

Abstract
When hematopoietic stem and progenitor cells (HSPC) are harvested for transplantation, either from the bone marrow or from mobilized blood, the graft contains a significant number of T cells. It is these T cells that are the major drivers of graft-vs-host disease (GvHD). The risk for GvHD can simply be reduced by the removal of these T cells from the graft. However, this is not always desirable, as this procedure also decreases the engraftment of the transplanted HSPCs and, if applicable, a graft-vs-tumor effect. This poses an important conundrum in the field: T cells act as a double-edged sword upon allogeneic HSPC transplantation, as they support engraftment of HSPCs and provide anti-tumor activity, but can also cause GvHD. It has recently been suggested that T cells also enhance the engraftment of autologous HSPCs, thus supporting the notion that T cells and HSPCs have an important functional interaction that is highly beneficial, in particular during transplantation. The underlying reason on why and how T cells contribute to HSPC engraftment is still poorly understood. Therefore, we evaluate in this review the studies that have examined the role of T cells during HSPC transplantation and the possible mechanisms involved in their supporting function. Understanding the underlying cellular and molecular mechanisms can provide new insight into improving HSPC engraftment and thus lower the number of HSPCs required during transplantation. Moreover, it could provide new avenues to limit the development of severe GvHD, thus making HSPC transplantations more efficient and ultimately safer.
Keywords: Hematopoietic stem cells, Hematopoietic stem and progenitor cells, CD8 T cells, Transplantation, Engraftment, Memory T cells, Facilitating cells, Bone marrow
Core tip: T cells act as a double-edged sword upon allogeneic hematopoietic stem and progenitor cells (HSPC) transplantation, as they support engraftment of HSPCs and provide anti-tumor activity, but are also the cause of graft-vs-host disease (GvHD). Here, we discuss the findings from several studies that have addressed the still enigmatic role of T cells during HSPC transplantation, either in an allogeneic or autologous setting, in mice or men, and with HSPCs derived from bone marrow, peripheral blood or cord blood. We anticipate that a better comprehension of how T cells support HSPC engraftment may lead to new strategies to optimize HSPCs transplantations and prevent GvHD.
INTRODUCTION
Over the past 60 years, hematopoietic stem cell transplantation (HSCT) has developed into routine treatment for several hematological and immunological malignancies and deficiencies. Hematopoietic stem cells (HSCs) are the rare, self-renewing progenitor cells at the top of the hematopoietic hierarchy that can give rise to all blood cell lineages, and are thus able to restore hematopoiesis and the immune system in transplanted recipients. Hematopoietic stem and progenitor cells (HSPCs) are a mixture of HSCs and more differentiated progenitor cells, which provide respectively long and short-term repopulation of blood cells following transplantation. In the past, HSPCs required for transplantation were solely acquired from the bone marrow (BM), typically from the hipbone. This is an invasive procedure and if the BM harvest was not optimal, this often resulted in reduced engraftment of HSPCs and limited hematopoietic/immunologic recovery. Transplantation of higher doses resolved the majority of engraftment problems. Nowadays, this is facilitated by more favorable and less invasive HSPC harvesting procedures from mobilized peripheral blood (MPB) or umbilical cord blood (UCB). In the case of MPB HSPCs, donors are usually pretreated with granulocyte colony-stimulating factor (G-CSF), which mobilizes the HSPCs from the BM into the blood stream[1,2]. Subsequently, donors undergo one or two apheresis sessions to reach the desired HSPC dose for transplantation, normally 2-10 × 106 CD34+ cells/kg recipient body weight[3-5]. In case of UCB HSPCs, the UCB is collected from the postpartum placenta, as this is a rich source of HSPCs. Typically, two grafts are required to reach sufficient numbers of UCB HSPCs when transplanting an adult. UCB HSPC transplants are generally used in an allogeneic transplantation setting, whereas mobilized HSPCs are used both during autologous and allogeneic HSCT. Autologous HSCT following high-dose chemotherapy has become routine treatment for many types of lymphomas[6]. It is considered a relatively low risk treatment, as the recipients receive their own HSPCs that were harvested before the chemotherapy was started. Allogeneic HSCT is regarded as a more precarious procedure, as HSPCs from a non-self origin are transplanted, which are thus subject to rejection by the host. In addition, allogeneic HSCT is combined with conditioning regimes of different intensity, leading to more variable transplantation outcomes. As with any allogeneic transplantation, matching of the human leukocyte antigen (HLA)-profile between donor and patient is instrumental to lower the risks of graft rejection. The first step in finding a suitable donor is to search within the immediate family. Related siblings have a 25% chance of being perfect donors, i.e., matching 10 out of the 10 HLA antigens. Unrelated donors can also match the HLA antigens perfectly, although the chance of finding a perfectly HLA-matched, unrelated donor in a timely manner is much lower. Transplantation with partially matched (haploidentical), related donors (parent, child or sibling) is now considered as a viable alternative. Although these donors are usually more readily available, haploidentical donors have more HLA-disparities when compared to the recipient. This increases the risk of graft rejection, but also the development of graft-vs-host disease (GvHD)[7]. GvHD is a complicating side effect of an allogeneic HSPC transplantation that can develop early or late after the transplantation, in which transplanted donor T cells mount an extensive immune response against the recipient’s tissues. A mild degree of GvHD is considered beneficial when the HSPC transplantation is part of an anti-cancer treatment, as the allo-responsive donor T cells in the graft can also eradicate the remaining tumor cells present in the recipient. However, severe forms of GvHD are very hazardous and hence the predominant cause of the high morbidity and mortality rate associated with allogeneic HSPC transplantations. A highly efficient procedure to minimize the risk of developing acute and chronic GvHD is T cell depletion (TCD) from donor grafts[8]. Unfortunately, transplantations with TCD grafts also revealed major pitfalls, such as graft failure and disease relapse. This was observed in BM transplants with grafts from HLA-identical siblings and HLA-non-identical (but related) donors with minimal mismatch[8,9]. What was apparent from these studies is that conditioning regimes and post-transplant immune suppression treatments can all affect the outcome of transplantation with TCD grafts. To this day, it is still unclear how the depletion of T cells leads to increased risk of graft failure. What is certain is that T cells can aid the engraftment of HSPCs in the damaged BM environment in which they find themselves post-transplant. Here, we review what is currently known about the contribution of T cells on HSPC engraftment in different transplantation settings, as this knowledge can be used to improve both the efficiency and safety of this important clinical procedure.
FACILITATING T CELLS
While grafts depleted of T cells minimize the risk of developing GvHD, T cell depletion also compromises the engraftment of transplanted HSPCs. This unwanted effect has been attributed to the loss of specific cell subsets that assist the engraftment, the so-called facilitating cells (FC) that were depleted during the T cell depletion process. In 1994, Kaufman et al[10] showed for the first time that engraftment of murine BM HSPCs was facilitated by BM cells that were positive for CD8, CD45, CD45R, CD3, dull/intermediate for MHC class II and negative for the TCR. The absence of the TCR indicates that these cells are not T cells. However, some discrepancy does exist regarding this finding. Gandy et al[11] observed increased survival of mice transplanted with allogeneic HSPCs together with BM CD8+ cells. When separated into TCRβ+ and TCRβ- fractions, both CD8+ TCRβ+ and CD8+ TCRβ- cells had the ability to enhance survival of transplanted mice. The TCRβ+ population displayed morphology resembling T lymphocytes. The majority of the TCRβ- cells had granular cytoplasm and low nuclear to cytoplasm ratio with a lymphoid dendritic cell phenotype. Further examination on the CD8+ TCRβ+ cells, which are predominately present in the BM, revealed that they express CD44[11]. This indicates that these T cells have a memory phenotype. In the BM, three different subsets of CD8+ T cells co-exist; effector memory (TEM; CD44+ CD62L−), central memory (TCM; CD44+ CD62L+) and naïve T cells (TNV; CD44− CD62L+)[12]. We recently showed that the frequency of total CD8+ T cells is similar within the different bones found throughout the murine body. Additionally, we observed that during steady state conditions, TNV cells are the dominant subset and that this quickly changes after an acute infection with lymphocytic choriomeningitis virus, as the TEM cells replace the TNV cells[13]. Also in humans, it has been shown that CD8+ cells are important for HSPC engraftment. Martin et al[14] demonstrated that removal of CD8+ cells but not CD4+ cells from donor bone marrow grafts results in graft failure. Interestingly, they also showed that the dose of the CD8+ cells in the grafts is of major importance as more than half of the patients that received grafts containing less than 3.9 × 106 CD8+ cells/kg experienced graft failure. They further observed that the high dose of CD8+ cells required to prevent graft rejection also increases the risk for acute and chronic GvHD[14]. Taken together, many studies in mice and human have quite clearly shown that CD8+ T cells have a beneficial effect during HSCT. This in itself is surprising given the fact that T cells, depending on their activation state, are known to have a strong skewing impact on hematopoiesis. We and many others have shown that activated T cells can directly affect HSC function by increasing differentiation and limiting self-renewal[15]. Interferon-gamma (IFN-γ) is one of the pro-inflammatory cytokines produced by activated T cells, which can inhibit HSC self-renewal and enhance their differentiation in a direct manner[16,17], but also indirectly by acting on surrounding niche cells[18,19]. This indicates that the impact that T cells can have on the behavior and function of HSPCs is complex and not only dependent on the T cell subset, but also on the activation status of the T cells and the niche cells they interact with.
THE INFLUENCE OF T CELLS ON HSPC ENGRAFTMENT DURING ALLOGENEIC AND AUTOLOGOUS TRANSPLANTATION
Although early studies demonstrated a clear contribution of CD8+ T cells on HSPC engraftment, this concept received surprisingly limited follow-up, both scientifically and clinically. This is most likely due to the fact that current transfusion protocols are performed with high numbers of HSPCs, which compensates for any suboptimal engraftment condition[14]. Nonetheless, understanding how to optimize the engraftment potential of HSPCs is still desirable, especially when HSPC numbers are limited. We therefore also took into account studies that investigated which T cell subsets are involved in the development of GvHD. The majority of these studies did not examine HSPC engraftment per se, but do provide interesting clues on which T cell subsets may be beneficial for this process, as they did assess immune reconstitution after transplantation. Chen et al[20] depleted CD62L+ T cells (TNV and TCM) from murine BM grafts and found that CD62L- T cells (TEM) accelerated the recovery of CD4+ and CD8+ T cells after transplantation, which could indicate enhanced hematopoietic engraftment. In addition, transplantation of the TEM subset alone did not result in GvHD, while grafts that still included TNV and TCM did. Another interesting observation made is that transplantation of CD62L- T cells led to increased donor chimerism, as it lowered the numbers of residual recipient T cells[20]. Similar results were obtained in human studies. Naïve human T cells express CD45RA and switch to the CD45RO isoform upon antigen encounter and develop into memory T cells. Touzot et al[21] demonstrated that allogeneic HLA-mismatched HSCT with CD45RA-depleted BM grafts were successful and did not lead to severe GvHD, suggesting that this could be a potential approach to treat patients with primary combined immuno–deficiencies. Importantly, they also observed that viruses detected prior to the HSCT were rapidly cleared post-HSCT, indicating that the CD45RA-depleted graft contained CD8+ T cells functionally active against pathogens. Furthermore, Triplett et al[22] found similar results when transplanting patients suffering from hematological malignancy with haploidentical CD45RA-depleted grafts. Here, patients received on day 0 G-CSF MPB grafts that was highly enriched for CD34+ cells and thus depleted of CD3+ cells, with a median dose of 11.2 and 0.012 × 106/kg, respectively). On day 1 patients received MPB grafts depleted of CD45RA+ T cells (and thus enriched for memory T cells), and on day 6, they received an infusion with purified NK cells from the same donor[22]. The authors demonstrated that this combination of differently prepared grafts led to rapid neutrophil engraftment, quick conversion to full donor chimerism and fast reconstitution of innate and adaptive immunity. These three clinical parameters signify rapid HSPC engraftment, which may well have been the result of the co-injected CD45RO+ memory T cells on day 1, although this was not formally tested in this study. Importantly, none of the patients developed acute GvHD. Several patients did show signs of chronic oral GvHD, but not of severe nature[22]. Next to removing specific subsets that might cause GvHD, many studies also focused on adding back T cells after transplantation. The transfer of donor T cells after transplantation has in fact become a frequently applied clinical procedure, called donor lymphocyte infusion (DLI). This is usually performed to cause a milder and more controllable degree of GvHD, aiming for the donor T cells to eliminate residual recipient cells and thereby improve donor chimerism and/or remove residual tumor cells (graft-vs-tumor effect). For DLI, peripheral blood is donated by the same HSPC-donor, this time without G-CSF pre-treatment. Next, CD3+ cells are isolated and given to the patient after a brief recovery period after the initial HSCT[23]. A study performed in mice found that DLI was able to improve engraftment of HSC without resulting in GvHD[24]. They observed that mice, which had received low (sub-lethal) dose of irradiation, rejected allogeneic donor BM cells, unless this procedure was combined with an injection of peripheral blood mononuclear cells. Further analysis revealed that CD8+ cells were facilitating the engraftment. Importantly, this beneficial effect was only observed when the DLI was given on the same or the following day, but not on third or seventh day of the HSCT[24]. This suggests that early DLI may be sufficient to counteract the beginning of an anti-donor response by boosting HSPC engraftment. Interestingly, a study in humans did not show similar effect of DLI; Kreiter et al[25] found that minimal conditioning prior to T cell-reduced allogeneic HSCT combined with subsequent DLI was insufficient to sustain long-term engraftment. This study, similar to Nakamura’s study, gave DLI on the same day as the HSCT. However, the fact that none of the transplanted subjects reached complete donor T cell chimerism indicates that this specific combination of minimal conditioning and DLI dose was not optimal[25]. In contrast to the mice in Nakamura’s study, these human subjects were patients suffering from hematological malignancies. It remains to be determined if and how the conditioning regimes and the presence of disease affect the possible facilitating role of DLI on HSPC engraftment. Interestingly, also in a DLI setting, infusion of T cells depleted of naïve T cells was shown to favor engraftment without causing GvHD[26]. Additional investigation on the murine CD62L- T cell subset originally described by Chen et al[20] revealed that addition of 1 × 106 CD62L- T cells could rescue 90% of graft rejection that developed after transplantation with TCD grafts in mice. The CD62L- T cell subset was also shown to prevent tumor growth and help combat viral infection[26]. More importantly, addition of CD62L- T cells resulted in 100% donor chimerism within 30 d and was maintained long-term. Similar results were obtained in human studies, as Shook et al[27] transplanted patients with CD3+-depleted haploidentical grafts and infused CD45RA-depleted cells the following day. They observed that all patients reached complete donor chimerism. In this study patients received myeloablative conditioning. Remarkably, 3 mo after the HSCT, the majority of CD4+ and CD8+ T cells were still CD45RA-, indicating that the T cells were derived from the CD45RA-depleted grafts[27]. DLIs can also be given to patients not responding to anti-viral medication during an infection post HSCT. This is particularly important after HSCT with T cell-depleted grafts, as protective immunity is not transferred in this setting and engraftment, and thus immune reconstitution is delayed. Stemberger et al[28] demonstrated that as few as 3750 antigen-specific T cells per kg body weight was sufficient to decrease viral load in a patient suffering from systemic CMV infection after CD3-depleted HSCT[28]. In this study, the impact on HSPC engraftment was not reported. Nevertheless, this study highlights a feasible strategy to combat persisting infections post HSCT. So far, the facilitating role of CD8+ T cells, especially memory T cells in HSPC engraftment has been well established in allogeneic HSCT setting. Less explored is if these cells have similar effects in autologous HSCT. Interestingly, Rutella et al[29] demonstrated that patients undergoing autologous transplantation with selected CD34+ cells instead of unmanipulated PBMCs experienced delayed repopulation of the T cell lineage. This suggests that the lack of T cells might also affect engraftment in an autologous setting. Furthermore, Russell et al[30] assessed mobilization and engraftment in autologous donors. They observed that grafts with low numbers of CD34+ cells (poor mobilizers) contain more CD8+ T cells than grafts from moderate or high mobilizers. Subsequently, they assessed if the CD8+ T cell content was associated with time to neutrophil engraftment after HSPCT. The results obtained suggest that engraftment occurs faster when there are more CD8+ T cells present in the grafts. This was limited to grafts that contain low numbers of CD34+ cells[30]. Taken together, these studies show that when HSPC numbers are limiting, memory CD8+ T cells have a beneficial effect on HSPC engraftment, both in allogeneic and autologous transplantation. The effects of different (graft) treatments on HSCT are summarized in Table 1.
Table 1.
Effects of (graft) treatments on hematopoietic stem cell transplantation
| Treatment | Removed | Remaining | Effect |
| Complete T cell depletion | All T cells | N/A | GvHD ↓[8,14,44] |
| Disease relapse ↑[8,9,44] | |||
| Graft failure ↑[8,9,44] | |||
| Immune reconstitution ↑[44] | |||
| Partial T cell depletion | CD45RA (TNV) | CD45RO (TMEM) | GvHD ↓[20,21,22] |
| CD62L+ (TNV, TCM)1 | CD62L- (TEM)1 | Neutrophil engraftment ↑[22] | |
| Immune reconstitution ↑[20] | |||
| Protective immunity ↑[21,22] | |||
| Donor chimerism ↑[20,22] | |||
| Donor lymphocyte infusion | CD45RA (TNV) | CD45RO (TMEM) | GvHD ↓[26] |
| CD62L+ (TNV, TCM)1 | CD62L- (TEM)1 | Tumor growth ↓[26] | |
| Engraftment ↑[26] | |||
| Graft failure ↓[26] | |||
| Immune reconstitution ↑[26] | |||
| Protective immunity ↑[26,28] | |||
| Donor chimerism ↑[26,27] |
Signifies the murine equivalent of the human T cell subset described above. Here, we summarize the impact that either full or partial T cell depletion of an HSPC graft, or selective donor lymphocyte infusion, can have on the clinical outcome of a HSPC transplantation. Indicated are the T cell subsets that have either been removed or that remain, and the biological or clinical effects that have been reported following this treatment. N/A: Not available; HSPC: Hematopoietic stem and progenitor cell; GvHD: Graft-vs-host disease.
THE ROLE OF T CELLS UPON TRANSPLANTATION OF HSPCS FROM UMBILICAL CORD BLOOD
In the clinic, when an HLA-matched sibling and unrelated matched donor are not available, the next best option is HSCT with UCB. It is now well established that transplantation with UCB grafts results in lower rates of GvHD disease when compared to HSCT from BM or MPB. This in itself is very interesting, especially as the majority of the T cells present in a UCB graft are CD45RA+[31], and thus potentially capable of inducing GvHD. However, these CD45RA+ UCB T cells are functionally distinct and less mature than CD45RA+ naïve T cells found in adults[32], explaining why these cells are less related to the development of GvHD. T cells in UCB have the ability to respond to allogeneic stimulation, but the response generated is less cytotoxic than that of adult T cells. Additionally, dendritic cells present in UBC have been found to be in an immature state and thus limiting the activation of UCB T cells[32]. Nevertheless, while the development of GvHD is reduced, patients who undergo UCBT are subjected to high incidence of infection, as immune reconstitution is slow. It is believed that the low numbers of HSPCs and downstream progenitors transplanted during UCBT compared to MPB HSCT are the cause of the delay in hematopoietic reconstitution, while the absence of memory T cells would render the recipient more sensitive to viral infections. However, following our line of reasoning, the lack of memory T cells during UCBT might contribute to impaired HSPC engraftment. Currently, the focus on improving engraftment has been on reducing conditioning regimes, performing double UCB transplantation, ex vivo expansion of UCB HSPCs and intra-bone infusion of UCB grafts[31]. An interesting approach is the combination of UCB grafts with CD34+ cells isolated from haploidentical grafts[33]. The idea behind this concept is that the haploidentical graft will provide early engraftment, while the UCB graft provides long-term engraftment. Indeed, the authors observed fast engraftment of neutrophils and platelets post haplo-cord SCT. Furthermore, UCB cells replaced this first wave of hematopoiesis by the haploidentical CD34+ cells within 100 d. An important future aspect of this approach is that not the cell number of the UCB graft but rather the matching of the HLA type to that of the patient will take priority when finding suitable UCB grafts for UCBT. This by itself will provide more options for adult patients lacking related and unrelated HLA matched donors.
POSSIBLE UNDERLYING MECHANISMS ON HOW CD8+ T CELLS IMPROVE ENGRAFTMENT OF HSPCS
The underlying reasons on why and how CD8+ T cells contribute to HSPC engraftment are still poorly understood. Currently, there are more questions than answers, which we will address here; the mechanisms discussed below are depicted in Figure 1. For example, do donor T cells contribute to engraftment by killing residual host HSPC and thus eliminating the competition? This is unlikely, as Gandy et al[11] showed that CD8+ T cells did not facilitate HSPC engraftment via their lytic potential, as CD8+ T cells deficient in their lytic activity were still able to assist engraftment. However, one of the most important observations made by several studies is that the addition of donor T cells eliminates residual host T cells in mice[20,24,26]. These observations suggest that removal of residual host T cells is an essential part in eliminating any type of resistance from the host to allow engraftment. Furthermore, is it possible that donor T cells somehow directly affect the function of HSPCs? An interesting observation made by Adams and colleagues is that in the β2m-/-NOD/SCID mice, CD8+ cells augmented homing and engraftment of CD34+ cells by modulating their response towards CXCL12 by affecting their phosphotyrosine-mediated signaling. Ex vivo, this modulated response towards CXCL12 resulted in increased migration through a BM endothelial cell line[34]. Further analysis revealed that this was not the result of factors secreted by CD8+ cells, though an active cytoskeleton in the CD8+ cells was required for the increased transmigration of CD34+ cells[34]. Moreover, it could also be that CD8+ T cells can affect the HSC niche by making the environment more favorable for engraftment of the newly arrived HSPCs. The production of IFN-γ by CD8+ T cells was shown to promote the release of interleukin-6 from mesenchymal stromal cells (MSCs), an essential component of the HSC niche[18]. This enhanced myeloid differentiation of more committed progenitors, though the impact of T cell-modulated MSCs on HSPC engraftment has not been examined. Lastly, an intriguing question on the functional impact of CD8+ T cells on HSCT is whether CD8+ T cells and HSCs co-localize in the BM. It has been shown that memory CD8+ T cells co-localize with VCAM-1-expressing stromal cells in BM[35], whereas HSC-supporting MSCs also express VCAM-1[36,37]. These findings are compatible with the hypothesis that HSCs and CD8+ memory T cells share the same niche, though actual co-localization between these cells has not yet been experimentally demonstrated.
Figure 1.
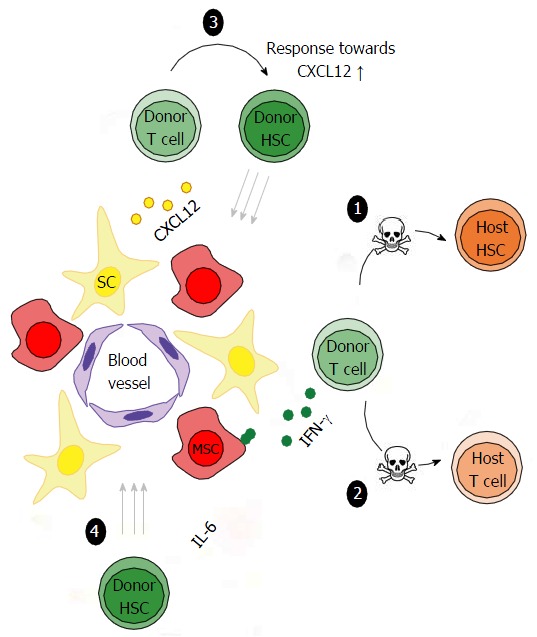
Potential mechanisms on how CD8+ T cells improve hematopoietic stem and progenitor cells engraftment. The following modes of action have been described or suggested by which donor T cells can support the engraftment of HSPCs upon transplantation: (1) killing of residual host HSPCs; (2) killing of residual host T cells; (3) augmented homing of HSPCs to CXCL12 produced by reticular SC or MSCs; (4) increased HSPC differentiation by IFN-γ-induced production of IL-6 by MSCs. HSPCs: Hematopoietic stem and progenitor cells; SC: Stromal cells; MSCs: Mesenchymal stromal cells; IFN-γ: Interferon-gamma; IL-6: Interleukin-6.
THE IMPACT OF OTHER FACILITATING CELL TYPES ON HSPC ENGRAFTMENT
Although the positive impact of CD8+ T cells on HSPC engraftment has been addressed most extensively, there is evidence that other cell types in the BM can also have this effect. As mentioned before, not all CD8+ cells that can facilitate HSPC engraftment also express the TCR[10]. In follow-up of these findings, Grimes et al[38] found that CD8+TCR- FC do not express TCR gene transcripts (TCRα and TCRβ), clearly distinguishing them from conventional T cells. Furthermore, they showed that CD8+TCR- FC do express CD3ε and that this complex is important for the beneficial effect of these cells during allogeneic transplantation[38]. Further gene expression analysis on the CD8+TCR- FC revealed that the DOCK2 gene was most significantly different between functional and functionally impaired FC cells. Indeed, FCs lacking the expression of DOCK2 do not enhance engraftment and do not promote homing and lodgment of HSPCs in the bone marrow[39]. Additionally, also human CD3+CD8+TCR- cells have been shown have facilitating potential when co-transplanted with suboptimal doses (3-5 × 104) of UCB CD34+ cells in NOD/SCID mice[40].
Next to CD8+ T cells, multiple studies have shown that CD4+ T cells, especially regulatory T cells (Tregs) can also support HSPC engraftment. Danby and colleagues showed that higher proportions of Tregs in MPB grafts improve recovery and clinical outcomes[41]. It has also been demonstrated that host Tregs co-localize with transplanted allo-HSPCs in BM[42], indicating that these cells may provide an immune privilege site for HSPCs in the BM. Furthermore, also TCRγδ+ T cells have gained recognition for their facilitating role in engraftment of HSPCs. Kawanishi et al[43] found that engraftment was associated with the dose of TCRγδ+ T cells present in BM grafts. Importantly, they found no association between the TCRγδ+ T cells dose and an increased risk for the development of acute GvHD in patients that received grafts from related donors[43]. In conclusion, it is clear that the BM contains multiple cell types that can enhance HSPC engraftment. This is highly relevant from a clinical perspective, though it remains unclear to what extent these cell types also support the function or maintenance of HSPCs in the BM under physiological conditions.
FUTURE PERSPECTIVES
After decades of development in the allogeneic HSCT field, GvHD is still a major complication. To this day, the best approach for decreasing the risk for GvHD is the removal of T cells from the graft. After it was apparent that TCD procedure led to poor engraftment, delayed immune reconstitution and increased disease relapse[44], TCD procedures were dismayed as a reliable method to safely and efficiently combat GvHD. However, several studies discussed here suggest that future of TCD HSCT may lie in partial instead of complete depletion of T cells. The aim of the variety of the approaches attempted so far was to remove T cells that contribute to GvHD while maintaining T cells that provide immediate but also long-term immune protection. The focus has never necessarily been to improve engraftment of HSPCs, as this potential problem is covered by the immense amounts of HSPCs transplanted. Nevertheless, identifying T cell subsets that specifically favor HSPC engraftment and the underlying mechanism may be more beneficial in the long run, as more efficient and rapid engraftment will be required if less and less intense conditioning regimes are used in the future. Moreover, efficiency of HSPC transplantation is significantly reduced when donor HSPCs numbers are limited or when HSPCs are genetically modified, which thus requires protocols in which their engraftment is fully optimized. More in depth studies are required to determine whether the future of allogeneic HSCT can/will develop into one where patients receive minimal conditioning with a low dose of HSPCs followed by multiple infusions of different T cells subsets; these could be chosen based on their ability to improve HSPC engraftment, to provide the first wave of protective immunity and/or to induce a low-grade level of GvHD to boost an anti-tumor response. Unpublished work from our group suggests that ex vivo expanded CD8+ T cells with a memory phenotype have facilitating potential at the level of HSPC engraftment. It is hence interesting to speculate that the future of transplantation may include the addition of ex vivo expanded T cells from the graft in order to enhance engraftment and immune reconstitution. Hopefully, the developments in HSCT treatment in the coming years will results in faster recovery, decrease disease relapse and overall shorter hospital stays.
ACKNOWLEDGMENTS
We thank Dr. Carlijn Voermans for critical reading of the manuscript.
Footnotes
Manuscript source: Invited manuscript
Specialty type: Cell and tissue engineering
Country of origin: The Netherlands
Peer-review report classification
Grade A (Excellent): A, A
Grade B (Very good): B
Grade C (Good): C
Grade D (Fair): 0
Grade E (Poor): 0
Conflict-of-interest statement: Authors declare no conflict of interest for this article.
Peer-review started: August 26, 2016
First decision: November 17, 2016
Article in press: January 14, 2017
P- Reviewer: Cao T, Wakao H, Wang L, Yao CL S- Editor: Kong JX L- Editor: A E- Editor: Li D
References
- 1.Scheding S, Brugger W, Mertelsmann R, Kanz L. Peripheral blood stem cells: in vivo biology and therapeutic potential. Stem Cells. 1994;12 Suppl 1:203–210; discussion 211. doi: 10.1002/stem.5530120717. [DOI] [PubMed] [Google Scholar]
- 2.Bensinger WI, Clift RA, Anasetti C, Appelbaum FA, Demirer T, Rowley S, Sandmaier BM, Torok-Storb B, Storb R, Buckner CD. Transplantation of allogeneic peripheral blood stem cells mobilized by recombinant human granulocyte colony stimulating factor. Stem Cells. 1996;14:90–105. doi: 10.1002/stem.140090. [DOI] [PubMed] [Google Scholar]
- 3.Mohty M, Bilger K, Jourdan E, Kuentz M, Michallet M, Bourhis JH, Milpied N, Sutton L, Jouet JP, Attal M, et al. Higher doses of CD34+ peripheral blood stem cells are associated with increased mortality from chronic graft-versus-host disease after allogeneic HLA-identical sibling transplantation. Leukemia. 2003;17:869–875. doi: 10.1038/sj.leu.2402909. [DOI] [PubMed] [Google Scholar]
- 4.Duong HK, Savani BN, Copelan E, Devine S, Costa LJ, Wingard JR, Shaughnessy P, Majhail N, Perales MA, Cutler CS, et al. Peripheral blood progenitor cell mobilization for autologous and allogeneic hematopoietic cell transplantation: guidelines from the American Society for Blood and Marrow Transplantation. Biol Blood Marrow Transplant. 2014;20:1262–1273. doi: 10.1016/j.bbmt.2014.05.003. [DOI] [PubMed] [Google Scholar]
- 5.Czerw T, Labopin M, Schmid C, Cornelissen JJ, Chevallier P, Blaise D, Kuball J, Vigouroux S, Garban F, Lioure B, et al. High CD3+ and CD34+ peripheral blood stem cell grafts content is associated with increased risk of graft-versus-host disease without beneficial effect on disease control after reduced-intensity conditioning allogeneic transplantation from matched unrelated donors for acute myeloid leukemia - an analysis from the Acute Leukemia Working Party of the European Society for Blood and Marrow Transplantation. Oncotarget. 2016;7:27255–27266. doi: 10.18632/oncotarget.8463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Holmberg L, Maloney DG. The role of autologous and allogeneic hematopoietic stem cell transplantation for Hodgkin lymphoma. J Natl Compr Canc Netw. 2011;9:1060–1071. doi: 10.6004/jnccn.2011.0087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Spitzer TR. Haploidentical stem cell transplantation: the always present but overlooked donor. Hematology Am Soc Hematol Educ Program. 2005:390–395. doi: 10.1182/asheducation-2005.1.390. [DOI] [PubMed] [Google Scholar]
- 8.Marmont AM, Horowitz MM, Gale RP, Sobocinski K, Ash RC, van Bekkum DW, Champlin RE, Dicke KA, Goldman JM, Good RA. T-cell depletion of HLA-identical transplants in leukemia. Blood. 1991;78:2120–2130. [PubMed] [Google Scholar]
- 9.Ash RC, Horowitz MM, Gale RP, van Bekkum DW, Casper JT, Gordon-Smith EC, Henslee PJ, Kolb HJ, Lowenberg B, Masaoka T. Bone marrow transplantation from related donors other than HLA-identical siblings: effect of T cell depletion. Bone Marrow Transplant. 1991;7:443–452. [PubMed] [Google Scholar]
- 10.Kaufman CL, Colson YL, Wren SM, Watkins S, Simmons RL, Ildstad ST. Phenotypic characterization of a novel bone marrow-derived cell that facilitates engraftment of allogeneic bone marrow stem cells. Blood. 1994;84:2436–2446. [PubMed] [Google Scholar]
- 11.Gandy KL, Domen J, Aguila H, Weissman IL. CD8+TCR+ and CD8+TCR- cells in whole bone marrow facilitate the engraftment of hematopoietic stem cells across allogeneic barriers. Immunity. 1999;11:579–590. doi: 10.1016/s1074-7613(00)80133-8. [DOI] [PubMed] [Google Scholar]
- 12.Sallusto F, Geginat J, Lanzavecchia A. Central memory and effector memory T cell subsets: function, generation, and maintenance. Annu Rev Immunol. 2004;22:745–763. doi: 10.1146/annurev.immunol.22.012703.104702. [DOI] [PubMed] [Google Scholar]
- 13.Geerman S, Hickson S, Brasser G, Pascutti MF, Nolte MA. Quantitative and Qualitative Analysis of Bone Marrow CD8(+) T Cells from Different Bones Uncovers a Major Contribution of the Bone Marrow in the Vertebrae. Front Immunol. 2015;6:660. doi: 10.3389/fimmu.2015.00660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Martin PJ, Rowley SD, Anasetti C, Chauncey TR, Gooley T, Petersdorf EW, van Burik JA, Flowers ME, Storb R, Appelbaum FR, et al. A phase I-II clinical trial to evaluate removal of CD4 cells and partial depletion of CD8 cells from donor marrow for HLA-mismatched unrelated recipients. Blood. 1999;94:2192–2199. [PubMed] [Google Scholar]
- 15.Libregts SF, Nolte MA. Parallels between immune driven-hematopoiesis and T cell activation: 3 signals that relay inflammatory stress to the bone marrow. Exp Cell Res. 2014;329:239–247. doi: 10.1016/j.yexcr.2014.09.016. [DOI] [PubMed] [Google Scholar]
- 16.de Bruin AM, Demirel Ö, Hooibrink B, Brandts CH, Nolte MA. Interferon-γ impairs proliferation of hematopoietic stem cells in mice. Blood. 2013;121:3578–3585. doi: 10.1182/blood-2012-05-432906. [DOI] [PubMed] [Google Scholar]
- 17.Matatall KA, Shen CC, Challen GA, King KY. Type II interferon promotes differentiation of myeloid-biased hematopoietic stem cells. Stem Cells. 2014;32:3023–3030. doi: 10.1002/stem.1799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Schürch CM, Riether C, Ochsenbein AF. Cytotoxic CD8+ T cells stimulate hematopoietic progenitors by promoting cytokine release from bone marrow mesenchymal stromal cells. Cell Stem Cell. 2014;14:460–472. doi: 10.1016/j.stem.2014.01.002. [DOI] [PubMed] [Google Scholar]
- 19.McCabe A, Zhang Y, Thai V, Jones M, Jordan MB, MacNamara KC. Macrophage-Lineage Cells Negatively Regulate the Hematopoietic Stem Cell Pool in Response to Interferon Gamma at Steady State and During Infection. Stem Cells. 2015;33:2294–2305. doi: 10.1002/stem.2040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Chen BJ, Cui X, Sempowski GD, Liu C, Chao NJ. Transfer of allogeneic CD62L- memory T cells without graft-versus-host disease. Blood. 2004;103:1534–1541. doi: 10.1182/blood-2003-08-2987. [DOI] [PubMed] [Google Scholar]
- 21.Touzot F, Neven B, Dal-Cortivo L, Gabrion A, Moshous D, Cros G, Chomton M, Luby JM, Terniaux B, Magalon J, et al. CD45RA depletion in HLA-mismatched allogeneic hematopoietic stem cell transplantation for primary combined immunodeficiency: A preliminary study. J Allergy Clin Immunol. 2015;135:1303–1309.e1-3. doi: 10.1016/j.jaci.2014.08.019. [DOI] [PubMed] [Google Scholar]
- 22.Triplett BM, Shook DR, Eldridge P, Li Y, Kang G, Dallas M, Hartford C, Srinivasan A, Chan WK, Suwannasaen D, et al. Rapid memory T-cell reconstitution recapitulating CD45RA-depleted haploidentical transplant graft content in patients with hematologic malignancies. Bone Marrow Transplant. 2015;50:968–977. doi: 10.1038/bmt.2014.324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kolb HJ, Schattenberg A, Goldman JM, Hertenstein B, Jacobsen N, Arcese W, Ljungman P, Ferrant A, Verdonck L, Niederwieser D, et al. Graft-versus-leukemia effect of donor lymphocyte transfusions in marrow grafted patients. Blood. 1995;86:2041–2050. [PubMed] [Google Scholar]
- 24.Nakamura K, Inaba M, Sugiura K, Yoshimura T, Kwon AH, Kamiyama Y, Ikehara S. Enhancement of allogeneic hematopoietic stem cell engraftment and prevention of GVHD by intra-bone marrow bone marrow transplantation plus donor lymphocyte infusion. Stem Cells. 2004;22:125–134. doi: 10.1634/stemcells.22-2-125. [DOI] [PubMed] [Google Scholar]
- 25.Kreiter S, Winkelmann N, Schneider PM, Schuler M, Fischer T, Ullmann AJ, Huber C, Derigs HG, Kolbe K. Failure of sustained engraftment after non-myeloablative conditioning with low-dose TBI and T cell-reduced allogeneic peripheral stem cell transplantation. Bone Marrow Transplant. 2001;28:157–161. doi: 10.1038/sj.bmt.1703107. [DOI] [PubMed] [Google Scholar]
- 26.Zhang J, Barefoot BE, Mo W, Deoliveira D, Son J, Cui X, Ramsburg E, Chen BJ. CD62L- memory T cells enhance T-cell regeneration after allogeneic stem cell transplantation by eliminating host resistance in mice. Blood. 2012;119:6344–6353. doi: 10.1182/blood-2011-03-342055. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Shook DR, Triplett BM, Eldridge PW, Kang G, Srinivasan A, Leung W. Haploidentical stem cell transplantation augmented by CD45RA negative lymphocytes provides rapid engraftment and excellent tolerability. Pediatr Blood Cancer. 2015;62:666–673. doi: 10.1002/pbc.25352. [DOI] [PubMed] [Google Scholar]
- 28.Stemberger C, Graef P, Odendahl M, Albrecht J, Dössinger G, Anderl F, Buchholz VR, Gasteiger G, Schiemann M, Grigoleit GU, et al. Lowest numbers of primary CD8(+) T cells can reconstitute protective immunity upon adoptive immunotherapy. Blood. 2014;124:628–637. doi: 10.1182/blood-2013-12-547349. [DOI] [PubMed] [Google Scholar]
- 29.Rutella S, Rumi C, Laurenti L, Pierelli L, Sora’ F, Sica S, Leone G. Immune reconstitution after transplantation of autologous peripheral CD34+ cells: analysis of predictive factors and comparison with unselected progenitor transplants. Br J Haematol. 2000;108:105–115. doi: 10.1046/j.1365-2141.2000.01824.x. [DOI] [PubMed] [Google Scholar]
- 30.Russell A, Malik S, Litzow M, Gastineau D, Roy V, Zubair AC. Dual roles of autologous CD8+ T cells in hematopoietic progenitor cell mobilization and engraftment. Transfusion. 2015;55:1758–1765; quiz 1757. doi: 10.1111/trf.13073. [DOI] [PubMed] [Google Scholar]
- 31.Danby R, Rocha V. Improving engraftment and immune reconstitution in umbilical cord blood transplantation. Front Immunol. 2014;5:68. doi: 10.3389/fimmu.2014.00068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Szabolcs P. The immunobiology of cord blood transplantation. Korean J Hematol. 2010;45:224–235. doi: 10.5045/kjh.2010.45.4.224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Liu H, Rich ES, Godley L, Odenike O, Joseph L, Marino S, Kline J, Nguyen V, Cunningham J, Larson RA, et al. Reduced-intensity conditioning with combined haploidentical and cord blood transplantation results in rapid engraftment, low GVHD, and durable remissions. Blood. 2011;118:6438–6445. doi: 10.1182/blood-2011-08-372508. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Adams GB, Chabner KT, Foxall RB, Weibrecht KW, Rodrigues NP, Dombkowski D, Fallon R, Poznansky MC, Scadden DT. Heterologous cells cooperate to augment stem cell migration, homing, and engraftment. Blood. 2003;101:45–51. doi: 10.1182/blood-2002-02-0486. [DOI] [PubMed] [Google Scholar]
- 35.Sercan Alp Ö, Durlanik S, Schulz D, McGrath M, Grün JR, Bardua M, Ikuta K, Sgouroudis E, Riedel R, Zehentmeier S, Hauser AE, Tsuneto M, Melchers F, Tokoyoda K, Chang HD, Thiel A, Radbruch A. Memory CD8(+) T cells colocalize with IL-7(+) stromal cells in bone marrow and rest in terms of proliferation and transcription. Eur J Immunol. 2015;45:975–987. doi: 10.1002/eji.201445295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Méndez-Ferrer S, Michurina TV, Ferraro F, Mazloom AR, Macarthur BD, Lira SA, Scadden DT, Ma’ayan A, Enikolopov GN, Frenette PS. Mesenchymal and haematopoietic stem cells form a unique bone marrow niche. Nature. 2010;466:829–834. doi: 10.1038/nature09262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Ding L, Saunders TL, Enikolopov G, Morrison SJ. Endothelial and perivascular cells maintain haematopoietic stem cells. Nature. 2012;481:457–462. doi: 10.1038/nature10783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Grimes HL, Schanie CL, Huang Y, Cramer D, Rezzoug F, Fugier-Vivier I, Ildstad ST. Graft facilitating cells are derived from hematopoietic stem cells and functionally require CD3, but are distinct from T lymphocytes. Exp Hematol. 2004;32:946–954. doi: 10.1016/j.exphem.2004.07.011. [DOI] [PubMed] [Google Scholar]
- 39.Wen Y, Elliott MJ, Huang Y, Miller TO, Corbin DR, Hussain LR, Ratajczak MZ, Fukui Y, Ildstad ST. DOCK2 is critical for CD8(+) TCR(-) graft facilitating cells to enhance engraftment of hematopoietic stem and progenitor cells. Stem Cells. 2014;32:2732–2743. doi: 10.1002/stem.1780. [DOI] [PubMed] [Google Scholar]
- 40.Bridenbaugh S, Kenins L, Bouliong-Pillai E, Kalberer CP, Shklovskaya E, Gratwohl A, Wodnar-Filipowicz A. Clinical stem-cell sources contain CD8+CD3+ T-cell receptor-negative cells that facilitate bone marrow repopulation with hematopoietic stem cells. Blood. 2008;111:1735–1738. doi: 10.1182/blood-2007-02-076000. [DOI] [PubMed] [Google Scholar]
- 41.Danby RD, Zhang W, Medd P, Littlewood TJ, Peniket A, Rocha V, Roberts DJ. High proportions of regulatory T cells in PBSC grafts predict improved survival after allogeneic haematopoietic SCT. Bone Marrow Transplant. 2016;51:110–118. doi: 10.1038/bmt.2015.215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Fujisaki J, Wu J, Carlson AL, Silberstein L, Putheti P, Larocca R, Gao W, Saito TI, Lo Celso C, Tsuyuzaki H, et al. In vivo imaging of Treg cells providing immune privilege to the haematopoietic stem-cell niche. Nature. 2011;474:216–219. doi: 10.1038/nature10160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Kawanishi Y, Passweg J, Drobyski WR, Rowlings P, Cook-Craig A, Casper J, Pietryga D, Garbrecht F, Camitta B, Horowitz M, et al. Effect of T cell subset dose on outcome of T cell-depleted bone marrow transplantation. Bone Marrow Transplant. 1997;19:1069–1077. doi: 10.1038/sj.bmt.1700807. [DOI] [PubMed] [Google Scholar]
- 44.Ho VT, Soiffer RJ. The history and future of T-cell depletion as graft-versus-host disease prophylaxis for allogeneic hematopoietic stem cell transplantation. Blood. 2001;98:3192–3204. doi: 10.1182/blood.v98.12.3192. [DOI] [PubMed] [Google Scholar]