

Abstract
There is a growing interest in using mobile phone technology to offer real-time psychological interventions and support. However, questions remain on the clinical effectiveness and feasibility of such approaches in psychiatric populations. Our aim was to systematically review the published literature on mobile phone apps and other mobile phone-based technology for psychotherapy in mental health disorders. To achieve this, electronic searches of PubMed, ScienceDirect, and Google Scholar were carried out in January 2016. Generated abstracts were systematically screened for eligibility to be included in the review. Studies employing psychotherapy in any form, being delivered through mobile-based technology and reporting core mental health outcomes in mental illness were included in the study. We also included trials in progress with published protocols reporting at least some outcome measures of such interventions. From a total of 1563 search results, 24 eligible articles were identified and reviewed. These included trials in anxiety disorders (8), substance use disorders (5), depression (4), bipolar disorders (3), schizophrenia and psychotic disorders (3), and attempted suicide (1). Of these, eight studies involved the use of smartphone apps and others involved personalized text messages, automated programs, or delivered empirically supported treatments. Trial lengths varied from 6 weeks to 1 year. Good overall retention rates indicated that the treatments were feasible and largely acceptable. Benefits were reported on core outcomes in mental health illness indicating efficacy of such approaches though sample sizes were small. To conclude, mobile phone-based psychotherapies are a feasible and acceptable treatment option for patients with mental disorders. However, there remains a paucity of data on their effectiveness in real-world settings, especially from low- and middle-income countries.
Keywords: eHealth, mHealth, psychiatric disorders, psychotherapy, smartphone, technology
INTRODUCTION
The use of mobile technology to support various aspects of health care delivery has been on the rise for more than a decade, and is now commonly referred to as “Mobile Health” or simply “mHealth'.”[1] The first mobile software application (“app”) became available for use in 2008.[2] Since then, an exponential growth in the number of apps has resulted in more than 10,000 of them with a quarter of them dealing with mental health disorders; of these, 6% can be used to evaluate core mental health outcomes while another 18% deal with more peripheral issues such as sleep, appetite, relaxation, and substance use.[2,3] Hence, a sizeable chunk of apps available can be harnessed for promoting mental health. Their impact has been felt on multiple domains of mental health-care delivery including real-time symptom monitoring and treatment progress tracking for clients with common mental disorders.[4]
mHealth technology has been leveraged to improve care delivery, medication adherence, and data collection in a wide range of mental health conditions including mood disorders, schizophrenia, anxiety, and substance use.[5,6,7,8] However, usage of mobile phones to provide psychotherapeutic services is at a relatively early stage of evaluation. The recent proliferation of research in this field coupled with vast heterogeneity among studies warrants a focused review of the evidence of mobile phone-based psychotherapy across mental health disorders. Previous reviews conducted in specific mental health disorders such as anxiety and mood disorders have shown discrepancies in the efficacy of mHealth interventions.[5,9] Hence, there is a need to synthesize available information to better understand the accumulated evidence, as well as the background, context, and participant characteristics in individual trials which may influence results. Against this background, the present systematic review aimed to provide an update on efficacy and current research trends of various mobile phone-based psychotherapeutic techniques in psychiatric conditions.
MATERIALS AND METHODS
Objective
The primary objective was to assess the efficacy of mobile phone-based psychotherapy interventions in various psychiatric disorders. For ongoing trials, the objective was to assess their feasibility and/or acceptability.
Search strategy and study selection
Electronic searches of PubMed, ScienceDirect, and Google Scholar were carried out in January 2016. We aimed to identify studies evaluating smartphone apps or other mobile phone-based technology for psychotherapy in mental health disorders. Psychotherapeutic treatments were defined as interventions that are predicated upon a scientific theoretical background and that employ psychological techniques to reduce symptoms and enhance general well-being through modifying motivational, emotional, cognitive, behavioral, or interpersonal processes.[10] For this review, a sequential search strategy was carried out. The first search was done using the following subject headings or free text terms: Psychotherapy, psychological therapy, psychoeducation, cognitive-behavior therapy (CBT), supportive management and schizophrenia, psychosis, psychotic disorders, mood disorders, bipolar disorders, depression, attempted suicide, childhood disorders, anxiety disorders, substance use disorders, alcohol use, and smoking. The second search included terms to capture the aspect of electronic health services delivery such as mobile technology, mobile health, mHealth, mHealth, virtual, eHealth, smartphone, internet, iPad, app, tablet, cellular phone, cell phone, information technology, telemedicine, and telepsychiatry. The two searches were then combined to generate a list of abstracts that included both concepts. This search strategy was primarily used for PubMed and then adapted for use in other databases. A supplemental Google Search using random combinations of above search terms was also carried out to further comb the extant literature. There was no restriction on the date of publication. Two authors (Vikas Menon and Tess Maria Rajan) independently carried out the search and the search findings were compared, and a consolidated list of abstracts was drawn up to avoid duplication. Any differences were sorted out through mutual consensus. In case of inadequate information in the abstract to decide on relevance, the corresponding full text was retrieved. The inclusion criteria for trials in the review are shown in Box 1. Studies were excluded if they dealt with general healthy population or studied nonspecific factors (such as stress, lifestyle, and exercise). The flowchart for literature search is shown in Figure 1. From the 1563 initial results, 930 studies were excluded as they did not include mobile-based technologies or because they dealt with disorders, not under the purview of this paper. Of the remaining 633, 615 were excluded because of following reasons: Dealing with general health-related behaviors or stress associated with commuting, pregnancy, surgery or work, using mobile devices for diagnostic data capture or only to enhance medication adherence or using mobile phones to access websites. One study was excluded as it dealt only with preventive interventions. Seven studies were added by a supplementary search of the cross-references of selected studies. Thus, a total of 24 articles were shortlisted and has been reviewed here. We did not attempt a meta-analysis considering the small number of completed studies for specific disorders (such as one for bipolar disorder) and the significant heterogeneity in outcome measures reported.
Box 1.
Inclusion criteria for reviewed trials
Figure 1.
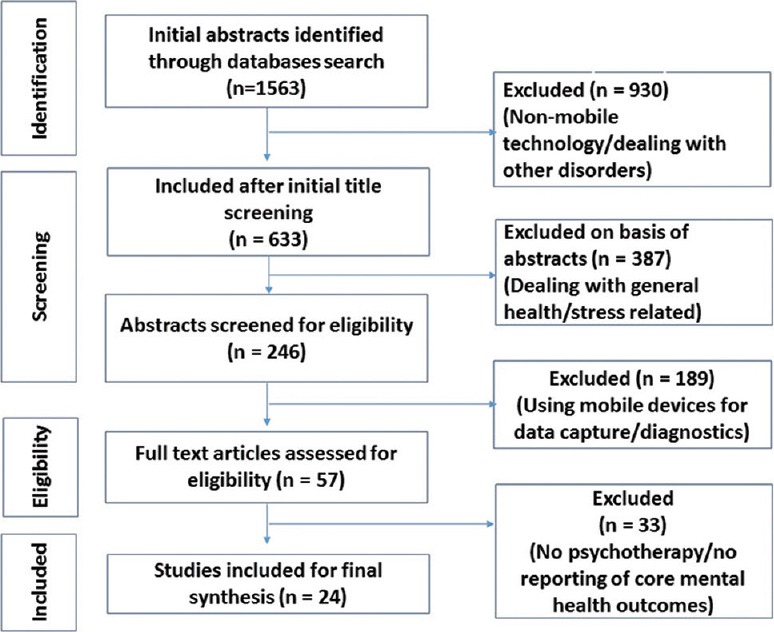
Flowchart for literature search
Data extraction
The information extracted from the articles included the author and year of study, place where the study was conducted, sample size and sampling method, mobile-based intervention carried out, treatment details for the control group, and reported findings. If effect sizes were calculated and reported by the authors, this was used. Else, we reported whatever findings were available in the text. Data extraction was done by Vikas Menon and Tess Maria Rajan. Any discrepancies were sorted out through mutual discussion and consensus.
RESULTS
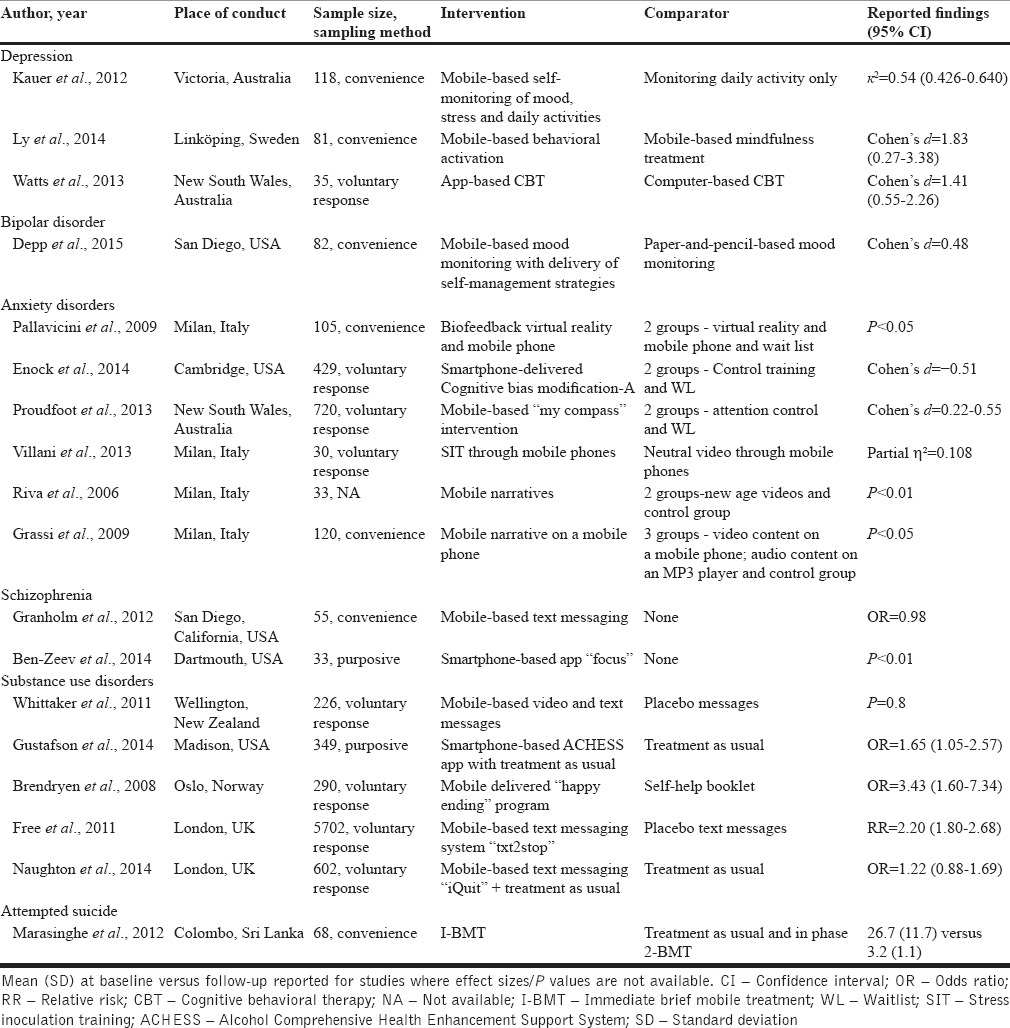
Our review identified 24 completed or on-going studies examining the role of mobile phone-based psychotherapy with 8 for anxiety disorders, 5 for substance use disorders, 4 for depressive disorders, 3 for bipolar disorders, 3 for schizophrenia and psychotic disorders, and 1 for attempted suicide. The characteristics of completed studies are shown in Table 1.
Table 1.
Characteristics of included studies
Depression
Kauer et al.[11] using a randomized controlled design evaluated the effects of an app that offered psychoeducation in the form of emotional self-awareness and found the app to reduce the burden of depressive symptoms. Another study compared a behavioral activation app with a mindfulness app and found both the apps to be feasible and effective.[12] Similarly, mobile-based CBT app was found to be as efficacious as computer-based CBT program for reducing depressive symptoms in a randomized trial spread over 6 weeks.[13]
The “Kokoro” app[14] is a smartphone-based CBT program which has shown feasibility and acceptability as an add-on therapy for treatment-resistant depression and is now undergoing trial of efficacy.
Bipolar disorders
Depp et al.[15] recently completed a 24-week RCT in which participants with bipolar disorder assigned to a mobile phone-based interactive mood monitoring system coupled with self-management advice performed better than traditional paper-and-pencil-based mood monitoring in reducing scores of depression and mania.
Another ongoing study aims to develop and validate a smartphone app that offers customized psychoeducation material and facilitates remote self-monitoring of symptoms, which is likely to empower patients to identify early symptoms and reduce risk of relapse.[16]
The Personalized Real-Time Intervention for Stabilizing Mood (PRISM)[17] is another mobile-based fully automated intervention that combines real-time experience sampling with an evidence-based brief psychoeducational intervention (“Life Goals”)[18] in bipolar disorder. As the “Life Goals” manual did not prove effective as a standalone intervention,[19] PRISM combined it with interactive mood charting and monitoring method with results showing high feasibility and acceptability.
Anxiety disorders
The SmartCAT App[20] was developed to deliver CBT for children with anxiety. The app, in a pilot evaluation, received good feedback from therapists and patients.
Pallavicini et al. examined the use of a mobile-based platform as an adjunct to existing treatments in generalized anxiety disorder.[21] Specifically, the intervention composed of biofeedback-enhanced virtual reality system to facilitate relaxation strategies. Using a double-blind randomized controlled design, investigators tested the efficacy of attention bias modification training exercises using a smartphone.[22] Those who received the active intervention had significant reductions on measures of social anxiety.
The “myCompass” program is a fully automated self-help program that can be used for individuals with mild to moderate depression, anxiety, or stress.[23] The program includes symptom tracking features apart from medication reminders. Participants in the myCompass program outperformed attention control or waitlisted controls on outcome measures for depression, anxiety, stress, social, and work functioning at the end of 7 weeks.
Stress inoculation training through mobile phone demonstrated significant reductions in trait and state anxiety as well as enhanced coping skills compared to controls.[24] The use of mobile multimedia-based narratives to regulate and manage emotions has been tested in nonpsychiatric populations with results showing that such approaches can be used to increase relaxation and decrease state anxiety ratings without real-time physician contact.[25,26]
An ongoing study[27] seeks to assess the effectiveness rather than the efficacy of a mobile-phone-delivered CBT package for anxiety spectrum disorders. The major difference here is the therapists are not constrained to deliver only the protocol-mandated intervention but can add other components as needed such as enlisting social support thus reflecting the eclectic nature of therapy in the real-world setting. This study is likely to illuminate organizational and community issues that may contribute to the effectiveness of CBT for anxiety disorders.
Schizophrenia and psychotic disorders
Many applications of mobile technology in schizophrenia have been pointed out in a recent paper.[28]
The mobile assessment and treatment of schizophrenia trial[29] was conducted to deliver personalized text messages to improve outcomes in patients with schizophrenia. The text messages were aimed at changing attitude toward auditory hallucinations using CBT principles, encourage socialization, and medication adherence. The intervention was found to be feasible and effective.
Ben-Zeev et al.[30] have developed and validated a smartphone app (focus) for use among patients with schizophrenia, addressing various symptom dimensions through cognitive restructuring and medication adherence. The same authors, in another study to assess feasibility, acceptability and preliminary efficacy of the app,[31] showed that a large majority (>90%) rated the app as highly acceptable and had significant reductions in psychotic, depressive, and general psychopathology symptoms following 1 month of intervention.
The Actissist app was designed to deliver CBT for patients with first-episode psychosis.[32] It runs for a 12-week and aims to address a variety of evidence-based risk factors for relapse. Recruitment to test its feasibility, acceptability and efficacy is currently ongoing.
Substance use disorders
Alcohol Comprehensive Health-Enhancement Support System is a smartphone-based recovery and relapse prevention support system.[33] The focus is on coping skills, social support, and internal motivation. A 4-month study showed that those who used this app had reduced their heavy drinking days by 65% at 4, 8, and 12 months compared to a control group.
STUB IT is a social-cognitive theory-based intervention approach employing video messages that combine observational learning with evidence-based behavioral support.[34] However, the investigators failed to achieve target sample size due to recruitment problems, and hence results were inconclusive.
A fully automated smoking cessation program (“Happy Ending”) comprising E-mail, text messages, or interactive voice response delivered via computer and mobile phone over a period of 1 year, was administered to smokers (n = 144) and compared for efficacy with a control group of smokers (n = 146) who received a self-help booklet.[35] Using intent-to-treat analysis, participants in the intervention group had significantly higher levels of repeated point abstinence.
Mobile-based technology incorporating graded text messages, motivational messages, and personalized behavior change strategies was evaluated for smoking cessation by Free et al.[36] There was higher rate of continuous biochemically confirmed abstinence in the intervention group versus the control group. An ideologically similar intervention, combining variably scheduled text messages and customized patient advice report, called the iQuit system, was evaluated in primary care setting.[37] Short-term abstinence rates did not differ significantly between the intervention and control, though the intervention's efficacy was noted for long-term abstinence.
Attempted suicide
One trial compared a brief mobile-based intervention to treatment as usual among suicide attempters and found significant reductions in suicidal ideations and depression in the mobile phone group.[38]
DISCUSSION
Although the number of trials reviewed was not large, available results appear promising and seem to suggest that mobile phone-based technology can be used to deliver psychotherapeutic interventions across a range of mental health disorders.
The literature on depression included one on community-based sample and another on self-referred patients showing that diverse clinical populations can be engaged meaningfully in such technology-driven mediums. In contrast, literature in bipolar disorder is more limited, and there was only one trial available which reported mood outcomes. It is plausible that individuals in acute mania may find it difficult to engage with the app consistently for good results[39] and this may explain why on-going trials in bipolar disorder have focused on remote self-monitoring of symptoms in stable patients.
Maximum number of trials was found for anxiety disorders. The effect sizes were comparable with findings from meta-analytic reviews evaluating conventionally administered CBT and other psychological treatments in depression[10,40,41] but somewhat lower than the figures reported in a recent meta-analysis of treatment efficacy in anxiety disorders.[42]
Only three trials were available for psychotic disorders, and only one of them reported efficacy outcomes and demonstrated the possibility of tackling both positive and negative symptoms. Hence, inputs from this trial may be utilized to develop further ecological and ambulatory interventions for people with schizophrenia. The evidence base in psychotic disorders is largely preliminary in nature and further studies with a comparison group and longer time horizons are required to clearly establish the advantages of using mobile technology for long-term care in psychotic disorders. A similar conclusion could be arrived at for attempted suicide since only one trial was available.
The substance use disorder literature demonstrated the feasibility and efficacy of combining text messages with personalized support and relapse prevention strategies. However, little insights are available into how and which component of the intervention worked to bring about the desired behavioral change.[43] Qualitative studies eliciting participant experiences and reflections may help to tease out the effective components of the intervention. The effect sizes reported in these trials were very similar to other behavioral interventions for substance use such as group therapy and one-on-one counseling.[44,45]
Looking the evidence in totality, mobile phone technology offers a simple, flexible, convenient, and widely accessible platform for delivery of mental health-care services and decision support systems. It allows patients and health-care providers to track symptoms and early changes in a collaborative manner. This facilitates need-based allocation of resources and therefore this technology holds great promise for low- and middle-income countries. As many studies have included a self-education component for mental health conditions,[15,16,33] similar apps could be developed for the general population which may hold promise from a mental health prevention and promotion standpoint.
There are a few limitations to the current review. First, the studies reviewed were quite heterogeneous in their aims, methodology, and outcome measures and hence drawing clear conclusions from them are onerous. Second, it is possible that, despite our best efforts and comprehensive search strategy, some studies especially those unpublished or ongoing or not available on academic databases were excluded from this review. A third limitation pertains to the generalization of results to the real-world settings over longer periods of time, given that most trials were of short duration involving small samples and possibility of participants in controlled settings showing greater adherence to interventions. Possibility of nonspecific factors such as increased physician support in trials leading to improvement also cannot be discounted.[46,47] Finally, it is possible that some trials may have been missed as they did not fit into the definition of psychotherapy used for the purpose of this review.
CONCLUSION
To conclude, the emerging literature highlights the potential benefits, feasibility, and acceptability of mobile phone-based psychotherapeutic applications across a range of psychiatric conditions. However, effectiveness trials are scarce. Most of the trials were conducted in the West, and very little information is available from low- and middle-income countries. Many trials reviewed here reported equivocal effect on core psychiatric outcomes and await further validation. With incremental improvements in design, methodology, and innovation, mobile technology has the potential to play a key role in transforming the healthcare delivery process. Future directions of research are highlighted in Box 2. The reviewed evidence provide some hope that mobile phone technology will prove to be a useful adjunctive, if not a standalone, treatment for psychotherapy in a broad range of mental health conditions.
Box 2.
Future directions of research for mobile delivered psychotherapeutic interventions
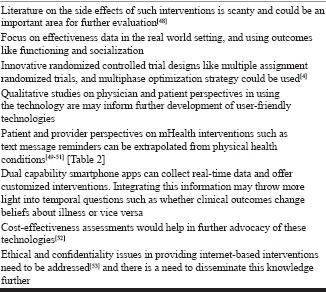
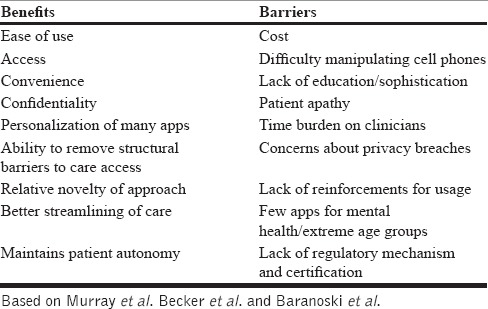
Table 2.
Patient and health-care provider perspectives on mhealth interventions
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Istepanian R, Jovanov E, Zhang YT. Introduction to the special section on M-Health: Beyond seamless mobility and global wireless health-care connectivity. IEEE Trans Inf Technol Biomed. 2004;8:405–14. doi: 10.1109/titb.2004.840019. [DOI] [PubMed] [Google Scholar]
- 2.Donker T, Petrie K, Proudfoot J, Clarke J, Birch MR, Christensen H. Smartphones for smarter delivery of mental health programs: A systematic review. J Med Internet Res. 2013;15:e247. doi: 10.2196/jmir.2791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Tomlinson M, Rotheram-Borus MJ, Swartz L, Tsai AC. Scaling up mHealth: Where is the evidence? PLoS Med. 2013;10:e1001382. doi: 10.1371/journal.pmed.1001382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Price M, Yuen EK, Goetter EM, Herbert JD, Forman EM, Acierno R, et al. mHealth: A mechanism to deliver more accessible, more effective mental health care. Clin Psychol Psychother. 2014;21:427–36. doi: 10.1002/cpp.1855. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Loo Gee B, Griffiths KM, Gulliver A. Effectiveness of mobile technologies delivering Ecological momentary interventions for stress and anxiety: A systematic review. J Am Med Inform Assoc. 2016;23:221–9. doi: 10.1093/jamia/ocv043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Harrison V, Proudfoot J, Wee PP, Parker G, Pavlovic DH, Manicavasagar V. Mobile mental health: Review of the emerging field and proof of concept study. J Ment Health. 2011;20:509–24. doi: 10.3109/09638237.2011.608746. [DOI] [PubMed] [Google Scholar]
- 7.Lindhiem O, Bennett CB, Rosen D, Silk J. Mobile technology boosts the effectiveness of psychotherapy and behavioral interventions: A meta-analysis. Behav Modif. 2015;39:785–804. doi: 10.1177/0145445515595198. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Marsch LA. Leveraging technology to enhance addiction treatment and recovery. J Addict Dis. 2012;31:313–8. doi: 10.1080/10550887.2012.694606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Torous J, Powell AC. Current research and trends in the use of smartphone applications for mood disorders. Internet Interv. 2015;2:169–73. [Google Scholar]
- 10.Linde K, Sigterman K, Kriston L, Rücker G, Jamil S, Meissner K, et al. Effectiveness of psychological treatments for depressive disorders in primary care: Systematic review and meta-analysis. Ann Fam Med. 2015;13:56–68. doi: 10.1370/afm.1719. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kauer SD, Reid SC, Crooke AH, Khor A, Hearps SJ, Jorm AF, et al. Self-monitoring using mobile phones in the early stages of adolescent depression: Randomized controlled trial. J Med Internet Res. 2012;14:e67. doi: 10.2196/jmir.1858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ly KH, Trüschel A, Jarl L, Magnusson S, Windahl T, Johansson R, et al. Behavioural activation versus mindfulness-based guided self-help treatment administered through a smartphone application: A randomised controlled trial. BMJ Open. 2014;4:e003440. doi: 10.1136/bmjopen-2013-003440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Watts S, Mackenzie A, Thomas C, Griskaitis A, Mewton L, Williams A, et al. CBT for depression: A pilot RCT comparing mobile phone vs. computer. BMC Psychiatry. 2013;13:49. doi: 10.1186/1471-244X-13-49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Watanabe N, Horikoshi M, Yamada M, Shimodera S, Akechi T, Miki K, et al. Adding smartphone-based cognitive-behavior therapy to pharmacotherapy for major depression (FLATT project): Study protocol for a randomized controlled trial. Trials. 2015;16:293. doi: 10.1186/s13063-015-0805-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Depp CA, Ceglowski J, Wang VC, Yaghouti F, Mausbach BT, Thompson WK, et al. Augmenting psychoeducation with a mobile intervention for bipolar disorder: A randomized controlled trial. J Affect Disord. 2015;174:23–30. doi: 10.1016/j.jad.2014.10.053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hidalgo-Mazzei D, Mateu A, Reinares M, Undurraga J, Bonnín Cdel M, Sánchez-Moreno J, et al. Self-monitoring and psychoeducation in bipolar patients with a smart-phone application (SIMPLe) project: Design, development and studies protocols. BMC Psychiatry. 2015;15:52. doi: 10.1186/s12888-015-0437-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Depp CA, Mausbach B, Granholm E, Cardenas V, Ben-Zeev D, Patterson TL, et al. Mobile interventions for severe mental illness: Design and preliminary data from three approaches. J Nerv Ment Dis. 2010;198:715–21. doi: 10.1097/NMD.0b013e3181f49ea3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bauer MS, McBride L, Williford WO, Glick H, Kinosian B, Altshuler L, et al. Collaborative care for bipolar disorder: Part I. Intervention and implementation in a randomized effectiveness trial. Psychiatr Serv. 2006;57:927–36. doi: 10.1176/ps.2006.57.7.927. [DOI] [PubMed] [Google Scholar]
- 19.Bauer MS, McBride L, Williford WO, Glick H, Kinosian B, Altshuler L, et al. Collaborative care for bipolar disorder: Part II. Impact on clinical outcome, function, and costs. Psychiatr Serv. 2006;57:937–45. doi: 10.1176/ps.2006.57.7.937. [DOI] [PubMed] [Google Scholar]
- 20.Pramana G, Parmanto B, Kendall PC, Silk JS. The SmartCAT: An m-health platform for ecological momentary intervention in child anxiety treatment. Telemed J E Health. 2014;20:419–27. doi: 10.1089/tmj.2013.0214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Pallavicini F, Algeri D, Repetto C, Gorini A, Riva G. Biofeedback, virtual reality and mobile phones in the treatment of generalized anxiety disorder (GAD): A phase-2 controlled clinical trial. J Cyber Ther Rehabil. 2009;2:315–28. [Google Scholar]
- 22.Enock PM, Hofmann SG, McNally RJ. Attention bias modification training via smartphone to reduce social anxiety: A randomized, controlled multi-session experiment. Cogn Ther Res. 2014;38:200–16. [Google Scholar]
- 23.Proudfoot J, Clarke J, Birch MR, Whitton AE, Parker G, Manicavasagar V, et al. Impact of a mobile phone and web program on symptom and functional outcomes for people with mild-to-moderate depression, anxiety and stress: A randomised controlled trial. BMC Psychiatry. 2013;13:312. doi: 10.1186/1471-244X-13-312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Villani D, Grassi A, Cognetta C, Toniolo D, Cipresso P, Riva G. Self-help stress management training through mobile phones: An experience with oncology nurses. Psychol Serv. 2013;10:315–22. doi: 10.1037/a0026459. [DOI] [PubMed] [Google Scholar]
- 25.Riva G, Preziosa A, Grassi A, Villani D. Stress management using UMTS cellular phones: A controlled trial. Stud Health Technol Inform. 2006;119:461–3. [PubMed] [Google Scholar]
- 26.Grassi A, Gaggioli A, Riva G. The green valley: The use of mobile narratives for reducing stress in commuters. Cyberpsychol Behav. 2009;12:155–61. doi: 10.1089/cpb.2008.0156. [DOI] [PubMed] [Google Scholar]
- 27.Ekberg J, Timpka T, Bång M, Fröberg A, Halje K, Eriksson H. Cell phone-supported cognitive behavioural therapy for anxiety disorders: A protocol for effectiveness studies in frontline settings. BMC Med Res Methodol. 2011;11:3. doi: 10.1186/1471-2288-11-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ben-Zeev D. Mobile technologies in the study, assessment, and treatment of schizophrenia. Schizophr Bull. 2012;38:384–5. doi: 10.1093/schbul/sbr179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Granholm E, Ben-Zeev D, Link PC, Bradshaw KR, Holden JL. Mobile assessment and treatment for schizophrenia (MATS): A pilot trial of an interactive text-messaging intervention for medication adherence, socialization, and auditory hallucinations. Schizophr Bull. 2012;38:414–25. doi: 10.1093/schbul/sbr155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Ben-Zeev D, Kaiser SM, Brenner CJ, Begale M, Duffecy J, Mohr DC. Development and usability testing of FOCUS: A smartphone system for self-management of schizophrenia. Psychiatr Rehabil J. 2013;36:289–96. doi: 10.1037/prj0000019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Ben-Zeev D, Brenner CJ, Begale M, Duffecy J, Mohr DC, Mueser KT. Feasibility, acceptability, and preliminary efficacy of a smartphone intervention for schizophrenia. Schizophr Bull. 2014;40:1244–53. doi: 10.1093/schbul/sbu033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Bucci S, Barrowclough C, Ainsworth J, Morris R, Berry K, Machin M, et al. Using mobile technology to deliver a cognitive behaviour therapy-informed intervention in early psychosis (Actissist): Study protocol for a randomised controlled trial. Trials. 2015;16:404. doi: 10.1186/s13063-015-0943-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Gustafson DH, McTavish FM, Chih MY, Atwood AK, Johnson RA, Boyle MG, et al. A smartphone application to support recovery from alcoholism: A randomized clinical trial. JAMA Psychiatry. 2014;71:566–72. doi: 10.1001/jamapsychiatry.2013.4642. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Whittaker R, Dorey E, Bramley D, Bullen C, Denny S, Elley CR, et al. A theory-based video messaging mobile phone intervention for smoking cessation: Randomized controlled trial. J Med Internet Res. 2011;13:e10. doi: 10.2196/jmir.1553. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Brendryen H, Drozd F, Kraft P. A digital smoking cessation program delivered through internet and cell phone without nicotine replacement (happy ending): Randomized controlled trial. J Med Internet Res. 2008;10:e51. doi: 10.2196/jmir.1005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Free C, Knight R, Robertson S, Whittaker R, Edwards P, Zhou W, et al. Smoking cessation support delivered via mobile phone text messaging (txt2stop): A single-blind, randomised trial. Lancet. 2011;378:49–55. doi: 10.1016/S0140-6736(11)60701-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Naughton F, Jamison J, Boase S, Sloan M, Gilbert H, Prevost AT, et al. Randomized controlled trial to assess the short-term effectiveness of tailored web- and text-based facilitation of smoking cessation in primary care (iQuit in practice) Addiction. 2014;109:1184–93. doi: 10.1111/add.12556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Marasinghe RB, Edirippulige S, Kavanagh D, Smith A, Jiffry MT. Effect of mobile phone-based psychotherapy in suicide prevention: A randomized controlled trial in Sri Lanka. J Telemed Telecare. 2012;18:151–5. doi: 10.1258/jtt.2012.SFT107. [DOI] [PubMed] [Google Scholar]
- 39.Beiwinkel T, Kindermann S, Maier A, Kerl C, Moock J, Barbian G, et al. Using smartphones to monitor bipolar disorder symptoms: A pilot study. JMIR Ment Health. 2016;3:e2. doi: 10.2196/mental.4560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Barth J, Munder T, Gerger H, Nüesch E, Trelle S, Znoj H, et al. Comparative efficacy of seven psychotherapeutic interventions for patients with depression: A network meta-analysis. PLoS Med. 2013;10:e1001454. doi: 10.1371/journal.pmed.1001454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Cuijpers P, Smit F, Bohlmeijer E, Hollon SD, Andersson G. Efficacy of cognitive-behavioural therapy and other psychological treatments for adult depression: Meta-analytic study of publication bias. Br J Psychiatry. 2010;196:173–8. doi: 10.1192/bjp.bp.109.066001. [DOI] [PubMed] [Google Scholar]
- 42.Bandelow B, Reitt M, Röver C, Michaelis S, Görlich Y, Wedekind D. Efficacy of treatments for anxiety disorders: A meta-analysis. Int Clin Psychopharmacol. 2015;30:183–92. doi: 10.1097/YIC.0000000000000078. [DOI] [PubMed] [Google Scholar]
- 43.Michie S, Fixsen D, Grimshaw JM, Eccles MP. Specifying and reporting complex behaviour change interventions: The need for a scientific method. Implement Sci. 2009;4:40. doi: 10.1186/1748-5908-4-40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Lancaster T, Stead LF. Individual behavioural counselling for smoking cessation. Cochrane Database Syst Rev. 2005;2:CD001292. doi: 10.1002/14651858.CD001292.pub2. [DOI] [PubMed] [Google Scholar]
- 45.Stead LF, Lancaster T. Group behaviour therapy programmes for smoking cessation. Cochrane Database Syst Rev. 2005;2:CD001007. doi: 10.1002/14651858.CD001007.pub2. [DOI] [PubMed] [Google Scholar]
- 46.Ilardi SS, Craighead WE. The role of nonspecific factors in cognitive-behavior therapy for depression. Clin Psychol Sci Pract. 1994;1:138–55. [Google Scholar]
- 47.Chatoor I, Krupnick J. The role of non-specific factors in treatment outcome of psychotherapy studies. Eur Child Adolesc Psychiatry. 2001;10(Suppl 1):I19–25. doi: 10.1007/s007870170004. [DOI] [PubMed] [Google Scholar]
- 48.Rozental A, Andersson G, Boettcher J, Ebert DD, Cuijpers P, Knaevelsrud C, et al. Consensus statement on defining and measuring negative effects of internet interventions. Internet Interv. 2014;1:12–9. [Google Scholar]
- 49.Murray MC, O’Shaughnessy S, Smillie K, Van Borek N, Graham R, Maan EJ, et al. Health care providers' perspectives on a weekly text-messaging intervention to engage HIV-positive persons in care (WelTel BC1) AIDS Behav. 2015;19:1875–87. doi: 10.1007/s10461-015-1151-6. [DOI] [PubMed] [Google Scholar]
- 50.Becker S, Miron-Shatz T, Schumacher N, Krocza J, Diamantidis C, Albrecht UV. mHealth 2.0: Experiences, possibilities, and perspectives. JMIR Mhealth Uhealth. 2014;2:e24. doi: 10.2196/mhealth.3328. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Baranoski AS, Meuser E, Hardy H, Closson EF, Mimiaga MJ, Safren SA, et al. Patient and provider perspectives on cellular phone-based technology to improve HIV treatment adherence. AIDS Care. 2014;26:26–32. doi: 10.1080/09540121.2013.802282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Palmier-Claus JE, Rogers A, Ainsworth J, Machin M, Barrowclough C, Laverty L, et al. Integrating mobile-phone based assessment for psychosis into people's everyday lives and clinical care: A qualitative study. BMC Psychiatry. 2013;13:34. doi: 10.1186/1471-244X-13-34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Childress CA. Ethical issues in providing online psychotherapeutic interventions. J Med Internet Res. 2000;2:E5. doi: 10.2196/jmir.2.1.e5. [DOI] [PMC free article] [PubMed] [Google Scholar]