

Abstract
Aim
The aim of our study was to chronologically analyse various public health measures of fluoride use in caries prevention.
Methods
We systematically searched the PubMed database on the preventive role of fluorides in public health, published from 1984 to 2014. The search process was divided into four steps, where inclusion and exclusion criteria were defined. Qualitative methodology was used for the article analysis. In the research process, the described forms of F use, diversity of the described F agents, and the observed population group were analysed.
Results
In our systematic review, 40 relevant reviews were revealed. Fluorides have been used in many different forms, but only a few studies showed their significant role in public health. Water fluoridation was the most important public health measure. In the recent decades, the number of studies on topical fluorides is constantly rising. The most extensively described topical forms of fluorides are professionally applied fluoride agents and fluoride toothpaste for home-use. The use of fluoride containing toothpaste in caries prevention is a safe and successful public health measure (PHM) if their use is widespread, and it is recommended for all. The results on other topical forms of fluorides are insufficient to be suggested as an important PHM.
Conclusions
The role of fluorides in public health prevention has changed in accordance with the knowledge about the fluoride cariostatic mechanism. Previously the most important pre-eruptive effect of fluorides was supplemented by the post eruptive effect. Abundant evidence exists to show the effectiveness of systemic and topical fluorides.
Keywords: fluorides, public health dentistry, caries prevention, epidemiology
Izvleček
Namen
Namen naše raziskave je bil kronološko analizirati različne načine javnozdravstvene uporabe fluoridov pri preventivi kariesa.
Metode
Sistematično smo pregledali pregledne članke v bibliografski bazi PubMed, ki so bili objavljeni v obdobju od leta 1984 do leta 2014. Iskalni proces je potekal v štirih fazah, v katerih smo določili vključitvene in izključitvene kriterije za določitev člankovza končno analizo. Za analizo člankovsmo uporabili kvalitativno metodologijo. V procesu analiziranja smo se osredotočili na razlicne oblike in načine uporabe fluoridov, jih opisali ter opredelili uporabo fluoridov in pomen za populacijo, v kateri so bili uporabljeni.
Rezultati
V našem sistematičnem pregledu smo analizirali 40 preglednih člankov. Opisane so številne oblike uporabe fluoridov, vendar le nekatere raziskave poudarjajo javnozdravstveni pomen. Fluoridiranje pitne vode je najpomembnejši javnozdravstveni ukrep. Povecalo se je število raziskav, ki proučujejo topikalne fluoride. Največ raziskav opisuje profesionalne pripravke s fluoridi in kreme za zobe s fluoridi za domačo uporabo. Uporaba kreme za zobe s fluoridi je varen in uspešen javnozdravstveni ukrep v preventivi kariesa, zato ga priporočamo za celotno populacijo. Rezultati o drugih oblikah topikalnih fluoridov so nezadostni, zato jih ni mogoče označiti kot pomembne javnozdravstvene ukrepe.
Zaključki
Vloga fluoridov se je spremenila v skladu z znanjem o njihovem delovanju. V preteklosti najpomembnejšemu preeruptivnemu delovanju se je pridružilo razumevanje o posteruptivnem učinku fluoridov. Obstajajo jasni dokazi o učinkovitosti tako sistemskih kot topikalnih fluoridov.
1. Introduction
Caries is a widespread oral disease (1). The prevention of caries with fluoride/s (F) has been proven to be an effective public health measure (PHM), and it is considered to be one of the ten greatest achievements of PH in the 20th century (2).
Fluorides are salts of the chemical element fluorine (3). People can be exposed to F in various ways: through air, soil, water, or beverages (1).
Black and McKay first recognised the preventive effect of F in Colorado Springs at the beginning of the 20th century (4). In 1931, Churchill identified a higher concentration of F in Colorado Spring’s water (5). This discovery encouraged Dean to perform several population interventions with water fluoridation (WF) to prevent caries at the population level (6). His work served as a basis for decades of population caries prevention by using WF. Systemic F had been widely recommended until the 1970s, when the new concept of understanding caries and F anticariogenic action was introduced (7). It was established that F controls caries mainly through its topical effect (3, 8). The topical mechanism is achieved either with systemic F or with topical F. In contrast, WF is a major factor in preventing pit and fissure caries, the most common site of tooth decay (9, 10).
According to the described historical facts, F are still divided into two groups according to their form of action, namely: systemic and topical (local). Systemic F (F water, milk or salt, F supplements as tablets, drops or lozenges) are ingested and incorporated into tooth enamel during tooth development. They also provide some topical protection of already erupted teeth as a reservoir of F in oral mucosa and saliva (12). Topical F (F toothpaste, mouthwashes, varnishes, gels, foams, slow-release F devices) reduce demineralisation of the enamel, promote remineralisation, and disable the metabolism of the bacteria in dental plaque (8, 11).
After nearly 100 years, F remains an important research subject. The availability of many different forms of F in the modern developed world and their cumulative preventive effect are among the most urgent topics in dentistry.
The aim of our study was to chronologically analyse various PH F uses in caries prevention.
2. Methods
2.1. Search Strategy
We systematically searched the PubMed database on the preventive role of F in PH, published from 1984 to 2014. The search was conducted in February 2015, and revised in September 2015.
The search process consisted of four steps (Figure 1), namely:
A basic search with included Medical Subject Headings (MESH): fluorides, dentistry, community health. We specified the search by reviewing the articles that also included the following words in the title or abstract: caries and preventive or prevention (Step 1).
The first screen was performed using the following three inclusion criteria: full text availability; written in English; narrative review or systematic review or meta-analysis as the type of the articles (shorted: reviews) (Step 2).
-
In the second screen, the article selection was narrowed down by reading abstracts from the selected reviews in the first search (Step 3).
We only included articles with the main theme of the preventive/community health role of F. We excluded reviews about the mechanism of action, F-containing materials, dental fluorosis, and the effect of F on bone remodelling, caries management with other chemical products or sealants.
Since none of the seven reviews published before 1984 met the criteria for inclusion, we determined the observed window of time as being from 1984 until the present.
After the second screen selection, three assessors independently read full-text articles and confirmed or declined the inclusion. Twenty-eight reviews met all our inclusion criteria, and further data were extracted and analysed. The hand-search of the bibliography resulted in the inclusion of twelve reviews (Step 4).
Figure 1.
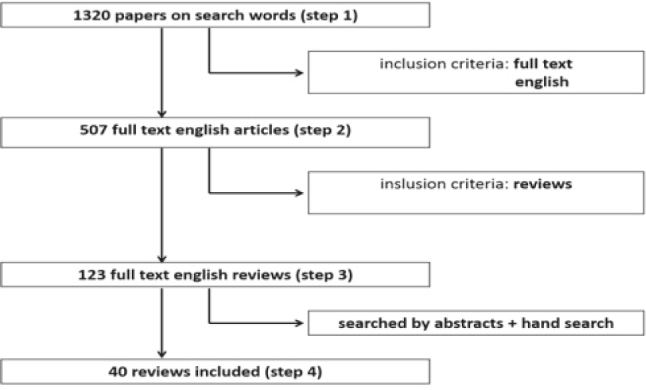
According to the described search strategy, 40 relevant articles were read in full (Figure 1).
2.2. Data Description
Qualitative methodology was used for the article analysis. In the first step, the relevant articles were extracted in the form of a specifically designed table: the described forms of F use (systemic, topical or both), diversity of the described F agents, and observed population group. In the second step, we summarised the main results on various uses of F as preventive agents over the previous 30 years.
3. Results
3.1. Search Strategy
According to the described search strategy, 40 relevant articles were read in full (Figure 1). In terms of content, articles were analysed according to the described F preventive agent(s) (Table 1).
Table 1.
Results of the reviews by year of publication and described form of the use of F preventive agents (PubMed, 1984-2014).
| First author, year of publication | Review type | W | T | S | M | I | P | V | G | R | D | To | Co |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sheiham, 1984 | NR | • | • | • | • | • | |||||||
| Hargreaves, 1990 | NR | • | |||||||||||
| Horowitz, 1990 | NR | • | |||||||||||
| Manji, 1990 | NR | • | • | • | • | ||||||||
| Lewis, 1994 | NR | • | |||||||||||
| Levy, 1994 | NR | • | • | • | |||||||||
| Johnston, 1994 | NR | • | • | ||||||||||
| O’Mullane, 1994 | NR | • | • | • | • | ||||||||
| Bowen, 1995 | NR | • | • | • | |||||||||
| Limeback, 1999 | NR | • | |||||||||||
| Marinho, 2002 | MA | • | |||||||||||
| Marinho, 2002 | MA | • | |||||||||||
| Marinho, 2003 | MA | • | |||||||||||
| Marinho, 2003 | MA | • | |||||||||||
| Twetman, 2003 | MA | • | |||||||||||
| Warren, 2003 | NR | • | • | • | • | • | |||||||
| Axelsson, 2004 | SR | • | |||||||||||
| Fejerskov, 2004 | NR | • | • | • | |||||||||
| Marinho, 2004 | MA | • | |||||||||||
| Marinho, 2004 | MA | • | |||||||||||
| Petersson, 2004 | MA | • | |||||||||||
| Twetman, 2004 | SR | • | |||||||||||
| Yeung, 2005 | SR | • | |||||||||||
| Bonner, 2006 | SR | • | |||||||||||
| Griffin, 2007 | SR | • | • | ||||||||||
| Pizzo, 2007 | SR | • | |||||||||||
| Ismail, 2008 | SR | • | |||||||||||
| Kumar, 2008 | NR | • | • | • | • | • | • | ||||||
| Pessan, 2008 | SR | • | |||||||||||
| Espelid, 2009 | SR | • | • | • | |||||||||
| Marinho, 2009 | SR | • | • | • | • | • | • | ||||||
| Toumba, 2009 | SR | • | |||||||||||
| Carvalho, 2010 | SR | • | |||||||||||
| Walsh, 2010 | MA | • | |||||||||||
| Wong, 2011 | SR | • | |||||||||||
| Lam, 2012 | NR | • | • | • | • | • | • | ||||||
| Petersen, 2012 | NR | • | • | • | • | • | • | • | |||||
| Marinho, 2013 | MA | • | |||||||||||
| Chong, 2014 | SR | • | |||||||||||
| Moyer, 2014 | SR | • | • | • |
Legend: NR - narrative review; SR - systematic review; MA - meta-analysis; W - water fluoridation, T - fluoridated tablets, drops, lozenges; S - fluoridate salt; M - fluoridate milk; I - ingested fluorides in food, drinks or as dental agents; P - toothpaste with fluorides; V - fluoride varnishes; G - fluoride gels; R - fluoride mouthwashes/mouth rinses; D - slow-release fluoride devices; To - topical fluorides in general; Co - combination of various fluoride agents.
3.2. Analysis by Periods of Observation
We arranged the reviews into three periods according to publication dates (Figure 2).
Figure 2.
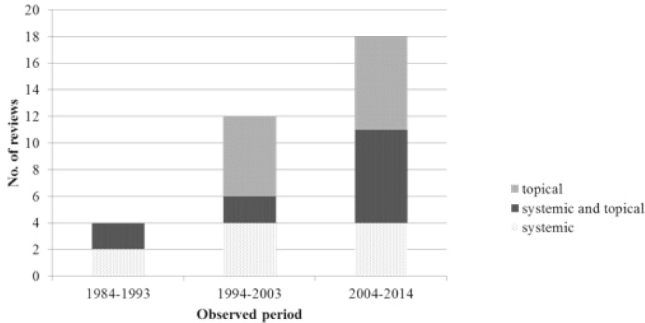
The number and substantive set of reviews about the preventive role of fluoride according to the publication date (PubMed, 1984-2014).
Nineteen different F interventions were observed in the selected reviews. The representation by their described F agents in caries prevention is shown in Figure 3 (systemic use) and Figure 4 (topical use).
Figure 3.
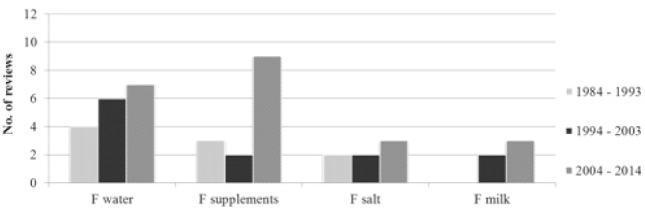
The number of reviews on systemic fluorides in the observed periods according to the form of use and publication time (F - fluoride/s).
Figure 4.
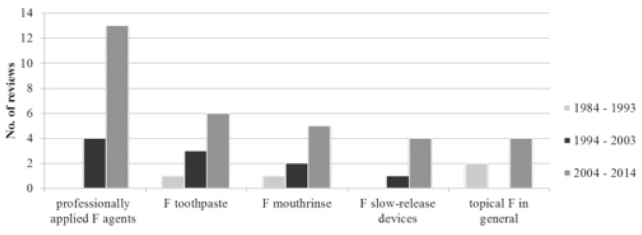
The number of reviews on topical fluorides in the observed periods, according to the form of use and publication time (F – fluoride/s).
In Figure 5, we arranged the reviews according to the observed population. Eight reviews did not specify the group of interest according to age. In terms of using different F interventions, systemic F were observed in all age groups, but for the analysis of topical effects in adults and the elderly, the data were too limited or nonexistent.
Figure 5.
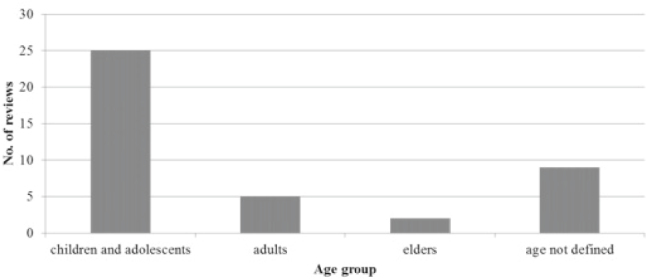
The distribution of the reviews about the preventive role of F according to the observed population group.
3.3. Results of Contents by Periods
3.3.1. The Period between 1984 and 1993
In the first observation period, only four relevant reviews were published. None of them focused on the topical F only and among the topical F agents; only Sheiham described toothpaste and mouth rinse (13). Hargreaves (14) and Manji (15) mentioned the possibility of topical F, but also warned about their insufficiently researched effects. All four reviews describe WF as an effective PHM of prevention of caries with 27-35% decline in caries prevalence in the exposed population, in comparison to the unexposed (13-16). The use of topical F (toothpaste, mouthwash) was reported to reduce the incidence of caries, especially during teeth eruption (13, 15).
Horowitz reported a lack of evidence on the combined use of systemic and topical F (16). He also reported that the use of topical products had helped to produce caries reduction in areas without WF and, thus, diminished the absolute differences in caries prevalence between WF and non-WF areas (16).
Nevertheless, Hargreaves emphasised the lack of knowledge in recommending different F agents according to the age and development of the individual for maximum effect with minimum risk (14).
3.3.2. The Period between 1994 and 2003
Between 1994 and 2003, twelve relevant reviews were published. Four described systemic F; six described topical F; and the remaining two described both forms of use.
Levy (17) presented a new concept of prevention with F: the concept of optimal intake of F. Limeback reported that extensive use of systemic F might have masked the topical action of systemic F (18). Moreover, he wrote that the topical action could be even more important than the systemic effect (18).
More than 50 years of experience with water fluoridation showed a reduction in the burden of caries among the exposed population in many countries (19). Differences in DMFS (decayed, missed, filled surfaces) were smaller than in the past; therefore, Lewis estimates WF as a relevant PHM in poor communities, but unnecessary in countries with low prevalence of caries (20). As an alternative, considerably less known or studied systemic F interventions were proposed (F supplements, fluoridated salt, milk or sugar) (17, 19-22).
Studies on F supplements revealed significant limitations: poor patient compliance and inappropriate prescription (17, 22).
When designing prevention programmes or individual counseling regarding F, the total intake of F should be taken into account, which also means taking into account F ingested with food, drink and oral care products (accidental) (17, 22).
During this period, several authors described the effectiveness of topical uses of F. Gels were the favourite choice of the operators (23). Their estimated efficiency was 21-26% in a population unexposed to other F treatments (24). The prevented fraction (PF) of F varnishes and F mouthwashes was high in primary and permanent deciduous teeth, although no significant association was found between the estimates of D(M)FS PFs and baseline caries or background exposure to F (25-27).
The reviews and meta-analysis confirmed that the effect of fluoride toothpaste is higher with higher F concentration and frequency of use (21, 28, 29). Moreover, Twetman found only limited evidence for anti-caries differences between low-fluoride and standard toothpaste (28). To summarise, they all concluded that the preventive action of F toothpaste when brushing every day in young permanent teeth was based on strong evidence (28, 29).
3.3.3. The Period between 2004 and 2014
We identified 21 reviews published in the last decade. Systemic F were described in four reviews, topical F in eleven reviews, and seven reviews included both.
In spite of rising numbers of evidence-based reviews on the importance of the topical effect of F, systemic F remained an important anti-cariogenic measure, especially in terms ofcost-effectiveness (30). In 2006, over 300 million people in 39 countries lived in WF-supplied areas (31).
F milk and F salt had shown some preventive effect, but they are difficult to prescribe in correctdoses, and scientific evidence for assessing their effect is insufficient to draw conclusions (30, 32-35).
Nevertheless, of all systemic F, the safety and efficiency of F supplements seem to be an issue of some debate among professionals (36). Reduction in caries increment differs a lot between different age groups, and in terms of the duration of action, proper supervision and motivation. The most popular form of professionally applied F agents in the reviews was F varnishes. The lack of evidence-based studies makes it impossible to determine whether the concentration in the varnish affects its prophylactic activity (37-39). There is a moderate benefit in preventing future caries with F varnish application in all children starting at the age of eruption of primary teeth (40, 41). F varnish is appealing for PH programmes, because it is easily incorporated (30, 37).
The two reviews mentioned F tooth-mousse and F gels as alternative forms of professionally applied F agents (33, 38).
In countries where F toothpasteis wide spread, it is the most relevant and accessible method of topical F (38, 42). More than 500 million people around the world use F toothpaste, and its effectiveness is well documented (34, 38, 42).
The efficiency of F toothpaste is increased with supervised brushing, a higher concentration of F, frequent use, and in higher-risk patients (29, 30, 33, 43). The evidence of the combined use of F toothpaste and another F agent remains limited; however, simultaneous use results in caries reduction compared with F toothpaste use alone (34, 38, 44-46). In comparison with gels or mouthwashes, toothpaste appears to have similar effectiveness for caries prevention in children (46).
Weekly rinsing under supervision has been proved to be effective and even an alternative to operative applied or unsupervised home use of F (30, 33). For the relatively new F agents, slow-release F devices, only a few studies are available, but they have shown a caries reduction capacity (47-50).
Although children and adolescents are still usually the population of interest, Griffin found that fluorides are effective among all adults, and the implementation of fluoride programmes should also serve this population (51).
4. Discussion
The prevention of caries with F has been a significant PH intervention since it started with the implementation of F in drinking water. In our study, we have presented the shift from the traditional to the modern understanding of F use in caries prevention.
Since 1984, when the first review of literature about PH fluoride prevention was conducted, fluorides have remained one of the milestones of caries prevention. Nevertheless, the recommendations and PH programmes have changed, and the number of published reviews about F prevention in the field of PH is constantly increasing.
In the first observed decade (1984-1993), the main points of interest were systemic F. In the second decade (1994-2003), only half of the reviews were about systemic F. In the latest decade, only a minority of the reviews focused on systemic F, with half of the reviews during 2004-2014, describing topical F as a PHM. Most of the research on F prevention was done in groups of children and adolescents. It is thought that F use in caries prevention is also an important measure among adults and especially among the elderly.
In 2004, Fejerskov described the shift from “caries resistance concept” to understanding caries to be a multifactorial disease, following the ecological shift in the tooth-surface biofilm (7).
At first, only WF seemed to be a major PHM, but in recent decades, topical F, especially widespread and very efficient F toothpaste, are considered as possible PHM, especially in populations with low caries increment.
Although all the reviews agree that community WF is safe and effective in caries prevention, its role has been combined with the use of topical F as PHM. WF is cost saving and still recommendedby the US Community Preventive Services Task Force (41) and recent guidelines (52–54). Even in an era with a widespread availability of fluoride from other sources, studies prove that water fluoridation continues to be effective in reducing dental decay (55, 56). WF is believed to be a major factor in preventing pit and fissure caries, the most common site of tooth decay (9, 10). Maximal caries-preventive effects of water fluoridation are achieved by exposure to optimal fluoride levels both pre- and post-eruptively (55). Moreover, the latest Cochrane review on WF from 2015, concluded that there is insufficient information to determine the effect of stopping water fluoridation programmes on caries prevalence (57).
The post-eruptive effect became more important with the decreasing severity of caries attack (58). Efforts of the PH preventive programme for oral health should be directed towards the maintenance of a permanent low concentration of fluoride in the mouth in as many people as possible (3). Even the current guidelines recommend fluoride toothpaste as the basic fluoride regimen for the majority of European communities (52).
In Slovenia, the level of F in the water supply is below 0.2 ppm (59), which is below the level of significance for WF. In addition, artificial fluoridation has never been implemented. In the 1970s, the topical application of a 2% sodium fluoride in school-age children (7–15 years) was introduced, which was changed, in the 1980s, to the application of aminofluoride gel and the widespread use of toothpaste with fluoride (60). Today, preventive dental care in Slovenia follows updated guidelines on the use of F in Europe (52). We wish to (re-)establish a modern, scientific-based collective approach to F use in caries prevention, which is currently, unfortunately, based on the commitment of individuals or smaller professional groups, working in dental (prevention) offices.
Our article presents the F use in caries prevention through the perspective of PH. Independently of the described form of F use, we highlighted the most significantfindings about all forms of F use in order to give the reader the best perspective on the field. A comprehensive knowledge on fluorides is described. At the same time, the comprehensive approach to our topic is also a restriction. We chose to limit our study to review articles; consequently, we could not assess the strength of evidence-based facts for each form of use.
Our review showed that the use of F in caries prevention is very active. It is important to improve the evidence ability for different forms of use, and to research the cumulative effects of using different forms of F. The effect of different F agents should be measured in various ages and social environments. Furthermore, the need for the systematic use of F in societies with low caries prevalence should be scientifically assessed. More research should also be done in the older population groups, not focusing only on children and adolescents.
5. Conclusion
In contrast to traditional systemic forms of F as PHMs, nowadays, the use of topical F is becoming the primary approach. As the operative treatment of caries is very expensive, and F has proven to be efficient in caries reduction, it remains recommended as the standard for caries prevention. At the same time, it is necessary to promote oral health also at other levels (good oral hygiene, healthy nutrition, regular check-ups, being included in oral preventive programmes).
Funding Statement
None
Footnotes
Conflicts of interest The authors declare that no conflicts of interest exist.
Ethical Approval
Review articles were studied.
References
- 1.Petersen PE. The world oral health report 2003: continuous improvement of oral health in the 21st century - the approach of the WHO Global Oral Health Programme. Community Dent Oral Epidemiol. 2003;31(Suppl 1):3–23. doi: 10.1046/j..2003.com122.x. [DOI] [PubMed] [Google Scholar]
- 2.Recommendations for using fluoride to prevent and control dental caries in the United States. MMWR Morb Mortal Wkly Rep. 2001;50:1–42. Centers for Disease Control and Prevention. [PubMed] [Google Scholar]
- 3.Fluorides and oral health; WHO Technical Report Series No. 846. Geneva: WHO; 1994. WHO Expert Committee on Oral Health Status and Fluoride Use. [PubMed] [Google Scholar]
- 4.Black GV, McKay FS. Original communications - mottled teeth: an endemic developmental imperfection of the enamel of the teeth heretofore unknown in the literature of dentistry. Dental Cosmos. 1916;58:129–56. [Google Scholar]
- 5.Churchill HV. Occurrence of fluorides in some waters of the United States. J Ind Eng Chem. 193123:996–8. [Google Scholar]
- 6.Arnold FA, Likins RC, Russell AL, Scott DB. Fifteenth year of the Grand Rapids fluoridation study. J Am Dent Assoc. 1962;65:780–5. [Google Scholar]
- 7.Fejerskov O.. Changing paradigms in concepts on dental caries: consequences for oral health care. Caries Res. 2004;38:182–91. doi: 10.1159/000077753. [DOI] [PubMed] [Google Scholar]
- 8.Buzalaf MA, Pessan JP, Honório HM, ten Cate JM. Mechanisms of action of fluoride for caries control. Monogr Oral Sci. 2011;22:97–114. doi: 10.1159/000325151. [DOI] [PubMed] [Google Scholar]
- 9.Singh KA, Spencer AJ. Relative effects of pre- and post-eruption water fluoride on caries experience by surface type of permanent first molars. Community Dent Oral Epidemiol. 2004;32:435–46. doi: 10.1111/j.1600-0528.2004.00182.x. [DOI] [PubMed] [Google Scholar]
- 10.Van Eck AAJM. Pre-and post-eruptive effect of fluoridated drinking water on dental caries experience. Utrecht: University of Utrecht. 1987 [Google Scholar]
- 11.Fejerskov O, Ekstrand J, Burt BA. Fluoride in dentistry. Copenhagen: Munksgaard. 1996 [Google Scholar]
- 12.Rošin-Grget K, Peroš K, Sutej I, Basić K.. The cariostatic mechanisms of fluoride. Acta Med Acad. 2013;42(Suppl 2):179–88. doi: 10.5644/ama2006-124.85. [DOI] [PubMed] [Google Scholar]
- 13.Sheiham A.. Changing trends in dental caries. Int J Epidemiol. 1984;13:142–7. doi: 10.1093/ije/13.2.142. [DOI] [PubMed] [Google Scholar]
- 14.Hargreaves JA. Water fluoridation and fluoride considerations for the future supplementation. J Dent Res. 1990;69:765–70. doi: 10.1177/00220345900690S148. [DOI] [PubMed] [Google Scholar]
- 15.Manji F, Fejerskov O.. Dental caries in developing countries. J Dent Res. 1990;96:733–41. doi: 10.1177/00220345900690S143. [DOI] [PubMed] [Google Scholar]
- 16.Horowitz HS. The future of water fluoridation and other systemic fluorides. J Dent Res. 1990;69:760–4. doi: 10.1177/00220345900690S147. [DOI] [PubMed] [Google Scholar]
- 17.Levy SM. Review of fluoride exposures and ingestion. Community Dent Oral Epidemiol. 1994;22:173–80. doi: 10.1111/j.1600-0528.1994.tb01836.x. [DOI] [PubMed] [Google Scholar]
- 18.Limeback H.. A re-examination of the pre-eruptive and post-eruptive mechanism of the anticaries effects of fluoride: is there any anticaries benefit from swallowing fluoride? Community Dent Oral Epidemiol. 1999;27:62–71. doi: 10.1111/j.1600-0528.1999.tb01993.x. [DOI] [PubMed] [Google Scholar]
- 19.O’Mullane DM. Systemic fluorides. Adv Dent Res. 1994;8:181–4. doi: 10.1177/08959374940080020801. [DOI] [PubMed] [Google Scholar]
- 20.Lewis DW, Banting DW. Water fluoridation: current effectiveness and dental fluorosis. Community Dent Oral Epidemiol. 1994;22:153–8. doi: 10.1111/j.1600-0528.1994.tb01833.x. [DOI] [PubMed] [Google Scholar]
- 21.Bowen WH. Are preventive programs sufficient for the needs of tomorrow? Adv Dent Res. 1995;9:77–81. doi: 10.1177/08959374950090021901. [DOI] [PubMed] [Google Scholar]
- 22.Warren JJ, Levy SM. Current and future role of fluorides in nutrition. Dent Clin North Am. 2003;47:225–43. doi: 10.1016/s0011-8532(02)00098-8. [DOI] [PubMed] [Google Scholar]
- 23.Johnston DW. Current status of professionally applied topical fluorides. Community Dent Oral Epidemiol. 1994;22:159–63. doi: 10.1111/j.1600-0528.1994.tb01834.x. [DOI] [PubMed] [Google Scholar]
- 24.Marinho VCC, Higgins JP, Sheiham A, Logan S.. Fluoride gels for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2002;1:CD002280. doi: 10.1002/14651858.CD002280. [DOI] [PubMed] [Google Scholar]
- 25.Marinho VCC, Higgins JP, Logan S, Sheiham A.. Fluoride varnishes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2002;3:CD002279. doi: 10.1002/14651858.CD002279. [DOI] [PubMed] [Google Scholar]
- 26.Twetman S, Petersson L, Axelsson S, Dahlgren H, Holm A-K, Kallestal C. et al. Cariespreventive effect of sodium fluoride mouthrinses: a systematic review of controlled clinical trials. Acta Odontol Scand. 2004;62:223–30. doi: 10.1080/00016350410001658. [DOI] [PubMed] [Google Scholar]
- 27.Marinho VCC, Higgins JPT, Logan S, Sheiham A.. Fluoride mouthrinses for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2003;3:CD002284. doi: 10.1002/14651858.CD002284. [DOI] [PubMed] [Google Scholar]
- 28.Twetman S, Axelsson S, Dahlgren H, Holm A, Källestål C, Lagerlöf F. et al. Caries preventive effect of fluoride toothpaste: a systematic review. Acta Odontol Scand. 2003;61:347–55. doi: 10.1080/00016350310007590. [DOI] [PubMed] [Google Scholar]
- 29.Marinho VCC, Higgins JP, Logan S, Sheiham A.. Fluoride toothpastes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2003;4:CD002782. doi: 10.1002/14651858.CD002782. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Kumar JV, Moss ME. Fluorides in dental public health programs. Dent Clin North Am. 2008;52:387–401. doi: 10.1016/j.cden.2007.11.003. [DOI] [PubMed] [Google Scholar]
- 31.Pizzo G, Piscopo MR, Pizzo I, Giuliana G.. Community water fluoridation and caries prevention: a critical review. Clin Oral Investig. 2007;11:189–93. doi: 10.1007/s00784-007-0111-6. [DOI] [PubMed] [Google Scholar]
- 32.Espelid I.. Caries preventive effect of fluoride in milk, salt and tablets: a literature review. Eur Arch Paediatr Dent. 2009;10:149–56. doi: 10.1007/BF03262676. [DOI] [PubMed] [Google Scholar]
- 33.Petersen PE, Phantumvanit P.. Perspectives in the effective use of fluoride in Asia. J Dent Res. 2012;91:119–21. doi: 10.1177/0022034511429347. [DOI] [PubMed] [Google Scholar]
- 34.Marinho VCC. Cochrane reviews of randomized trials of fluoride therapies for preventing dental caries. Eur Arch Paediatr Dent. 2009;10:183–91. doi: 10.1007/BF03262681. [DOI] [PubMed] [Google Scholar]
- 35.Yeung CA, Hitchings JL, Macfarlane TV, Threlfall AG, Tickle M, Glenny A-M. Fluoridated milk for preventing dental caries. Cochrane Database Syst Rev. 2005;3:CD003876. doi: 10.1002/14651858.CD003876.pub2. [DOI] [PubMed] [Google Scholar]
- 36.Ismail AI, Hasson H.. Fluoride supplements, denal caries and fluorosis: a systematic review. J Am Dent Assoc. 2008;139:1457–68. doi: 10.14219/jada.archive.2008.0071. [DOI] [PubMed] [Google Scholar]
- 37.Carvalho DM, Salazar M, Heliosa de Olivera B, Silva Freire Coutinho E.. Fluoride varnishes and caries incidence decrease in preschool children: a systematic review. Rev Bras Epidemiol. 2010;13(Suppl 1):1–11. doi: 10.1590/s1415-790x2010000100013. [DOI] [PubMed] [Google Scholar]
- 38.Lam A, Chu C.. Caries management with fluoride agents. N Y State Dent J. 2012;78:29–36. [PubMed] [Google Scholar]
- 39.Petersson LG, Twetman S, Dahlgren H, Norlund A, Holm AK, Nordenram G. et al. Professional fluoride varnish treatment for caries control: a systematic review of clinical trials. Acta Odontol Scand. 2004;62:170–6. doi: 10.1080/00016350410006392. [DOI] [PubMed] [Google Scholar]
- 40.Marinho VCC, Worthington HV, Walsh T, Clarkson JE. Fluoride varnishes for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2013;7:CD002279. doi: 10.1002/14651858.CD002279.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Moyer VA. Prevention of dental caries in children from birth through age 5 years: US Preventive Services Task Force recommendation statement. Pediatrics. 2014;13:1102–11. doi: 10.1542/peds.2014-0483. [DOI] [PubMed] [Google Scholar]
- 42.Wong MCM, Clarkson J, Glenny A-M, Lo ECM, Marinho VCC, Tsang BWK. et al. Cochrane reviews on the benefits/risks of fluoride toothpastes. J Dent Res. 2011;90(Suppl 5):573–9. doi: 10.1177/0022034510393346. [DOI] [PubMed] [Google Scholar]
- 43.Walsh T, Worthington HV, Glenny A-M, Appelbe P, Marinho VCC, Shi X.. Fluoride toothpastes of different concentrations for preventing dental caries in children and adolescents. Cochrane Database of Syst Rev. 2010;1:CD007868. doi: 10.1002/14651858.CD007868.pub2. [DOI] [PubMed] [Google Scholar]
- 44.Marinho VCC, Higgins JPT, Sheiham A, Logan S.. Combinations of topical fluoride (toothpastes, mouthrinses, gels, varnishes) versus single topical fluoride for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2004;1:CD002781. doi: 10.1002/14651858.CD002781.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Axelsson S, Söder B, Nordenram G, Petersson LG, Dahlgren H, Norlund A. et al. Effect of combined caries-preventive methods: a systematic review of controlled clinical trials. Acta Odontol Scand. 2004;62(Suppl 3):163–9. doi: 10.1080/00016350410006842. [DOI] [PubMed] [Google Scholar]
- 46.Marinho V, Higgins J, Sheiham A, Logan S.. One topical fluoride (toothpastes, or mouthrinses, or gels, or varnishes) versus another for preventing dental caries in children and adolescents. Cochrane Database Syst Rev. 2004;1:CD002780. doi: 10.1002/14651858.CD002780.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Pessan JP, Al-Ibrahim NS, Buzalaf MAR, Toumba KJ. Slow-release fluoride devices: a literature review. J Appl Oral Sci. 2008;16:238–46. doi: 10.1590/S1678-77572008000400003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Toumba KJ, Al-Ibrahim NS, Curzon MEJ. A review of slow-release fluoride devices. Eur Arch Paediatr Dent. 2009;10:175–82. doi: 10.1007/BF03262680. [DOI] [PubMed] [Google Scholar]
- 49.Chong LY, Clarkson JE, Dobbyn-Ross L, Bhakta S.. Slow-release fluoride devices for the control of dental decay. Cochrane Database Syst Rev. 2014;11:CD005101. doi: 10.1002/14651858.CD005101.pub3. [DOI] [PubMed] [Google Scholar]
- 50.Bonner BC, Clarkson JE, Dobbyn L, Khanna S.. Slow-release fluoride devices for the control of dental decay. Cochrane Database of Syst Rev. 2006;4:CD005101. doi: 10.1002/14651858.CD005101.pub2. [DOI] [PubMed] [Google Scholar]
- 51.Griffin SO, Regnier E, Griffin PM, Huntley V.. Effectiveness of fluoride in preventing caries in adults. J Dent Res. 2007;86:410–5. doi: 10.1177/154405910708600504. [DOI] [PubMed] [Google Scholar]
- 52.Guidelines on the use of fluoride in children: an EAPD policy document. 2009;10:129–35. doi: 10.1007/BF03262673. European Academy of Paediatric Dentistry. [DOI] [PubMed] [Google Scholar]
- 53.The use of fluorides in Australia: guidelines. Aust Dent J. 2006;51:195–9. doi: 10.1111/j.1834-7819.2006.tb00427.x. Australian Research Centre for population Oral Health. [DOI] [PubMed] [Google Scholar]
- 54.CDA position on use of fluorides in caries prevention, 2012. Jan 10, 2016 https://www.cda-adc.ca/_files/position_statements/fluoride.pdf Canadian Dental Association. [Google Scholar]
- 55.Newbrun E.. Systemic benefits of fluoride and fluoridation. J Public Health Dent. 2004;64:35–9. [Google Scholar]
- 56.Brunelle JA, Carlos JP. Recent trends in dental caries in U.S. children and the effect of water fluoridation. J Dent Res. 1990;69(Spec Iss):723–7. doi: 10.1177/00220345900690S141. [DOI] [PubMed] [Google Scholar]
- 57.Iheozor-Ejiofor Z, Worthington HV, Walsh T, O’Malley L, Clarkson JE, Macey R. et al. Water fluoridation for the prevention of dental caries. Cochrane Database of Syst Rev. 2015;6:CD010856. doi: 10.1002/14651858.CD010856.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Groeneveld A, van Eck AAMJ, Backer Dirks O.. Fluoride in caries prevention: is the effect pre- or post-eruptive? J Dent Res. 1990;69:751–5. doi: 10.1177/00220345900690S145. [DOI] [PubMed] [Google Scholar]
- 59.Monitoring pitne vode - rezultati januar 2015 - avgust 2015. Nov 10, 2015 http://www.mpv.si/rezultati NLZOH. [in Slovene] [Google Scholar]
- 60.Artnik B.. Javnozdravstveni pogled na uporabo fluoridov v skrbi za boljše ustno zdravje. Juričič M, Mugoša J. 100 let šolske medicine na Slovenskem: 1909-2009. Zbornik prispevkov. Ljubljana: Sekcija za šolsko in visokošolsko medicino. 2009:186–97. [Google Scholar]