted (Figure 5, Figure 6).
Figure 4.

Photomicrograph showing a cystic lesion with papillary projections lined by pseudostratified columnar epithelium with some mucous pools and pseudoglandular areas (a) H&E stain at 10x magnification, (b) H&E stain at 40x magnification
Figure 5.

Post-operative intra-oral view
Figure 6.

Post-operative panoramic radiograph
Discussion
GOC is a rare lesion with a frequency rate of only 0.012% to 1.3% of all the jaw cysts [5]. Till date, less than 200 cases of this lesion have been reported in literature. A literature review performed using the search terms “glandular odontogenic cyst”, “sialo-odontogenic cyst” on the PubMed interface yielded only 19 cases of histopathologically confirmed GOC that were reported in India, which have been detailed in Table 1, Table 2. GOC usually occurs in middle-aged adults, most often after the fourth decade of life, with a slight male predilection. It is four times more common in the mandible as compared to the maxilla and has a predilection for the anterior region of the jaws [20]. The present case differs from the literature in that it was diagnosed in a 64-year old female, and occurred in the maxilla extending antero-posteriorly from the canine to the first molar region, which is not commonly seen. Clinically features of this cyst are not specific, with lesions usually presenting as asymptomatic swellings. The radiographic appearance also varies and is not pathognomonic. It may present as a unilocular or multilocular radiolucency, which usually shows well-defined borders [20]. Occasionally, scalloping of the border may be noted, while root resorption and displacement are not commonly seen [3]. Radiographically, GOC may resemble lesions like radicular cyst, keratocystic odontogenic tumor, ameloblastoma and central giant cell granuloma. The radiographic features of our case were similar to those described previously, but were suggestive of a residual cyst primarily due to the absence of teeth 24 and 25. An interesting observation in our literature review of the previous cases of GOC reported in India showed that 7 out of 19 cases were also located in edentulous or partially edentulous areas (where teeth were extracted previously). This could indicate that GOC may possibly grow within the jaws without any symptoms in the initial stages, and cause swelling and cortical expansion only at a later date.
Table 1.
Clinical data of 19 cases of GOC previously reported in India along with the present case
| Authors of the Case Report | Age of Patient (years) | Sex | Swelling | Pain | Location |
|---|---|---|---|---|---|
| Baliga et al (1997) [6] | 26 | Male | Present | Present | Left anterior maxilla 21-22 |
| Jose et al (2000) [7] | 18 | Female | Present | Present | Right maxilla 16-17 and maxillary sinus |
| Krishnamurthy et al (2009) [5] | 42 | Female | Present | Absent | Anterior mandible, extending from right to left body of mandible 36-45 |
| 21 | Male | Present | Absent | Left mandible, from midline till ascending ramus | |
| Prabhu et al (2010) [8] | 47 | Female | Present | NR | Right maxilla 14-18 (missing 16) |
| Rao et al (2010) [9] | 60 | Female | Present | Absent | Left maxilla 26-28 and maxillary sinus (missing 27, 28) |
| Guruprasad et al (2011) [10] | 17 | Female | Present | Present | Right posterior maxilla and maxillary sinus |
| Amberkar et al (2011) [11] | 29 | Male | Present | Present | Bilateral - right maxilla 14-16 and left maxilla 24-26 |
| Purohit et al (2014) [2] | 30 | Female | Present | Absent | Right maxilla 15-17 |
| Shah M et al (2014) [12] | 40 | Male | Present | Present | Anterior mandible – left to right side 36-43 |
| Tambawala et al (2014) [13] | 17 | Female | Present | Present | Right mandible – angle and ramus |
| Mittal et al (2015) [14] | 17 | Female | Present | Present | Left anterior to right posterior mandible 34-47 |
| Faisal et al (2015) [15] | 11 | Male | Present | Absent | Anterior mandible, extending from right to left body of mandible 36-45 |
| Raju et al (2015) [16] | 65 | Female | Present | Absent | Anterior mandible, extending from right to left body of mandible (missing 31, 32, 41, 42) |
| Anchlia et al (2015) [17] | 63 | Female | Present | Present | Right anterior mandible, 31-45 |
| Shah A et al (2016) [3] | 25 | Male | Present | Absent | Left mandible 35-37 (missing 36) |
| 30 | Female | Present | Absent | Right mandible 46 (missing 46) | |
| Surej Kumar et al (2016) [18] | 46 | Female | Present | Absent | Anterior maxilla 12-13 |
| Chandra et al (2016) [19] | 70 | Female | Present | Present | Anterior maxilla 21-23 |
| Present Case | 64 | Female | Present | Present | Left maxilla 23-26 |
Table 2.
Radiographic data of 19 cases of GOC previously reported in India along with the present case
| Authors of the Case Report | Radiographic Appearance | Margins / Borders | Internal Structure | Root Resorption | Tooth / Root Displacement | Cortical Expansion | Impacted Tooth |
|---|---|---|---|---|---|---|---|
| Baliga et al (1997) [6] | Unilocular | Well-defined, Corticated | Radiolucent | Absent | Present 22 | Palatal | Absent |
| Jose et al (2000) [7] | NR | NR | Radiolucent | NR | NR | Buccal, palatal | Absent |
| Krishnamurthy et al (2009) [5] | Multilocular | Well-defined | Radiolucent | Edentulous | Edentulous | Buccal, lingual | Absent |
| Multilocular | Well-defined, corticated | Radiolucent | Absent | Absent | Buccal | Absent | |
| Prabhu et al (2010) [8] | Unilocular | Well-defined | Radiolucent | NR | NR | Buccal, palatal | Absent |
| Rao et al (2010) [9] | Unilocular | Well-defined | Radiolucent | Absent | Absent | Buccal | Absent |
| Guruprasad et al (2011) [10] | Unilocular | Well-defined | Radiolucent | Absent | Absent | NR | Present 18 |
| Amberkar et al (2011) [11] | Unilocular | Well-defined | Radiolucent | Absent | Present 14, 15 | NR | Absent |
| Purohit et al (2014) [2] | Unilocular | Well-defined | Radiolucent | Present 16 | Present 15, 17 | Buccal | Absent |
| Shah M et al (2014) [12] | Multilocular | Well-defined, Corticated | Radiolucent | Absent | Absent | Buccal | Absent |
| Tambawala et al (2014) [13] | Multilocular | Well-defined | Radiolucent | Present 47 | Absent | Buccal, lingual with perforation | Absent |
| Mittal et al (2015) [14] | Multilocular | Well-defined | Radiolucent | NR | NR | NR | Absent |
| Faisal et al (2015) [15] | Multilocular | Well-defined, Corticated | Radiolucent | Absent | Absent | Buccal, lingual, with perforation | Absent |
| Raju et al (2015) [16] | Multilocular | Well-defined | Radiolucent | Absent | Absent | NR | Absent |
| Anchlia et al (2015) [17] | Unilocular | Well-defined, Corticated | Radiolucent | Absent | Present 43 | NR | Absent |
| Shah A et al (2016) [3] | Unilocular | Well-defined, Corticated | Radiolucent | Absent | Absent | Buccal, lingual | Absent |
| Unilocular | Well-defined, Corticated | Radiolucent | -- | Absent | NR | Absent | |
| Surej Kumar et al (2016) [18] | Unilocular | Well-defined, Corticated | Radiolucent | Absent | Present | Buccal | Absent |
| Chandra et al (2016) [19] | Multilocular | Ill-defined | Radiolucent | Edentulous | Edentulous | Buccal, palatal | Absent |
| Present Case | Unilocular | Well-defined, Corticated | Radiolucent | Absent | Absent | Buccal | Absent |
NR: Not reported
Histologically, GOC shows certain characteristic features that were subdivided by Kaplan et al into major and minor criteria based on the frequency of occurrence of each feature in the previously reported cases [2]. At least focal presence of the major criteria is mandatory, while the presence of minor criteria further supports the correct diagnosis [3]. The major criteria include a lining of squamous epithelium of varying thickness which may show epithelial ‘spheres’ or ‘whorls’ with absence of basal palisading, cuboid-shaped eosinophilic (‘hobnail’) cells, and intraepithelial mucous / goblet cells or pools, with presence of glandular or duct-like structures [3, 13]. Papillary proliferation of the epithelial lining, multicystic appearance, and presence of ciliated or clear cells in the epithelium were included as minor criteria [13]. The present case showed most of the characteristic histopathological features of GOC described above. The histopathological features of GOC have been found to resemble a number of lesions having a wide clinico-pathologic spectrum ranging from other odontogenic cysts like lateral periodontal cyst to malignant neoplasms such as central low-grade mucoepidermoid carcinoma, and hence careful and detailed microscopic examination is essential in arriving at a correct diagnosis [5]. The exact treatment of choice of this lesion remains controversial, and varies from enucleation and curettage to local block excision depending on the size and aggressiveness [1]. Enucleation is preferred for small unilocular lesions, whereas management of large lesions includes enucleation with peripheral ostectomy for unilocular cases and marginal resection or partial jaw resection in multilocular cases [16]. Some of the previous cases reported in literature have been found to have an aggressive potential and hence a long-term follow-up is important to monitor for any signs of recurrence. The present case resembled a residual cyst and was thus treated by enucleation and curettage, and has been kept under regular observation till date, with no evidence of recurrence.
Conclusion
GOC is an uncommon cystic lesion, with less than 200 cases reported world-wide till date. This cyst shows non-specific clinico-radiographic characteristics which may resemble a wide-spectrum of lesions. A final diagnosis can only be obtained after a careful histopathologic examination and a long-term follow-up is required to rule out recurrences.
Acknowledgement
Dr. Anita Spadigam, Professor & Head, and Dr. Anita Dhupar, Professor, Department of Oral and Maxillofacial Pathology, Goa Dental College & Hospital, Bambolim, Goa – India, for providing the histopathological analysis, report and photographs.
Competing interests
The authors declare no competing interests
Authors’ contributions
All authors have read and agreed to the final version of this manuscript and have equally contributed to its content and to the management of the case.
References
- 1.Osny FJ, Azavedo LR, Sant’Ana E, Lara VS. Glandular odontogenic cyst: case report and review of the literature. Quintessence Int. 2004 May;35(5):385–9. [PubMed] [Google Scholar]
- 2.Purohit S, Shah V, Bhakhar V, Harsh A. Glandular odontogenic cyst in maxilla: A case report and literature review. J Oral Maxillofac Pathol. 2014 May;18(2):320–3. doi: 10.4103/0973-029X.140923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Shah AA, Sangle A, Bussari S, Koshy AV. Glandular odontogenic cyst: A diagnostic dilemma. Indian J Dent. 2016 Jan-Mar;7(1):38–4. doi: 10.4103/0975-962X.179371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Luczak K, Nowak R, Rzeszutko M. Glandular Odontogenic Cyst of the Mandible Associated with Impacted Tooth - Report of a Case and Review of Literature. Dent Med Probl. 2007 Jul;44(3):403–6. [Google Scholar]
- 5.Krishnamurthy A, Sherlin HJ, Ramalingam K, Natesan A, Premkumar P, Ramani P, Chandrasekar T. Glandular Odontogenic Cyst: Report of Two Cases and Review of Literature. Head Neck Pathol. 2009 Jun;3(2):153–8. doi: 10.1007/s12105-009-0117-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Baliga M, Aby J, Vidya M. Glandular odontogenic cyst: a case report. Indian J Dent Res. 1997 Jul-Sep;8(3):82–4. [PubMed] [Google Scholar]
- 7.Jose M, Rao NN, Solomon MC. Glandular odontogenic cyst. A rare entity with aggressive biological behaviour - A case report. Indian J Dent Res. 2000 Jul-Sep;11(3):107–10. [PubMed] [Google Scholar]
- 8.Prabhu S, Rekha K, Kumar G. Glandular odontogenic cyst mimicking central mucoepidermoid carcinoma. J Oral Maxillofac Pathol. 2010 Jan;14(1):12–5. doi: 10.4103/0973-029X.64303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rao JB, Jeevan Kumar KA, Kumar BP. Glandular odontogenic cyst involving the posterior part of maxillary sinus, a rare entity. J Maxillofac Oral Surg. 2010 Mar;9(1):72–5. doi: 10.1007/s12663-010-0020-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Guruprasad Y, Chauhan DS. Glandular odontogenic cyst of maxilla. J Clin Imaging Sci. 2011;1:54. doi: 10.4103/2156-7514.90074. 4103/2156-7514.90074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Amberkar VS, Jahagirdar A, Ahmed Mujib BR. Glandular odontogenic cyst: report of an unusual bilateral occurrence. Indian J Dent Res. 2011 Mar-Apr;22(2):364. doi: 10.4103/0970-9290.84285. [DOI] [PubMed] [Google Scholar]
- 12.Shah M, Kale H, Ranginwala A, Patel G. Glandular odontogenic cyst: A rare entity. J Oral Maxillofac Pathol. 2014 Jan;18(1):89–92. doi: 10.4103/0973-029X.131922. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Tambawala SS, Karjodkar FR, Yadav A, Sansare K, Sontakke S. Glandular odontogenic cyst: A case report. Imaging Sci Dent. 2014 Mar;44(1):75–9. doi: 10.5624/isd.2014.44.1.75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Mittal A, Narang V, Kaur G, Sood N. Glandular Odontogenic Cyst of Mandible: A Rare Entity. J Clin Diagn Res. 2015 Dec;9(12):ED09–10. doi: 10.7860/JCDR/2015/15005.6901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Faisal M, Ahmad SA, Ansari U. Glandular odontogenic cyst - Literature review and report of a paediatric case. J Oral Biol Craniofac Res. 2015 Sep-Dec;5(3):219–25. doi: 10.1016/j.jobcr.2006.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Raju SP, Reddy SP, Ananthnag J. Glandular odontogenic cyst of the anterior mandible. N Am J Med Sci. 2015 Feb;7(2):65–9. doi: 10.4103/1947-2714.152081. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Anchlia S, Bahl S, Shah V, Vyas S. Glandular odontogenic cyst: a rare entity revealed and a review of the literature. BMJ Case Rep. 2015 Aug 21; doi: 10.1136/bcr-2015-211502. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Surej Kumar LK, Manuel S, Nair BJ, Nair SV. An ambiguous asymptomatic swelling in the maxillary anterior region - A case report. Int J Surg Case Rep. 2016;23:65–9. doi: 10.1016/j.ijscr.2016.02.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Chandra S, Reddy ES, Sah K, Srivastava A. Maxillary Glandular Odontogenic Cyst: An Uncommon Entity at an Unusual Site. Arch Iran Med. 2016 Mar;19(3):221–4. 0161903/AIM.0012. [PubMed] [Google Scholar]
- 20.Manor R, Anavi Y, Kaplan I, Calderon S. Radiological features of glandular odontogenic cyst. Dentomaxillofac Radiol. 2003 Mar;32(2):73–9. doi: 10.1259/dmfr/22912856. [DOI] [PubMed] [Google Scholar]