

Abstract
Background:
Although results of many studies have indicated an increased risk of asthma in former late preterm (LPT) infants, most of these studies did not fully address covariate imbalance.
Objective:
To compare the cumulative frequency of asthma in a population-based cohort of former LPT infants to that of matched term infants in their early childhood, when accounting for covariate imbalance.
Methods:
From a population-based birth cohort of children born 2002–2006 in Olmsted County, Minnesota, we assessed a random sample of LPT (34 to 36 6/7 weeks) and frequency-matched term (37 to 40 6/7 weeks) infants. The subjects were followed-up through 2010 or censored based on the last date of contact, with the asthma status based on predetermined criteria. The Kaplan-Meier method was used to estimate the cumulative incidence of asthma during the study period. Cox models were used to estimate the hazard ratio and 95% confidence interval for the risk of asthma, when adjusting for potential confounders.
Results:
LPT infants (n = 282) had a higher cumulative frequency of asthma than did term infants (n = 297), 29.9 versus 19.5%, respectively; p = 0.01. After adjusting for covariates associated with the risk of asthma, an LPT birth was not associated with a risk of asthma, whereas maternal smoking during pregnancy was associated with a risk of asthma.
Conclusion:
LPT birth was not independently associated with a risk of asthma and other atopic conditions. Clinicians should make an effort to reduce exposure to smoking during pregnancy as a modifiable risk factor for asthma.
Keywords: Asthma, epidemiology, risk, late preterm, smoking, birth cohort, covariate imbalance, modifiable, confounder, population-based
Late preterm (LPT) birth 34–36 6/7 weeks gestation annually accounts for 1 in 12 births in the United States.1 In recent years, research has increasingly focused on the morbidities in this population, including respiratory outcomes, e.g., asthma2–5 as the most common chronic illness among children.6 Although LPT infants are generally “healthy” compared with those born extremely premature, they still experience significant early respiratory morbidities compared with term infants.7 A few studies demonstrated a higher risk of asthma among LPT infants, but the validity of the results may be impacted by inadequate control of covariate imbalance.8–10 We assessed whether known risk factors for asthma (e.g., confounders) account for the association between LPT and the risk of asthma.
METHODS
Study Design
This was a retrospective birth cohort study that compared the incidence of asthma between LPT infants and term infants born in Olmsted County, Minnesota. The study was reviewed and approved by the institutional review board at the Mayo Clinic and Olmsted Medical Center.
Study Setting and Subjects
Health care in Olmsted County, Minnesota, is geographically self-contained within the region. All infants born to mothers who resided in Olmsted County between January 1, 2002, and December 31, 2006, were eligible for this study and were initially screened for inclusion by using the Rochester Epidemiology Project.11,12 Subjects were included if their parent had given research authorization, been born during the study period at a gestational age of 34 0/7 to 40 6/7 weeks, and been an Olmsted County resident at birth. Birth hospitalization notes were reviewed, and patients were excluded based on conditions listed in Supplemental Table 1. We included all LPT infants who were identified as small for gestational age or large for gestational age based on birth weight cutoffs for sex and completed week of gestation. Among LPT infants who were appropriate for gestational age, 200 subjects were randomly selected. Term subjects were frequency matched based on sex, birth hospital, size for gestational age, gestational age distribution, and year of birth.
Asthma Ascertainment
The primary outcome was the development of asthma as defined by criteria previously described and noted in Supplemental Table 2.13,14 Definite and probable asthma cases were considered to be subjects with asthma because most probable asthmas become definite asthmas over time.14 Secondary outcomes included physician-diagnosed other atopic conditions (eczema and/or atopic dermatitis, and allergic rhinitis and/or hay fever).
Other Variables
We reviewed the entire medical record, including the birth certificate, to collect all pertinent covariates and potential confounders for the study (Table 1).
Table 1.
Relationship between LPT births and the risk of asthma when controlling matching variables
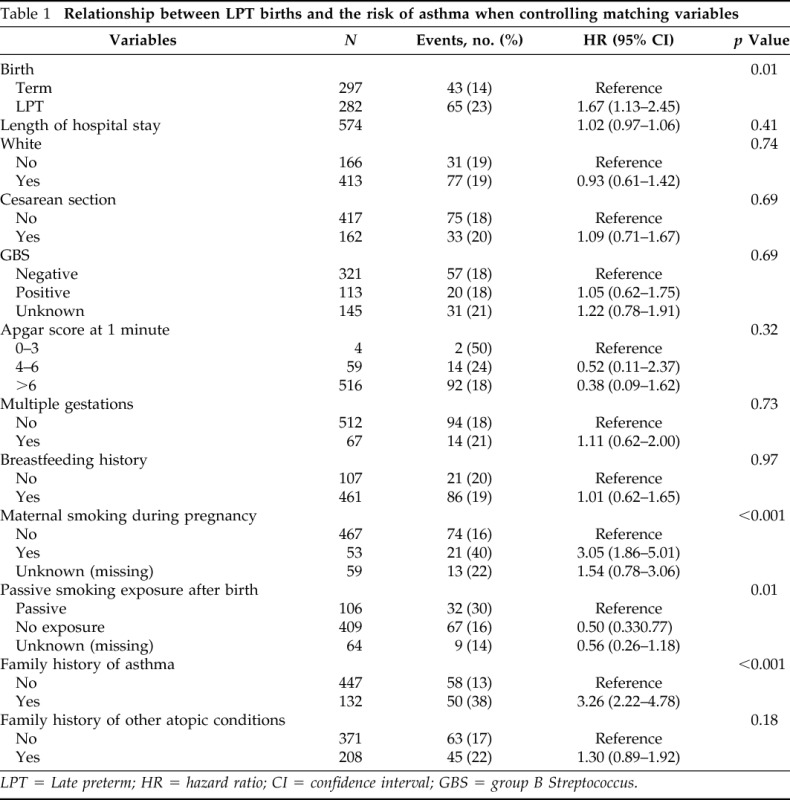
LPT = Late preterm; HR = hazard ratio; CI = confidence interval; GBS = group B Streptococcus.
Statistical Analysis
Descriptive statistics (median [25th, 75th percentile] for continuous variables, and counts [percentages]) were used to compare the two cohorts. For each characteristic, the difference was compared by using logistic regression models when adjusting for matching factors. The cumulative incidence of asthma during the first 8 years of life was calculated by using Kaplan-Meier estimates and the log-rank test for statistical significance. The risk of asthma between LPT and term infants was compared by using unadjusted Cox proportional hazards models. Characteristics were tested for an association with LPT by using logistic regression, and a p value of <0.2 indicated a potential relationship. These potential confounders were then tested for association with the risk of asthma univariately by using Cox proportional hazards models. A multivariable Cox regression model was created to assess the relationship between LPT and the risk of asthma after controlling for all potential confounders (Table 1). Similar analyses were conducted for risk of other atopic conditions. All statistical analyses were adjusted for matching factors and performed by using SAS software, version 9.3 (SAS Institute Inc., Cary, NC).
RESULTS
During 2002–2006, there were 8113 eligible births in Olmsted County. Eleven infants were excluded because there was no identifiable birth weight. Of the remaining 8102 infants, 647 were LPT and 7455 were term births. In the LPT cohort, we enrolled 29 small for gestational age, a random sample of 195 appropriate for gestational age, and 58 large for gestational age infants. The final term cohort included the following: 27 small for gestational age, 200 appropriate for gestational age, and 70 large for gestational age infants. The LPT cohort was slightly smaller than the term cohort because not all excluded subjects had a suitable replacement match. The demographic and clinical characteristics are shown in Table 1. There were significant differences in risk factors for asthma, such as smoking during pregnancy, passive smoke exposure after birth, and a family history of asthma. Each of these factors was more common in the LPT cohort, whereas breast milk exposure was less common in the LPT group (78 versus 85%; p = 0.04).
The cumulative incidence of asthma is shown in Fig. 1, with each “step” denoting the age in years in which a subject met the criteria for asthma. The cumulative incidence of asthma at 5 years in the LPT cohort was 29.9% compared with 19.5% in the term cohort (unadjusted hazard ratio [HR]1.67 [95% confidence interval {CI}, 1.13–2.45]; p = 0.01) (Table 1). We analyzed the potential confounders related to LPT in univariate Cox models as summarized in Table 1. The following factors were associated with an increased risk of asthma: maternal smoking during pregnancy (HR 3.05 [95% CI, 1.86–5.01]), passive smoke exposure after birth (HR 1.99 [95% CI, 1.29–3.07]), family history of asthma (HR 3.26 [95% CI, 2.22–4.78]), and family history of other atopic conditions (HR 1.30 [95% CI, 0.89–1.92]). Also, after controlling for all pertinent covariates, we found that the association between LPT births and the risk of asthma was significantly attenuated and lacked statistical significance (adjusted HR 1.44; p = 0.07) (Table 2). However, a family history of asthma and maternal smoking during pregnancy imparted an independent association for the risk of asthma (Table 2). LPT births were not associated with a risk of other atopic conditions (HR 1.26 [95% CI, 0.93–1.71]; p = 0.13).
Figure 1.

Cumulative incidence of asthma in late preterm and term infants, and the parameter estimate by univariate analysis.
Table 2.
Multivariable Cox models for the association between LPT and the risk of asthma and other atopic conditions
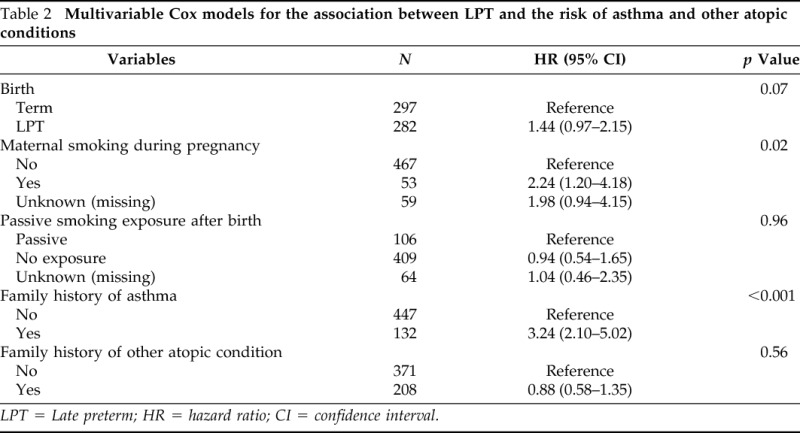
LPT = Late preterm; HR = hazard ratio; CI = confidence interval.
DISCUSSION
We found that healthy LPT infants had a higher incidence of asthma by school age, with an HR of 1.67 (p = 0.01) in an unadjusted Cox proportional hazard model. However, after controlling for maternal smoking during pregnancy, passive smoke exposure after birth, and a family history of asthma and other atopic conditions, the HR for asthma in LPT infants was significantly attenuated, at 1.44, and was no longer significantly different (p = 0.07). A recent review of outcomes of LPT birth specifically addresses what is known on respiratory outcomes in this population.15 Overall, the published literature continues to demonstrate contradictory findings, some of which may be attributed to subject bias and difficulty controlling confounding variables.8,10,16 We also recently demonstrated that a historical birth cohort of LPT infants had a significantly increased risk of asthma compared with term infants.2 After fully adjusting for covariate imbalance by using propensity score matching, there was no significant difference in the incidence of asthma (HR 1.13; p = 0.56).2
The key finding of our study was the role of maternal smoking during pregnancy as a modifiable environmental exposure, which accounted for the association between LPT and the risk of asthma. Several other studies noted the importance of maternal smoking during pregnancy and the impact on the risk of asthma.17–21 Smoking during pregnancy has been shown to increase the risk of preterm birth, which likely accounts for the difference of this confounder between the two cohorts in our study.22,23 This confounder must be included in any study that assesses the association of preterm birth and asthma.
Our study had inherent limitations as a retrospective study design. Our study population was predominantly suburban and white, so the findings may not be generalizable to other populations and settings. Because information regarding smoking during pregnancy and passive smoke exposure after birth was collected from the medical record, we were unable to accurately assess the precise timing of maternal smoking during pregnancy. Future prospective studies that focus on the timing of smoke exposure in utero and passive exposure after birth may help to further define the full impact of these confounders. Our study had several strengths. First, we minimized selection bias by sampling a population-based birth cohort. Second, our use of standard definitions of LPT and utilization of birth records to determine subjects' gestational ages minimized the risk of misclassification bias of LPT births. Third, we improved the accuracy of the asthma diagnosis by using predetermined criteria instead of International Classification of Diseases codes or self-report for asthma. Fourth, the main findings and the identified confounders were consistent between our current and previous study2; similarly, the absence of an association between LPT birth and the risks of other atopic conditions demonstrated consistency and biologic coherence.
CONCLUSION
LPT birth is not independently associated with the risk of asthma and other atopic conditions. We found a critical role of smoking during pregnancy in the development of asthma among LPT infants. Smoking cessation programs during pregnancy have not been highly successful in the past, and more efforts could be made in this area because it would likely reduce the risk of preterm births and asthma.24 Although clinicians should make an effort to reduce exposure to smoking during pregnancy, parents whose child was born LPT should be reassured about their child's own risk for eventually developing asthma.
ACKNOWLEDGMENTS
We thank Kelly Okeson for her administrative assistance.
Footnotes
This work was supported by National Institutes of Health (NIH) R01 grant (R01 HL126667), R21 grant (R21AI116839), and a Mayo Clinic Small Grant Program. It was made possible by Rochester Epidemiology Project (R01-AG34676) from the National Institute on Aging and Clinical and Translational Science Awards Program grant UL1 TR000135 from the National Center for Advancing Translational Sciences. Its contents are solely the responsibility of the authors and do not necessarily represent the official view of the NIH
Y. Juhn is the principal investigator of the Innovative Asthma Research Methods Award from Genentech. The remaining authors have no conflicts of interest to declare pertaining to this article
Supplemental data available at www.IngentaConnect.com
REFERENCES
- 1. Hamilton BE, Martin JA, Ventura SJ. Births: Preliminary data for 2012. Natl Vital Stat Rep 62;1–20, 2013. Available online at http://www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_03.pdf; accessed December 15, 2013. [PubMed] [Google Scholar]
- 2. Voge GA, Katusic SK, Qin R, Juhn YJ. Risk of asthma in late preterm infants: A propensity score approach. J Allergy Clin Immunol Pract 3:905–910, 2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. von Mutius E. No risk of asthma in late-preterm infants: Confounding or misclassification? J Allergy Clin Immun Pract 3:911–912, 2015. [DOI] [PubMed] [Google Scholar]
- 4. Odibo IN, Mac Bird T, McKelvey SS, et al. Childhood respiratory morbidity after late preterm and early term delivery: A study of Medicaid patients in South Carolina. Paediatr Perinat Epidemiol 30:67–75, 2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Saifi M, Bird JA. The burden of childhood asthma and late preterm and early term births. Pediatrics 134(suppl. 3):S163, 2014. [DOI] [PubMed] [Google Scholar]
- 6. Gergen PJ, Mullally DI, Evans R., III National survey of prevalence of asthma among children in the United States, 1976 to 1980. Pediatrics 81:1–7, 1988. [PubMed] [Google Scholar]
- 7. Leone A, Ersfeld P, Adams M, et al. Neonatal morbidity in singleton late preterm infants compared with full-term infants. Acta Paediatr 101:e6–e10, 2012. [DOI] [PubMed] [Google Scholar]
- 8. Dombkowski KJ, Leung SW, Gurney JG. Prematurity as a predictor of childhood asthma among low-income children. Ann Epidemiol 18:290–297, 2008. [DOI] [PubMed] [Google Scholar]
- 9. Raby BA, Celedon JC, Litonjua AA, et al. Low-normal gestational age as a predictor of asthma at 6 years of age. Pediatrics 114:e327–e332, 2004. [DOI] [PubMed] [Google Scholar]
- 10. Abe K, Shapiro-Mendoza CK, Hall LR, Satten GA. Late preterm birth and risk of developing asthma. J Pediatr 157:74–78, 2010. [DOI] [PubMed] [Google Scholar]
- 11. St. Sauver JL, Grossardt BR, Yawn BP, et al. Use of a medical records linkage system to enumerate a dynamic population over time: The Rochester Epidemiology Project. Am J Epidemiol 173:1059–1068, 2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Rocca WA, Yawn BP, St. Sauver JL, et al. History of the Rochester Epidemiology Project: Half a century of medical records linkage in a US population. Mayo Clin Proc 87:1202–1213, 2012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Juhn YJ, Weaver A, Katusic S, Yunginger J. Mode of delivery at birth and development of asthma: A population-based cohort study. J Allergy Clin Immunol 116:510–516, 2005. [DOI] [PubMed] [Google Scholar]
- 14. Yunginger JW, Reed CE, O'Connell EJ, et al. A community-based study of the epidemiology of asthma. Incidence rates, 1964–1983. Am Rev Respir Dis 146:888–894, 1992. [DOI] [PubMed] [Google Scholar]
- 15. Kugelman A, Colin AA. Late preterm infants: Near term but still in a critical developmental time period. Pediatrics 132:741–751, 2013. [DOI] [PubMed] [Google Scholar]
- 16. Goyal NK, Fiks AG, Lorch SA. Association of late-preterm birth with asthma in young children: Practice-based study. Pediatrics 128:e830–e838, 2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Jaakkola JJ, Gissler M. Maternal smoking in pregnancy, fetal development, and childhood asthma. Am J Public Health 94:136–140, 2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Simoes EA. Maternal smoking, asthma, and bronchiolitis: Clear-cut association or equivocal evidence? Pediatrics 119:1210–1212, 2007. [DOI] [PubMed] [Google Scholar]
- 19. Carter S, Percival T, Paterson J, Williams M. Maternal smoking: Risks related to maternal asthma and reduced birth weight in a Pacific Island birth cohort in New Zealand. N Z Med J 119:U2081, 2006. [PubMed] [Google Scholar]
- 20. Lewis S, Richards D, Bynner J, et al. Prospective study of risk factors for early and persistent wheezing in childhood. Eur Respir J 8:349–356, 1995. [DOI] [PubMed] [Google Scholar]
- 21. Vardavas CI, Hohmann C, Patelarou E, et al. The independent role of prenatal and postnatal exposure to active and passive smoking on the development of early wheeze in children. Eur Respir J 48:115–124, 2016. [DOI] [PubMed] [Google Scholar]
- 22. Andres RL, Day MC. Perinatal complications associated with maternal tobacco use. Semin Neonatol 5:231–241, 2000. [DOI] [PubMed] [Google Scholar]
- 23. Cnattingius S. The epidemiology of smoking during pregnancy: Smoking prevalence, maternal characteristics, and pregnancy outcomes. Nicotine Tob Res 6(suppl. 2):S125–S140, 2004. [DOI] [PubMed] [Google Scholar]
- 24. Lumley J, Chamberlain C, Dowswell T, et al. Interventions for promoting smoking cessation during pregnancy. Cochrane Database Syst Rev (3):CD001055, 2009. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.