

ABSTRACT
The real cause of intussusception is not fully understood and a variety of conditions have been associated with it (Meckel diverticulum, polyps, duplication cysts, parasites, Henoch-Schönlein purpura, cystic fibrosis, hemolytic-uremic syndrome and infectious gastroenteritis). Furthermore few European countries, following WHO recommendation to monitor baseline incidence of intussusception before implementation of immunization program for rotavirus, used intussusception rate as a baseline value to compare the same figures in the period before and after introduction of vaccination. In this study, data of intussusception hospitalizations occurred among Italian children aged 0 through 59 months from 2009 to 2014 were analyzed.
A total amount of 3,088 children were included, accounting for a hospitalization rate of 20.2 per 100,000. Overall, the hospitalization rate for intussusception had a slight increase in trend from 2009 to 2014 (18%). In particular children 0–11 months had a hospitalization rate higher than 12–59 months with an aggregate value of 36 Vs. 16 per 100,000 respectively. Among all children hospitalized for intussusception a total of 239 (7.7%) had also a previous or concomitant hospitalization for gastroenteritis.
This study demonstrates that Italian hospitalizations for intussusception are increasing by time and the role played by different risk factors, including acute gastroenteritis, have to be investigated in the future. These data could be useful to monitor intussusception hospitalization in the perspective of anti-rotavirus vaccination introduction in Italy.
KEYWORDS: bacterial, gastroenteritis, hospitalization rate, intussusception, italy, infectious, rotavirus, vaccination, viral
Introduction
Intussusception is the invagination of an intestine segment within a more distal one and it is the most common cause of bowel obstruction in children.1 About 60% of affected children are under one year of age and 80% to 90% have less than 2 years, appearing to be less common before the 3 months and after 6 y.2 In Switzerland, from 2003 to 2006, the mean yearly incidence rates of intussusception in the first, second, and third year of life were 38, 31, and 26 cases per 100,000, respectively.3 Furthermore, German estimated crude incidence for children younger than 1 y was 26.6/100,000, with only minor seasonal fluctuations.4
The most accredited pathogenesis ascribes intussusception to an imbalance of longitudinal forces caused by a mass connecting with disorganized pattern of peristalsis.5 However, the etiology of intussusceptions is likely attributable to a combination of several conditions, including Meckel diverticulum,6 polyps,7 duplication cysts,8 parasites (eg, Ascaris lumbricoides),9 Henoch-Schönlein purpura,10 cystic fibrosis,11 and hemolytic-uremic syndrome.12 Furthermore, an increasing body of evidence has suggested also viral triggers as contributors, identifying a strong association with enteric and non-enteric species of adenovirus, for which the evidence of recent infection was described from 30 to 40% of cases in different studies.13,14,15,16 Bacterial enteritis was also associated with intussusception. In a series of 293 intussusception cases among children seen at military treatment facilities, bacterial enteritis ensued in 37 cases (2.6%). This association was noted for infection with Salmonella, E. coli, Shigella, or Campylobacter.17
Although some of clinical manifestation are still unknown, intussusception increased its popularity in the last 2 decades because of its potential temporal association with rotavirus vaccination.18 Anti-RV is a live-attenuated vaccine which have been designed to mimic the immunologic responses stimulated by natural rotavirus infection.19 Nowadays in Italy the anti-RV vaccination is not offered as UMV by the National Health System. In particular, it is supplied by co-payment in some administrative regions and it is free only for children at risk in others with small vaccination coverage.20 Among all administrative Italian regions, Sicily was the first to provide the anti-RV vaccine as UMV from 2013.21 According to WHO recommendation, that suggest to monitor baseline incidence of intussusception before the perspective of rotavirus vaccines introduction,22 the present study was aimed to evaluate incidence rates of intussusception among infants hospitalized in Italy from 2009 to 2014, a period without rotavirus vaccination availability, to define baseline incidence of intussusception.
Results
A total of 3,437 children, aged 0–59 months, were hospitalized for intussusception in Italy from 2009 to 2014. Of these 349 had at least one repeated hospital admission and were excluded by following analysis. Therefore 3,088 children accounting for an average 515 cases per year and a hospitalization rate of 20.2 per 100,000 were evaluated in this report. They were more frequently male cases (M:F sex ratio 1.8) with a median age of 1 y (IQR 0–2). Over one third (n = 1,086; 35.2%) of cases occurred in the age class 0–11 months. Furthermore 94.2% of hospitalizations were fully recovered and discharged from hospital, and only 2 died have occurred for respiratory failure and sepsis respectively (Table 1). Of all children hospitalized for intussusception a total of 239 (7.7%) had also a concurrent or during previous 30 d hospitalization for gastroenteritis (data not shown in table). Among these the more common type of gastroenteritis was infectious unspecified (43.5%) followed by viral (32.6%), not infectious (13.0%) and bacterial etiology (10.9%).
Table 1.
Characteristics of children hospitalized for intussusception aged 0–59 months in Italy (2009–2014).
| Italian intussusception hospitalization | N = 3,088 |
|---|---|
| Gender, n (%) | |
| Male | 1,970 (63.8) |
| Female | 1,118 (36.2) |
| Age, median in year (IQ range) | 1 (0–2) |
| Age classes in months, n (%) | |
| 0–11 | 1,086 (35.2) |
| 12–59 | 2,002 (64.8) |
| Hospitalization rate per 100,000 (CI 95%) | |
| 0–11 months | 36.5 (32.9–40.1) |
| 12–59 months | 16.2 (13.4–19.2) |
| 0–59 months | 20.2 (18.0–22.4) |
| Mean of intussusception hospitalizations per year ( ± SD) | 515 (45.5) |
| Hospitalization length, median in days (IQ range) | 3 (2–5) |
| Discharge status, n (%) | |
| Transferred | 178 (5.7) |
| Death | 2 (0.1) |
| Discharged | 2,908 (94.2) |
Figure 1 shows the trends of hospitalization rate for intussusception in Italy among children aged 0–59 and in 2 subgroups 0–11 and 12–59 months. Among the whole population, the hospitalization rate showed an increasing trend from 2009 to 2014 (18%) reaching a peak in 2012 of 22.6 per 100,000. However, children 0–11 months had a hospitalization rate higher with an aggregate value of 36 per 100,000 and a slight reduction (−9%) from 2009 to 2014, whereas, those 12–59 months were hospitalized with a mean rate of 16 per 100,000 during the study period but showing an increasing trend with a growth of 40%.
Figure 1.
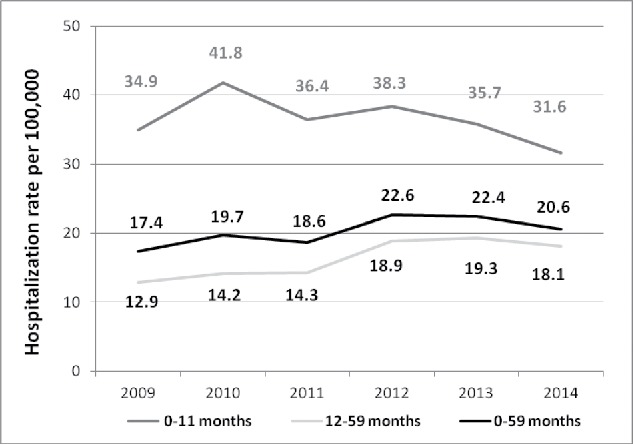
Intussusception hospitalization rate by age in months among Italian children (2009–2014).
Furthermore, the distribution of intussusception hospitalizations by month of age during the first year of life shows a higher rate of hospital admissions in the second half of the year than in the first half. In particular there is an increase number of intussusceptions from 4 months of age reaching a peak during 7 months of age with a value of 138 cases (Fig. 2).
Figure 2.
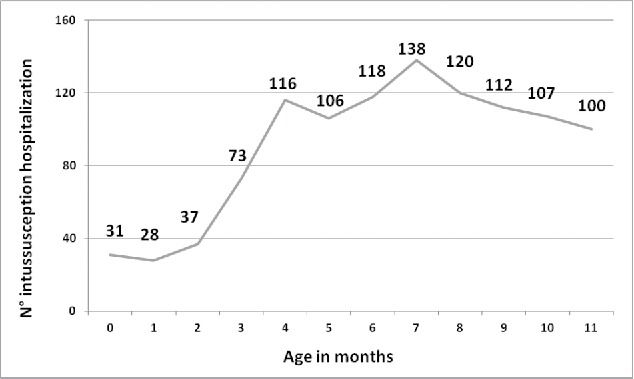
Intussusception hospitalization cases during first year of life (2009–2014).
Discussion
This study reported the baseline hospitalization rate for intussusception in Italy, a country without nationwide rotavirus vaccination availability. Italian hospitalization rate for intussusception in children 0–59 months increased in hospitalization rate of 18% during the study period. A similar raising trend was also showed in France, where it was analyzed emergency department data in children below 18 y.23 Furthermore, Italian data according to other studies, demonstrate a major risk of intussusception hospitalization among children 0–11 months than 12–59 months.2,24 In detail, hospitalization rate of 0–11 months children with a value of 36.5 per 100,000 was similar to value reported in Switzerland (38 per 100,000),3 but slightly increased than hospitalization rate reported in Germany and the UK (26.2 and 24.8 per 100,000 respectively).4,25 Overall, these data confirm that intussusception is a relatively frequent disease during the first year of life probably due to a higher exposure to risk factors and the higher frequency of atypical clinical manifestation leading to a delay in healthcare treatment.26,27 Even if these different data among neighboring nations could reflect different organization levels of primary care that should be evaluated in future comparison.
Moreover, the increasing number of intussusception cases in Italy needs to investigate risk factors associated with its origin. Although our study was based on official HDR, and we were unable to evaluate potential risk factors acting before intussusception onset, some considerations have to be done. Several studies identified the possible risk factors in breastfeeding, health status of children, environmental characteristics and gastroenteritis of different etiology.17,28,29 This latter relationship was supported by the disproportionate development of the immune response and a consequent lymphoid tissue hypertrophy of the Peyer's patches in children with gastroenteritis that exposed them at greater risk of intussusception.30 In Italian children a little percentage of cases (7.7%) occurred in those who had a concurrent or 30-day previous hospital admission for severe gastroenteritis. In detail, the percentage of Italian intussusception with gastroenteritis was less than Germany and Switzerland (18% and 24% of children hospitalized for intussusception respectively).4,3 Italian HDR data also revealed undetermined infectious type as the most frequent cause of gastroenteritis hospital admission in children with intussusception. This phenomenon can be partially explained with lack to perform test identifying etiology of gastroenteritis in clinical practice.31
Furthermore, these data provide evidence on the age onset of intussusception in children 0–11 months before anti-RV vaccination introduction. In detail, intussusception among Italian children 0–11 months without vaccination had an initial increase during 4th month with a peak in the 7th month of life. This increase was in accordance to data reported among children hospitalized in Switzerland and the UK.3,25
In our series mortality for intussusception occurred in <1% of patients. This result was in accordance with those reported in developed countries,32 whereas in countries where access to quality health care is less common it was reported a median intussusception mortality of 11%.33 The 2 Italian deaths seem can be due to a delayed access to health services which is well recognized to be associated with adverse outcomes and poor prognosis.34 This finding underscores the importance of increasing awareness about intussusception and understanding the atypical clinical presentation among healthcare provider.35
A main limit of this study must be stressed, because the use of HDR could be cause of underestimation according to international reported data about intussusception cases missed in analyses using only inpatient discharge data.36 However, in our opinion, considering the temporal stability of hospitalized intussusception cases and the long period analyzed in this Italian study, HDR-based inpatient data could be a reasonable proxy for overall intussusception rates and should reflect its trends over time.
Finally this study demonstrated an intussusceptions increasing trend during study period in absence of a nationwide anti-RV vaccination program. This data should be considered useful to investigate the specific role played by different risk factors in order to sustain the introduction of anti-rotavirus vaccination in Italy.
Material and methods
This analysis included data of hospitalizations occurred among children aged 0 through 59 months from 2009 to 2014 and resident in Italy, a country with a newborn cohort of about 500,000 children per year.
HDR were the source of data and they were obtained from the Italian Ministry of Health Office, which routinely collects these data from all national public and private hospitals. Each HDR includes admission and discharge dates, discharge status (categorized as “discharged,” “transferred” or “death”), demographic information (birthplace, residence, gender, and age) and up to 6 discharge diagnoses (1 principal and 5 secondary diagnoses) coded according to ICD-9-CM.
Cases of intussusception were defined as all hospitalizations with an ICD-9-CM diagnosis code of 560.0 included among one of discharge diagnoses. Moreover, hospitalization for bacterial gastroenteritis (ICD-9-CM diagnosis code from 001 to 005 excluding 005.2 and including from 008.0 to 008.5), parasitic gastroenteritis (ICD-9-CM diagnosis code from 006 to 007 excluding 006.2–006.6), viral gastroenteritis (ICD-9-CM diagnosis code from 008.6 to 008.8), gastroenteritis of unspecified infectious origin (ICD-9-CM diagnosis code from 009.0 to 009.3) and not infectious gastroenteritis (ICD-9-CM diagnosis code from 558 to 558.9) were also comparatively analyzed in the same children with intussusception.37 Repeated cases of intussusception were excluded from the analysis due to an anonymous code of identification.
Furthermore, hospitalizations for intussusception occurred among Sicilian children were excluded from this study because there was already implemented a UMV against rotavirus from 2013 and intussusception hospitalization was already analyzed.24,38,39,40
Statistical analysis
Hospitalization rates (per 100,000) and CI 95% for each investigated year were calculated using the census population for children aged 5 or less years. The trends in infants' hospitalizations were analyzed after stratifying by sex and age. To compare normally and not normally distributed variables were used Student's t-test and Mann–Whitney test respectively. Chi-square were used to compare categorical variables. Statistical significance was set at p < 0.05 (p values are 2-tailed). All analyses were performed using the STATA v14.1 software package.
Abbreviations
- anti-RV
anti-rotavirus
- CI
confidence interval
- HDR
Hospital discharge record
- ICD9-CM
International Classification of Disease, Ninth Revision, Clinical Modification
- IQ range
interquartile range
- UMV
Universal Mass Vaccination
- WHO
World Health Organization
Disclosure of potential conflicts of interest
No potential conflicts of interest were disclosed.
Acknowledgments
The Authors are grateful to General Directorate for Health Planning, VI Office, Italian Ministry of Health, for providing data useful to carry out the analysis.
References
- [1].Lloyd DA, Kenny SE. The surgical abdomen In: Walker WA, Goulet O, Kleinman RE, et al (Eds). Pediatric Gastrointestinal Disease: Pathopsychology, Diagnosis, Management 4th ed. Ontario: BC Decker, 2004; 604 [Google Scholar]
- [2].Mandeville K, Chien M, Willyerd FA, Mandell G, Hostetler MA, Bulloch B. Intussusception: clinical presentations and imaging characteristics. Pediatr Emerg Care 2012; 28:842; PMID:22929138; http://dx.doi.org/ 10.1097/PEC.0b013e318267a75e [DOI] [PubMed] [Google Scholar]
- [3].Buettcher M, Baer G, Bonhoeffer J, Schaad UB, Heininger U. Three-year surveillance of intussusception in children in Switzerland. Pediatrics 2007; 120:473; PMID:17766518; http://dx.doi.org/ 10.1542/peds.2007-0035 [DOI] [PubMed] [Google Scholar]
- [4].Jenke AC, Klaassen-Mielke R, Zilbauer M, Heininger U, Trampisch H, Wirth S. Intussusception: incidence and treatment-insights from the nationwide German surveillance. J Pediatr Gastroenterol Nutr 2011; 52(4):446-51; PMID:21415671; http://dx.doi.org/ 10.1097/MPG.0b013e31820e1bec [DOI] [PubMed] [Google Scholar]
- [5].Perrin WS, Lindsay EC. Intussusception: a monograph based on 400 cases. Br J Surg 1921; 9:46-71; http://dx.doi.org/ 10.1002/bjs.1800093308 [DOI] [Google Scholar]
- [6].St-Vil D, Brandt ML, Panic S, Bensoussan AL, Blanchard H. Meckel's diverticulum in children: a 20-year review. J Pediatr Surg 1991; 26:1289; PMID:1812259; http://dx.doi.org/ 10.1016/0022-3468(91)90601-O [DOI] [PubMed] [Google Scholar]
- [7].Hwang CS, Chu CC, Chen KC, Chen A. Duodenojejunal intussusception secondary to hamartomatous polyps of duodenum surrounding the ampulla of Vater. J Pediatr Surg 2001; 36:1073; PMID:11431783; http://dx.doi.org/ 10.1053/jpsu.2001.24757 [DOI] [PubMed] [Google Scholar]
- [8].Chen Y, Ni YH, Chen CC. Neonatal intussusception due to a cecal duplication cyst. J Formos Med Assoc 2000; 99:352; PMID:10870323 [PubMed] [Google Scholar]
- [9].Khuroo MS. Ascariasis. Gastroenterol Clin North Am 1996; 25:553; PMID:8863040; http://dx.doi.org/ 10.1016/S0889-8553(05)70263-6 [DOI] [PubMed] [Google Scholar]
- [10].Choong CK, Beasley SW. Intra-abdominal manifestations of Henoch-Schönlein purpura. J Paediatr Child Health 1998; 34:405; PMID:9767498; http://dx.doi.org/ 10.1046/j.1440-1754.1998.00263.x [DOI] [PubMed] [Google Scholar]
- [11].Holmes M, Murphy V, Taylor M, Denham B. Intussusception in cystic fibrosis. Arch Dis Child 1991; 66:726; PMID:2053797; http://dx.doi.org/ 10.1136/adc.66.6.726 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Grodinsky S, Telmesani A, Robson WL, Fick G, Scott RB. Gastrointestinal manifestations of hemolytic uremic syndrome: recognition of pancreatitis. J Pediatr Gastroenterol Nutr 1990; 11:518; PMID:1702151; http://dx.doi.org/ 10.1097/00005176-199011000-00013 [DOI] [PubMed] [Google Scholar]
- [13].Bhisitkul DM, Todd KM, Listernick R. Adenovirus infection and childhood intussusception. Am J Dis Child 1992; 146:1331; PMID:1415074 [DOI] [PubMed] [Google Scholar]
- [14].Guarner J, de Leon-Bojorge B, Lopez-Corella E, Ferebee-Harris T, Gooding L, Garnett CT, Shieh WJ, Dawson J, Erdman D, Zaki SR. Intestinal intussusception associated with adenovirus infection in Mexican children. Am J Clin Pathol 2003; 120:845; PMID:14671973; http://dx.doi.org/ 10.1309/LBRNGF9MJW2MHT97 [DOI] [PubMed] [Google Scholar]
- [15].Hsu HY, Kao CL, Huang LM, Ni YH, Lai HS, Lin FY, Chang MH. Viral etiology of intussusception in Taiwanese childhood. Pediatr Infect Dis J 1998; 17:893; PMID:9802631; http://dx.doi.org/ 10.1097/00006454-199810000-00009 [DOI] [PubMed] [Google Scholar]
- [16].Bines JE, Liem NT, Justice FA, Son TN, Kirkwood CD, de Campo M, Barnett P, Bishop RF, Robins-Browne R, Carlin JB. Risk factors for intussusception in infants in Vietnam and Australia: adenovirus implicated, but not rotavirus. J Pediatr 2006; 149:452; PMID:17011313; http://dx.doi.org/ 10.1016/j.jpeds.2006.04.010 [DOI] [PubMed] [Google Scholar]
- [17].Nylund CM, Denson LA, Noel JM. Bacterial enteritis as a risk factor for childhood intussusception: a retrospective cohort study. J Pediatr 2010; 156:761; PMID:20138300; http://dx.doi.org/ 10.1016/j.jpeds.2009.11.026 [DOI] [PubMed] [Google Scholar]
- [18].Murphy TV, Gargiullo PM, Massoudi MS, Nelson DB, Jumaan AO, Okoro CA, Zanardi LR, Setia S, Fair E, LeBaron CW, et al.. Intussusception among infants given an oral rotavirus vaccine. N Engl J Med 2001; 344(8):564-72; PMID:11207352; http://dx.doi.org/ 10.1056/NEJM200102223440804 [DOI] [PubMed] [Google Scholar]
- [19].Ward RL. Mechanisms of protection against rotavirus in humans and mice. J Infect Dis 1996; 174(Suppl 1):S51-8; PMID:8752291; http://dx.doi.org/ 10.1093/infdis/174.Supplement_1.S51 [DOI] [PubMed] [Google Scholar]
- [20].Favaretti C, Di Pietro ML, Kheiraoui F, Capri S, Specchia ML, Cadeddu C, et al.. Health Technology Assessment della vaccinazione anti-rotavirus con il vaccino Rotarix. Available on December 13th, 2016 at http://www.ijph.it/pdf/2014-v3-n7.pdf [Google Scholar]
- [21].Sicilian Health Authority Sicilian vaccination schedule. Modifications and integration to regional vaccination schedule. Available on July 30th, 2016 at http://www.gurs.regione.sicilia.it/Gazzette/g12-23/g12-23.pdf [Google Scholar]
- [22].WHO Information for Policy Makers, Programme Managers, and Health Workers. 2013. Available July 20th, 2016 at http://www.who.int/immunization/monitoring_surveillance/burden/vpd/surveillance_type/sentinel/rotavirus_intro_guidance_who_july31_2013.pdf [Google Scholar]
- [23].Noel G, Minodier P, Merrot T. Intussusception risk after rotavirus vaccination in U.S. infants. N Engl J Med 2014; 370(18):1766; PMID:24785219; http://dx.doi.org/ 10.1056/NEJMc1402790 [DOI] [PubMed] [Google Scholar]
- [24].Costantino C, Restivo V, Cuccia M, Furnari R, Amodio E, Vital F. Analysis of hospitalizations due to intussusception in Sicily in the pre-rotavirus vaccination era (2003-2012). Ital J Pediatr 2015; 1:41-52 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Samad L, Cortina-Borja M, Bashir HE, Sutcliffe AG, Marven S, Cameron JC, Lynn R, Taylor B. Intussusception incidence among infants in the UK and Republic of Ireland: a pre-rotavirus vaccine prospective surveillance study. Vaccine 2013; 31(38):4098-102; PMID:23871447; http://dx.doi.org/ 10.1016/j.vaccine.2013.06.084 [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Sassower KC, Allister LM, Westra SJ. Case records of the Massachusetts General Hospital. Case 12-2012. A 10-month-old girl with vomiting and episodes of unresponsiveness. N Engl J Med 2012; 366:1527; PMID:22512486; http://dx.doi.org/ 10.1056/NEJMcpc1103563 [DOI] [PubMed] [Google Scholar]
- [27].Weihmiller SN, Monuteaux MC, Bachur RG. Ability of pediatric physicians to judge the likelihood of intussusception. Pediatr Emerg Care 2012; 28:136; PMID:22270504 [DOI] [PubMed] [Google Scholar]
- [28].Johnson B, Gargiullo P, Murphy TV, Parashar UD, Patel MM. Sociodemographic and dietary risk factors for natural infant intussusception in the United States. J Pediatr Gastroenterol Nutr 2010; 51(4):458-63; PMID:20562726; http://dx.doi.org/ 10.1097/MPG.0b013e3181d3273f [DOI] [PubMed] [Google Scholar]
- [29].Monsour A, El Koutby M, El Barbary MM, Mohamed W, Shehata S, El Mohammady H, Mostafa M, Riddle MS, Sebeny PJ, Young SY, et al.. Enteric viral infections as potential risk factors for intussusception. J Infect Dev Ctries 2013; 7(1):28-35; PMID:23324817 [DOI] [PubMed] [Google Scholar]
- [30].Robinson CG, Hernanz-Schulman M, Zhu Y, Griffin MR, Gruber W, Edwards KM. Evaluation of anatomic changes in young children with natural rotavirus infection: is intussusception biologically plausible? J Infect Dis 2004; 189:1382-1387; PMID:15073674; http://dx.doi.org/ 10.1086/382655 [DOI] [PubMed] [Google Scholar]
- [31].Obuchowski NA, Goske MJ, Applegate KE. Assessing physicians' accuracy in diagnosing paediatric patients with acute abdominal pain: measuring accuracy for multiple diseases. Stat Med 2001; 20(21):3261-78; http://dx.doi.org/ 10.1002/sim.944 [DOI] [PubMed] [Google Scholar]
- [32].Desai R, Curns AT, Patel MM, Parashar UD. Trends in intussusception-associated deaths among US infants from 1979-2007. J Pediatr 2012; 160(3):456-60; PMID:21925681; http://dx.doi.org/ 10.1016/j.jpeds.2011.08.012 [DOI] [PubMed] [Google Scholar]
- [33].WHO Acute intussusception in infants and children Incidence, clinical presentation and management: a global perspective Geneva: World Health Organization, 2002. 1-98. Document WHO/V & B/02.19. Available August 01, 2016 at http://vaccine-safety-training.org/tl_files/vs/pdf/acute-intussusception-infants-children.pdf [Google Scholar]
- [34].Bratton SL, Haberkern CM, Waldhausen JH, Sawin RS, Allison JW. Intussusception: hospital size and risk of surgery. Pediatrics 2001; 107:299-303; PMID:11158462; http://dx.doi.org/ 10.1542/peds.107.2.299 [DOI] [PubMed] [Google Scholar]
- [35].Losek JD. Intussusception: don't miss the diagnosis! Pediatr Emerg Care 1993; 9:46-51; PMID:8488146; http://dx.doi.org/ 10.1097/00006565-199302000-00014 [DOI] [PubMed] [Google Scholar]
- [36].Belongia EA, Irving SA, Shui IM, Kulldorff M, Lewis E, Yin R, Lieu TA, Weintraub E, Yih WK, Li R, et al.. Real-time surveillance to assess risk of intussusception and other adverse events after pentavalent, bovine-derived rotavirus vaccine. Pediatr Infect Dis J 2010; 29(1):1-5; PMID:19907356; http://dx.doi.org/ 10.1097/INF.0b013e3181af8605 [DOI] [PubMed] [Google Scholar]
- [37].Desai R, Curns AT, Steiner CA, Tate JE, Patel MM, Parashar UD. All-cause gastroenteritis and rotavirus-coded hospitalizations among US children, 2000-2009. Clin Infect Dis 2012; 55(4):e28-34; PMID:22543022; http://dx.doi.org/ 10.1093/cid/cis443 [DOI] [PubMed] [Google Scholar]
- [38].Costantino C, Amodio E, Vitale F. Impact on rotavirus gastro-enteritis hospitalisation during the first year of universal vaccination in Sicily. Paediatr Int Child Health 2015; 35(4):342-3; PMID:26744161; http://dx.doi.org/ 10.1080/20469047.2015.1109240 [DOI] [PubMed] [Google Scholar]
- [39].Vitale F, Tramuto F, Amodio E, Restivo V, Costantino C. Results after one year of rotavirus universal mass vaccination in Sicily. Italian J Pediatr 2015; 41(Suppl 2):A77 [Google Scholar]
- [40].Vitale F, Costantino C, Restivo V, Casuccio N, Corsello G, Palermo M, Tozzo I. Precise reply and clarifications on behalf of Sicilian Public Health Authorities to the case report published by La Rosa and collegues. Hum Vaccin Immunother 2016; 12(11):2969-71. [DOI] [PMC free article] [PubMed] [Google Scholar]