

Abstract
Background
Tuberculosis is an infection that requires at least 6 months of chemotherapy in order to clear the bacteria from the patient’s lungs. Usually, therapeutic monitoring is dependent on smear microscopy where a decline in acid-fast bacilli is observed. However, this might not be indicative of the actual decline of bacterial load and thus other tools such as culture and molecular assays are required for patient management.
Case presentation
Here, we report the case of a 12-year-old Black African boy co-infected with tuberculosis and human immunodeficiency virus who remained smear culture positive and liquid culture negative for a prolonged period of time following chemotherapy. In order to determine whether there was any live bacteria present in his specimens, we applied the newly developed molecular bacterial load assay that detects the presence of 16S ribosomal ribonucleic acid derived from the bacteria. Using this methodology, we were able to quantify his bacterial load and inform the management of his treatment in order to reduce the disease burden. Following this intervention he went on to make a complete recovery.
Conclusions
This case report highlights the value of improved biomarkers for monitoring the treatment of tuberculosis and the role of molecular assays such as the molecular bacterial load assay applied here. The molecular bacterial load assay detects bacterial ribonucleic acid which corresponds closely with the number of live bacilli as compared with polymerase chain reaction that detects deoxyribonucleic acid and may include dead bacteria.
Keywords: Case report, Tuberculosis treatment monitoring, Molecular bacterial load, Rapid assay, Clinical decisions, Childhood tuberculosis
Background
Tuberculosis (TB) infection is considered a global health emergency. In 2013, there were an estimated 9 million cases of TB, of which 550,000 (6.1 %) were pediatric [1]. Recent modeling work suggests these pediatric estimates are outdated and only represent 35 % of the true burden [2]. An estimated 13 % of new TB cases were human immunodeficiency virus (HIV) positive and 360,000 of the 1.5 million deaths were in patients who were HIV positive.
TB-HIV co-infection represents a lethal combination: the immunodeficiency induced by HIV leads to progression of TB disease and TB itself decreases the CD4 count and worsens the immunodeficiency caused by HIV in children [3]. Children with HIV infection are 20 times more likely to develop TB and have a six times greater risk of dying from TB than children who do not have HIV infection [3]. Anti-retroviral therapy (ART) has great potential to reduce the risk of TB disease [4]. Diagnosis of TB in patients with HIV is challenging since the presentation may be nonspecific and the combination of clinical features and radiological findings frequently overlap with other common clinical presentations in HIV. In addition, immunological-based assays including the tuberculin skin test (TST) and interferon-gamma release assays may be less sensitive in patients with HIV [5]. Furthermore, the management of TB-HIV co-infection is challenging as concurrent administration of anti-TB therapy (ATT) and ART is associated with significant drug interactions, potentially limiting their efficacy [6].
There is an urgent need for development of new biomarkers that will enable better diagnosis and treatment of TB, particularly in patients with HIV infection. Childhood TB has historically been neglected but recent initiatives are currently examining new therapeutics and novel diagnostic tools specifically for children. One of the key issues for microbiological diagnosis of TB is obtaining timely confirmation of the presence of viable bacteria: culture is slow and can miss specific subpopulations that are viable but non-culturable, whereas mycobacterial deoxyribonucleic acid (DNA) persists beyond the point where there is evidence of viable organisms, making DNA-based assays unsuitable for monitoring the decline of live bacteria in clinical samples [7, 8]. We previously developed a molecular test, the molecular bacterial load (MBL) assay, based on the detection of mycobacterial ribosomal ribonucleic acid (RNA) that detects live mycobacteria independent of those that are dead [9, 10]. This assay has been previously used in retrospective studies for monitoring TB treatment as well as in early bactericidal assays and it is currently implemented in clinical trials by the Pan African Consortium for the Evaluation of Antituberculosis Antibiotics. Here we report a case of pediatric TB-HIV co-infection where the MBL assay, a research tool, was utilized in real time to gain information about the disease progression, inform treatment decisions, and monitor treatment compliance.
Case presentation
We present the case of a 12-year-old Black African boy with perinatally acquired HIV infection and pulmonary TB. He was born in the United Kingdom (UK) and did not receive the Bacillus Calmette–Guérin (BCG) vaccine. He remained clinically well and off ART until 2013 when he developed recurrent episodes of shingles. At this time, his CD4 count fell below 500 cells/mm3 for the first time. He commenced ART with Kivexa® (abacavir/lamivudine), darunavir, and ritonavir in March 2014. In July 2014, he presented to his local accident and emergency department (A&E) with a cough associated with hemoptysis. At this time he reported a 6-month history of non-productive cough, loss of appetite, and weight loss. He denied fever and night sweats. He had travelled to Kenya in 2012 with his family, but had no confirmed contact with individuals with active TB. A sputum sample was found to have acid-fast bacilli (AFB) on microscopy. A chest X-ray and computed tomography (CT) scan of his thorax were indicative of pulmonary TB infection (Fig. 1). He was transferred to Great Ormond Street Hospital for Sick Children, National Health Service (NHS) Trust, London, UK for ongoing care. He was commenced on ATT with isoniazid, rifabutin, ethambutol, and pyrazinamide as per local guidelines. He had no further episodes of hemoptysis and following review by the thoracic surgeons and radiologists, it was agreed he did not require intervention at that stage (Fig. 1). The AFB were confirmed to be Mycobacterium tuberculosis complex and found to be fully drug sensitive via drug susceptibility testing.
Fig. 1.
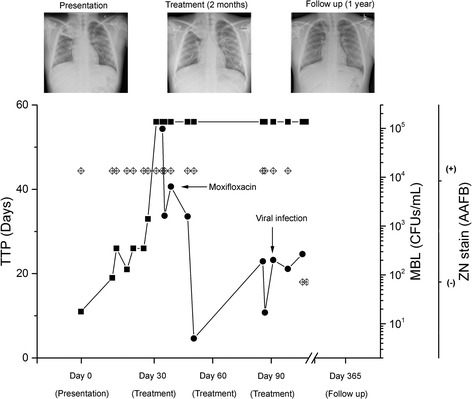
The clinical presentation of the patient over time. Three representative X-ray pictures from patient presentation, during therapy, and follow-up are shown on top of the graph. The time to positivity from culture is reported in days on the left y-axis with black squares. A time to positivity of 56 is considered to be negative. The molecular bacterial load values are shown on right y-axis as black dots. Smear microscopy is referred to as acid-fast bacilli positive or acid-fast bacilli negative for positive or negative samples respectively and is shown on the graph as diamonds. AAFB+ acid-fast bacilli positive, AAFB– acid-fast bacilli negative, CFU colony-forming unit, MBL molecular bacterial load, TTP time to positivity, ZN Ziehl–Neelsen
Despite being on an appropriate treatment regimen, his sputum remained smear positive. In view of this, repeat resistance testing was performed that did not show evidence of resistance to first-line therapy. For this reason, an MBL assay was performed on serial sputum samples in order to examine the status of the bacilli. This assay demonstrated that despite a month of effective therapy there were still detectable numbers of live bacteria in the sputum samples (Fig. 1). On the basis of these results, his ATT was modified to moxifloxacin, isoniazid, pyrazinamide, and ethambutol. He was discharged home on this regimen under video observed therapy (VOT) and reviewed regularly by the Pediatric TB service to ensure compliance with treatment. Serial sputum samples tested using the MBL assay over the next 2 weeks demonstrated declining numbers of live bacteria, despite ongoing sputum smear positivity (Fig. 1).
He remained clinically well until an out-patient clinic review 4 weeks later. At this time, he had an upper respiratory tract infection and a new onset cough. A sputum sample at this time was smear positive. He was readmitted and treated with oral co-amoxiclav for a presumed intercurrent infection. Nasopharyngeal aspirate and sputum sample testing did not reveal a virological or bacteriological cause for this. A repeat chest X-ray showed radiological improvement (Fig. 1). A further sputum sample sent 3 days later was also smear positive. Both of these samples were also sent for MBL assay in addition to mycobacterial culture via the BACTEC MGIT 960 System (Becton Dickinson) and resistance testing. The MBL assay confirmed a very low bacterial load, ~200 colony-forming units (CFUs), whereas culture and resistance testing was negative. Clinically he continued to improve and all further samples were smear and culture negative (Fig. 1). He has had no further sputum smear or culture positive results and completed a 9-month treatment course without further incident.
Conclusions
In this case of prolonged sputum smear positivity, the MBL assay was extremely useful both for informing the decision to change from rifabutin to moxifloxacin and for following this to confirm mycobacterial response to the appropriate anti-tuberculous treatment. In addition, when he presented with renewed sputum smear positivity, presumably due to mobilization of dead mycobacteria secondary to a viral-induced cough, the MBL assay provided reassurance that there was a very low bacterial load in his sputum samples.
Our patient responded well both clinically and with decreasing levels of live bacteria as measured by the MBL assay to a switch in treatment from rifabutin to moxifloxacin. Last generation fluoroquinolones have anti-TB bactericidal activity that is comparable with rifamycins and data from adult patients suggest that this treatment is efficacious [11]. There are no clinical trials on the use of these drugs in children, although a recent pharmacokinetic and safety study for multidrug-resistant TB in children supports their use [12]; however, further studies are required before they can be routinely recommended for drug-sensitive TB.
It is clear that effective treatment monitoring can be utilized for TB infections and a rapid biomarker such as the MBL assay, which enables the enumeration of live mycobacteria in sputum, is vital for appropriate patient management and to avoid development of resistance. Since smear microscopy cannot differentiate between live and dead bacilli and some populations of M. tuberculosis might not be recovered using microbiological-based culture, a molecular tool that utilizes bacterial RNA for its detection can identify accurately the presence of live bacteria in clinical samples [13]. Our patient had a complete recovery; however, his last MBL tests constantly exhibited values of around 200 CFUs (Fig. 1). The significance of these low numbers of bacteria in the clinical samples and their potential relevance for causing further disease progression or relapse is unclear. One hypothesis is that the immune system can perhaps effectively contain these low numbers of bacilli without any clinical symptoms, but further work is required.
Acknowledgements
Not applicable.
Funding
DE and TDMcH are part of the PreDiCT-TB consortium (http://www.predict-tb.eu/) which is funded from the Innovative Medicines Initiative Joint Undertaking (http://www.imi.europa.eu) under grant agreement No 115337, resources of which are composed of financial contributions from the European Union’s Seventh Framework Programme (FP7/2007–2013) and European Federation of Pharmaceutical Industries and Associations (EFPIA) companies in kind contribution.
Availability of data and materials
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Authors’ contributions
EW and DS have been involved in medical examination and image capture; DE was involved in generating the molecular bacterial load data; DE, EW, TDMcH, and DS analyzed and compared all datasets; DE and EW wrote the first draft of the manuscript. All authors reviewed and improved the manuscript. All authors read and approved the final manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Written informed consent was obtained from the patient’s legal guardians for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Ethics approval and consent to participate
This assay was performed as part of the clinical management of the patient and so did not require ethical approval.
Abbreviations
- A&E
Accident and emergency department
- AFB
Acid-fast bacilli
- ART
Anti-retroviral therapy
- ATT
Anti-tuberculosis therapy
- BCG
Bacillus Calmette–Guérin
- CFU
Colony-forming unit
- CT
Computed tomography
- HIV
Human immunodeficiency virus
- MBL
Molecular bacterial load
- NHS
National Health Service
- TB
Tuberculosis
- TST
Tuberculin skin test
- VOT
Video observed therapy
Contributor Information
Dimitrios Evangelopoulos, Phone: +44(0)20 8816 2449, Email: dimitrios.evangelopoulos@crick.ac.uk.
Elizabeth Whittaker, Email: e.whittaker@imperial.ac.uk.
Isobella Honeyborne, Email: i.honeyborne@ucl.ac.uk.
Timothy D. McHugh, Email: t.mchugh@ucl.ac.uk
Nigel Klein, Email: n.klein@ucl.ac.uk.
Delane Shingadia, Email: Delane.Shingadia@gosh.nhs.uk.
References
- 1.WHO . Global tuberculosis report 2014: WHO report. Geneva: World Health Organization; 2014. [Google Scholar]
- 2.Dodd PJ, Gardiner E, Coghlan RH, Seddon JA. Burden of childhood tuberculosis in 22 high-burden countries: A mathematical modelling study. Lancet Glob Health. 2014;2:453–9. doi: 10.1016/S2214-109X(14)70245-1. [DOI] [PubMed] [Google Scholar]
- 3.Palme IB, Gudetta B, Degefu H, Bruchfeld J, Muhe L, Giesecke J. Risk factors for human immunodeficiency virus infection in Ethiopian children with tuberculosis. Pediatr Infect Dis J. 2001;20(11):1066–72. doi: 10.1097/00006454-200111000-00012. [DOI] [PubMed] [Google Scholar]
- 4.Verhagen LM, Warris A, van Soolingen D, de Groot R, Hermans PW. Human immunodeficiency virus and tuberculosis coinfection in children: challenges in diagnosis and treatment. Pediatr Infect Dis J. 2010;29(10):e63–70. doi: 10.1097/INF.0b013e3181ee23ae. [DOI] [PubMed] [Google Scholar]
- 5.Mandalakas AM, van Wyk S, Kirchner HL, Walzl G, Cotton M, Rabie H, Kriel B, Gie RP, Schaaf HS, Hesseling AC. Detecting tuberculosis infection in HIV-infected children: a study of diagnostic accuracy, confounding and interaction. Pediatr Infect Dis J. 2013;32(3):e111–8. doi: 10.1097/INF.0b013e31827d77b7. [DOI] [PubMed] [Google Scholar]
- 6.Cohen JM, Whittaker E, Walters S, Lyall H, Tudor-Williams G, Kampmann B. Presentation, diagnosis and management of tuberculosis in HIV-infected children in the UK. HIV Med. 2008;9:277–84. doi: 10.1111/j.1468-1293.2008.00559.x. [DOI] [PubMed] [Google Scholar]
- 7.Kennedy N, Gillespie SH, Saruni AO, Kisyombe G, McNerney R, Ngowi FI, Wilson S. Polymerase chain reaction for assessing treatment response in patients with pulmonary tuberculosis. J Infect Dis. 1994;170(3):713–6. doi: 10.1093/infdis/170.3.713. [DOI] [PubMed] [Google Scholar]
- 8.Friedrich SO, Rachow A, Saathoff E, Singh K, Mangu CD, Dawson R, Phillips PP, Venter A, Bateson A, Boehme CC, et al. Assessment of the sensitivity and specificity of Xpert MTB/RIF assay as an early sputum biomarker of response to tuberculosis treatment. Lancet Respir Med. 2013;1(6):462–70. doi: 10.1016/S2213-2600(13)70119-X. [DOI] [PubMed] [Google Scholar]
- 9.Honeyborne I, Mtafya B, Phillips PP, Hoelscher M, Ntinginya EN, Kohlenberg A, Rachow A, Rojas-Ponce G, McHugh TD, Heinrich N. The molecular bacterial load assay replaces solid culture for measuring early bactericidal response to antituberculosis treatment. J Clin Microbiol. 2014;52(8):3064–7. doi: 10.1128/JCM.01128-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Honeyborne I, McHugh TD, Phillips PP, Bannoo S, Bateson A, Carroll N, Perrin FM, Ronacher K, Wright L, van Helden PD, et al. Molecular bacterial load assay, a culture-free biomarker for rapid and accurate quantification of sputum Mycobacterium tuberculosis bacillary load during treatment. J Clin Microbiol. 2011;49(11):3905–11. doi: 10.1128/JCM.00547-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bonora S, Mondo A, Trentini L, Calcagno A, Lucchini A, Di Perri G. Moxifloxacin for the treatment of HIV-associated tuberculosis in patients with contraindications or intolerance to rifamycins. J Infect. 2008;57(1):78–81. doi: 10.1016/j.jinf.2008.05.005. [DOI] [PubMed] [Google Scholar]
- 12.Thee S, Garcia-Prats AJ, Draper HR, McIlleron HM, Wiesner L, Castel S, Schaaf HS, Hesseling AC. Pharmacokinetics and safety of moxifloxacin in children with multidrug-resistant tuberculosis. Clin Infect Dis. 2015;60(4):549–56. doi: 10.1093/cid/ciu868. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Sabiiti W, Mtafya B, Kuchaka D, Azam K, Viegas S, Mdolo A, Farmer EC, Khonga M, Evangelopoulos D, Honeyborne I, et al. Optimising molecular diagnostic capacity for effective control of tuberculosis in high-burden settings. Int J Tuberc Lung Dis. 2016;20(8):1004–9. doi: 10.5588/ijtld.15.0951. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets analyzed during the current study are available from the corresponding author on reasonable request.