

Abstract
[Purpose] We investigated Achilles tendon injury in Kendo players in junior and senior high schools to obtain a possible indicator for preventing an outbreak of Achilles tendon injury and tendonitis, possible risk factors concerning foot function and morphology were extracted. [Subjects and Methods] The subjects were 60 Kendo players aged 14–18 years from Wakayama Prefecture, Japan (33 boys and 27 girls). A questionnaire survey was conducted on the past history, current status, time of occurrence about Achilles tendon pain or rupture, and site of Achilles tendon pain or rupture. Based on the responses to the questionnaire, these students were divided into two groups, i.e., those who had a history of Achilles tendon pain (n=30) or rupture (n=3) (pain group) and those who had no history of Achilles tendon pain (no-pain group), and they were examined for foot alignment, flexion and extension Range of motion test of the first toe, flexion and extension muscle strength of the first toe, and opening movement of the toes. [Results] Achilles tendon pain had occurred in 53% of the Kendo players (including 3 who had suffered Achilles tendon rupture). Poor foot alignment and deterioration of opening movement of the toes were noted in the pain group. [Conclusion] Foot alignment was poor and opening function of the toes deteriorated in the pain group, suggesting that these may be some of factors for Achilles tendon injury. Training aimed at improving foot alignment and function is important to prevent and improve Achilles tendon injury.
Key words: Achilles tendon injury, Foot function, Kendo players
INTRODUCTION
Kendo is one of the traditional Japanese sports in which the two players wearing protective guards lunge at each other with a bamboo sword, involving a swift and strong step forward with bare feet. As a result, Kendo players often suffer injuries to the lower leg and foot1). In particular, Achilles tendon pain is common among cases of pain in the lower leg and foot2, 3). In addition, although Achilles tendon rupture is not frequent in view of overall sports injuries, it deserves special attention among injuries in Kendo players in comparison with other sports2, 4,5,6). Because Kendo players wear heavy protective guards and usually take a step forward with the left foot from the ready position standing on tiptoe, left Achilles tendon rupture occurs more frequently7,8,9). In this regard, we investigated Achilles tendon injury in Kendo players in junior and senior high schools to obtain a possible indicator for preventing an outbreak of Achilles tendon injury and tendonitis, possible risk factors concerning foot function and morphology were extracted.
SUBJECTS AND METHODS
The subjects in this study were 60 Kendo players aged 14–18 years (33 boys and 27 girls) from Wakayama Prefecture, Japan, who received an explanation of the study and who gave consent to participate in the study. Their mean age was 15.8 ± 1.5 years; mean height, 165.9 ± 7.6 cm for boys and 157.8 ± 4.7 cm for girls; mean weight, 57.1 ± 16.2 kg for boys and 50.3 ± 6.5 kg for girls; and the mean length of experience, 8.0 ± 2.0 years. A questionnaire survey was conducted with each subject to examine for a history of Achilles tendon pain or rupture and the status of current Achilles tendon pain. In addition, players who had a history of Achilles tendon rupture or pain were also asked about the time of occurrence and the site of pain. Subjects were divided into two groups, i.e., a group of players who had a history of Achilles tendon pain (n=30) or rupture (n=3) (pain group) and another group of players who had no history of Achilles tendon pain (no-pain group) based on the results of the questionnaire survey, and examined for the following 4 items: 1) foot alignment: The method of James et al.10) was employed to measure the leg heel alignment (LHA). With the central part of the lower one third of the lower leg, calcaneal tuberosity, and the heel point as landmark points, the angle between a line connecting each point and the calcaneal bisector line was measured by a goniometer with an increment of 1° (Fig.1-a-1). LHA (± 0°) is the base point, valgus heel alignment (outward twisting of the heel) is shown as “+,” and varus heel alignment (inward twisting of the heel) is shown as “−”. The angle was measured in the upright position with a foot progression angle of 0°. The foot arch height ratio was measured with a ruler as the length (arch height) from the plantar surface (the floor surface) to the surface of the navicular in the standing position (body weight-loaded). The foot arch height was divided by the foot length to calculate a foot arch height ratio (foot arch height ratio (%)=navicular height/foot length) (Fig. 1-a-2); 2) flexibility of the first toe: Range of motion-test of flexion and extension (according to the method prescribed by the Japanese Orthopaedic Association) (Fig. 1-b); 3) Muscle strength of the first toe: Flexion and extension muscle strength of the first toe was measured with a pinch gauge. The values were converted into the strength-to-body weight ratio (Fig. 1-c); and 4) examination of the opening movement of the toes (toe opening movement was checked after verbally instructing to open the toes as wide as possible). The results were compared between the pain group and the no-pain group and between the right and left foot in male and female subjects. Statistical analysis was performed by repeated measures analysis of variance (Tukey’s HSD). We used the statistical processing software SPSS12.0 for Windows, and each significance level was less than 5%. This study was approved by the ethics committee of Sumiya Orthopaedic Hospital.
Fig. 1.

Evaluation of the foot function
RESULTS
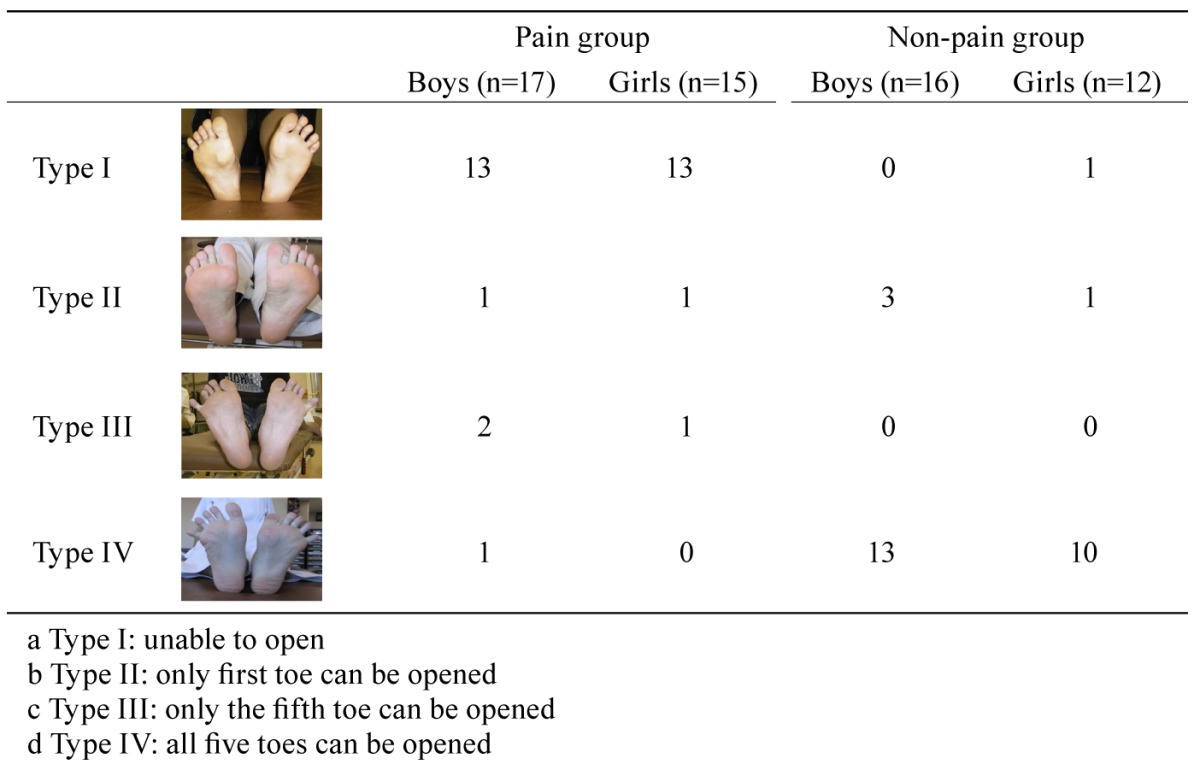
Among the 60 students, 32 (17 boys and 15 girls) had suffered Achilles tendon pain in the past, and 3 (1 boy and 2 girls) had experienced Achilles tendon rupture. Seven students (3 boys and 4 girls) had persistent pain at the time of the survey. Twenty eight (16 boys and 12 girls) of the 60 students had no history of Achilles tendon pain. Achilles tendon pain occurred during elementary school in 5 students, junior high school in 17, and senior high school in 10, showing that injury was most common in junior high school students. Achilles tendon rupture occurred in the third year of junior high school in 1 student (girl) and in the third year of senior high school in 2 students (1 boy and 1 girl). Pain occurred in the medial part of the left Achilles tendon in 18 students, in the central part of the left Achilles tendon in 12, and in the attachment site of the calcaneal tuberosity in 2; there were none with pain in the right foot. Intergroup comparison regarding foot alignment revealed that the leg-heel alignment angle was significantly higher in the pain group among both boys and girls, indicating the valgus (pronated) position of the heel bone. In terms of the foot arch height ratio, the foot arch was significantly smaller in the pain group. Although there were no significant differences between the right and left foot, the pronation of the heel bone tended to be more prominent, and the foot arch smaller, in the left foot in the pain group (Table 1). As distinct findings of the flexibility of the first toe in Kendo players, the range of motion was significantly greater in flexion of the right foot and in extension of the left foot in both boys and girls (p<0.05). No significant differences were noted in intergroup comparison of the pain and no-pain groups (Table 2). There were no significant differences in muscle strength between the two groups or between the right and left foot (Table 3). Opening movement of the toes was classified into the following four types: Type I, unable to open; Type II, only first toe can be opened; Type III, only the fifth toe can be opened; Type IV, all five toes can be opened. In the no-pain group, Type IV accounted for 80%, whereas Type II and Type I accounted for 15% and 5%, respectively. In the pain group, Type I accounted for 80%; Type II, 4%; and Type III and Type IV, 8% each. In contrast to the no-pain group, toe opening movement was poor in the pain group (Table 4).
Table 1. Foot alignment.
| Pain group | Non-pain group | ||||
|---|---|---|---|---|---|
| Boys (n=17) | Girls (n=15) | Boys (n=16) | Girls (n=12) | ||
| Leg-heel alignment (°) | rt | 16.5 ± 1.8 | 16.8 ± 1.8 | 4.4 ± 2.0** | 4.7 ± 0.9** |
| lt | 17.3 ± 0.9 | 17.4 ± 1.2 | 4.9 ± 2.3** | 4.3 ± 1.1** | |
| Foot arch height ratio (%) | rt | 15.1 ± 1.8 | 14.8 ± 1.4 | 19.1 ± 1.2** | 18.2 ± 1.1** |
| lt | 14.3 ± 2.1 | 13.9 ± 2.1 | 18.5 ± 1.3** | 17.9 ± 1.3** | |
Mean ± SD. **p<0.01, *p<0.05 (vs. pain group). rt: right, lt: left
Table 2. Flexibility of the first toe (ROM: flexion extension).
| Pain group | Non-pain group | ||||
|---|---|---|---|---|---|
| Boys (n=17) | Girls (n=15) | Boy (n=16) | Girls (n=12) | ||
| Flexion (°) | rt | 40.7 ± 1.7 | 41.4 ± 2.3 | 41.1 ± 1.8 | 41.4 ± 2.3 |
| lt | 37.1 ± 2.5+ | 37.9 ± 2.5+ | 37.8 ± 2.5+ | 38.9 ± 2.4+ | |
| Extension (°) | rt | 74.3 ± 8.6 | 77.9 ± 0 | 78.8 ± 11.7 | 79.4 ± 8.5 |
| lt | 81.4 ± 8.7+ | 83.6 ± 7.4+ | 84.5 ± 7.5+ | 85.0 ± 6.5+ | |
Mean ± SD. ++p<0.01, +p<0.05 (vs. right). rt: right, lt:left
Table 3. Muscle strength of the first toe (muscle strength to body weight ratio in flexion/extension).
| Pain group | Non-pain group | ||||
|---|---|---|---|---|---|
| Boys (n=17) | Girls (n=15) | Boys (n=16) | Girl (n=12) | ||
| Flexion (%) | rt | 4.2 ± 0.3 | 3.9 ± 0.6 | 4.4 ± 0.5 | 4.0 ± 0.4 |
| lt | 4.2 ± 0.4 | 3.9 ± 0.5 | 4.4 ± 0.4 | 4.0 ± 0.4 | |
| Extension (%) | rt | 2.8 ± 0.05 | 1.9 ± 0.2 | 2.9 ± 0.04 | 2.0 ± 0.2 |
| lt | 2.8 ± 0.06 | 2.0 ± 0.2 | 2.9 ± 0.03 | 2.0 ± 0.1 | |
Mean ± SD. rt: right, lt: left
Table 4. Toe opening movement chec.
DISCUSSION
In this study, Achilles tendon pain occurred in 53% of Kendo players (including three who had Achilles tendon rupture). It was considered that this was an injury that was unusually prevalent in Kendo players. Most Achilles’ tendon injuries occurred during or after junior high school ages. From this, it is suggested that increased self-care from junior high school ages is important. These results provide some suggestions of the relationships between foot part function and the injury occurrence.
Based on findings from studies on the history of Kendo techniques, the focus of techniques has changed from strides centering on shuffling to diving, stamping, and treading-in; Nakamura11) has stated that a decrease in defensive rightward or leftward body movement has been noted since the early Showa period, showing convergence with linear techniques. In the treading-in movement, the Kendo player takes a step forward with the left foot alone from the ready position of standing on the toes of both feet. Strong stress imposed at this time on the left triceps surae muscle or Achilles tendon seems to serve as a causative factor of injury. It has been reported that Achilles tendon rupture occurs when Kendo players make a lunge step forward from the rear position because they assume a ready position with the left foot placed backward and the right foot forward12, 13). Arner et al. reported three mechanisms underlying the occurrence of Achilles tendon rupture: abrupt, forced dorsal flexion of the ankle; sudden change of the position of the ankle from plantar flexion to dorsal flexion; and pushing off with body weight on the forefoot in the knee extension position, and stated that the third mechanism is responsible for most cases of sports injuries14). These injuries occur because of tension exceeding the contractility of the triceps surae muscle is applied to the Achilles tendon15). Since Achilles tendon ruptures in Kendo players occur under the same conditions, we previously thought that the muscle strength of the triceps surae muscle and the toes (particularly the flexor hallucis longus muscle) serving as deep muscles supporting the Achilles tendon is important to reduce the stress. However, the present study revealed no difference between the pain group and the no-pain group, suggesting that the muscle strength and flexibility of the toes are not closely associated with the occurrence or prevention of injuries. In contrast, the pain group showed poor foot alignment, such as decreased foot arch during loading and prominent pronation in leg-heel alignment, and limited movement of opening the toes. Therefore, it is inferred that poor alignment and limited opening of the toes may be involved in the occurrence of Achilles tendon pain and rupture. These are factors detrimental to shock absorption during exercise and efficient transmission of the kicking out force at the time of lunging, and therefore, decreased efficiency of shock absorption and force transmission may impose a heavy burden on the Achilles tendon. Kawamura et al. reported that athletes who often suffered from injuries characteristically showed an imbalanced morphology with right-left asymmetry16). In the present study, there was a right-left difference in foot alignment in the pain group, although the difference was not statistically significant. Thus, for the purpose of preventing Achilles tendon injury, it is necessary to compensate for the right-left imbalance of foot alignment and perform muscle training and stretching aimed at improving flexibility to build the body with good posture balance. In addition, Takashi et al. have reported that poor foot alignment is related to poor treading-in movement (knee-in toe-out) in young Kendo players during the growth phase17). This indicates that it is important to instruct Kendo players in the growth phase to master the correct treading-in movement.
REFERENCES
- 1.Baba H, Imamura K, Iwasaki K: Survey of the actual situation of orthopedic sports injuries in boys playing Kendo. Jpn J Orthop Sports Med, 1995, 15: 361–365. [Google Scholar]
- 2.Watarai K, Takeda H, Oguro K, et al. : Sports injuries in young Kendo players. J Clin Sports Med, 1987, 4: 18–22. [Google Scholar]
- 3.Kisi S, Yoshikawa N, Sakaguchi Y, et al. : A consideration of injuries in the lower leg and the foot in Kendo players. Jpn J Clin Sports Med, 2000, 8: 278–285. [Google Scholar]
- 4.Waku T, Ozawa S: Longitudinal study of sports injuries in Kendo: association between the occurrence of injuries and time of practice. Proceedings of the Department of Sports Sciences College of Arts and Sciences, The University of Tokyo, 1994, 28: 54–51.
- 5.Watanabe H, Kira S: Injuries of extremities and their treatment in university students playing Kendo. Jpn J Sch Health, 1997, 39: 139–146. [Google Scholar]
- 6.Watanabe H, Tanabe G, Kira S: Site of pain in Kendo players: from the questionnaire survey in the 29th Teachers and Staff’s National KENDO Championships. J Clin Sports Med, 1988, 5: 231–234. [Google Scholar]
- 7.Mizumachi S, Mizushima T, Morisaki N, et al. : Martial art-related injuries during the past 12 years. J Jpn Orthop Assoc, 1942, 17: 634–636. [Google Scholar]
- 8.Ito K: Sports injuries in Kendo. Saigai Igaku, 1957, 1: 111–116. [Google Scholar]
- 9.Ishikawa T, Matsui S. (eds.): Sports Medicine, 4th ed. Kyorin-Shoin, 1986, pp 438–440. [Google Scholar]
- 10.James SL, Bates BT, Osternig LR: Injuries to runners. Am Sports Med, 1978, 6: 40–50. [DOI] [PubMed] [Google Scholar]
- 11.Nakamura T: Kendo Jiten. Saitama: Shimazu Shobo, 2004, p 36. [Google Scholar]
- 12.Nakayama S, Takakura Y, Tanaka Y: Sports and Achilles tendon rupture. MB. Orthop, 2003, 16: 8–15. [Google Scholar]
- 13.Sato K, Yuzuki O: Achilles tendon rupture in Kendo players. J Kansai Clin Sports Med Sci, 2000, 10: 51–53. [Google Scholar]
- 14.Arner O, Lindholm A: Subcutaneous rupture of the Achilles tendon; a study of 92 cases. Acta Chir Scand Suppl, 1959, 116: 1–51. [PubMed] [Google Scholar]
- 15.Nango A: Achilles tendon rupture in athletes: characteristic features of competitive sports and the mechanisms of injuries. J Clin Sports Med, 2007, 24: 1049–1055. [Google Scholar]
- 16.Kawamura T, Hirai J, Imai S, et al. : Relationship between the type of physique and injuries in martial arts athletes. Bulletin of Institute of Health and Sport Science, University of Tsukuba, 1978, 1: 87–99. [Google Scholar]
- 17.Kisi S, Yoshikawa N, Chiba S, et al. : A consideration of pain in the lower leg and foot in Kendo players: effects of the treading-in movement in the growth phase on the foot arch. Jpn J Clin Sports Med, 2002, 10: 82–89. [Google Scholar]