

Abstract
Background
Work-related musculoskeletal disorders (WMSD) among construction workers remain high. Participatory ergonomics (PE) interventions that engage workers and employers in reducing work injury risks have shown mixed results.
Methods
Eight-six workers from seven contractors participated in a PE program. A logic model guided the process evaluation and summative evaluation of short term and intermediate impacts and long term outcomes from surveys and field records.
Results
Process measures showed good delivery of training, high worker engagement, and low contractor participation. Workers’ knowledge improved and workers reported changes to work practices and tools used; contractor provision of appropriate equipment was low (33%). No changes were seen in symptoms or reported physical effort.
Conclusions
The PE program produced many worker-identified ergonomic solutions, but lacked needed support from contractors. Future interventions should engage higher levels of the construction organizational system to improve contractor involvement for reducing WMSD.
Keywords: injury prevention, musculoskeletal disorder, process evaluation, work, training program
INTRODUCTION
Construction workers are at high risk of work-related musculoskeletal disorders (WMSD) and lose 39% more time from work than workers in all private industries (CPWR - The Center for Construction Research and Training, 2013). WMSD may be caused by high risk work tasks, but the complex nature of construction work often makes it challenging to address these risks (Silverstein and Evanoff, 2011). Physically demanding activities such as carrying loads, working in awkward, bent-over or twisted postures for long periods of time, and handling vibrating tools create such risks, yet the dynamic nature of activities over the lifecycle of construction projects requires innovative interventions to eliminate the high risk physical exposures (Hecker, et al., 2001, Ringen and Englund, 2006, Ringen, et al., 1995). A participatory intervention that engages the skilled workers who perform the work and the employers who execute the project timeline may be able to increase capacity for creating safer work practices of the high risk tasks (Haines, et al., 2002, Koningsveld, et al., 2005, Vink, et al., 2006, Wells, et al., 2009, Wilson, 1997).
Participatory ergonomics (PE) is an intervention that is designed to engage both workers and managers to effect meaningful changes in work risks by pooling the workers’ knowledge and the employer’s resources (Bohr, et al., 1997, Brown, 2005, Haukka, et al., 2008, Hignett, et al., 2005, Israel, et al., 1989, Wilson, 1997). There are few PE interventions in construction, (Moir and Buchholz, 1996) many of which have been promoted by construction owners who were concerned with work productivity related to the work tasks (van der Molen, et al., 2005a). These management-driven programs solicited varying levels of worker input and even though the program identified good solutions, results showed limited worker adoption and transfer of recommended methods to future builds (de Jong and Vink, 2000, de Jong and Vink, 2002, de Looze, et al., 2001, Hess, et al., 2004, van der Molen, et al., 2005b, Vink, et al., 1997). On these temporary construction worksites with little supervision by employers, workers are empowered to structure their own work tasks as long as they work within the rules and expectations of the project. Inadequate engagement of workers in the development and implementation of interventions is a common limitation reported in PE interventions in construction.
Participatory ergonomic studies across all industries have shown mixed results (Driessen, et al., 2011, Haukka, et al., 2008). These studies are often limited by inadequate delivery of the program due to lack of time, lack of management commitment, and work pressures (Cantley, et al., 2014, Carrivick, et al., 2005, Cole, et al., 2009, Driessen, et al., 2010, Haukka, et al., 2008, Oude Hengel, et al., 2013). Despite these recognized challenges, a PE approach continues to be a preferred intervention to reduce or prevent WMSDs in complex environments (Glina, et al., 2011, Punnett, et al., 2013). Recent reviews suggest that future studies should provide greater detail about program delivery and intermediate outcomes to identify facilitators and barriers of the program (Rivilis, et al., 2008, Robson, et al., 2001, Salem, et al., 2008, van Eerd, et al., 2010).
We used a logic model to guide the evaluation of a construction-based PE program with the following two aims: 1) determine the extent to which the program was implemented as intended; and 2) determine the impact of a participatory ergonomics training intervention on construction worker learning, actions, health, and injury risk. We hypothesized that a well-delivered PE program would result in improvements in short term impacts measured by ergonomic skills, awareness, knowledge, and attitudes of the participating workers; intermediate impacts measured by an increase in ergonomic changes to work practices, tools or equipment during work activities; and long term outcomes measured by a decrease in WMSD symptoms, missed work days and risk level in task.
MATERIALS AND METHODS
Subjects
Seven small-sized contractors from three different construction trades provided the research team access to groups of their workers. Each work group consisted of apprentices, journeymen, and foremen. Our study protocol was reviewed and approved by the Institutional Review Boards of Washington University School of Medicine and Saint Louis University. All subjects provided informed consent to participate in this study.
Program description
Contractor representative recruitment/participation
We met with local union and management leaders primarily through the local apprenticeship programs to locate contractors who had available work and that may be willing to participate in the project. We received recommendations for 11 floor layer contractors (4 did not meet study criteria and 4 were too busy or did not respond to calls), 9 sheet metal contractors (5 did not meet study criteria and 1 did not respond), and 4 carpenter contractors (2 did not meet criteria and one did not respond). We recruited 7 subcontractors (3 floor layer contractors, 3 sheet metal contractors, 1 carpenter contractor). During initial recruitment meetings with contractors, researchers described the goals of the program and the contractor specific activities needed to conduct the participatory intervention. Each contractor signed a partnership form indicating their support for the program and ability to meet predefined research expectations. These expectations were to provide a stable work crew of at least three workers, have available work for the crew for a duration of at least three months, allow the workers to participate in training and data collection of surveys and focus groups and a contractor representative who would participate in the worksite program and support the development and implementation of ergonomic solutions. Ideally, the contractor representative was actively involved in developing and delivering training sessions and facilitating discussions within the work group. The contractor representative for the research program was either the company safety manager or construction project foreman/supervisor.
Participatory Ergonomic Training Program
Each work group received training in ergonomics as part of the program. A series of training objectives were delivered using an interactive format and active participation by a contractor representative, workers, and researcher team members (see Appendix I for the Training Objectives). During the training, each work group was encouraged to identify high risk work tasks and propose solutions using the available tools/equipment, knowledge or experiences from co-workers, or previously proposed solutions provided by the researchers obtained from past literature and other sources (Albers and Estill, 2007, Cal/OHSA, 2003, Canadian Centre for Occupational Health and Safety (CCOHS), 2011, Dababneh, et al., 2004, National Institute for Occupational Safety and Health (NIOSH), 2004, Occupational Safety & Health Administration (OSHA), 2003, Washington State Department of Labor and Industries, 2000). After delivering the training to the initial work groups of floor layers, the training format for the program was revised from two 30-minute formal classroom sessions to six 10-minute interactive tool box talks so the training more naturally fit within the construction work schedule (CPWR - The Center for Construction Research and Training, 2015), although the same objectives were covered in both training methods. In addition to training, the researchers were available at the worksite one or more times per week throughout the program period to interact with the workers and contractor representatives, assist with recognition of problem tasks, identify available solutions, acquire trial equipment for workers’ use, and record interactions in field notes. The frequency and duration of interactions between the research team and work group depended on the nature of the construction project and availability of the worker, foreman, and contractor representative on each worksite.
Logic Model for Process and Summative Evaluation
We have previously described the logic model (Figure I) used to guide the implementation and evaluation of our PE program (Jaegers, et al., 2014). Process evaluation measures were documented during delivery of the program to show the 1) fidelity of contractor recruitment and subsequent participation, 2) fidelity of worker training, 3) reach to intended workers, 4) frequency of training sessions, 5) duration of the program, and 6) engagement or participation by workers and contractor representatives as indicated on the left side of Figure 1 (Glanz and Bishop, 2010, Hasson, 2010, Linnan and Steckler, 2002). Summative evaluation, shown on the right side of Figure 1, included measures of short term impacts of the program on worker skills, awareness, knowledge, and attitudes, intermediate impact on worker behavior changes, and long term outcomes of reduced symptoms and reduced effort in work tasks.
Figure I.
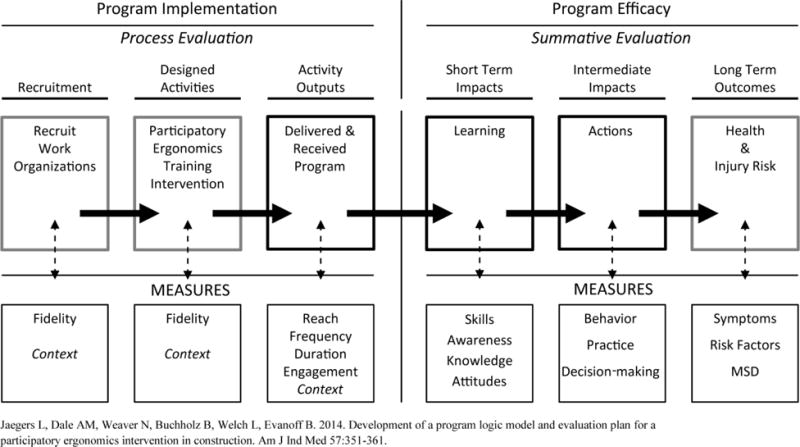
Logic Model Utilized to Guide a Participatory Ergonomics Training Program Implementation and Evaluation
Quantitative and qualitative data collection
Quantitative data was gathered through attendance records, work logs, and surveys. Surveys were collected prior to the start of the training program, several times during the program, and at the end of the intervention when the researchers stopped collecting data at the construction project. Survey items covered process measures to record reach and worker engagement, worker knowledge and attitudes toward the use of ergonomics for short term impacts, worker and work group behaviors related to ergonomics for intermediate impacts, and symptoms, missed work days, and worker perceived effort in tasks for long term outcomes (see Appendix II for survey items and sources). Workers rated their level of agreement with each item on a 6-point response scale ranged from strongly disagree to strongly agree. The survey also captured worker demographics and work history including age, gender, handedness, race, job classification, years worked in the trade, time worked for current contractor, weekly hours worked, and the worker perceived safety climate of the contractor group (Hahn and Murphy, 2008).
Qualitative data was obtained from open-ended questions on the survey, worker focus groups, contractor interviews, and researcher field notes. These data were used in the process evaluation to determine the contractor representatives’ engagement and to evaluate worker behavior changes for intermediate program impacts.
Data Analysis
Process Evaluation
We examined the demographics, contractor group safety climate scores, and participation of the contractors and all recruited workers in the program based on survey responses and training attendance, in order to determine the fidelity of training, reach, frequency, duration, and worker engagement. We described the contractor representative’s participation in the program by a qualitative review of all data and independent ratings with a consensus process by the two onsite researchers in the project (AMD, LJ). Contractor representatives were coded as fully engaged, partially engaged, or not engaged in the program.
Summative Evaluation
We analyzed the survey responses for each outcome (short-term, intermediate, and long-term). We dichotomized the response scale to compare the proportion of workers that agreed with each item (score 5–6) with those that slightly agreed or disagreed (score 1–4). We summarized self-reported worker behavior changes quantitatively by determining the proportion of subjects that reported making a behavior change due to the program and used mixed logistic regression models to test the odds of worker agreement of dichotomized response scales at follow-up compared to baseline, with workers nested within contractor work groups. We also evaluated worker behavior change qualitatively by consensus coding of open-ended survey items, interviews, and field notes. Two researchers (AMD, LJ) determined the number of problems that had been identified during the study by the workers or researchers for each work task in the qualitative data, then reviewed the history of each problem to determine whether there was a solution identified for each problem, the type of solution (equipment, tool, or work practice), whether the solution was the contractor’s responsibility and/or worker’s responsibility, and barriers to implementation of solutions. We determined the timing of implementation of each solution, whether the solution was available before the ergonomic program, during the program, or planned for implementation after the end of the project. Finally, we compared the presence of symptoms, reported missed days due to symptoms, as well as improvements in perceived effort required for tasks following the program to baseline reports.
RESULTS
Demographics
The seven participating contractors employed between 20 and 40 workers annually on average. Three contractors employed safety directors. There were 97 workers among the seven work groups; two were ineligible (1 by age, 1 planned retirement in one month). We enrolled 95 workers into the study: 25 workers from three floor laying contractors, 42 workers from three sheet metal contractors, and 28 workers from one carpenter drywall contractor. Nine (9.5%) of the 95 workers did not attend any training. Trained workers (n=86) had a mean age of 40 years (range 19 to 60 years), were white (98.8%), experienced in the trade for an average of 16.8 years (range 2 months to 39 years), and employed by their current contractor for an average of 7.7 years (range from 1 week to 36 years).
Table I presents the baseline characteristics of each separate work group. The size of the participatory work groups ranged from 2 to 24 workers and most workers were journeyman. The safety climate scores showed all work groups were in the “fair” range (16.9–18.9 summated scores).
Table I.
Contractor and participatory work group characteristics
| Participatory Work Groups
|
|||||||
|---|---|---|---|---|---|---|---|
| Characteristics | F01 | F02 | F03 | S01 | S02 | S03 | C01 |
| Average annual Contractor size (n)* | 35 | 20 | 25 | 40 | 35 | 30 | 25 |
| Trained subjects (n) | 16 | 2 | 5 | 16 | 7 | 16 | 24 |
| Journeyman | 7 | 2 | 5 | 14 | 4 | 14 | 20 |
| Apprentices | 4 | 0 | 1 | 1 | 2 | 2 | 0 |
| missing | 5 | 0 | 0 | 1 | 1 | 0 | 4 |
| Onsite PE program participants** | W,F,R | W,R | W,F,R | W,F,SD,R | W,F,R | W,F,SD,R | W,F,SD,R |
| Duration of program (in weeks) | 15 | 13 | 17 | 13 | 15 | 9 | 8 |
|
| |||||||
| mean (sd) | mean (sd) | mean (sd) | mean (sd) | mean (sd) | mean (sd) | mean (sd) | |
| Years employed with contractor | 3.2 (2.7) | 10 (0) | 4.9 (4.9) | 7.4 (4.2) | 6.4 (7.5) | 14.4 (12.6) | 7.0 (10.0) |
| Years in trade | 8.2 (7.3) | 10 (0) | 12.8 (11.6) | 17.5 (9.5) | 12.3 (10.7) | 23.5 (12.0) | 20.2 (9.0) |
| Age, in years | 30.6 (8.4) | 32.5 (3.5) | 37.2 (10.5) | 41.5 (9.5) | 37.6 (12.3) | 46.9 (10.9) | 42.4 (8.1) |
| Average annual hours | 1132 (360) | 990 (0) | 720 (701) | 1514 (272) | 1403 (943) | 1634 (317) | 1323 (825) |
F: floor layer, S: sheet metal, C: carpenter
Total average # employed by contractor
W: worker, F: foreman, SD: safety director, R: researcher
Process evaluation
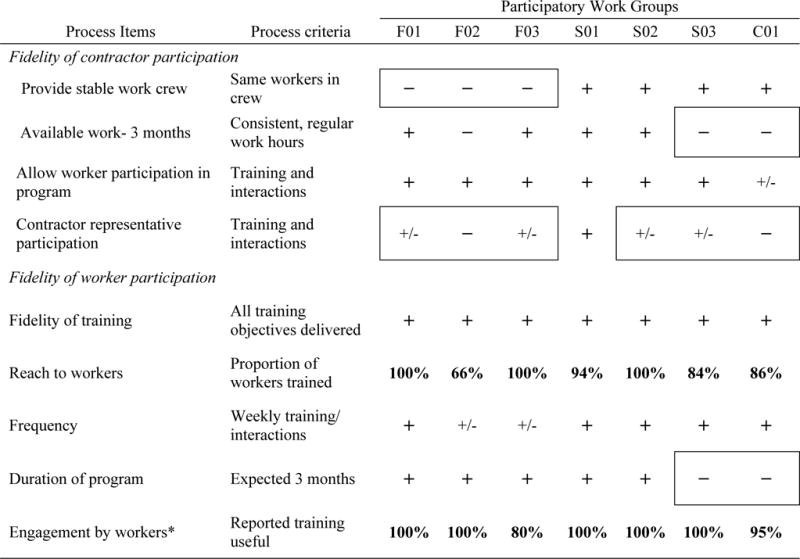
The process evaluation, used to assess the fidelity of the program, showed the contactors were unable to meet several of the research expectations of the program as presented in Table 2. All of the floor laying contractors had difficulty providing stable work crews and one contractor from each trade showed limited available work of at least three months. The carpenter group’s project was put on an accelerated time line for early job completion so the research team was asked to stop the program since workers had no time for participation. The participation of the contractor representative was very limited with only one group showing good participation.
Table II.
Process Evaluation Results by Participatory Work Group
|
Scale: fully met expectation (+), partially met expectation (+/−), or did not meet expectation (−); F: floor layer, S: sheet metal, C: carpenter
missing responses: F03-1, C01-2 (total n=83).
The worker-related process measures showed relatively good fidelity of the program. All training objectives were delivered, the training reached most workers, the frequency of the training and the interactions were fairly consistent, although the duration of the program was shorter than expected for two groups. The engagement of the workers determined by worker assessment of the usefulness of training was excellent for most groups.
Summative evaluation
Short Term Impacts
Table IIIa shows the short term impacts of the program. At baseline, most workers reported a high level of skill and awareness in recognizing problematic tasks and willingness to try new tools or change work tasks. Workers reported lower baseline levels of knowledge in how to use ergonomics in their jobs and plans for trying new tools and making changes, but these items showed the greatest improvement in worker agreement after training, (OR 2.1; 95% CI 1.1–4.0) and (OR 2.1; 95% CI 1.1–4.0), respectively. In mixed models, we examined whether the categorized safety climate score by contractor group was an effect modifier in each model and found no effect.
Table IIIa.
Proportion of Worker Agreement* with Short Term and Intermediate Impact items baseline and follow-up (n=83)
| IIIa. Short Term Impact | |||
|---|---|---|---|
|
| |||
| Construct | Survey Item | Baseline % |
Follow-up % |
| Skills | I am able to point out why some work tasks are physically demanding. | 82.3 | 83.5 |
| There are actions that I can take to reduce my risk of pain and discomfort in my job. | 58.2 | 68.4 | |
| Awareness | There is risk of muscle or joint pain/discomfort in my job. | 87.3 | 96.2 |
| Knowledge | I have had enough training to know how to use ergonomics in my job. | 46.8 | 64.6* |
| I am willing to try new tools or change how I perform work tasks to reduce my risk of pain and discomfort in my job. | 82.1 | 87.3 | |
| Attitudes | I feel like I have the freedom to try new tools or change how I perform work tasks. | 68.4 | 65.8 |
| I am planning to try new tools or change how I perform work tasks to reduce my risk of pain and discomfort in my job. | 46.8 | 63.3* | |
For each item, dichotomized response scale for agreement (agree or strongly agree) to disagree/neutral response (strongly disagree, disagree, slightly disagree, slightly agree)
significant results of mixed logistic regression models for worker within contractor groups on agreement of dichotomized response scales at follow-up compared to baseline for individual items (p<0.05).
Intermediate Impacts
Table IIIb shows the proportion of workers who reported agreement with safer behavior, practice, and decision-making actions at baseline (before program) and follow-up (after program). At baseline, most workers felt they could find ways to make their job physically easier and that they were involved in making decisions about their health and safety. The lowest proportion of workers reported good practice for talking about ergonomics, tools, or techniques in their work group, with their foreman, and with their employer. At baseline, only 58% of workers reported taking action to change work tasks to make their job physically easier to do. At follow-up, there was little change in response for most behaviors and practices with the exception of improvement in talking within the work group about ergonomics. There were no significant changes of worker agreement with any survey items using mixed logistic regression analysis.
Table IIIb.
Intermediate Impact
| Constructs | Survey Item | Baseline | Follow-up | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Behavior | I find ways to make my job physically easier to do. | 83 | 83.5 | 83 | 82.3 |
| I am taking or have taken action to reduce my risk of pain or discomfort at my job. | 82 | 73.4 | 83 | 74.7 | |
| I change my work tasks to make my job physically easier to do. | 83 | 58.2 | 82 | 66.7 | |
| I assisted others to make sure they performed their work safely. | 79 | 69.6 | 79 | 68.4 | |
| Our work group has identified good solutions to work problems/hazards. | 81 | 62.3 | 83 | 58.2 | |
| Practice | Our work group talks about ergonomics solutions at least once a week. | 83 | 31.6 | 83 | 35.2 |
| Our work group has tried new solutions. | 83 | 48.1 | 83 | 49.4 | |
| My foreman talks about tools or techniques to make work tasks easier. | 83 | 54.4 | 83 | 50.6 | |
| My employer talks about tools or techniques to make work tasks easier. | 83 | 35.4 | 83 | 35.4 | |
| Decision making | I was regularly involved in decisions affecting my health and safety. | 79 | 81.0 | 79 | 72.5 |
Individual worker-reported changes in work behaviors on surveys were common with 76 of the 86 trained workers reported making at least one change. Ten workers (13%) reported making a tool change, 16 (21%) made a work method change, and 41 (54%) reported a change in both a tool and work method. Few workers trialed or purchased a new tool (12%). Nine (12%) workers reported making no change in their work activities.
Researcher review of qualitative data from field notes and surveys reported the problems in work tasks that were identified by workers, researchers and worker-researcher interactions, and implementation of solutions for each problem during the project. There were 105 problems described in tasks across all seven work groups. Solutions were developed for 90% of the problems with the details shown in Figure II. Nearly half (45%) of the solutions required the availability of equipment and power tools which were the contractor’s responsibility to provide (n=43). For more than half of these solutions (n=25, 58%), the contractor provided equipment at the worksite before the start of the PE program; however, the equipment was often deemed not useful (n=13) due to being inappropriate for the design of the build (narrow halls, confined space, muddy environment), being poorly maintained/broken, or having inadequate number of resources for all workers. Only three contractor equipment changes were made during the program and four were planned to be made for use on the next project; ten problematic tasks (23%) had no equipment provided by the contractor during the program. Only 33% of the solutions within the contractor responsibility were addressed appropriately either before or during the project period. Workers were responsible for providing their own manual tools and appropriately addressed 75% of the solutions involving manual tools (33/44 problems). Seventeen of the tools were available before the program and another 16 tools were purchased or trialed as a result of information learned during the program. Eight problems had solutions that required no new equipment or tools, but required a change in work practice.
Figure II.
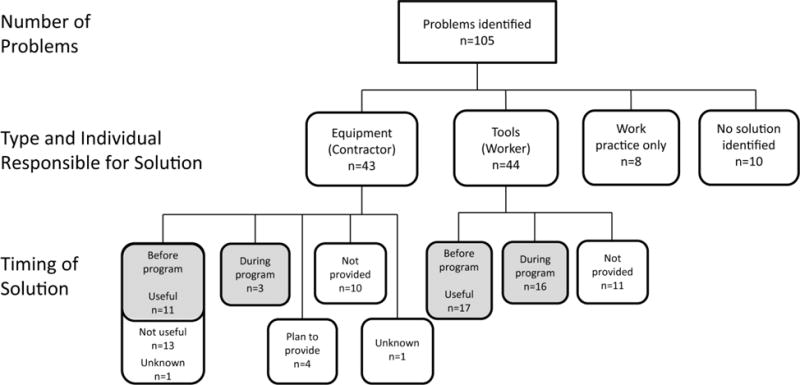
Flowchart of Problems and Solutions Developed and Timing of Implementation across all Participatory Work Groups
Despite the availability of equipment, tools, or new work practices, successful worker adoption of solutions was limited. Based on field notes, workers consistently used beneficial equipment, tools, and work methods for only 14% of the recommended solutions (n=95). The reasons for lack of consistency in work practice included having an insufficient number or no tools or equipment available, poor location and access to equipment, difficulty coordinating with other team members, multistep work processes, or inaccessible work areas to use equipment due to the design of the building.
Long Term Outcomes
There were no improvements in long term outcomes during the program. Self-perceived effort needed to perform work activities was high at baseline (mean range of effort scores: 4.18 to 5.23) and did not improve during the period of the program. There was no significant change in the proportion of workers reporting pain or discomfort in the prior 4 weeks (n=78, baseline 85.9%, follow-up 88.5%).
DISCUSSION
The PE program delivered to work groups in three construction trades showed minimal improvement in short-term and intermediate impacts and no improvement in long term health outcomes. The logic model provided a structured way to show the progression of steps from the implementation of the program (process evaluation) to the program efficacy (summative evaluation), and to evaluate which steps in the intervention process were or were not successful. According to the process evaluation, the fidelity of the delivery of the program was not achieved. Even though all participants received the training information, there were several barriers to delivery of the program which differed across work groups. Lack of crew stability, shortened program duration, and a general lack of contractor support reduced the intended benefit of participation by the workers. The summative evaluation showed that most workers reported increased knowledge and skill (short term impacts), some workers reported making ergonomic changes (intermediate impacts), and only two workers showed a change in long term outcomes. Many workers made a change in tool use, purchased equipment and demonstrated willingness to use equipment provided by the contractors, but contractors showed much less support in providing beneficial equipment that was appropriate for use by the workers on the project. There were other barriers to implementation of solutions beyond the control of the work group and contractor including the project timeline, design of the build, environmental conditions, and interactions with other trades. The efficacy of the PE program as delivered within the subcontractor work groups was limited by many barriers; only a portion of these barriers could have been addressable within the immediate subcontractor work group.
Management commitment and worker participation are considered the most important elements for a successful PE program (Brown, 2005). Our results showed strong interest and creative ideas from the workers, but lacked cooperation and engagement from the contractors, even though we used informational interviews to assure contractor interest and commitment prior to the project. Equipment provided by contractors at the beginning of the project was often not appropriate for use by workers; contractors were unable to make the necessary changes providing more beneficial equipment within the project, but planned to provide the equipment on the next project. This result is opposite to the effect observed in other construction PE programs that used a management driven process to discover and implement solutions for specific high risk work task and had difficulty gaining worker buy-in to adopt solutions (van der Molen, et al., 2005b). The current program, performed in small contracting firms, was more worker-driven (75% of worker problems were addressed) and showed less buy-in from management (33% of contractor problems were addressed). Regardless of the focus of the intervention (task-specific or general training to apply across current tasks), this study shows that it is necessary to gain buy-in from both management and workers to participate in the program.
There were several production demands that limited the delivery of the program. In some work groups, the contractor representative was unwilling to allow workers to receive sessions of training as intended, stating pressure from the production schedule could not accommodate the time. Consequently, the training was condensed and delivered during previously scheduled toolbox talks. PE programs conducted in more stable work environments such as manufacturing have encountered similar barriers of time and commitment by management (Cole, et al., 2009, St-Vincent, et al., 2006). Haukka and colleagues delivered a randomized control trial of a PE program to 18 kitchen work groups (Haukka, et al., 2008). The results showed no change in musculoskeletal health with management support cited as one of the most important facilitators. St. Vincent and colleagues delivered PE programs to 11 companies including slaughterhouses and manufacturers and showed various barriers, primarily related to time for the program (St-Vincent, et al., 2006). Greater detail provided by the process evaluation allowed insight into the barriers for delivery of the program and similarities of PE process between construction and other industries (Driessen, et al., 2011, St-Vincent, et al., 2006). Given the dynamic nature of construction, PE programs in construction likely face additional challenges not encountered in other industries.
In past studies, the PE program often was viewed as a stand alone program, created to solve a specific problem, but it did not fit within the companies’ management system (Yazdani, et al., 2015). In the current study, many barriers to the PE program were outside of the contractor and worker control such as the design of the structure and project schedule. These system level issues have been recognized in other studies as caused by the architectural design that dictates the type, size, and weight of materials without regard to the methods for installation (Kim, et al., 2011, Smallwood, 2012), and limited working space for the workers (Wiberg, 2012). Other system barriers may be in the control of the construction management or general contractor (Fulmer, et al., 2006). Since the general contractor may be the part of the organizational structure with the greatest influence on safety and the planning process of the build, this group should be fully integrated into future intervention efforts. PE programs which partner with single contracting companies may not be successful without also engaging additional levels of the temporary organizational system of the project.
Our study had limitations that may have affected our findings. Our overall sample size was small, and some work groups had a very small number of workers. We were unable to compare results between groups although there were notable differences in the organizational structure and method of delivery of the program across the work groups. We studied small contractors, who had few in-house resources for safety and health intervention, and were subject to significant economic pressures during the time of our study. The researchers were present on each worksite for a short time each week, so some information related to delivery of the program may have been missed. Even with the limited follow-up at the worksite, the recorded observations showed inconsistent work practices and use of equipment and tools for most proposed solutions. Finally, it is likely that the short period of time to deliver the program and support development of interventions was inadequate for work groups to fully incorporate the information gained from the training program and change work practices (Carlan, et al., 2012, CPWR - The Center for Construction Research and Training, 2012). Using an intervention group-only design, we were not able to test for factors outside of the context of the program, but it is unlikely that workers were receiving ergonomics content from other sources concurrent with the intervention.
The strengths of the study included the similar training and intervention program delivered to seven different small construction companies and observation of workers at the worksite for at least 3 months during the intervention program. In addition, data was gathered from the contractor and the workers to learn how each stakeholder viewed delivery and effectiveness of the program as well as the barriers to implementing solutions at the worksite.
Conclusions
The temporary organizations created in construction projects strongly rely on skilled workers and positive, effective working relationships between trades and between management and workers for successful completion of the builds. The unique ergonomic hazards created by the design of the build and other external factors requires engagement of managers and workers to deliver relevant and timely solutions. Although workers are willing participants in a PE program, many subcontractors do not have the organizational structure and resources to engage in the program, which causes tension between competing interests of production versus health and safety. Strong, organized, and attentive leadership from the general contractor may facilitate the process of participatory ergonomics and structure the work to allow workers’ voices and suggestions to be incorporated into the planning of the work.
Supplementary Material
Acknowledgments
We would like to thank the Carpenters’ District Council of Greater St. Louis, Sheet Metal Workers’ Local 36 and the contractors, carpenters, and sheet metal workers, who participated in this study.
Disclosure of Grant Funding This research was funded as part of a grant to CPWR— the Center for Construction Research and Training from the National Institute for Occupational Safety and Health/Centers for Disease Control (Grant No. NIOSH U60 OH009762) and by the Washington University Institute of Clinical and Translational Sciences Grant UL1 TR000448 from the National Center for Advancing Translational Sciences (NCATS) of the National Institutes of Health (NIH). Its contents are solely the responsibility of the authors; the study sponsors had no specific involvement in this manuscript; and the findings do not necessarily represent the official views of CDC, NIOSH, NCATS or NIH.
Footnotes
This work was performed at the Washington University School of Medicine, St. Louis, MO.
Conflict of Interest Statement: The authors declare that they have no conflicts of interest relevant to the publication of this manuscript; Drs. Dale, Jaegers, Welch, Gardner, Buccholz, and Evanoff report a grant from CDC/NIOSH during the conduct of the study.
CONTRIBUTORS
All coauthors participated in this study. Drs. Dale, Jaegers, Welch, Buccholz, and Evanoff planned and conducted the research; Drs. Weaver and Gardner advised the study team during preparation of the manuscript and all authors were involved in interpretation of the data analysis. Drs. Dale, Jaegers, and Gardner were the primary writers, with all other authors contributing to and editing portions of the manuscript. All authors reviewed the final manuscript. All authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Ethics Review and Approval The Washington University School of Medicine Institutional Review Board provided the ethical approval of this study. All participants provided written informed consent and were compensated for their participation.
References
- Albers JT, Estill CF. Simple Solutions: Ergonomics for Construction Workers Cincinatti. OH: DHHS (NIOSH); 2007. (Publication No. 2007–122). [Google Scholar]
- Bohr PC, Evanoff BA, Wolf LD. Implementing participatory ergonomics teams among health care workers. Am J Ind Med. 1997;32:190–196. doi: 10.1002/(sici)1097-0274(199709)32:3<190::aid-ajim2>3.0.co;2-1. [DOI] [PubMed] [Google Scholar]
- Brown OJ. Participatory Ergonomics. In: Stanton N, Hedge A, Brookhuis K, Salas E, Hendrick H, editors. Handbook of Human Factors and Ergonomics Methods. CRC Press LLC; 2005. p. 7. [Google Scholar]
- Cal/OHSA. Ergonomic Survival Guide for Sheet Metal Workers. 2003 http://www.dir.ca.gov/dosh/dosh_publications/CErg_SheetMetal.pdf. Accessed September 15, 2015.
- Canadian Centre for Occupational Health and Safety (CCOHS) Hand Tool Ergonomics: Health Hazards. 2011 http://www.ccohs.ca/oshanswers/ergonomics/handtools/hazards.html.
- Cantley LF, Taiwo OA, Galusha D, Barbour R, Slade MD, Tessier-Sherman B, Cullen MR. Effect of systematic ergonomic hazard identification and control implementation on musculoskeletal disorder and injury risk. Scand J Work Environ Health. 2014;40:57–65. doi: 10.5271/sjweh.3394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carlan NA, Kramer DM, Bigelow P, Wells R, Garritano E, Vi P. Digging into construction: Social networks and their potential impact on knowledge transfer. Work. 2012;42:223–232. doi: 10.3233/WOR-2012-1345. [DOI] [PubMed] [Google Scholar]
- Carrivick PJW, Lee AH, Yau KKW, Stevenson MR. Evaluating the effectiveness of a participatory ergonomics approach in reducing the risk and severity of injuries from manual handling. Ergonomics. 2005;48:907–914. doi: 10.1080/0014013042000327698. [DOI] [PubMed] [Google Scholar]
- Cole DC, Theberge N, Dixon SM, Rivilis I, Neumann WP, Wells R. Reflecting on a program of participatory ergonomics interventions: a multiple case study. Work. 2009;34:161–178. doi: 10.3233/WOR-2009-0914. [DOI] [PubMed] [Google Scholar]
- CPWR - The Center for Construction Research and Training. Best Practices for Health and Safety Technology Transfer in Construction: Symposium Report 2012 [Google Scholar]
- CPWR - The Center for Construction Research and Training. The Construction Chart Book: The US Construction Industry and Its Workers. 5th. Silver Spring, MD: CPWR - The Center for Construction Research and Training; 2013. [Google Scholar]
- CPWR - The Center for Construction Research and Training. Ergonomic Tool Box Talks (TBT) Training Guide. elcosh - Electronic Library of Construction Occupational Safety and Health. 2015 http://www.elcosh.org/document/3835/d001304/Ergonomics%2BTool%2BBox%2BTalks%2B%2528TBT%2529%2BTraining%2BGuide.html. Accessed September 15, 2015.
- Dababneh A, Lowe B, Krieg E, Kong YK, Waters T. Ergonomics. A checklist for the ergonomic evaluation of nonpowered hand tools. J Occup Environ Hyg. 2004;1:D135–145. doi: 10.1080/15459620490883150. [DOI] [PubMed] [Google Scholar]
- de Jong AM, Vink P. The adoption of technological innovations for glaziers; evaluation of a participatory ergonomics approach. Int J Ind Ergon. 2000;26:39–46. [Google Scholar]
- de Jong AM, Vink P. Participatory ergonomics applied in installation work. Appl Ergon. 2002;33:439–448. doi: 10.1016/s0003-6870(02)00033-9. [DOI] [PubMed] [Google Scholar]
- de Looze MP, Urlings IJM, Vink P, van Rhijn JW, Miedema MC, Bronkhorst RE, van der Grinten MP. Towards successful physical stress reducing products: an evaluation of seven cases. Appl Ergon. 2001;32:525–534. doi: 10.1016/s0003-6870(01)00018-7. [DOI] [PubMed] [Google Scholar]
- Driessen MT, Proper KI, Anema JR, Knol DL, Bongers PM, van der Beek AJ. The effectiveness of participatory ergonomics to prevent low-back and neck pain–results of a cluster randomized controlled trial. Scand J Work Environ Health. 2011;37:383–393. doi: 10.5271/sjweh.3163. [DOI] [PubMed] [Google Scholar]
- Driessen MT, Proper KI, van Tulder MW, Anema JR, Bongers PM, van der Beek AJ. The effectiveness of physical and organisational ergonomic interventions on low back pain and neck pain: a systematic review. Occup Environ Med. 2010;67:277–285. doi: 10.1136/oem.2009.047548. [DOI] [PubMed] [Google Scholar]
- Fulmer S, Azaroff LS, Moir S. Factors influencing ergonomic intervention in construction: Trunkman case study*. New Solutions. 2006;16:235–247. doi: 10.2190/1842-7382-9773-T673. [DOI] [PubMed] [Google Scholar]
- Glanz K, Bishop DB. The Role of Behavioral Science Theory in Development and Implementation of Public Health Interventions. Annu Rev Public Health. 2010;31:399–418. doi: 10.1146/annurev.publhealth.012809.103604. [DOI] [PubMed] [Google Scholar]
- Glina DMR, Cardoso AS, Isosak M, Rocha LE. Participatory ergonomics: Understanding the contributions of reflection groups in a hospital food service. Int J Ind Ergon. 2011;41:96–105. [Google Scholar]
- Hahn SE, Murphy LR. A short scale for measuring safety climate. Safety Science. 2008;46:1047–1066. [Google Scholar]
- Haines H, Wilson JR, Vink P, Koningsveld E. Validating a framework for participatory ergonomics (the PEF) Ergonomics. 2002;45:309–327. doi: 10.1080/00140130210123516. [DOI] [PubMed] [Google Scholar]
- Hasson H. Systematic evaluation of implementation fidelity of complex interventions in health and social care. Implementation Science. 2010;5 doi: 10.1186/1748-5908-5-67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Haukka E, Leino-Arjas P, Viikari-Juntura E, Takala EP, Malmivaara A, Hopsu L, Mutanen P, Ketola R, Virtanen T, Pehkonen I, Holtari-Leino M, Nykänen J, Stenholm S, Nykyri E, Riihimäki H. A randomised controlled trial on whether a participatory ergonomics intervention could prevent musculoskeletal disorders. Occup Environ Med. 2008;65:849–856. doi: 10.1136/oem.2007.034579. [DOI] [PubMed] [Google Scholar]
- Hecker S, Gibbons B, Barsotti A. Making ergonomic changes in construction: Worksite training and task intervention. In: Alexander D, Raboum R, editors. Appl Ergon. London: Taylor & Francis; 2001. pp. 162–189. [Google Scholar]
- Hess JA, Hecker S, Weinstein M, Lunger M. A participatory ergonomics intervention to reduce risk factors for low-back disorders in concrete laborers. Appl Ergon. 2004;35:427–441. doi: 10.1016/j.apergo.2004.04.003. [DOI] [PubMed] [Google Scholar]
- Hignett S, Wilson JR, Morris W. Finding ergonomic solutions–participatory approaches. Occupational Medicine-Oxford. 2005;55:200–207. doi: 10.1093/occmed/kqi084. [DOI] [PubMed] [Google Scholar]
- Israel BA, Schurman SJ, House JS. Action research on occupational stress: involving workers as researchers. Int J Health Serv. 1989;19:135–155. doi: 10.2190/L2JF-U13W-FT0X-DFXM. [DOI] [PubMed] [Google Scholar]
- Jaegers L, Dale AM, Weaver N, Buchholz B, Welch L, Evanoff B. Development of a program logic model and evaluation plan for a participatory ergonomics intervention in construction. Am J Ind Med. 2014;57:351–361. doi: 10.1002/ajim.22249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim S, Nussbaum MA, Jia B. Low back injury risks during construction with prefabricated (panelised) walls: effects of task and design factors. Ergonomics. 2011;54:60–71. doi: 10.1080/00140139.2010.535024. [DOI] [PubMed] [Google Scholar]
- Koningsveld EAP, Dul J, Van Rhijn GW, Vink P. Enhancing the impact of ergonomics interventions. Ergonomics. 2005;48:559–580. doi: 10.1080/00140130400029136. [DOI] [PubMed] [Google Scholar]
- Linnan L, Steckler A. Process evaluation for public health interventions and research: An overview. In: Steckler A, Linnan L, editors. Process evaluation for pubc health interventions and research. San Francisco: Jossey-Bass; 2002. pp. 1–23. [Google Scholar]
- Moir S, Buchholz B. Emerging participatory approaches to ergonomic interventions in the construction industry. Am J Ind Med. 1996;29:425–430. doi: 10.1002/(SICI)1097-0274(199604)29:4<425::AID-AJIM31>3.0.CO;2-1. [DOI] [PubMed] [Google Scholar]
- National Institute for Occupational Safety and Health (NIOSH) Easy Ergonomics: A Guide to Selecting Non-Powered Hand Tools: DHHS (NIOSH) 2004. (Publication No. 2004–164). [Google Scholar]
- Occupational Safety & Health Administration (OSHA) Ergonomics eTool: Solutions for Electrical Contractors. Materials Handeling. 2003 https://www.osha.gov/SLTC/etools/electricalcontractors/materials/index.html.
- Oude Hengel KM, Blatter BM, van der Molen HF, Bongers PM, van der Beek AJ. The effectiveness of a construction worksite prevention program on work ability, health, and sick leave: results from a cluster randomized controlled trial. Scand J Work Environ Health. 2013;39:456–467. doi: 10.5271/sjweh.3361. [DOI] [PubMed] [Google Scholar]
- Punnett L, Warren N, Henning R, Nobrega S, Cherniack M, The CPH-NEW Research Team Participatory Ergonomics as a Model for Integrated Programs to Prevent Chronic Disease. J Occup Environ Med. 2013;55:S19–24. doi: 10.1097/JOM.0000000000000040. [DOI] [PubMed] [Google Scholar]
- Ringen K, Englund A. The construction industry. Ann N Y Acad Sci. 2006;1076:388–393. doi: 10.1196/annals.1371.007. [DOI] [PubMed] [Google Scholar]
- Ringen K, Englund A, Welch L, Weeks JL, Seegal JL. Why construction is different. Occup Med. 1995;10:255–259. [PubMed] [Google Scholar]
- Rivilis I, Van Eerd D, Cullen K, Cole DC, Irvin E, Tyson J, Mahood Q. Effectiveness of participatory ergonomic interventions on health outcomes: a systematic review. Appl Ergon. 2008;39:342–358. doi: 10.1016/j.apergo.2007.08.006. [DOI] [PubMed] [Google Scholar]
- Robson LS, Shannon HS, Goldenhar LM, Hale AR. Guide to Evaluating the Effectiveness of Strategies for Preventing Work Injuries: How to Show Whether a Safety Intervention Really Works: NIOSH - DHHS (NIOSH) 2001. (Publication No. 2001–119). [Google Scholar]
- Salem S, Genaidy A, Albers J, Shell R, Sobeih T, Rinder MM. Use and acceptability of reduced-weight Portland cement bags in masonry construction: An observational pilot study. Human Factors and Ergonomics in Manufacturing & Service Industries. 2008;18:253–269. [Google Scholar]
- Silverstein B, Evanoff B. Musculoskeletal Disorders. In: Levy BS, Wegman DH, Baron SL, Sokas RK, editors. Occupational and Environmental Health: Recognizing and Preventing Disease and Injury. 6th. Oxford: Oxford University Press; 2011. pp. 335–365. [Google Scholar]
- Smallwood J. Mass of materials: the impact of designers on construction ergonomics. Work. 2012;41:5425–5430. doi: 10.3233/WOR-2012-0842-5425. [DOI] [PubMed] [Google Scholar]
- St-Vincent M, Bellemare M, Toulouse G, Tellier C. Participatory ergonomic processes to reduce musculoskeletal disorders: summary of a Québec experience. Work. 2006;27:123–135. [PubMed] [Google Scholar]
- van der Molen HF, Sluiter JK, Hulshof CT, Vink P, van Duivenbooden C, Frings-Dresen MH. Conceptual framework for the implementation of interventions in the construction industry. Scand J Work Environ Health. 2005a;31:96–103. [PubMed] [Google Scholar]
- van der Molen HF, Sluiter JK, Hulshof CT, Vink P, van Duivenbooden C, Holman R, Frings-Dresen MH. Implementation of participatory ergonomics intervention in construction companies. Scandinavian Journal of Work Environment & Health. 2005b;31:191–204. doi: 10.5271/sjweh.869. [DOI] [PubMed] [Google Scholar]
- van Eerd D, Cole D, Irvin E, Mahood Q, Keown K, Theberge N, Village J, St Vincent M, Cullen K. Process and implementation of participatory ergonomic interventions: a systematic review. Ergonomics. 2010;53:1153–1166. doi: 10.1080/00140139.2010.513452. [DOI] [PubMed] [Google Scholar]
- Vink P, Koningsveld EA, Molenbroek JF. Positive outcomes of participatory ergonomics in terms of greater comfort and higher productivity. Appl Ergon. 2006;37:537–546. doi: 10.1016/j.apergo.2006.04.012. [DOI] [PubMed] [Google Scholar]
- Vink P, Urlings IJM, vanderMolen HF. A participatory ergonomics approach to redesign work of scaffolders. Safety Science. 1997;26:75–85. [Google Scholar]
- Washington State Department of Labor and Industries. Evaluation tools: Caution and Hazard Zone Checklists. 2000 http://www.lni.wa.gov/Safety/Topics/Ergonomics/ServicesResources/Tools/default.asp. Accessed September 15, 2015.
- Wells R, Laing A, Cole D. Characterizing the intensity of changes made to reduce mechanical exposure. Work. 2009;34:179–193. doi: 10.3233/WOR-2009-0915. [DOI] [PubMed] [Google Scholar]
- Wiberg V. Communication of Ergonomics in building and construction. Work. 2012;41(Suppl 1):4111–4115. doi: 10.3233/WOR-2012-1038-4111. [DOI] [PubMed] [Google Scholar]
- Wilson JR, Haines HM. Participatory ergonomics. In: Salvendy G, editor. Handbook of human factors and ergonomics. 2nd. New York: Wiley; 1997. pp. 490–513. [Google Scholar]
- Yazdani A, Neumann WP, Imbeau D, Bigelow P, Pagell M, Wells R. Prevention of musculoskeletal disorders within management systems: A scoping review of practices, approaches, and techniques. Appl Ergon. 2015;51:255–262. doi: 10.1016/j.apergo.2015.05.006. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.