

Abstract
Colorectal cancer, which is the leading cancer in Singapore, can be prevented by increased use of screening and polypectomy. A range of screening strategies such as stool-based tests, flexible sigmoidoscopy, colonoscopy and computed tomography colonography are available, each with different strengths and limitations. Primary care physicians should discuss appropriate screening modalities with their patients, tailored to their individual needs. Physicians, patients and the government should work in partnership to improve uptake of colorectal cancer screening to reduce the morbidity and mortality from colorectal cancer.
Keywords: colorectal cancer, polypectomy, screening
55-year-old Mr Tan visited your clinic for a routine medical check-up. He had a history of well-controlled hyperlipidaemia and smoked 2–3 cigarettes per day. His uncle was diagnosed with colorectal cancer at 72 years of age. Mr Tan had no symptoms. You raised the issue of colorectal cancer screening during the consultation. He had heard many unpleasant stories about colonoscopy, including the bowel preparation protocol, and did not like the idea of having an instrument inserted into his colon. He had also heard that colonoscopy is a major procedure requiring general anaesthesia. Mr Tan said that he had sent his stool to the Health Promotion Board for a free test last year, and was told that it was normal. He felt that he was not at risk and there was no further need to screen for colorectal cancer.
HOW COMMON IS THIS IN MY PRACTICE?
Colorectal cancer (CRC) is an important health problem worldwide. It is the most common cancer in Singapore: 9,320 new cases of CRC were diagnosed between 2010 and 2014,(1) giving a crude incidence of 48.9 per 100,000. The incidence of CRC in Singapore is among the highest in the world. Risk factors for developing CRC are older age, male gender, family history, Chinese race, smoking and obesity.(2) Many patients with CRC are diagnosed at Stage III or later, which is associated with poor survival. CRC screening can help to detect and remove pre-malignant lesions, such as colonic adenoma, or diagnose early asymptomatic cancer to improve outcomes. However, a successful screening programme requires concerted efforts from family doctors, specialists and the government to improve uptake.
WHAT IS COLORECTAL CANCER SCREENING?
Screening is defined as the application of tests or procedures for the early detection of disease in asymptomatic people.(3) CRC can arise from colorectal adenomas, giving rise to the classic adenoma-carcinoma sequence of pathogenesis as depicted by Morson et al.(4,5) It can also arise from flat neoplasms and serrated adenomas. The average time taken for the evolution from small adenoma to cancer (‘polyp dwell time’) has not been established, but indirect evidence suggests that it takes an average of about ten years for an adenomatous polyp, particularly one that is < 1 cm in diameter, to develop into invasive cancer.(6) This long period of progression from polyp to cancer provides the rationale behind CRC screening: it allows detection and removal of adenomas (i.e. polypectomy) or early-stage CRC that is asymptomatic. Removal of the precursors of cancers can prevent CRC. CRC screening should begin at 50 years of age. This is supported by the updated Asia-Pacific consensus recommendations on colorectal cancer screening,(2) as well as the United States Preventive Services Task Force (USPSTF) recommendation statement,(7) as it has been shown that screening adults aged 50–75 years reduces CRC mortality.
Screening tests for CRC include stool-based and direct visualisation tests. Table I summarises the characteristics of each CRC screening strategy. It was demonstrated that any form of screening for colorectal cancer is cost-effective compared to no screening.
Table I.
Characteristics of colorectal cancer screening strategies.(7)

Stool-based tests
The three stool-based tests are: (a) guaiac-based faecal occult blood tests (gFOBT); (b) faecal immunochemical tests for haemoglobin (FIT); and (c) multitargeted stool DNA tests (FIT-DNA). Both gFOBT and FIT detect the presence of components of haemoglobin in faeces. Several randomised clinical trials (RCTs)(8-12) have shown that biennial or annual screening with gFOBT reduces colorectal cancer mortality. Biennial screening with Hemoccult II® resulted in a reduction in CRC-specific mortality, from 9% to 22% after 2–9 rounds of screening with 11–30 years of follow-up,(9-12) whereas annual screening with Hemoccult II, after 11 rounds of screening, resulted in a greater reduction of 32% in CRC-specific mortality than biennial screening at 30 years of follow-up.(8)
FIT uses antibodies raised against the globin moiety of human haemoglobin and has improved sensitivity compared to gFOBT for detecting colorectal cancer.(13) With a single stool specimen, its sensitivity and specificity for CRC was demonstrated to be 73%–88% and 91%–96%, respectively.(14,15) FIT-based screening programmes were associated with a 22% reduction in CRC mortality. Moreover, the advantages of FIT over gFOBT include: (a) it has increased specificity, as the antibodies bind only to human globin; (b) it is not confounded by blood loss proximal to the colon; (c) it is unlikely to be affected by antioxidants such as vitamin C or vegetable peroxidases; (d) it requires fewer stool samples (one compared with three); and (e) analysis can be automated. FIT-DNA is an emerging screening technique that combines FIT with testing for altered DNA biomarkers in colorectal cancer cells shed into the stool. It has increased sensitivity but lower specificity than the use of FIT alone for detecting colorectal cancer.(16)
Direct visualisation tests
Flexible sigmoidoscopy
Flexible sigmoidoscopy examines the distal part (descending or left-sided) of the colon. Five randomised trials of screening sigmoidoscopy have shown a decrease in cancer incidence and colorectal cancer mortality.(17-21) Using Markov modelling analysis, Dan et al showed that performing single sigmoidoscopies on individuals in Singapore when they are 60 years of age is the cheapest screening strategy; it would reduce CRC incidence by 19% and mortality by 16%, compared with no screening.(22) It is important to emphasise, however, that all studies using flexible sigmoidoscopy showed no reduction in proximal CRC incidence, which is not surprising, as the examination is limited to the left colon. Flexible sigmoidoscopy combined with FIT has also been studied in a randomised controlled trial(17) and was found to reduce the CRC-specific mortality rate more than flexible sigmoidoscopy alone. It is potentially an attractive option for patients who want endoscopic screening but prefer limited exposure to colonoscopy and want to avoid the full bowel preparation regime.
Colonoscopy
Colonoscopy is considered the ‘gold standard’ test for CRC screening. There are no randomised controlled trials on the effectiveness of screening colonoscopy to reduce CRC incidence and mortality in average-risk patients. However, studies on flexible sigmoidoscopy provide indirect evidence that colonoscopy reduces CRC mortality. A prospective cohort study also found an association between self-reports from patients who were screened with colonoscopy and a lower CRC mortality rate.(23) Moreover, data from computed tomography (CT) colonography studies has enabled the sensitivity of colonoscopy to be estimated so that the results can be applied to community practice.(24-27) Compared with CT colonography or colonoscopy with CT colonography (e.g. segmental unblinding), the sensitivity of colonoscopy is 89%–98% for detecting adenomas ≥ 10 mm and 75%–93% for adenomas ≥ 6 mm.(24,25,27)
The diagnostic accuracy and therapeutic safety of colonoscopy depends, in part, on the quality of the colonic cleansing or preparation. Hence, it is important that patients are educated and engaged in the colonoscopy preparation process. Patient counselling, along with written instructions that are simple, easy to follow and in the patient’s native language, should be provided.(28) Risks of colonoscopy include sedation-related adverse events, perforations (four in 10,000 procedures) and major bleeding (eight in 10,000 procedures).(7)
CT colonography
CT colonography, also known as virtual colonoscopy, is minimally invasive imaging of the entire colon and rectum. Its utility in screening for colorectal cancer has been studied. Based on seven studies of CT colonography with bowel preparation, the per-person sensitivity and specificity for detecting adenomas ≥ 10 mm were 67%–94% and 86%–98%, respectively. To detect adenomas ≥ 6 mm, the per-person sensitivity and specificity were 73%–98% and 80%–93%, respectively.(7) Incidental extracolonic findings are common, occurring in about 40%–70% of screening examinations. Between 5% and 37% of these findings result in diagnostic follow-up, and about 3% require definitive treatment, indicating potential overdiagnosis and overtreatment from CT colonography.(7) Radiation risk is a relative disadvantage of CT colonography; nonetheless, with new developments in technique, the risk of ionising radiation from CT colonography is extremely low and likely to be negligible.(29)
WHAT CAN I DO IN MY PRACTICE?
Despite advancements in screening modalities, treatment of pre-neoplastic adenomas and treatment options for CRC, the incidence of CRC in Singapore continues to rise rapidly. A major reason may be poor screening uptake, which is where primary care providers can play an important role. In addition to creating awareness by actively discussing CRC screening among suitable individuals, primary care providers can also address certain specific concerns and fears about screening modalities with their patients. In a local, nationwide, representative household survey, Wong et al(30) reported that both patient and physician factors were barriers to CRC screening. The study demonstrated the impact of the physician in advocating screening, with screening uptake showing a positive association with the physician’s recommendation. In particular, screening in women was positively associated with attending a public talk on CRC. However, only 22.6% of the patients in the study were advised by their physicians to undergo screening.(30) Addressing both patient and physician barriers to CRC screening is a crucial step in overcoming poor patient understanding of CRC as a fatal disease; the inability to identify symptoms of CRC; and a lack of awareness that screening is an important tool against cancer development.
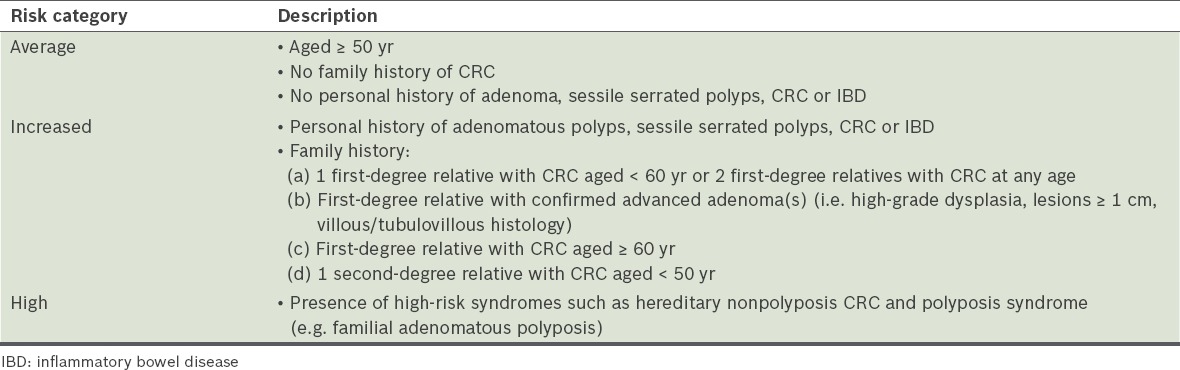
Like all screening programmes, CRC screening should be considered for all appropriate individuals at both acute and chronic consultations. The primary care physician can proactively screen at-risk individuals in the community for CRC by first assessing individual risk before making specific recommendations for CRC screening. History-taking is important and should emphasise risk factors for colorectal cancer, including age, smoking history, personal history of colorectal adenomas and inflammatory bowel disease (IBD), and family history (age of onset, number of affected family members and degree of consanguinity). Individuals can then be stratified according to their risk factors into average, increased and high risk groups (Table II).
Table II.
Risk categories for colorectal cancer (CRC).(31)
For average-risk individuals, the USPSTF guidelines emphasise shared decision-making, a process in which the physician and patient share information, then reach a shared medical decision about the screening test that is best for the patient. Table I shows the recommended screening intervals for CRC.
Individuals with increased risk of CRC should have personalised screening strategies. In particular, for those who have an affected first-degree relative diagnosed before 60 years of age or two first-degree relatives with CRC at any age, colonoscopy is recommended every five years, beginning ten years prior to the earliest diagnosis in the family or at 40 years of age at the latest.(31) Individuals who have a first-degree relative with a confirmed history of advanced adenoma(s) (i.e. high-grade dysplasia with lesions ≥ 1 cm and villous/tubulovillous histology) should undergo colonoscopy at the relative’s age of onset of adenoma, or by 50 years of age at the latest.(31) For those with one affected first-degree relative diagnosed at 60 years of age or older, or one second-degree relative diagnosed prior to 50 years of age, colonoscopy should begin at 50 years of age. High-risk individuals with a family history of familial adenomatous polyposis or hereditary nonpolyposis colorectal cancer, or those who have IBD must be referred and co-managed by a gastroenterologist, colorectal surgeon and/or cancer geneticist for regular and active surveillance of CRC.(32,33)
In Singapore, citizens and permanent residents aged ≥ 50 years are invited to screen for colorectal cancer annually using free FIT kits from Community Health Assist Scheme general practice clinics under the Integrated Screening Programme. In addition, the free FIT kit is available for collection at the Singapore Cancer Society and selected retail pharmacy outlets. However, more can be done to encourage screening uptake. Both patient and physician factors must be identified and addressed.
WHEN SHOULD I REFER TO A SPECIALIST?
Specialist referral is indicated if patients have a positive faecal occult blood test or prefer other screening modalities such as colonoscopy or CT colonography. In addition, primary care providers can refer individuals found to have increased or high risk of CRC to specialist care. In such cases, colonoscopy is the preferred screening or surveillance modality.
TAKE HOME MESSAGES
CRC is the leading cancer in Singapore.
CRC screening and polypectomy can prevent CRC.
Screening tests for CRC include stool-based tests (i.e. gFOBT, FIT and FIT-DNA) and direct visualisation tests (i.e. flexible sigmoidoscopy, alone or combined with FIT, colonoscopy and CT colonography).
Physicians should discuss appropriate screening modalities with patients.
Mr Tan eventually opted for an annual faecal immunochemical test for haemoglobin to screen for colorectal cancer (CRC). The result was positive and you referred him to a gastroenterologist. Six months later, he visited your clinic for a routine review. He mentioned that he underwent a colonoscopy five months ago. It revealed a small, 6-mm benign polyp (tubular adenoma with low-grade dysplasia) in his sigmoid colon, which was successfully removed during the colonoscopy. His gastroenterologist had since discharged him with a memo and Mr Tan was well. You advised him to undergo a surveillance colonoscopy in five years’ time if all goes well. He was glad to have heeded your recommendation to undergo CRC screening.
REFERENCES
- 1.National Registry of Diseases Office (NRDO), Health Promotion Board, Singapore. Singapore Cancer Registry Annual Registry Report Trends in Cancer Incidence in Singapore 2010 – 2014 [online] [Accessed December 13, 2016]. Available at: https://www.nrdo.gov.sg/docs/librariesprovider3/default-document-library/cancer-trends-report-2010---2014_web.pdf?sfvrsn=0 .
- 2.Sung JJ, Ng SC, Chan FK, et al. Asia Pacific Working Group. An updated Asia Pacific Consensus Recommendations on colorectal cancer screening. Gut. 2015;64:121–32. doi: 10.1136/gutjnl-2013-306503. [DOI] [PubMed] [Google Scholar]
- 3.Academy of Medicine Singapore. Report of the Screening Test Review Committee [online] 2011. [Accessed December 13 2016]. Available at: http://ams.edu.sg/view-pdf.aspx?file=media%5C626_fi_842.pdf&ofile=str2011.pdf .
- 4.Day DW, Morson BC. The adenoma-carcinoma sequence. Major Probl Pathol. 1978;10:58–71. [PubMed] [Google Scholar]
- 5.Hill MJ, Morson BC, Bussey HJ. Aetiology of adenoma-carcinoma sequence in large bowel. Lancet. 1978;1:245–7. doi: 10.1016/s0140-6736(78)90487-7. [DOI] [PubMed] [Google Scholar]
- 6.Winawer SJ, Fletcher RH, Miller L, et al. Colorectal cancer screening: clinical guidelines and rationale. Gastroenterology. 1997;112:594–642. doi: 10.1053/gast.1997.v112.agast970594. [DOI] [PubMed] [Google Scholar]
- 7.US Preventive Services Task Force. Bibbins-Domingo K, Grossman DC, Curry SJ, et al. Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. JAMA. 2016;315:2564–75. doi: 10.1001/jama.2016.5989. [DOI] [PubMed] [Google Scholar]
- 8.Shaukat A, Mongin SJ, Geisser MS, et al. Long-term mortality after screening for colorectal cancer. N Engl J Med. 2013;369:1106–14. doi: 10.1056/NEJMoa1300720. [DOI] [PubMed] [Google Scholar]
- 9.Scholefield JH, Moss SM, Mangham CM, Whynes DK, Hardcastle JD. Nottingham trial of faecal occult blood testing for colorectal cancer: a 20-year follow-up. Gut. 2012;61:1036–40. doi: 10.1136/gutjnl-2011-300774. [DOI] [PubMed] [Google Scholar]
- 10.Lindholm E, Brevinge H, Haglind E. Survival benefit in a randomized clinical trial of faecal occult blood screening for colorectal cancer. Br J Surg. 2008;95:1029–36. doi: 10.1002/bjs.6136. [DOI] [PubMed] [Google Scholar]
- 11.Kronborg O, Jørgensen OD, Fenger C, Rasmussen M. Randomized study of biennial screening with a faecal occult blood test: results after nine screening rounds. Scand J Gastroenterol. 2004;39:846–51. doi: 10.1080/00365520410003182. [DOI] [PubMed] [Google Scholar]
- 12.Faivre J, Dancourt V, Lejeune C, et al. Reduction in colorectal cancer mortality by fecal occult blood screening in a French controlled study. Gastroenterology. 2004;126:1674–80. doi: 10.1053/j.gastro.2004.02.018. [DOI] [PubMed] [Google Scholar]
- 13.Whitlock EP, Lin JS, Liles E, Beil TL, Fu R. Screening for colorectal cancer: a targeted, updated systematic review for the U.S. Preventive Services Task Force. Ann Intern Med. 2008;149:638–58. doi: 10.7326/0003-4819-149-9-200811040-00245. [DOI] [PubMed] [Google Scholar]
- 14.de Wijkerslooth TR, Stoop EM, Bossuyt PM, et al. Immunochemical fecal occult blood testing is equally sensitive for proximal and distal advanced neoplasia. Am J Gastroenterol. 2012;107:1570–8. doi: 10.1038/ajg.2012.249. [DOI] [PubMed] [Google Scholar]
- 15.Brenner H, Tao S. Superior diagnostic performance of faecal immunochemical tests for haemoglobin in a head-to-head comparison with guaiac based faecal occult blood test among 2235 participants of screening colonoscopy. Eur J Cancer. 2013;49:3049–54. doi: 10.1016/j.ejca.2013.04.023. [DOI] [PubMed] [Google Scholar]
- 16.Imperiale TF, Ransohoff DF, Itzkowitz SH, et al. Multitarget stool DNA testing for colorectal-cancer screening. N Engl J Med. 2014;370:1287–97. doi: 10.1056/NEJMoa1311194. [DOI] [PubMed] [Google Scholar]
- 17.Holme Ø, Løberg M, Kalager M, et al. Effect of flexible sigmoidoscopy screening on colorectal cancer incidence and mortality. JAMA. 2014;312:606–15. doi: 10.1001/jama.2014.8266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Schoen RE, Pinsky PF, Weissfeld JL, et al. PLCO Project Team. Colorectal-cancer incidence and mortality with screening flexible sigmoidoscopy. N Engl J Med. 2012;366:2345–57. doi: 10.1056/NEJMoa1114635. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Segnan N, Armaroli P, Bonelli L, et al. SCORE Working Group. Once-only sigmoidoscopy in colorectal cancer screening: follow-up findings of the Italian Randomized Controlled Trial--SCORE. J Natl Cancer Inst. 2011;103:1310–22. doi: 10.1093/jnci/djr284. [DOI] [PubMed] [Google Scholar]
- 20.Atkin WS, Edwards R, Kralj-Hans I, et al. UK Flexible Sigmoidoscopy Trial Investigators. Once-only flexible sigmoidoscopy screening in prevention of colorectal cancer: a multicentre randomised controlled trial. Lancet. 2010;375:1624–33. doi: 10.1016/S0140-6736(10)60551-X. [DOI] [PubMed] [Google Scholar]
- 21.Hoff G, Grotmol T, Skovlund E, Bretthauer M Norwegian Colorectal Cancer Prevention Study Group. Risk of colorectal cancer seven years after flexible sigmoidoscopy screening: randomised controlled trial. BMJ. 2009;338:b1846. doi: 10.1136/bmj.b1846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Dan YY, Chuah BY, Koh DC, Yeoh KG. Screening based on risk for colorectal cancer is the most cost-effective approach. Clin Gastroenterol Hepatol. 2012;10:266–71. doi: 10.1016/j.cgh.2011.11.011. e1-6. [DOI] [PubMed] [Google Scholar]
- 23.Nishihara R, Wu K, Lochhead P, et al. Long-term colorectal-cancer incidence and mortality after lower endoscopy. N Engl J Med. 2013;369:1095–105. doi: 10.1056/NEJMoa1301969. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Zalis ME, Blake MA, Cai W, et al. Diagnostic accuracy of laxative-free computed tomographic colonography for detection of adenomatous polyps in asymptomatic adults: a prospective evaluation. Ann Intern Med. 2012;156:692–702. doi: 10.7326/0003-4819-156-10-201205150-00005. [DOI] [PubMed] [Google Scholar]
- 25.Pickhardt PJ, Choi JR, Hwang I, et al. Computed tomographic virtual colonoscopy to screen for colorectal neoplasia in asymptomatic adults. N Engl J Med. 2003;349:2191–200. doi: 10.1056/NEJMoa031618. [DOI] [PubMed] [Google Scholar]
- 26.Johnson CD, Fletcher JG, MacCarty RL, et al. Effect of slice thickness and primary 2D versus 3D virtual dissection on colorectal lesion detection at CT colonography in 452 asymptomatic adults. AJR Am J Roentgenol. 2007;189:672–80. doi: 10.2214/AJR.07.2354. [DOI] [PubMed] [Google Scholar]
- 27.Johnson CD, Chen MH, Toledano AY, et al. Accuracy of CT colonography for detection of large adenomas and cancers. N Engl J Med. 2008;359:1207–17. doi: 10.1056/NEJMoa0800996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.ASGE Standards of Practice Committee. Saltzman JR, Cash BD, et al. Bowel preparation before colonoscopy. Gastrointest Endosc. 2015;81:781–94. doi: 10.1016/j.gie.2014.09.048. [DOI] [PubMed] [Google Scholar]
- 29.de Haan MC, Pickhardt PJ, Stoker J. CT colonography: accuracy, acceptance, safety and position in organised population screening. Gut. 2015;64:342–50. doi: 10.1136/gutjnl-2014-308696. [DOI] [PubMed] [Google Scholar]
- 30.Wong RK, Wong ML, Chan YH, et al. Gender differences in predictors of colorectal cancer screening uptake: a national cross sectional study based on the health belief model. BMC Public Health. 2013;13:677. doi: 10.1186/1471-2458-13-677. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines - Colorectal cancer screening [online] [Accessed December 13, 2016]. Available at: https://www.nccn.org/professionals/physician_gls/pdf/colorectal_screening.pdf .
- 32.Syngal S, Brand RE, Church JM, et al. American College of Gastroenterology. ACG clinical guideline: Genetic testing and management of hereditary gastrointestinal cancer syndromes. Am J Gastroenterol. 2015;110:223–62. doi: 10.1038/ajg.2014.435. quiz 263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.American Society for Gastrointestinal Endoscopy Standards of Practice Committee. Shergill AK, Lightdale JR, et al. The role of endoscopy in inflammatory bowel disease. Gastrointest Endosc. 2015;81:1101–21. doi: 10.1016/j.gie.2014.10.030. e1-13. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.