

Abstract
Background:
Specific learning disabilities (SLDs) are an important cause of academic underachievement in children and are also associated with comorbidities like attention deficit hyperactivity disorder (ADHD) which further have an impact on the child's education.
Aims:
To estimate the prevalence and psychosocial profile and psychiatric comorbidities in children with SLD in two settings, i.e., on special (remedial) education and schools and to compare the findings with normal children.
Materials and Methods:
This study was carried out in schools situated in urban and semi-urban areas and special education schools. A total of 96 children were chosen for the study. After taking informed consent from the parents, the details about socioeconomic status, family, developmental history, and school history of the children were collected on a semi-structured pro forma and then the children were screened for SLD. They were administered colored/standard progressive matrices and Malin's intelligence scale for assessing their intelligence quotient and NIMHANS SLD index and developmental psychopathology checklist to study psychopathology. Chi-square test and ANOVA were done.
Results:
The prevalence of SLD in schools is found out to be 6.6%. There was a significant association with prematurity, cesarean section, delayed speech, and family history of SLD. Among comorbidities of SLD, association with ADHD alone has been found to be significant.
Conclusion:
The most common type of SLD is combined type comorbid with ADHD. There is a need for early identification of learning disabilities in schools so that with early recognition and remedial intervention children can be helped with to cope with studies.
Keywords: Comorbidity, school children, specific learning disability
INTRODUCTION
Specific learning disabilities (SLDs) are a generic term that refers to a heterogeneous group of neurobehavioral disorders manifested by significant unexpected, specific, and persistent difficulties in the acquisition and use of efficient reading (dyslexia), writing (dysgraphia), or mathematical (dyscalculia) abilities despite conventional instruction, intact senses, normal intelligence, proper motivation, and adequate sociocultural opportunity.[1] International Classification of Diseases-10 describes them as specific developmental disorders of scholastic skills[2] and Diagnostic and Statistical Manual 4th edition - text revision (DSM-IV) as learning disorders[3] and DSM-5 as specific learning disorders.[4]
Dyslexia (reading disorder) is the most common among the learning disorders, affecting 80% of all those identified as learning-disabled.[5] The incidence of dyslexia in primary school children in India has been reported to be 2–18%, dysgraphia 14%, and dyscalculia 5.5%.[6,7,8]
Learning disorders usually do not exist in isolation. They are found most commonly associated with other cortical-based disorders such as other learning disorders, language disorders, motor disorders, and organization and executive function disability.[9,10] The most common comorbidities include attention deficit hyperactivity disorder (ADHD),[11] conduct disorder, oppositional defiant disorder, anxiety disorder, and depression.[12]
Need for the study
Keeping the paucity of literature regarding SLDs in India, this study aims to document the sociodemographic profile and psychiatric comorbidities in school children.
Aims and objectives of the study
To study the number of children having SLDs and comorbidities in school setting
To study the comorbidities in children with SLDs who are identified and on remedial education
To study the comorbidities in children who do not have SLDs
To study the difference in sociodemographic variables as well as a comorbidity in the three groups.
MATERIALS AND METHODS
It is a cross-sectional study. The study was conducted at two settings. In one, the data are collected from a group of SLD children in remedial schools (Dyslexia Association of Andhra Pradesh, Hyderabad). The other in two urban and two semi-urban schools all of them are nongovernment, private organized English medium schools. A total of 96 children were taken into the study.
They were divided into three groups:
Group 1 consists of thirty children who are already diagnosed as having an SLD by a psychiatrist and are on remedial education. After taking written informed consent from the parents, the details as per the intake pro forma are taken and parent is interviewed according to the developmental psychopathology checklist (DPCL). Subsequently, the child is administered colored progressive matrices (CPM)/standard progressive matrices (SPM), Malin's intelligence scale for Indian children (MISIC) and NIMHANS SLD index.
Group 2 consists of 32 children diagnosed for the first time at schools during the study. After taking permission from the school management, the teachers were given a checklist which identifies children having problems in academic achievement. Following the screening, children were administered SPM/CPM and those who scored more than the 50th percentile were shortlisted. After taking written informed consent from the parents and using the inclusion and exclusion criteria and information obtained from parents interview and intake pro forma and DPCL, the children were then administered MISIC and NIMHANS SLD index.
Group 3 constituted of 34 children who were not included in the list after administering the checklist; they were administered SPM/CPM. The parents of those children who scored more than the 50th percentile were interviewed and information was collected in intake pro forma and DPCL after taking consent. The children were then administered MISIC and NIMHANS SLD index.
Inclusion criteria
Age: 6–12 years, average intelligence quotient (IQ > 90).
Exclusion criteria
Borderline intelligence and mental retardation
Epilepsy
Neurological problems
Sensory impairment (auditory and visual).
Statistics
Statistical analysis was done using SPSS IBM SPSS Version 10.0. Means and standard deviation, Chi-square test, and ANOVA were used for analysis.
Tools used
Semi-structured intake pro forma
-
Intelligence tests:
-
Raven's progressive matrices[13]
- Standard progressive matrices: The booklet comprises five sets (A to E) of 12 items each.(children: 11–12 years)
- Colored progressive matrices: The booklet comprises three sets (A, Ab, B) of 12 items each (children up to 11 years). Progressive matrices are used as a screening instrument to rule out children with low IQ
-
MISIC[14]
- The MISIC is an Indian adaptation of Wechsler intelligence scale for children
-
The NIMHANS index for SLDs is a battery of tests used for confirming the diagnosis of SLD. It consists of two levels:[15] Level 1: (5–7 years of age); Level 2: (8–12 years)
Checklist to identify learning disabilities[16]
DPCL for children.[17]
The DPCL is a screening tool to assess psychopathology in children. The DPCL has 124 items and 6 subsections.
RESULTS
The number of SLD children is amounting to a total of 62. They comprised 40 males (M) and 22 females (F) with the gender distribution ratio (M/F) of 1.8:1 [Table 1].
Table 1.
Sociodemographic and personal data
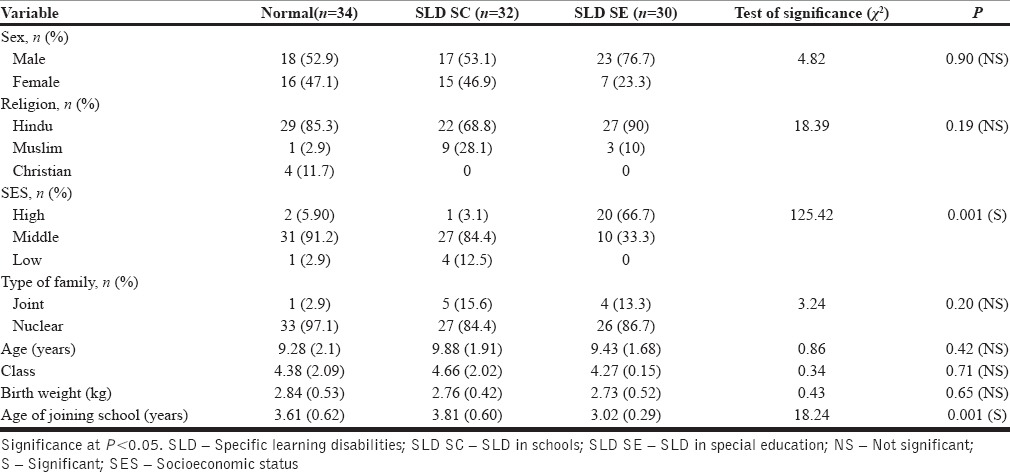
Prematurity (SLD special education group 6 (20%) and SLD schools group 1 (3.1%) (P = 0.006) and cesarean section (SLD special education group 63.4% and SLD schools group (31.3%) (P = 0.02) are found to be related to SLD in children. SLD children have delayed milestones particularly problems with speech, which is predominant in SLD special education group (36.7%) (P = 0.02).
SLD children have significant school problems in the form of school refusal, poor school performance, reading, writing, spelling, and arithmetic when compared to normal children. In SLD children, the problems with reading were found to be about 56 (90.3%), with comprehension 55 (88.7%), with arithmetic 17 (27.4%), with spelling 47 (75.8%), and with writing 28 (45.2%) [Table 2].
Table 2.
Break up of learning disabilities (NIMHANS specific learning disabilities index)
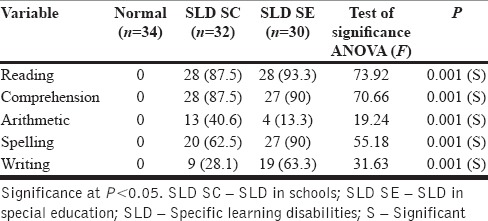
Table 3 shows various presentations of learning disabilities, pure reading disability is found in 22 (35.48%), writing disability in 1 (1.61%), dyscalculia in 3 (4.83%) whereas combined learning disability in 36 (58.06%), which is found to be the most common type of learning disability. Mathematic disability is found to occur less frequently in SLD special education group (16.7%) than in SLD schools group (34.4%).
Table 3.
Presentation of learning disabilities

Overall, the prevalence of SLD cases in schools is found to be 6.6%. Among the subtypes of learning disability, the prevalence of dyslexia is 4.58%, dysgraphia 0.2%, dyscalculia 0.63%, and combined learning disability in 7.5% respectively in school children.
Children with SLD committed significant errors on Bender Gestalt Test (BGT) (P = 0.001) as well as number cancellation test (P = 0.001). No statistical difference was found (P = 0.37) on scores on recall of BGT designs (memory) among three groups indicating that there is no statistical difference in memory in the three groups.
Table 4 shows the various variables under DPCL developmental history of children. Pre-, peri-, and post-natal problems in mother, epilepsy, head injury or infections in infancy, poor vision, speech and language – delay during childhood were found to be significant in children with SLD in both groups.
Table 4.
Developmental psychopathology checklist - developmental history
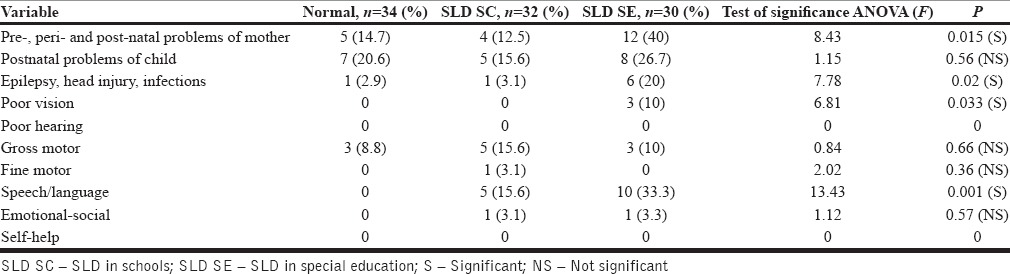
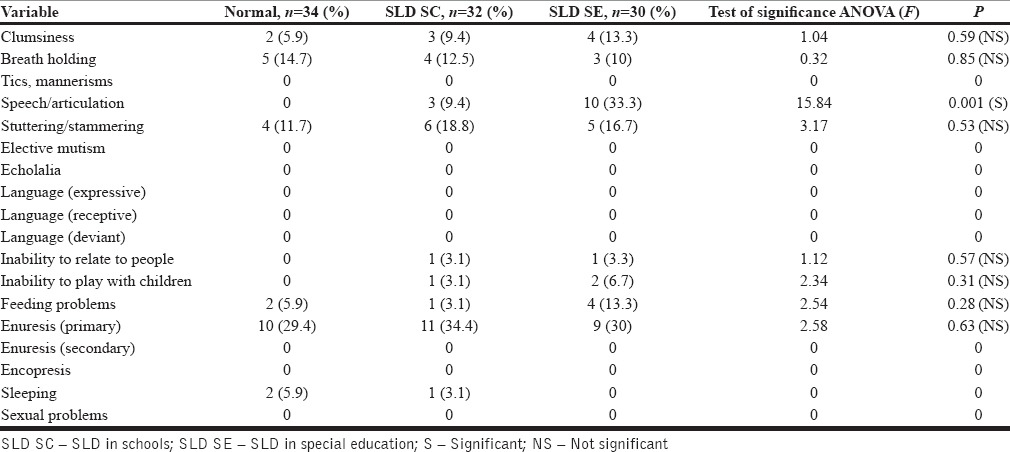
Table 5 shows various developmental problems. Only speech and articulation problems were found to be of highly statistically significant (P = 0.001) in children with SLD.
Table 5.
Developmental psychopathology checklist - developmental problems
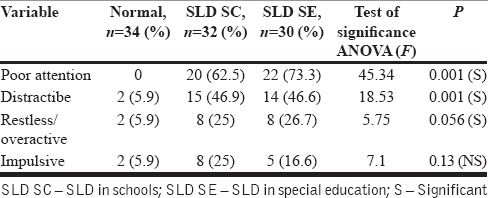
ADHD [Table 6] is found to be the most common comorbidity associated with SLD amounting to 26 (41.9%) with trends toward inattentive subtype.
Table 6.
Attention deficit hyperactivity disorder
Conduct disorder is found to be about 1 (3%) in SLD schools group with trends toward symptoms of disobedience. Emotional disorders are found to be about 2 (6.3%) in SLD schools group and 4 (13.3%) in SLD special education group. None of the children in both SLD groups met the criteria for somatic problems, psychosis, or obsessive-compulsive disorder.
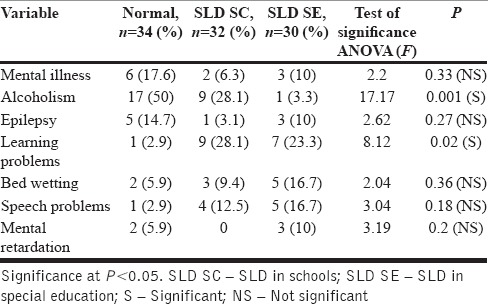
The family history of alcoholism was found to be significantly higher (P = 0.001) in normal children (50%) [Table 7]. The family history of learning problems has been found to be occurring more frequently in both SLD groups, which is found to be statistically significant (P = 0.02).
Table 7.
Developmental psychopathology checklist - family history
Stressors such as over expectation (26.7%) (P = 0.04) and over-involvement (36.7%) P = 0.001) by parents are found in children with SLD special education group.
DISCUSSION
The prevalence of SLD in Schools is found to be 6.6% with combined Learning disability being most common 7.5%. The male: female ratio in children with SLD if 1.8:1, indicating male preponderance. The similar findings were found by Karande et al.[11] in his study with a gender distribution ratio of 2.1:1. A higher representation of middle socioeconomic strata in SLD schools group (84.4%) and high socioeconomic strata in SLD special education group (66.7%) is observed. The higher representation of middle class is because the study sample is taken from urban and semi-urban areas, with English as the medium of instruction. It was being done due to the lack of standardized assessment tools for SLD in vernacular languages. This finding is similar to Karande et al.[11] study which states that SLD is higher (82%) in middle socioeconomic strata. The higher representation of high socioeconomic strata in SLD special education could be because the remedial or special education which was received by the students was from special educators/special education centers which charge a particular amount per month. Hence, most of the children who are receiving the special education are the ones whose parents could afford to pay them, apart from regular school fees.
Hindus are more represented in the study sample which goes with distribution of population. The findings are not in continuation of the previous study by Murnane[18] who stated that SLD are more common in a minority group and those belonging to low socioeconomic status.
The parents of children with SLD special education group belong to high education group (mothers 73.3% and fathers 46.7%) and most of them are professionals (mothers 23.3% and fathers 46.7%) while those parents of children with SLD schools group are educated up to secondary education (mothers 46.9% and fathers 25%). The previous study conducted by Kohli et al.[19] has noticed that parents of SLD children had 12–15 years of education.
Mean age of children with SLD in schools group is 9.88 years while the mean age of children with SLD in special education group is 9.43 years, respectively. The mean age of children with SLD as observed by Karande et al.[11] was 11.4 years. The majority of them belonged to is 4th standard. Children with SLD in special education group are joined in schools at an early age (i.e., 3.02 years) when compared to that of children with SLD schools group (3.81 years).
The difference is statistically significant (P = 0.001), indicating that children in SLD with special education group are being joined in the school at an earlier age than others and due to the high socioeconomic status of these parents of these children who keep them in special education schools for remedial methods. It is to be noted that none of the previous studies compared the age of the child at the time of joining school.
Prematurity (SLD special education group 20% and SLD schools group 3.1%) and cesarean section (SLD special education group 63.4% and SLD schools group 31.3%) are found to be related to SLD in children. The findings go with the result of previous study by Wood et al.,[20] where prematurity is found to be a risk factor with SLD. Furthermore, cesarean section also appears to be a risk factor. However, there are no such reports from the previous studies.
SLD children have delayed milestones particularly problems with speech, which is predominant in SLD special education group (36.7%) indicates that SLD special education group has developmental immaturity. The similar findings were reported by Karande et al.[11] in their study. Significant pre-, peri-, post-natal problems (40%) were found in mothers of children with SLD in special education group along with epilepsy, head injury or infections in infancy, poor vision, speech and language delay during childhood are found to be significant in both groups of SLD, clearly indicating that SLD is a developmental problem.
SLD children have significant school problems in the form of school refusal, poor school performance, reading, writing, spelling, and arithmetic when compared to normal children. In SLD children, the problems with reading were found to be about 90.3%, with comprehension 88.7%, with arithmetic 27.4%, with spelling 75.8%, and with writing 45.2%. Pure reading disability is found in 35.48%, writing disability in 1.61%, dyscalculia in 4.83% while combined learning disability in 58.06%, which is found to be the most common type of learning disability. Mathematic disability is found to occur less frequently in SLD special education group (16.7%) than in SLD schools group (34.4%). These findings are similar to the findings of Karande et al.[11] where combined subtype was represented more. However, compared to the study by Ramaa[21] where mathematic disability is found to be 5.98%, mathematic disabilities have found to occur less frequently in special education group; this could be probably due to the reason that most of the children brought to the special educators are having problems with reading and writing.
In this study, most common type of learning disability was found to be combined (reading + writing) 35.48% which was similar to a finding by Karande et al., 2007.[11] But as compared to the previous Indian studies, mathematic disabilities have found to occur less frequently in special education group, this could be probably due to the reason that most of the children brought to the special educators are having problems with reading, spelling, and writing.
Children with SLD committed statistically significant errors on BGT (P = 0.001) denoting perceptual and visuomotor integration problems in children with SLD. Furthermore, significant errors were committed in number cancellation test. This amounts to the high amount of inattentiveness seen in SLD and also the influence of other comorbid conditions like ADHD.
ADHD is found to be the most common comorbidity associated with SLD amounting to 41.9% with trends toward inattentive subtype. Analysis of the characteristics of the 26 (41.9%) children with ADHD in SLD group, it is found that there are 3 (11.5%) females and 23 (88.5%) males. On subtyping, the number of SLD children with ADHD inattentive type is found to be 11 (42.3%), ADHD hyperactive type 7 (26.9%), and combined type of ADHD in 8 (30.8%). The comorbidity of ADHD was about 35%.[12] In the present study, trends are toward inattentive type, whereas in other studies on Indian and Pakistani data found that combined subtype was more common.[22,23]
Conduct disorder is found to be about 3% in SLD schools group with trends toward symptoms of disobedience. Emotional disorders are found to be about 6.3% in SLD schools group and 13.3% in SLD special education group. None of the children in both SLD groups met the criteria for somatic problems, psychosis or obsessive compulsive disorder. On the whole, the comorbidities as assessed by DPCL showed significance on ADHD, conduct and emotional disorders which was not found in the study by Karande et al.[11] except for ADHD.
Significant family history of learning disabilities is found in children with both groups of SLD. Learning disorders in family history is found to be significant as also observed by Snowling et al.[24,25]
Stressors like over expectation and over involvement by parents are found in children with SLD special education group.
Limitations
The study was not conducted in government schools as the assessment of SLD in vernacular languages was not available. Hence, children with lower socioeconomic status are not represented in the study.
CONCLUSION
The prevalence of SLD in schools is found out to be 6.6%. There was a significant association with prematurity, cesarean section, delayed speech and family history of SLD. Among comorbidities of SLD, association with ADHD alone has been found to be significant.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
Dr. Niranjan, Clinical Psychologist, Child Psychiatric Department, Niloufor Hospital, Hyderabad, Mrs. Neela, Mrs. Urmila and Mrs. Pooja Jha, special educators, Hyderabad.
REFERENCES
- 1.Shapiro BK, Gallico RP. Learning disabilities. Pediatr Clin North Am. 1993;40:491–505. doi: 10.1016/s0031-3955(16)38546-7. [DOI] [PubMed] [Google Scholar]
- 2.World Health Organization. The International Classification of Diseases: Classification of Mental and Behavioral Disorders. Vol. 10. Geneva: World Health Organization; 1993. [Google Scholar]
- 3.American Psychiatric Association. Diagnostic and Statistical Manual-Text Revision (DSM-IV-TR) 4th ed. Washington, DC: American Psychiatric Association; 2000. [Google Scholar]
- 4.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Association; 2013. [Google Scholar]
- 5.Shaywitz SE. Dyslexia. Sci Am. 1996;275:98–104. doi: 10.1038/scientificamerican1196-98. [DOI] [PubMed] [Google Scholar]
- 6.Mittal SK, Zaidi I, Puri N, Duggal S, Rath B, Bhargava SK. Communication disabilities: Emerging problems of childhood. Indian Pediatr. 1977;14:811–5. [PubMed] [Google Scholar]
- 7.Shah BP, Khanna SA, Pinto N. Detection of learning disabilities in school children. Indian J Pediatr. 1981;48:767–71. doi: 10.1007/BF02758547. [DOI] [PubMed] [Google Scholar]
- 8.Ramaa S, Gowramma IP. A systematic procedure for identifying and classifying children with dyscalculia among primary school children in India. Dyslexia. 2002;8:67–85. doi: 10.1002/dys.214. [DOI] [PubMed] [Google Scholar]
- 9.Arnold EM, Goldston DB, Walsh AK, Reboussin BA, Daniel SS, Hickman E, et al. Severity of emotional and behavioral problems among poor and typical readers. J Abnorm Child Psychol. 2005;33:205–17. doi: 10.1007/s10802-005-1828-9. [DOI] [PubMed] [Google Scholar]
- 10.Mayes SD, Calhoun SL. Frequency of reading, math, and writing disabilities in children with clinical disorders. Learn Individ Differ. 2006;16:145. [Google Scholar]
- 11.Karande S, Satam N, Kulkarni M, Sholapurwala R, Chitre A, Shah N. Clinical and psychoeducational profile of children with specific learning disability and co-occurring attention-deficit hyperactivity disorder. Indian J Med Sci. 2007;61:639–47. [PubMed] [Google Scholar]
- 12.Kohli A, Malhotra S, Mohanty M, Khehra N, Kaur M. Specific learning disabilities in children: Deficits and neuropsychological profile. Int J Rehabil Res. 2005;28:165–9. doi: 10.1097/00004356-200506000-00011. [DOI] [PubMed] [Google Scholar]
- 13.Court JH, Raven J. Manual for Raven's Progressive Matrices and Vocabulary Scales. Section 7: Research and references: Summaries of normative, reliability, and validity studies and references to all sections. Oxford: Oxford University Press; 1995. San Antonio, TX: The Psychological Corporation. [Google Scholar]
- 14.Malins AJ. Manual for Malin's intelligence scale for Indian children (MISIC) Lucknow: Indian Psychological Corporation; 1969. [Google Scholar]
- 15.Hirisave U, Oommen A, Kapur M. Psychological Assessment of Children in the Clinical Setting. NIMHANS Index of Specific Learning Disabilities. Bangalore: Samudra Offset Printers; 2006. [Google Scholar]
- 16.Check List to Identify Learning Disabilities: (Department of Psychiatry, B.Y.L. Nair Hospital and T.N. Medical College) [Google Scholar]
- 17.Hirisave U, Oommen A, Kapur M. Psychological Assessment of Children in the Clinical Setting. Developmental Psychopathology Check List for Children (DPCL) Bangalore: Samudra Offset Printers; 2006. [Google Scholar]
- 18.Murnane RJ. Improving the education of children living in poverty. Future Child. 2007;17:161–82. doi: 10.1353/foc.2007.0019. [DOI] [PubMed] [Google Scholar]
- 19.Kohli A, Kaur M, Mohanty M, Malhotra S. Neuropsychological functioning in specific learning disorders – Reading, writing and mixed groups. J Indian Assoc Child Adolesc Ment Health. 2006;2:112–5. [Google Scholar]
- 20.Wood NS, Marlow N, Costeloe K, Gibson AT, Wilkinson AR. Neurologic and developmental disability after extremely preterm birth. EPICure Study Group. N Engl J Med. 2000;343:378–84. doi: 10.1056/NEJM200008103430601. [DOI] [PubMed] [Google Scholar]
- 21.Ramaa S. Two decades of research on learning disabilities in India. Dyslexia. 2000;6:268–83. doi: 10.1002/1099-0909(200010/12)6:4<268::AID-DYS177>3.0.CO;2-A. [DOI] [PubMed] [Google Scholar]
- 22.Malhi P, Singhi P. Spectrum of attention deficit hyperactivity disorders in children among referrals to psychology services. Indian Pediatr. 2000;37:1256–60. [PubMed] [Google Scholar]
- 23.Qureshi A, Thaver D. Cross sectional review of children with ADHD presenting to an outpatient psychiatric institute in Pakistan. J Pak Med Assoc. 2003;53:441–3. [PubMed] [Google Scholar]
- 24.Snowling MJ, Gallagher A, Frith U. Family risk of dyslexia is continuous: Individual differences in the precursors of reading skill. Child Dev. 2003;74:358–73. doi: 10.1111/1467-8624.7402003. [DOI] [PubMed] [Google Scholar]
- 25.Snowling MJ, Muter V, Carroll J. Children at family risk of dyslexia: A follow-up in early adolescence. J Child Psychol Psychiatry. 2007;48:609–18. doi: 10.1111/j.1469-7610.2006.01725.x. [DOI] [PubMed] [Google Scholar]