

Abstract
The dissemination of methicillin-resistant (MR) Staphylococcus aureus (SA) in community and health-care settings is of great concern and associated with high mortality and morbidity. Rapid detection of MRSA with short turnaround time can minimize the time to initiate appropriate therapy and further promote infection control. Early detection of MRSA directly from clinical samples is complicated by the frequent association of MRSA with methicillin-susceptible SA (MSSA) and coagulase-negative Staphylococcus (CoNS) species. Infection associated with true MRSA or MSSA is differentiated from CoNS, requires target specific primers for the presence of SA and mec A or nuc or fem A gene for confirmation of MR. Recently, livestock-associated MRSA carrying mec C variant complicates the epidemiology of MRSA further. Several commercial rapid molecular kits are available with a different combination of these targets for the detection of MRSA or MSSA. The claimed sensitivity and specificity of the currently available commercial kits is varying, because of the different target combination used for detection of SA and MR.
Keywords: Livestock-methicillin-resistant Staphylococcus aureus, methicillin-resistant Staphylococcus aureus, methicillin-susceptible Staphylococcus aureus, Xpert MRSA assay
Introduction
Methicillin-resistant (MR) Staphylococcus aureus (SA) is a major cause of hospital-acquired infection worldwide. In addition, dissemination of certain clones in the community has resulted in community-acquired MRSA causing severe infection in certain geographical regions. An example of this, is the spread of the hypervirulent USA 300 clones in the United States, causing significant morbidity and mortality through the community-onset skin and soft tissue infections and necrotizing pneumonia.[1] Unfortunately, the days when all community-acquired SA were methicillin susceptible (MS) and all hospital-acquired were MRSA are long gone. The mortality rate with critical MRSA infection is approximately two times higher than with MSSA infection.[2]
Delay in placing a patient on appropriate antibiotic therapy is an independent predictor for a longer hospital stay, hospital-acquired infection, and infection-related mortality.[3,4] Targeted therapy is based on the conventional culture and susceptibility testing which takes at least 24–48 h. In the last few years, various commercial rapid tests have been developed for use in clinical laboratories that detect MRSA directly from nasal swabs and blood cultures (BC). These new methodologies have the advantage of faster turnaround time (TAT) and can minimize the time to initiate optimal antimicrobial therapy and further reduce the cost of healthcare. In this paper, we discuss the available rapid molecular tests and their ongoing evolution to ensure accurate detection of MRSA from a patient specimen.
The Clinical Utility of Rapid Methicillin-Resistant Staphylococcus Aureus Detection
Rapid detection of MRSA from nasal swabs is essential to adequately identify colonized individuals and provide appropriate infection control. Furthermore, rapid detection of MRSA from clinical samples can also helps to optimize the care of the severely unwell patient. A common clinical conundrum is the patient who presents with sepsis and is found to have Gram-positive cocci in clusters (GPCCL) in the blood. This could be SA, a highly pathogenic organism, or coagulase-negative Staphylococcus (CoNS). CoNS accounts for 60%–80%[5,6] of GPCCL-positive BC and in the patient without central line or prosthetic material, usually represents contamination of the BC by organisms on the skin. Thus, it is essential that rapid tests can distinguish CoNS from SA with high accuracy.
Once SA is identified, a further clinical conundrum exists; is this MSSA or MRSA? These patients are usually managed with broad-spectrum antibiotics until the susceptibility of the organism is fully established 24 h later. If the clinicians give empirical antibiotics for MSSA to a severely unwell patient with a MRSA infection, that patient has an increased risk of mortality. However, the reverse is also true. A number of studies have shown that antimicrobials targeting MRSA, such as vancomycin, result in prolonged bacteremia and higher mortality rates than the β-lactams used to treat MSSA, such as cloxacillin.[7] One retrospective study looking at MSSA bacteremia in intravenous drug users found the mortality rate of 39.4% in those treated with vancomycin but only 11.4% in those treated with flucloxacillin. In a subgroup of patients who received vancomycin for 48 h while awaiting susceptibility results, the mortality was 40%, suggesting that choice of empiric therapy has a large effect on clinical outcome.[8] Ideally rapid tests can distinguish MRSA from MSSA with a high degree of accuracy.
A few prospective studies have analyzed the utility of rapid diagnostic tests for MRSA and its influence on the prescription of antimicrobials. Implementation of rapid diagnostics results in timely effective therapy which significantly reduces the length of hospital stay and cost.[9,10] A systemic review and meta-analysis compared the TAT of BD GeneOhm with the chromogenic medium. In comparison, the mean TAT of BD GeneOhm (13.2–21.6 h) was shorter than chromogenic medium (46.2–79.2 h) for detection of SA.[11] Rapid detection of SA resulted in 21% reduction in the number of patients treated with anti-MRSA drugs. In addition, among patients with negative BC for SA, the mean duration of antibiotic therapy was reduced from 19.7 to 12.2 h, and there was a mean reduction of 6.2 days in a hospital stay. On implementation of rapid molecular tests, the time to optimal therapy fell from 44.6 to 38.4 h among patients with MSSA bacteremia.[12,13] Thus, rapid identification of MRSA has a direct impact on patient care and infection control.
Molecular Detection of Methicillin-Resistant Staphylococcus Aureus
MRSA is encoded by the mec A gene located on the mobile genetic element staphylococcal cassette chromosome mec (SCCmec). To date, there are at least 11 SCCmec types (I–XI), and numerous subtypes (IVa, IVb, IVc, IVd, IVg, and IVh) have been described in MRSA.[14,15] Molecular detection of MRSA requires target-specific detection of SA (via the nuc, gyrB, or the Staphylococcus protein A gene) together with identification of MR (via SCCmec-orfX, fem A, or mec A).[16,17,18,19] Different kits use different combinations of these targets which are listed in Table 1. However, the emergence of novel mec variants means that targets for detection of MR need continuous reevaluation.
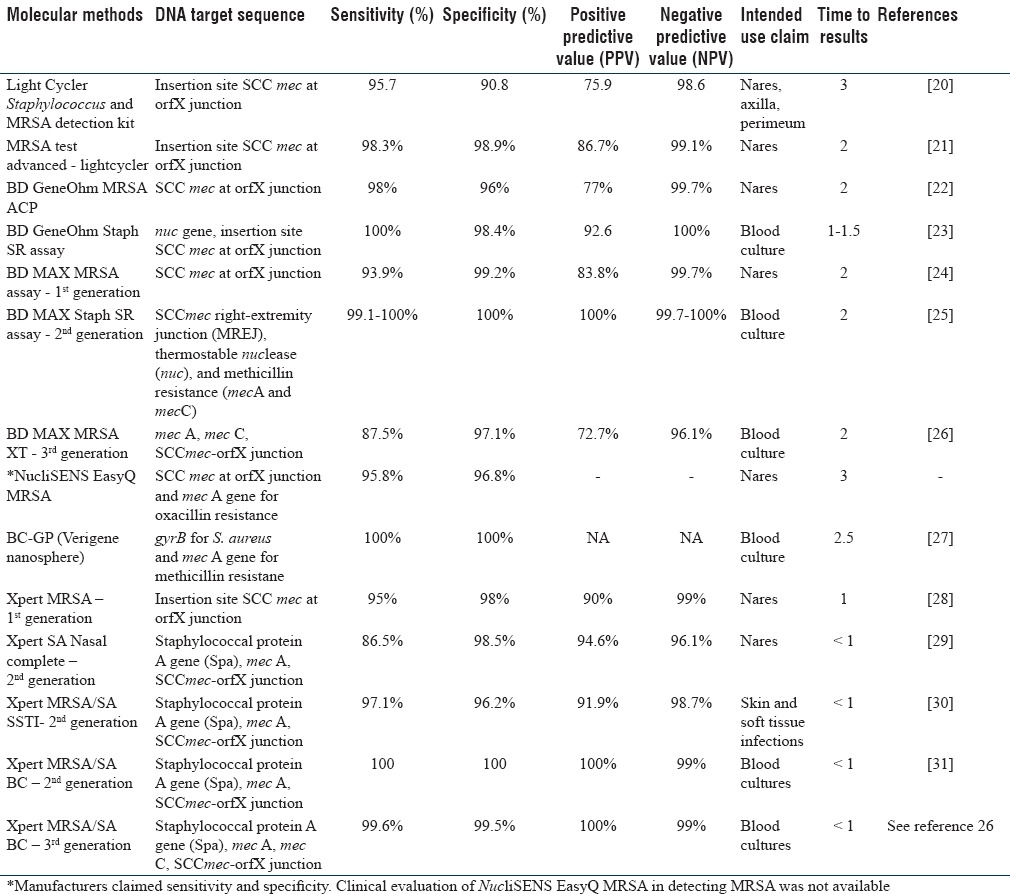
Table 1.
Sensitivity, Specificity and Predictive Value of Various Molecular Methods and Nucleic Acid Region/Targets in Detecting Methicillin Resistant S. Aureus (Mrsa)
Detection of Methicillin-Resistant Staphylococcus Aureus From Swabs (Nasal/Wound)
In 2004, Huletsky et al. introduced a novel real-time polymerase chain reaction (PCR) targeting the SCCmec-orfX junction for rapid identification of MRSA. The target SCCmec-orfX is in the highly conserved region of Staphylococcus sp.[32] This was followed by several other assays detecting the same target including BD GeneOhm MRSA ACP, BD MAX MRSA, Xpert MRSA, and MRSA test. Unfortunately, these tests had two limitations. First, they did not differentiate between MRSA and MR-CoNS as the SCCmec-orfX junction is present in all staphylococci. As most patients have nasal colonization by CoNS, many of which are MR but are rarely pathogenic, this was a big problem. Second, they did not directly detect mec A gene which encodes MR but rather depended on the integration of the SCCmec cassette proximal to orfX as a surrogate marker of resistance. This resulted in a specificity of only 90.4%; MS isolates with an SCCmec element but which lacked the mec A gene were falsely reported as positive. These were known as empty cassettes or mec A dropouts. However, these tests had the major advantage of being easy to perform with rapid TAT of <1 h.
From 2008 onward, FDA-approved second-generation kits became available. These included Xpert SA Nasal Complete for the screening of the anterior nares (2008) and Xpert MRSA/SA SSTI for wound specimens (2010). These kits targeted three genes; the SCCmec-orfX junction, the mec A gene, and the staphylococcal protein A (spa) gene [Figure 1]. The highly conserved SCCmec-orfX identifies all staphylococci, the spa gene identifies only SA, and the mec A gene identifies MR in staphylococci. All three targets must amplify for the isolate to be deemed as MRSA. Detection of SA based on these targets was well documented with the sensitivity and specificity of 100% and 99.5% for MSSA and for MRSA with sensitivity and specificity of 100%, respectively [Table 1].
Figure 1.
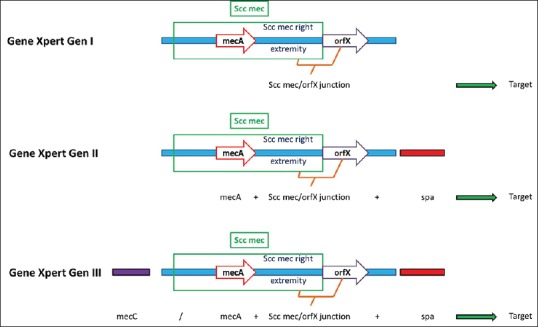
Targets used in the different generation of polymerase chain reaction for detection of methicillin-resistant Staphylococcus aureus. Initially, methicillin-resistant Staphylococcus aureus detection was based on SCCmec/orfX junction. Later, improvised automated systems consist of target specific for mec A gene and SCCmec/orfX junction. An additional target of mec C was provided for detection of methicillin-resistant Staphylococcus aureus containing mec C gene
Detection of Staphylococcus Aureus and Methicillin-Resistant Staphylococcus Aureus Directly From Blood Culture
The Staph SR (BD GeneOhm), the Gram-positive BC (BC-GP, Verigene), and the Xpert MRSA/SA BC (second generation) can rapidly distinguish SA from CoNS and MR from MS isolates directly from BC. They have sensitivity, specificity, and positive predictive value of 100%, and a negative predictive value of 99% [Table 1].
Staph SR uses the nuc gene to distinguish SA from CoNS but continues to use the orfX-SCCmec junction to establish MR with its associated problems. BC-GP uses gyrB gene (which codes for DNA gyrase subunit B) and mec A for detection of SA and MR, respectively. However, this gyrB gene is also found in other Gram-positive pathogens such as Streptococcus pneumoniae and Streptococcus anginosus group. The reliability of this gene in detecting and differentiating SA from other Gram-positive pathogen is not well established.
Like other Xpert MRSA assays such as Xpert MRSA nasal complete and Xpert MRSA/SA SSTI, the Xpert MRSA/SA BC detects the spa gene, the orfX–SCCmec junction, and the mec A gene. Compared with conventional phenotypic results, the Xpert MRSA/SA BC has a sensitivity and specificity of 100% and 96.7%, respectively, in differentiating SA from non-SA isolates. A prospective study evaluating the performance of Xpert MRSA/SA BC assay and its impact on antibiotic prescription among GPCCL-positive BC found that the proportion of MRSA bacteremic patients receiving optimal vancomycin therapy was increased from 46% to 100%. Vancomycin therapy was stopped in 27% of patients with MSSA or non-SA bacteremia and antibiotics were stopped completely in 16% of patients.[33] Similarly, the time taken to initiate appropriate antibiotics in patients with MSSA bacteremia was reduced from 49.8 h with conventional testing to 5.2 h while using Xpert MRSA/SA BC for detection of SA-associated bacteremia.[34]
Detection of MEC C Gene Directly From Blood Culture
As genetic mechanisms evolve in MRSA, variations in the mec gene may appear which are not detected by the current molecular assays. In 2011, a new mec A gene homolog, mecALGA251, was identified in isolates from humans and dairy cattle and became known as livestock-associated MRSA. The International Working Group on the Classification of Staphylococcal Cassette Chromosome Elements has since suggested that the mecALGA251 gene should be renamed as mec C.[35]
mec C is a mec A homolog identified on the SCCmec XI mobile genetic element. It encodes a protein with <63% amino acid identity with penicillin-binding protein 2a (PBP2a) and is resistant to methicillin.[36,37] Unfortunately, mec C is not detectable with routine diagnostics including the latex agglutination test for PBP2a and mec A-specific PCR due to variation in the protein PBP2a structure and nucleotide variation in the primer region. False negative results may lead to uncontrolled transmission of undetected MRSA strains, and outbreaks of mec C containing MRSA have now been reported in humans across Europe. The mec C MRSA now accounts for 3%–4% of all new MRSA cases in humans[38] necessitating the inclusion of mec C-specific targets into routine MRSA diagnostic kits.
Three third-generation kits are now available to detect mec C alongside mec A MRSA including Xpert MRSA Gen 3, BD MAX MRSA XT (eXTended Detection Technology), and BD MAX Staph SR. The sensitivity and specificity of Xpert MRSA Gen 3 have been reported as 95.7% and 100%, respectively, while that of BD MAX MRSA XT was reported as 87.5% and 97.1%, respectively [Table 1].
Although commercial kits are designed and updated to cover emerging clones, molecular diagnosis of MRSA remains challenging. The mutation, deletion, insertion, and rearrangement in SCCmec genetic element result in the evolution of MRSA strains with new SCCmec types or mec A homologs. These SCCmec or mec A homolog variants may not be detected by currently available primers, and so continuous evaluation of the performance of these test in clinical settings is warranted. Designing of new primers in this scenario is crucial to ensure detection of most prevalent MRSA strains.
Conclusion
Dissemination of MRSA strains in hospital and community settings continues to be an important problem worldwide. Rapid molecular methods are a valuable tool for detection of MRSA directly from a patient specimen. Molecular assays can detect SA and MRSA accurately from specimens such as nasal swabs and BC with the TAT of 1–3 h. Early identification of SA, particularly detection of MRSA isolates from positive BC, increases the likelihood of patients receiving appropriate antibiotic therapy, reduces the time to appropriate therapy, and further decreases the length of stay, hospital cost, and mortality. To achieve improved care for patients with SA bacteremia, an ideal diagnostic molecular kit for early detection of SA (spa, nuc gene), MR (mec A/C) with better accuracy indices is essential. Further, rapid molecular assays targeting SCCmec should be continuously monitored to ensure their claimed sensitivity and specificity in detecting MRSA strains is maintained. Genetic evolution of MRSA may affect the accuracy indices of the kit. Today's standard may not hold good tomorrow due to the evolving nature of genetic elements in MRSA.
Financial support and sponsorship
None
Conflicts of interest
There are no conflicts of interest.
References
- 1.Moran GJ, Krishnadasan A, Gorwitz RJ, Fosheim GE, McDougal LK, Carey RB, et al. Methicillin-resistant S. aureus infections among patients in the emergency department. N Engl J Med. 2006;355:666–74. doi: 10.1056/NEJMoa055356. [DOI] [PubMed] [Google Scholar]
- 2.Turnidge JD, Kotsanas D, Munckhof W, Roberts S, Bennett CM, Nimmo GR, et al. Staphylococcus aureus bacteraemia: A major cause of mortality in Australia and New Zealand. Med J Aust. 2009;191:368–73. doi: 10.5694/j.1326-5377.2009.tb02841.x. [DOI] [PubMed] [Google Scholar]
- 3.Lodise TP, McKinnon PS, Swiderski L, Rybak MJ. Outcomes analysis of delayed antibiotic treatment for hospital-acquired Staphylococcus aureus bacteremia. Clin Infect Dis. 2003;36:1418–23. doi: 10.1086/375057. [DOI] [PubMed] [Google Scholar]
- 4.Paul M, Kariv G, Goldberg E, Raskin M, Shaked H, Hazzan R, et al. Importance of appropriate empirical antibiotic therapy for methicillin-resistant Staphylococcus aureus bacteraemia. J Antimicrob Chemother. 2010;65:2658–65. doi: 10.1093/jac/dkq373. [DOI] [PubMed] [Google Scholar]
- 5.Weinstein MP. Blood culture contamination: Persisting problems and partial progress. J Clin Microbiol. 2003;41:2275–8. doi: 10.1128/JCM.41.6.2275-2278.2003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hall KK, Lyman JA. Updated review of blood culture contamination. Clin Microbiol Rev. 2006;19:788–802. doi: 10.1128/CMR.00062-05. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Gentry CA, Rodvold KA, Novak RM, Hershow RC, Naderer OJ. Retrospective evaluation of therapies for Staphylococcus aureus endocarditis. Pharmacotherapy. 1997;17:990–7. [PubMed] [Google Scholar]
- 8.Lodise TP, Jr, McKinnon PS, Levine DP, Rybak MJ. Impact of empirical-therapy selection on outcomes of intravenous drug users with infective endocarditis caused by methicillin-susceptible Staphylococcus aureus. Antimicrob Agents Chemother. 2007;51:3731–3. doi: 10.1128/AAC.00101-07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Brown J, Paladino JA. Impact of rapid methicillin-resistant Staphylococcus aureus polymerase chain reaction testing on mortality and cost effectiveness in hospitalized patients with bacteraemia: A decision model. Pharmacoeconomics. 2010;28:567–75. doi: 10.2165/11533020-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 10.Schweizer ML, Furuno JP, Harris AD, Johnson JK, Shardell MD, McGregor JC, et al. Comparative effectiveness of nafcillin or cefazolin versus vancomycin in methicillin-susceptible Staphylococcus aureus bacteremia. BMC Infect Dis. 2011;11:279. doi: 10.1186/1471-2334-11-279. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Polisena J, Chen S, Cimon K, McGill S, Forward K, Gardam M. Clinical effectiveness of rapid tests for methicillin resistant Staphylococcus aureus (MRSA) in hospitalized patients: A systematic review. BMC Infect Dis. 2011;11:336. doi: 10.1186/1471-2334-11-336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Bauer KA, West JE, Balada-Llasat JM, Pancholi P, Stevenson KB, Goff DA. An antimicrobial stewardship program's impact with rapid polymerase chain reaction methicillin-resistant Staphylococcus aureus/S. aureus blood culture test in patients with S. aureus bacteremia. Clin Infect Dis. 2010;51:1074–80. doi: 10.1086/656623. [DOI] [PubMed] [Google Scholar]
- 13.Parta M, Goebel M, Thomas J, Matloobi M, Stager C, Musher DM. Impact of an assay that enables rapid determination of Staphylococcus species and their drug susceptibility on the treatment of patients with positive blood culture results. Infect Control Hosp Epidemiol. 2010;31:1043–8. doi: 10.1086/656248. [DOI] [PubMed] [Google Scholar]
- 14.Turlej A, Hryniewicz W, Empel J. Staphylococcal cassette chromosome mec (SCCmec) classification and typing methods: An overview. Pol J Microbiol. 2011;60:95–103. [PubMed] [Google Scholar]
- 15.International Working Group on the Classification of Staphylococcal Cassette Chromosome Elements (IWG-SCC). Classification of staphylococcal cassette chromosome mec (SCCmec): Guidelines for reporting novel SCCmec elements. Antimicrob Agents Chemother. 2009;53:4961–7. doi: 10.1128/AAC.00579-09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Brakstad OG, Maeland JA, Chesneau O. Comparison of tests designed to identify Staphylococcus aureus thermostable nuclease. APMIS. 1995;103:219–24. [PubMed] [Google Scholar]
- 17.Kim JU, Cha CH, An HK, Lee HJ, Kim MN. Multiplex real-time PCR assay for detection of methicillin-resistant Staphylococcus aureus (MRSA) strains suitable in regions of high MRSA endemicity. J Clin Microbiol. 2013;51:1008–13. doi: 10.1128/JCM.02495-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kobayashi N, Wu H, Kojima K, Taniguchi K, Urasawa S, Uehara N, et al. Detection of mecA, femA, and femB genes in clinical strains of staphylococci using polymerase chain reaction. Epidemiol Infect. 1994;113:259–66. doi: 10.1017/s0950268800051682. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Sullivan KV, Turner NN, Roundtree SS, Young S, Brock-Haag CA, Lacey D, et al. Rapid detection of Gram-positive organisms by use of the Verigene Gram-positive blood culture nucleic acid test and the BacT/Alert pediatric FAN system in a multicenter pediatric evaluation. J Clin Microbiol. 2013;51:3579–84. doi: 10.1128/JCM.01224-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Levi K, Towner KJ. Rapid detection of methicillin-resistant Staphylococcus aureus from screening enrichment broths by real-time PCR. Eur J Clin Microbiol Infect Dis. 2005;24:423–7. doi: 10.1007/s10096-005-1336-4. [DOI] [PubMed] [Google Scholar]
- 21.Patel PA, Robicsek A, Grayes A, Schora DM, Peterson KE, Wright MO, et al. Evaluation of multiple real-time PCR tests on nasal samples in a large MRSA surveillance program. Am J Clin Pathol. 2015;143:652–8. doi: 10.1309/AJCPMDY32ZTDXPFC. [DOI] [PubMed] [Google Scholar]
- 22.Paule SM, Hacek DM, Kufner B, Truchon K, Thomson RB, Jr, Kaul KL, et al. Performance of the BD GeneOhm methicillin-resistant Staphylococcus aureus test before and during high-volume clinical use. J Clin Microbiol. 2007;45:2993–8. doi: 10.1128/JCM.00670-07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Stamper PD, Cai M, Howard T, Speser S, Carroll KC. Clinical validation of the molecular BD GeneOhm StaphSR assay for direct detection of Staphylococcus aureus and methicillin-resistant Staphylococcus aureus in positive blood cultures. J Clin Microbiol. 2007;45:2191–6. doi: 10.1128/JCM.00552-07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Dalpke AH, Hofko M, Zimmermann S. Comparison of the BD Max methicillin-resistant Staphylococcus aureus (MRSA) assay and the BD GeneOhm MRSA achromopeptidase assay with direct- and enriched-culture techniques using clinical specimens for detection of MRSA. J Clin Microbiol. 2012;50:3365–7. doi: 10.1128/JCM.01496-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ellem JA, Olma T, O’Sullivan MV. Rapid Detection of methicillin-resistant Staphylococcus aureus and methicillin-susceptible S. aureus directly from positive blood cultures by use of the BD Max StaphSR assay. J Clin Microbiol. 2015;53:3900–4. doi: 10.1128/JCM.02155-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Lepainteur M, Delattre S, Cozza S, Lawrence C, Roux AL, Rottman M. Comparative evaluation of two PCR-based methods for detection of methicillin-resistant Staphylococcus aureus (MRSA): Xpert MRSA Gen 3 and BD-Max MRSA XT. J Clin Microbiol. 2015;53:1955–8. doi: 10.1128/JCM.03679-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Wojewoda CM, Sercia L, Navas M, Tuohy M, Wilson D, Hall GS, et al. Evaluation of the Verigene Gram-positive blood culture nucleic acid test for rapid detection of bacteria and resistance determinants. J Clin Microbiol. 2013;51:2072–6. doi: 10.1128/JCM.00831-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Rossney AS, Herra CM, Brennan GI, Morgan PM, O’Connell B. Evaluation of the Xpert methicillin-resistant Staphylococcus aureus (MRSA) assay using the GeneXpert real-time PCR platform for rapid detection of MRSA from screening specimens. J Clin Microbiol. 2008;46:3285–90. doi: 10.1128/JCM.02487-07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Patel PA, Schora DM, Peterson KE, Grayes A, Boehm S, Peterson LR. Performance of the Cepheid Xpert ® SA nasal complete PCR assay compared to culture for detection of methicillin-sensitive and methicillin-resistant Staphylococcus aureus colonization. Diagn Microbiol Infect Dis. 2014;80:32–4. doi: 10.1016/j.diagmicrobio.2014.05.019. [DOI] [PubMed] [Google Scholar]
- 30.Wolk DM, Struelens MJ, Pancholi P, Davis T, Della-Latta P, Fuller D, et al. Rapid detection of Staphylococcus aureus and methicillin-resistant S. aureus (MRSA) in wound specimens and blood cultures: Multicenter preclinical evaluation of the Cepheid Xpert MRSA/SA skin and soft tissue and blood culture assays. J Clin Microbiol. 2009;47:823–6. doi: 10.1128/JCM.01884-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Spencer DH, Sellenriek P, Burnham CA. Validation and implementation of the GeneXpert MRSA/SA blood culture assay in a pediatric setting. Am J Clin Pathol. 2011;136:690–4. doi: 10.1309/AJCP07UGYOKBVVNC. [DOI] [PubMed] [Google Scholar]
- 32.Huletsky A, Giroux R, Rossbach V, Gagnon M, Vaillancourt M, Bernier M, et al. New real-time PCR assay for rapid detection of methicillin-resistant Staphylococcus aureus directly from specimens containing a mixture of staphylococci. J Clin Microbiol. 2004;42:1875–84. doi: 10.1128/JCM.42.5.1875-1884.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Davies J, Gordon CL, Tong SY, Baird RW, Davis JS. Impact of results of a rapid Staphylococcus aureus diagnostic test on prescribing of antibiotics for patients with clustered gram-positive cocci in blood cultures. J Clin Microbiol. 2012;50:2056–8. doi: 10.1128/JCM.06773-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kothari A, Morgan M, Haake DA. Emerging technologies for rapid identification of bloodstream pathogens. Clin Infect Dis. 2014;59:272–8. doi: 10.1093/cid/ciu292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.García-Álvarez L, Holden MT, Lindsay H, Webb CR, Brown DF, Curran MD, et al. Meticillin-resistant Staphylococcus aureus with a novel mecA homologue in human and bovine populations in the UK and Denmark: A descriptive study. Lancet Infect Dis. 2011;11:595–603. doi: 10.1016/S1473-3099(11)70126-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Ballhausen B, Kriegeskorte A, Schleimer N, Peters G, Becker K. The mecA homolog mecC confers resistance against ß-lactams in Staphylococcus aureus irrespective of the genetic strain background. Antimicrob Agents Chemother. 2014;58:3791–8. doi: 10.1128/AAC.02731-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Paterson GK, Harrison EM, Holmes MA. The emergence of mecC methicillin-resistant Staphylococcus aureus. Trends Microbiol. 2014;22:42–7. doi: 10.1016/j.tim.2013.11.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Petersen A, Stegger M, Heltberg O, Christensen J, Zeuthen A, Knudsen LK, et al. Epidemiology of methicillin-resistant Staphylococcus aureus carrying the novel mecC gene in Denmark corroborates a zoonotic reservoir with transmission to humans. Clin Microbiol Infect. 2013;19:E16–22. doi: 10.1111/1469-0691.12036. [DOI] [PubMed] [Google Scholar]