

Abstract
Introduction
In Slovenia, longevity is increasing rapidly. From 1997 to 2014, life expectancy at birth increased by 7 and 5 years for men and women, respectively. This paper explores how this gain in life expectancy at birth can be attributed to reduced mortality from five major groups of causes of death by 5-year age groups. It also estimates potential future gains in life expectancy at birth.
Methods
The importance of the five major causes of death was analysed by cause-elimination life tables. The total elimination of individual causes of death and a partial hypothetical adjustment of mortality to Spanish levels were analysed, along with age and cause decomposition (Pollard).
Results
During the 1997–2014 period, the increase in life expectancy at birth was due to lower mortality from circulatory diseases (ages above 60, both genders), as well as from lower mortality from neoplasms (ages above 50 years) and external causes (between 20 and 50 years) for men. However, considering the potential future gains in life expectancy at birth, by far the strongest effect can be attributed to lower mortality due to circulatory diseases for both genders. If Spanish mortality rates were reached, life expectancy at birth would increase by more than 2 years, again mainly because of lower mortality from circulatory diseases in very old ages.
Discussion and conclusions
Life expectancy analyses can improve evidence-based decision-making and allocation of resources among different prevention programmes and measures for more effective disease management that can also reduce the economic burden of chronic diseases.
Keywords: longevity, life tables, mortality, causes of death, cause elimination, age decomposition, potential gains in life expectancy, life expectancy at birth, Slovenia
Izvleček
Uvod
V Sloveniji se življenje hitro podaljšuje. V obdobju od leta 1997 do leta 2014 se je pričakovano trajanje življenja ob rojstvu podaljšalo za 7 let za moške in za 5 let za ženske. V članku ugotavljamo, koliko je k temu povišanju v Sloveniji do leta 2014 prispevalo zniževanje umrljivosti po petih glavnih skupinah vzrokov smrti in po posameznih starostnih razredih. Poleg tega v članku ocenjujemo tudi potencialno bodoče podaljšanje pričakovanega trajanja življenja ob rojstvu za Slovenijo.
Metode
Uporabili smo skrajšane tablice umrljivosti s petletnimi starostnimi razredi. Razčlenitev podaljševanja pričakovanega trajanja življenja ob rojstvu v posameznih starostnih razredih smo analizirali po prirejeni Pollardovi metodi. Znotraj posameznega starostnega razreda smo posamezni skupini glavnih vzrokov smrti (bolezni obtočil, novotvorbe, zunanji vzroki smrtnosti, bolezni dihal, bolezni prebavil) pripisali enak relativni vpliv na povišanje pričakovanega trajanja življenja, kot ga ima ta vzrok smrti na znižanje stopnje smrtnosti v tistem starostnem razredu. Potencialen prispevek posameznega vzroka smrti na podaljšanje pričakovanega trajanja življenja v prihodnosti smo analizirali s tablicami smrtnosti z izločenim posameznim vzrokom smrti. Ker je popolna izločitev posameznega vzroka smrti nerealistična, smo upoštevali tudi hipotetično prilagoditev stopenj smrtnosti na raven španije, ki ima najdaljše pričakovano trajanje življenja ob rojstvu v EU in je po dejavnikih tveganja za glavne skupine vzrokov smrti podobna Sloveniji.
Ugotovitve
V obdobju 1997-2014 je imelo največji vpliv na podaljševanje pričakovanega trajanja življenja zmanjševanje smrtnosti zaradi bolezni obtočil v starosti nad 60 let pri obeh spolih. Pri moških je mocno vplivala tudi nižja smrtnost zaradi novotvorb v starosti nad 50 let ter zaradi zunanjih vzrokov smrti v starosti med 20 in 50 let. Pri analizi potencialnega povišanja pričakovanega trajanja življenja smo ugotovili, da bi lahko največ pridobili z zniževanjem smrtnosti zaradi bolezni obtočil. Do podobnega sklepa pripelje prilagoditev stopenj smrtnosti v Sloveniji na ravni, ki jih ima španija. Pričakovano trajanje življenja ob rojstvu bi bilo v tem primeru višje za več kot 2 leti, pri čemer bi največ razlike ponovno prispevali najvišji starostni razredi z nižjo smrtnostjo zaradi bolezni obtočil in novotvorb, precej pa tudi moški vseh starosti zaradi zunanjih vzrokov.
Razprava in skelp
Analiza pričakovanega trajanja življenja po vzrokih smrti in starosti omogoča z dokazi podprto odločanje o razporejanju resursov med različne preventivne programe in programe obvladovanja bolezni.
1. Introduction
In developed countries, a major outcome of fertility decline and increased longevity is population ageing that holds important implications for labour markets, social security, healthcare systems, and related developmental strategies. Currently, however, many countries are undergoing a different demographic transition (1). Given that in developed countries the biggest gains in life expectancy are realised at older ages (1, 2), such countries are examining these gains’ policy implications.
The literature addressing gains in life expectancy can be placed in three broad groups. The first comprises numerous studies of life expectancy gains arising from specific medical interventions and innovations. The second group studies the relationship between risk factors and life expectancy but, given the complexity of this relationship, either the impact of a specific risk factor on different causes of death is investigated (3-5), or different risk factor modifications for a specific disease are observed (6-7). The third group investigate the impact of the major causes of death on life expectancy, often combined with decomposition by age (8-11).
This paper contributes to the third group of papers. The key motivation for this research is to build on the results for Slovenia shown in recent literature (10), where only aggregate estimations are provided. In 2015, a very influential paper looking at global, regional and national age-sex specific all-cause and cause-specific mortality was published (11). While studying the epidemiological convergence across countries, the decomposition of life expectancy showed the prominent role of reductions in age-standardised death rates for cardiovascular diseases and cancers in high-income regions, and reductions in child deaths from diarrhoea, lower respiratory infections, and neonatal causes in low-income regions. Because Slovenia is only briefly mentioned, our paper’s main goal is to provide a more detailed analysis of the main triggers for past and future potential improvements in life expectancy at birth. More specifically, we try to confirm that the mortality improvement pattern – whereby the biggest gains are achieved in older ages due to fewer cardiovascular diseases and cancers – also holds for Slovenia, implying that Slovenia, too, is in the “cardiovascular revolution” stage of epidemiological transition (12).
This paper therefore investigates longevity improvement in Slovenia between 1997 and 2014, for which detailed data are available. During this period, life expectancy at birth e0 increased by 7.0 and 5.0 years for men and women, respectively. Assuming the mortality pattern from 2014, e0 equals 78.2 years for men and 84.1 years for women. The e0 increase was particularly fast between 2004 and 2014, that is 4.6 years for men and 3.3 years for women. As also shown by Figure 1, the increase is more pronounced for men. Figure 1 reveals the increase in e0 in Slovenia was larger than in the EU-28 area, respectively 2.9 and 2.1 years for men and women.
Figure 1.
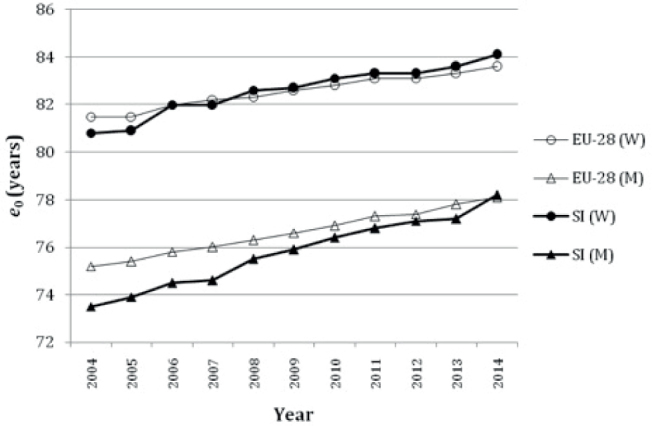
Life expectancy at birth for men (M) and women (W), 2004-2014, Slovenia (SI) and EU-28 (13).
Eurostat’s latest population projections for Slovenia assume a further rise in e0 (14). Technically, e0 is most strongly influenced by preventing infant mortality. However, infant mortality is already very low in developed countries, and significant improvements are no longer possible. On the other hand, preventing deaths at older ages has less impact on e0, but there is greater room for improvement as gains in e0 may be made by, for instance, controlling disease risk factors and preventing, postponing, or slowing down the progression of a disease. Analyses for developed countries show the e0 increases in the last decades were mainly due to lower mortality in older age groups (1, 2, 10).
As future gains in e0 are chiefly attributed to improved responses to noncommunicable diseases and changing social and environmental determinants of health (15), we can expect gains in e0 will continue to be made in higher age groups. A better understanding of potential improvements in e0 is growing in importance, because life expectancy gains concentrated at the end of life can unsettle any economy and may have even stronger negative effects in countries like Slovenia, having experienced a rapid rise in life expectancy and notable and rapid population ageing, requiring prompt policy and societal changes.
We estimate improvements in e0 due to reduced mortality from various groups of causes of death made between 1997 and 2014, and potential improvements, using Spain, with the highest e0 among all EU countries in 2014, as a benchmark. We also look for differences between groups of causes of death in age terms, in which the strongest gains in e0 are possible. By decomposing potential gains in e0 by age, we thus show whether these gains are potentially greater in working ages, or when people are mostly retired.
2. Methods
In this study, we employ life tables that are used to describe age-specific mortality rates of a population. A life table is a demographic model that builds on age-specific mortality rates of an actual population in a given year (16-18). Age specific mortality rates are converted into probabilities of dying, which are applied to a cohort of newborn children (a round number, usually 100,000, is assumed). The dying-off process is observed through life-table functions: from each age to the next, the population is decremented according to the fixed age-specific mortality probabilities until all members have died (16). If we divide the number of years to be lived by all cohort members during their life (the “total number of person-years”) by 100,000, we obtain life expectancy at birth e0. It shows the expected longevity if the mortality pattern remains unchanged. Thus, e0 is not affected by the age distribution and is therefore comparable geographically and across time. We use abridged period life tables for 5-year age groups (16-18) due to data availability. We use the 1997–2014 period data from the National Institute of Public Health (NIPH) (19) and Eurostat (20).
2.1. Potential Gains in Life Expectancy
By modifying the mortality pattern, we can estimate potential gains in e0 (8), attained by changing various determinants of life expectancy. According to WHO (15), much of the gain in e0, in developed countries, can be achieved by tackling noncommunicable diseases and changing social and environmental determinants of health.
In Slovenia, the five major groups of causes of death (according to ICD-10) in the last decades have been, namely: diseases of the circulatory system, neoplasms, external causes of morbidity and mortality, diseases of respiratory system, and diseases of digestive system (19). These five groups combined represented 90% of all deaths in Slovenia in 2014. All other causes of death with a notably smaller share are allocated to “Other causes of death”. The analysed groups of causes’ contributions to the total mortality rate are shown in Figure 2.
Figure 2.
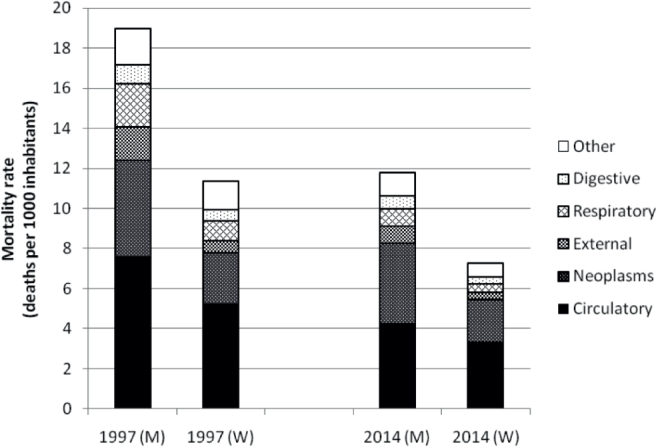
Age-standardised, cause-specific mortality rates for analysed groups of causes of death (according to ICD-10) for men (M) and women (W) in 1997 and 2014, Slovenia (standard age structure: total population 2014) (19, 20).
Figure 2 shows a substantial drop in mortality rates. The improvement in e0 due to reduced cause-specific mortality can be calculated using different approaches, involving either complete or partial elimination of causes of death. The obtained potential gain in e0 reveals the impact of each cause of death.
Cause-eliminated life tables answer the hypothetical question of what a life-table cohort’s mortality would be if a particular cause of death were completely eliminated (21). Compared to the master life table, the number of deaths is now set to 0 for the analysed cause, whereas it remains unaltered for all other causes. For persons who actually died from the analysed cause of death, it is thus assumed they would still be alive and as healthy as their peers in the same age group, leading to lower death rates and higher e0. In reality, eradicating a certain disease is likely to result in increased mortality due to other diseases, especially in older ages, when people often have more than one illness (“competing risks”) (18). However, by constructing cause-eliminated life tables no interdependencies among the causes of death are assumed. The assumption of independence can hardly be avoided until more is known about the interdependency of various causes of death (8). Also, when the causes are distant (disease) categories, the correlation has a very small effect on the results, and therefore the assumption of independence among causes of death may be considered acceptable (9).
Because entirely eliminating a cause of death is an unrealistic assumption, we analyse the effects of a partial reduction (8) in mortality. We assume the probability of dying for Slovenia could fall to the level of a better performing comparable country. We estimate the potential gains in e0 by assuming the probability of dying in Slovenia would decrease to the Spanish levels from 2014. Spain was selected because, in recent years, it has had the highest e0 among EU-28 countries (13). Ediev (22) argues that, although future gains will become ever harder to achieve when approaching the biological limit on the length of life, in the future, e0 could rise to above 95 and even close to 100 years, with up to 40% of a cohort becoming centenarians. Besides having the highest e0, Spain is comparable with Slovenia regarding risk factors, such as smoking and physical activity (23), the two key risk factors (7, 12) for the two most important groups of causes of death, namely: circulatory diseases and neoplasms. Relevant data are available from the Spanish national statistical institute (INE) (24).
2.2. Age- and Cause-Specific Decomposition
To investigate which age groups exhibit the strongest gains in e0, a decomposition by age is conducted. The most commonly applied decomposition methods include the Arriaga (25) and Pollard (26) approaches. Although mathematically equivalent (26), the various discrete approximations give somewhat different results. Arriaga’s approach underestimates the contribution of older age groups (21), but with the Pollard’s method, the total of partial contributions does not precisely add up (27) because of approximate formulae derived from the continuous approach. The Pollard’s method also requires detailed life tables for age groups above 85 years in order to measure the last open-ended age group’s contribution. In this paper, the correct summation of e0 differences across age groups is ensured by using a different weighting formula for Pollard’s approach suggested by Pressat (28):
where standard life-table function notations are used with 1 and 2 denoting different points in time, different countries, or any other different populations.
To this age decomposition we also apply a procedure (29) for simultaneous decomposition by cause of death. This technique requires mutually exclusive and exhaustive causes of death. Here we assume an individual cause of death’s contribution to the e0 change in each age group is proportional to the mortality change arising from that cause of death in the total mortality rate change for the same age group.
3. Results
Partial contributions of decreased mortality by individual age groups and different groups of causes of death to the total increase in e0 between 1997 and 2014 are presented in Table 1.
Table 1.
Contributions of age groups and different groups of causes of death to the 1997–2014 increase in life expectancy at birth e0 (in years) by gender in Slovenia.
| 1997–2014 change in e0 (years) | Men | Women | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age group | All causes | Circ. | Neopl. | Ext. | Resp. | Dig. | Other | All causes | Circ. | Neopl. | Ext. | Resp. | Dig. | Other |
| 0 | 0.29 | 0.00 | 0.00 | 0.01 | 0.02 | 0.00 | 0.27 | 0.20 | 0.01 | 0.01 | 0.02 | 0.00 | 0.00 | 0.17 |
| 1–4 | 0.05 | 0.02 | 0.01 | 0.00 | 0.00 | 0.01 | 0.01 | 0.06 | 0.00 | 0.03 | 0.01 | 0.00 | 0.00 | 0.02 |
| 5–9 | 0.09 | 0.00 | 0.00 | 0.06 | 0.00 | 0.01 | 0.03 | 0.00 | 0.00 | −0.01 | 0.01 | 0.00 | 0.00 | 0.01 |
| 10–14 | 0.08 | 0.00 | 0.02 | 0.05 | 0.00 | 0.00 | 0.00 | 0.01 | 0.00 | 0.02 | 0.00 | 0.00 | 0.00 | 0.00 |
| 15–19 | 0.09 | 0.00 | −0.01 | 0.10 | 0.00 | 0.00 | 0.00 | 0.07 | 0.00 | 0.00 | 0.04 | 0.00 | 0.00 | 0.03 |
| 20–24 | 0.22 | 0.01 | 0.02 | 0.18 | 0.00 | 0.00 | 0.01 | −0.02 | 0.00 | −0.01 | −0.01 | 0.00 | 0.00 | 0.00 |
| 25–29 | 0.23 | 0.00 | 0.00 | 0.18 | 0.00 | 0.01 | 0.03 | 0.04 | 0.00 | 0.01 | 0.02 | 0.00 | 0.00 | 0.00 |
| 30–34 | 0.17 | 0.04 | 0.00 | 0.11 | 0.01 | 0.02 | 0.00 | 0.04 | 0.00 | 0.02 | 0.01 | 0.00 | 0.00 | 0.01 |
| 35–39 | 0.24 | 0.02 | 0.05 | 0.10 | 0.00 | 0.04 | 0.03 | 0.11 | 0.01 | 0.03 | 0.05 | 0.00 | 0.01 | 0.02 |
| 40–44 | 0.37 | 0.09 | 0.04 | 0.15 | 0.01 | 0.05 | 0.03 | 0.17 | 0.03 | 0.06 | 0.03 | 0.00 | 0.03 | 0.02 |
| 45–49 | 0.46 | 0.12 | 0.12 | 0.11 | 0.01 | 0.06 | 0.04 | 0.20 | 0.01 | 0.08 | 0.04 | 0.00 | 0.03 | 0.04 |
| 50–54 | 0.54 | 0.19 | 0.13 | 0.11 | 0.03 | 0.05 | 0.05 | 0.23 | 0.05 | 0.05 | 0.03 | 0.01 | 0.04 | 0.06 |
| 55–59 | 0.55 | 0.21 | 0.12 | 0.08 | 0.04 | 0.06 | 0.03 | 0.27 | 0.07 | 0.06 | 0.03 | 0.02 | 0.07 | 0.02 |
| 60–64 | 0.74 | 0.25 | 0.24 | 0.08 | 0.04 | 0.08 | 0.05 | 0.30 | 0.13 | 0.04 | 0.03 | 0.02 | 0.05 | 0.02 |
| 65–69 | 0.79 | 0.34 | 0.19 | 0.05 | 0.12 | 0.04 | 0.06 | 0.49 | 0.20 | 0.11 | 0.03 | 0.03 | 0.04 | 0.08 |
| 70–74 | 0.66 | 0.36 | 0.12 | 0.02 | 0.08 | 0.04 | 0.04 | 0.53 | 0.29 | 0.03 | 0.04 | 0.07 | 0.02 | 0.08 |
| 75–79 | 0.67 | 0.37 | 0.09 | 0.04 | 0.13 | 0.00 | 0.04 | 0.71 | 0.43 | 0.05 | 0.01 | 0.09 | 0.04 | 0.08 |
| 80–84 | 0.43 | 0.27 | −0.04 | 0.01 | 0.14 | 0.01 | 0.04 | 0.78 | 0.45 | 0.02 | 0.05 | 0.10 | 0.03 | 0.13 |
| 85+ | 0.38 | 0.18 | −0.02 | 0.05 | 0.12 | −0.01 | 0.06 | 0.80 | 0.34 | 0.05 | 0.00 | 0.21 | 0.00 | 0.20 |
| All ages | 7.03 | 2.45 | 1.08 | 1.47 | 0.76 | 0.45 | 0.81 | 5.01 | 2.02 | 0.65 | 0.44 | 0.56 | 0.35 | 0.98 |
Explanation of abbreviations: Circ. – diseases of the circulatory system, Neopl. – neoplasms, Ext. – external causes of morbidity and mortality, Resp. – diseases of respiratory system, Dig. – diseases of digestive system, Other – all other causes of death not included in previous five groups.
Past improvements in e0 indicate the mortality patterns have been changing. The likely underlying reasons are living conditions and national income, patient awareness and empowerment in treatment options etc. (30, 31). By modifying the mortality pattern, we can assess potential gains in e0 from improving such determinants of life expectancy. One option is to estimate potential gains in e0 by completely eliminating one individual cause of death at a time (Table 2).
Table 2.
Potential gains in life expectancy (PGLE) at birth e0 (in years) if one group of causes of death is completely eliminated for persons born in 2014, Slovenia, by gender.
| 2014 PGLE (years) | Men | Women | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group of causes | Circ. | Neopl. | Ext. | Resp. | Dig. | Other | Circ. | Neopl. | Ext. | Resp. | Dig. | Other |
| All Ages | 5.74 | 4.75 | 1.42 | 0.69 | 0.71 | 1.46 | 10.98 | 3.73 | 0.67 | 0.59 | 0.49 | 1.30 |
Explanation of abbreviations: see Table 1.
As shown by Table 2, e0 could still be improved. However, given that complete elimination of individual causes of death is unrealistic, we focus more (presenting results also by age groups) on partial potential gains in e0. We assume that Slovenian mortality rates would change to Spanish levels in 2014 for each age group and each group of causes of death, resulting in e0 of 80.2 and 86.1 years for men and women, respectively (Table 3).
Table 3.
Age- and cause-specific decomposition of potential gains in life expectancy (PGLE) at birth e0 (in years) if Slovenian mortality levels are changed to Spanish ones in 2014, by gender.
| PGLE(years) | Men | Women | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age group | All causes | Circ. | Neopl. | Ext. | Resp. | Dig. | Other | All causes | Circ. | Neopl. | Ext. | Resp. | Dig. | Other |
| 0 | −0.11 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | −0.10 | −0.06 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | −0.05 |
| 1–4 | −0.02 | 0.00 | −0.01 | −0.01 | 0.00 | 0.00 | 0.00 | −0.03 | 0.00 | −0.01 | 0.00 | 0.00 | 0.00 | −0.01 |
| 5–9 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.01 | 0.00 | 0.01 | 0.00 | 0.00 | 0.00 | 0.00 |
| 10–14 | 0.01 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.02 | 0.00 | 0.00 | −0.01 | 0.01 | 0.00 | 0.00 | 0.00 |
| 15–19 | 0.04 | 0.00 | −0.01 | 0.04 | 0.00 | 0.00 | 0.01 | −0.01 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | −0.01 |
| 20–24 | 0.01 | −0.01 | −0.02 | 0.04 | 0.00 | 0.00 | 0.00 | 0.05 | −0.01 | 0.01 | 0.03 | 0.00 | 0.00 | 0.02 |
| 25–29 | 0.03 | 0.00 | −0.01 | 0.05 | 0.00 | 0.00 | −0.01 | −0.01 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 |
| 30–34 | 0.07 | −0.01 | 0.00 | 0.06 | −0.01 | 0.01 | 0.02 | 0.02 | 0.00 | 0.00 | 0.01 | 0.00 | 0.00 | 0.01 |
| 35–39 | 0.10 | 0.01 | 0.01 | 0.06 | −0.01 | 0.01 | 0.02 | 0.02 | −0.01 | 0.01 | 0.02 | 0.00 | 0.00 | 0.00 |
| 40–44 | 0.03 | −0.02 | 0.01 | 0.03 | −0.01 | 0.02 | 0.00 | −0.01 | −0.01 | 0.02 | −0.01 | 0.00 | 0.00 | −0.01 |
| 45–49 | 0.02 | −0.01 | −0.02 | 0.05 | −0.01 | 0.01 | 0.00 | 0.02 | 0.02 | 0.00 | 0.01 | −0.01 | 0.01 | −0.02 |
| 50–54 | 0.08 | 0.00 | 0.01 | 0.06 | −0.02 | 0.03 | 0.01 | 0.02 | 0.00 | 0.02 | 0.01 | −0.01 | 0.00 | −0.01 |
| 55–59 | 0.17 | 0.03 | 0.03 | 0.05 | −0.02 | 0.05 | 0.04 | 0.09 | 0.01 | 0.07 | 0.00 | −0.01 | 0.01 | 0.01 |
| 60–64 | 0.29 | 0.11 | 0.08 | 0.04 | −0.03 | 0.04 | 0.06 | 0.20 | 0.02 | 0.12 | 0.01 | −0.01 | 0.03 | 0.03 |
| 65–69 | 0.23 | 0.15 | 0.02 | 0.04 | −0.03 | 0.03 | 0.02 | 0.18 | 0.08 | 0.11 | 0.00 | 0.00 | 0.01 | −0.03 |
| 70–74 | 0.32 | 0.15 | 0.13 | 0.06 | −0.02 | 0.02 | −0.02 | 0.29 | 0.14 | 0.16 | 0.02 | −0.01 | 0.01 | −0.02 |
| 75–79 | 0.17 | 0.17 | 0.08 | 0.03 | −0.06 | 0.03 | −0.07 | 0.26 | 0.20 | 0.13 | 0.03 | −0.02 | 0.01 | −0.09 |
| 80–84 | 0.30 | 0.26 | 0.16 | 0.05 | −0.05 | 0.01 | −0.13 | 0.36 | 0.40 | 0.15 | 0.02 | −0.02 | 0.01 | −0.20 |
| 85+ | 0.28 | 0.56 | 0.12 | 0.05 | −0.09 | −0.02 | −0.33 | 0.61 | 1.46 | 0.13 | 0.14 | −0.12 | −0.02 | −0.99 |
| All ages | 2.05 | 1.39 | 0.58 | 0.70 | −0.37 | 0.21 | −0.46 | 2.01 | 2.31 | 0.91 | 0.33 | −0.23 | 0.07 | –1.38 |
Explanation of abbreviations: see Table 1.
If current mortality rates for Slovenia were to change to the levels of Spain in 2014, the largest contribution to longer e0 would stem from lower mortality from circulatory diseases for both genders, followed by neoplasms for women and external causes and neoplasms for men. For both genders, the biggest improvement in e0 would arise from the highest age groups due to circulatory diseases, neoplasms and digestive system diseases. For deaths due to external causes, similar potential gains in e0 could be achieved in different age groups for men.
Table 3 reveals negative values of potential gains in e0 for other causes of death and respiratory diseases, meaning that in 2014, Slovenian mortality – due to respiratory diseases and other causes of death (the latter is also clearly seen in the first year of life) – was already lower than Spanish. The large negative values in “Other causes of death” for higher age groups, especially for women, are due to lower mortality from causes of death characteristic of old age (such as diabetes, senility, osteoporosis, etc.). According to available data (19, 24), mortality from these causes is much higher in Spain than in Slovenia. We also computed the results for Sweden in 2014, whereby the “Other” group again has a highly negative value of -1.36 years for women and -0.46 years for men. We suspect that decreasing mortality from circulatory diseases and neoplasms results in higher mortality from other causes of death. However, comparing the e0 for Spain in 2014 with the e0 for Spain in 2006 (when e0 was almost the same as in Slovenia in 2014), the value is positive (0.35 years for men and 0.26 years for women) for the “Other” group and also for respiratory diseases. The peculiarly negative results for these two groups of causes of death in Slovenia need further investigation – whether mortality in Slovenia is actually lower, or whether there are problems with underreporting (32).
By combining Tables 2 and 3, we can assess what shares of Slovenian 2014 potential gains in e0 would be realised if Spanish mortality levels had been reached. Regarding three of the major groups of causes of death – circulatory diseases, neoplasms and external causes – much can be done. For external causes, about one-half of the potential gain in e0 (Table 2) could actually be realised by achieving Spanish mortality rates from 2014 (50% (=0.71/1.42) for men and 48% (=0.32/0.67) for women).
4. Discussion And Conclusions
In Slovenia, life expectancy at birth e0 has been zooming in the last decades, particularly between 2004 and 2014. Our analysis confirms that, in Slovenia, most of the improvement in e0 resulted from lower mortality in older age groups due to better prevention and treatment of circulatory diseases and neoplasms, which is in line with (1, 2, 10, 11). This paper also estimates possible future gains in e0 that could be achieved by reducing mortality from major groups of causes of death. Social change and health education generally are expected to continue improving longevity, and even have a stronger role than medical treatments themselves (33), also because people will reach old age in better health (34).
Estimated potential gains in e0 for Slovenia using Spain (i.e., the country with the highest e0 in the EU-28) as a benchmark reveal that mortality related to respiratory diseases and newborn care is already lower in Slovenia. This calls for further investigation. However, there is room for improvement in the area of circulatory diseases, especially at older ages. Spain also has considerably lower mortality due to neoplasms (particularly in older ages), as well as due to external causes for men in almost all age groups above 20 years.
The results presented in this paper identify which causes of death-and age-related improvements in mortality produce the highest potential gains in e0, thereby indicating certain priority areas for Slovenia. Identifying the best policy actions, however, is beyond this paper’s scope, even though it clearly shows challenging and unavoidable policy responses are required to prevent negative increased longevity impacts on economic sustainability. Future gains in e0, that will continue to be realised at later ages can be expected to lead to a lower labour force participation time span as a proportion of life expectancy at birth, unless there is a significant rise in labour force participation rates across middle and older ages. As Eggleston and Fuchs (1) note, lengthier retirement lives are inconsistent with continued rises in per capita income, unless there are notable increases in savings, investment and productivity. Improving productivity and increasing ability to work later in life will play a central role. Investments in public health and medical technologies that improve quality of life, assessing the value of innovation by considering not only costs of care, but also productivity gains and prevention, timely detection and effective management of chronic diseases, will help alleviate these diseases’ economic burden in the context of growing longevity.
Footnotes
Conflicts of interest: The authors declare that no conflicts of interest exist.
Funding
None
Ethical Approval
All data used in this study were provided by NIPH, INE and Eurostat. All personal data were anonymised.
References
- 1.Eggleston KN, Fuchs VR. The new demographic transition: most gains in life expectancy now realised late in life. J Econ Perspect. 2012;26:137–56. doi: 10.1257/jep.26.3.137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Canudas-Romo V, Schoen R.. Age-specific contribution to changes in the period and cohort life expectancy. Demogr Res. 2005;13:63–82. [Google Scholar]
- 3.Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. 2012;380:219–29. doi: 10.1016/S0140-6736(12)61031-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Renteria EJP, Forman D, Soerjomataram I.. The impact of cigarette smoking on life expectancy between 1980 and 2010: a global perspective. Tob Control. 2016;25:551–7. doi: 10.1136/tobaccocontrol-2015-052265. [DOI] [PubMed] [Google Scholar]
- 5.Machado de Rezende LF, de Sa TH, Mielke GI, Yukari Kodaira Viscondi J, Rey-Lόpez JP, Totaro Garcia LM. All-cause mortality attributable to sitting time analysis of 54 countries worldwide. Am J Prev Med. 2016;51:253–63. doi: 10.1016/j.amepre.2016.01.022. [DOI] [PubMed] [Google Scholar]
- 6.Jenko Pražnikar Z, Pražnikar J.. The effects of particulate matter air pollution on respiratory health and on the cardiovascular system. Zdr Varst. 2012;51:190–9. [Google Scholar]
- 7.Tsevat JI, Weinstein MC, Williams LW, Tosteson AN, Goldman L.. Expected gains in life expectancy from various coronary heart disease risk factor modifications. Circulation. 1991;83:1194–201. doi: 10.1161/01.cir.83.4.1194. [DOI] [PubMed] [Google Scholar]
- 8.Tsai SP, Lee ES, Hardy RJ. The effect of a reduction in leading causes of death: potential gains in life expectancy. Am J Public Health. 1978;68:966–71. doi: 10.2105/ajph.68.10.966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Conti S, Farchi G, Masocco M, Toccaceli V, Vichi M.. The impact of the major causes of death on life expectancy in Italy. Int J Epidemiol. 1999;28:905–10. doi: 10.1093/ije/28.5.905. [DOI] [PubMed] [Google Scholar]
- 10.Klenk J, Keil U, Jaensch A, Christiansen MC, Nagel G.. Changes in life expectancy 1950-2010: contributions from age-and disease-specific mortality in selected countries. Popul Health Metr. 2016;14:20. doi: 10.1186/s12963-016-0089-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Naghavi M, Wang HD, Lozano R, Davis A, Liang XF, Zhou MG. et al. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease study 2013. Lancet. 2015;385:117–71. doi: 10.1016/S0140-6736(14)61682-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bongaarts J.. Trends in causes of death in low-mortality countries: implications for mortality projections. Popul Dev Rev. 2014;40:189–212. [Google Scholar]
- 13.Life expectancy by age and sex. Eurostat. 5 April 2016 http://ec.europa.eu/Eurostat/data/database (Database by themes – Population and social conditions – Demography and migration – Mortality) [Google Scholar]
- 14.EUROPOP population projections. 2013 http://ec.europa.eu/Eurostat/data/database?node_code=proj Available 8 June 2016, from. [Google Scholar]
- 15.World Health Organization. WHO health statistics. 20152015 Geneva: WHO. [Google Scholar]
- 16.Poston DL, Bouvier LF. Population and society – an introduction to demography. Cambridge: Cambridge University Press; 2013. [Google Scholar]
- 17.Malačič J.. Demografija – teorija, analiza, metode in modeli. Ljubljana: Ekonomska fakulteta. 2006 [Google Scholar]
- 18.Kintner HJ. Swanson DA, Siegel JS. The methods and materials of demography. Vol. 2003. San Diego: Elsevier Science; The life table; pp. 301–40. [Google Scholar]
- 19.National Institute of Public Health Slovenia. Internal data on deaths by age and causes of death 1997-2014. On request [Google Scholar]
- 20.Population on 1 January by age and sex. Eurostat. http://ec.europa.eu/Eurostat/data/database Available 4 November 2015, from. (Database by themes – Population and social conditions – Demography and migration – Population) [Google Scholar]
- 21.Beltrán-Sánches H, Preston SH, Canudas-Romo V.. An integrated approach to cause-of-death analysis: cause-deleted life tables and decompositions of life expectancy. Demogr Res. 2008;19:1323. doi: 10.4054/DemRes.2008.19.35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ediev DM. Life expectancy in developed countries is higher than conventionally estimated: implications from improved measurement of human longevity. J Popul Ageing. 2011;4:5–32. [Google Scholar]
- 23.Smoking of tobacco products by sex, age and educational attainment level. Eurostat. http://ec.europa.eu/eurostat/data/database Available 19 November 2016, from. (Database by themes – Health – Health determinants – Tobacco consumption) [Google Scholar]
- 24.INE – Instituto Nacional de Estadistica. Death according to cause of death 2014. http://www.ine. es/dynt3/inebase/index.htm?type=pcaxis&path=/t15/p417/a2014&file=pcaxis&L=1 Available 12 April 2016, from. [Google Scholar]
- 25.Arriaga EE. Measuring and explaining the change in life expectancies. Demography. 1984;21:83–96. [PubMed] [Google Scholar]
- 26.Pollard JH. On the decomposition of changes in expectation of life and differentials in life expectancy. Demography. 1988;25:265–76. [PubMed] [Google Scholar]
- 27.Ponnapalli KM. A comparison of different methods for decomposition of changes in expectation of life at birth and differential in life expectancy at birth. Demographic Res. 2005;12:141–72. [Google Scholar]
- 28.Pressat R.. Contribution des écarts de mortalité par âge à la différence des vies moyennes. Population. 1985;4:765–70. [Google Scholar]
- 29.Arriaga EE. Ruzicka L, Wunsch G, Kane P. Differential mortality. Vol. 1995. Oxford: Clarendon Press; Changing trends in mortality decline during the last decades; pp. 105–30. [Google Scholar]
- 30.Bilas V, Franc S, Bošnjak M.. Determinant factors of life expectancy at birth in the European Union countries. Collegium Antropol. 2014;38:1–9. [PubMed] [Google Scholar]
- 31.Lichtenberg FR. The impact of pharmaceutical innovation on premature mortality, cancer mortality, and hospitalization in Slovenia, 1997-2010. Appl Health Econ Health Policy. 2015;13:207–22. doi: 10.1007/s40258-014-0144-3. [DOI] [PubMed] [Google Scholar]
- 32.Fleming DM, Schellevis FG, Van Casteren V.. The prevalence of known diabetes in eight European countries. Eur J Public Health. 2004;14:10–4. doi: 10.1093/eurpub/14.1.10. [DOI] [PubMed] [Google Scholar]
- 33.Ridsdale B, Gallop A.. Mortality by cause of death and by socioeconomic and demographic stratification 2010. ICA 2010 conference. http://www.actuaries.org/EVENTS/Congresses/Cape_Town/Presentations/Life%20Insurance%20 (IAALS)/183_PPT_Ridsdale.pdf Available 13 January 2016, from. [Google Scholar]
- 34.Vaupel JW. Biodemography of human aging. Nature. 2010;464:536–42. doi: 10.1038/nature08984. [DOI] [PMC free article] [PubMed] [Google Scholar]