

Abstract
A fundamental understanding of multitasking within nursing workflow is important in today’s dynamic and complex healthcare environment. We conducted a time motion study to understand nursing workflow, specifically multitasking and task switching activities. We used TimeCaT, a comprehensive electronic time capture tool, to capture observational data. We established inter-observer reliability prior to data collection. We completed 56 hours of observation of 10 registered nurses. We found, on average, nurses had 124 communications and 208 hands-on tasks per 4-hour block of time. They multitasked (having communication and hands-on tasks simultaneously) 131 times, representing 39.48% of all times; the total multitasking duration ranges from 14.6 minutes to 109 minutes, 44.98 minutes (18.63%) on average. We also reviewed workflow visualization to uncover the multitasking events. Our study design and methods provide a practical and reliable approach to conducting and analyzing time motion studies from both quantitative and qualitative perspectives.
Introduction
Nursing or clinical workflow describes a wide range of steps or activities that health personnel execute to accomplish an activity in patient care.1 A fundamental understanding of multitasking within the workflow of nurses is important in today’s dynamic and complex healthcare environment. Demands for healthcare and nursing care to become a more patient-centered, efficient, effective and cost effective process, while also producing high quality patient outcomes can result in work that is fragmented due to interruptions or multitasking. Kalish and Abersold (2010),2 identified nurse’s work as complex and error prone. Although nurses may manage interruptions or multitasking well, it is important to gain further understanding of nursing workflow in order to develop strategies to minimize errors and maximize processes that enhance patient safety. As techniques to measure nurses’ workflow are limited, we reviewed the definition of multitasking and time motion studies being conducted commonly to model clinical workflow.
Multitasking and task switching
Multitasking requires a conscious shift in attention over a short time span between different tasks.3 The definition of multitasking depends on context. Lay understanding of multitasking is the performance of two or more tasks simultaneously. Healthcare researchers often define multitasking in similar ways.2,4–7 The related concepts of concurrent multitasking, dual task performance, parallel task performance, interleaved multitasking, and sequential multitasking describe various aspects of the cognitive processes believed to be associated with multitasking. Because these concepts overlap and intertwine,8 below we reviewed the definition and established the scope for our observational study.
Walter (2015) investigated on the concept of multitasking and found that multitasking has been defined in various ways;9 it could be concurrent multitasking (or dual task), interleaved multitasking (also called task switching), or sequential multitasking.9 Functional MRIs showed evidence for multitasking and task switching,10–12 and the use of computer models of stimulus response activity13,14 helped our understanding of cognitive processes in the laboratory setting. Cognitive process theorists proposed that multitasking may actually be rapid task switching.14,15 Recent work in neuroimaging16, eye tracking17 and computer simulation18 demonstrated that multitasking could be considered as the rapid cognitive process of task switching.10,11,19 However, cognitive processes examination, using fMRI, eye tracking, or computer simulations are unobservable in the real world setting.
Task switching has also been described as a rudimentary function of cognitive control requiring the flexible ability to configure and reconfigure tasks to meet shifting internal and external demands and cues.13,15,20 Draheim (2016) define task switching as “the ability to allocate attentive resources to several tasks sequentially and fluently reallocate attentive resources from one task to another.”21 Task switching involves the performance of two or more different tasks in a rapidly integrated process and depends on several factors including complexity of task as well as familiarity of task.14
The daily workflow of nurses requires the performance of various skills or activities, such as communication, education, medication administration, electronic and paper documentation, as well as frequent and rapid shifts between these activities. Doing more than one thing at a time is colloquially referred to as multitasking and has been defined as “simultaneous performance of two discrete tasks.”7 In our study, we were unable to observe the rapid cognitive processes associated with task switching in a naturalistic setting. Therefore, we operationalized our definition of multitasking as the observable performance of two or more tasks simultaneously,2 for example, talking to a patient and preparing medication. Conversely, we defined task switching as alternating or changing between two separate tasks, sometimes rapidly but observably.22 We limit our definitions to observable behavior, as opposed to cognitive processing.
Studies measuring multitasking and task switching
Time-Motion Studies, or Time and Motion Studies, have been successfully adopted as a working method to describe and assess clinical workflow in healthcare environments.23 The National Library of Medicine’s controlled vocabulary thesaurus defines a Time-Motion Study (TMS) as “the observation and analysis of movements in a task with an emphasis on the amount of time required to perform the task”.24 TMS consists of two major components: time and motion analysis. Motion analysis represents workflow, which is a sequence of “steps” or “tasks” for a process or an event; time analysis focuses on time duration of the tasks or the entire process. Time-motion studies have been commonly used to discover nursing staff work patterns, workflow efficiency and multitasking.25–28
Measuring multitasking or task switching enables healthcare organizations to improve efficiencies, quality and safety, workflow, and clinician job satisfaction.29 Various methods have been used in the study of multitasking and task switching, including qualitative studies and observational studies using paper, pencil and stopwatches,30,31 post observational interviewing,32 observational studies using electronic data collection devices4,6,33 as well as mixed-methods studies using an excel spreadsheet for data collection during the observation phase.29
Although several studies have been published that have similar aims of measuring multitasking and task switching in the clinical setting, each has a slightly different design with respective strengths and limitations. Using electronic methods, Westbrook (2007)6,33 developed a Personal Data Assistance (PDA) program, called Work Observation Method By Activity Timing (WOMBAT), that allowed observers to select and record behavior from a list of categories. These categories included: direct care, indirect care, medication tasks, documentation, professional communication, ward related activities, in transit, supervision, social or non-work communications, and other tasks outside of these categories The PDA software allowed the observer to document both multitasking (adding tasks occurring at the same time) and interruption (pausing tasks that had been interrupted) occurrences.33 This method provided detailed results with a high level of accuracy secondary to time stamping and duration recording functions of the software. However, it lacked the ability to record a detailed picture of each task switching or multitasking event; rather, it simply allowed the observer to denote that an event falling into one of these two categories occurred (task switching or multitasking). Lack of a universal definition of “interruption” and the inability to reliably capture these interruptions, limited the trustworthiness of the data.
Bastian (2016)29 conducted a time motion study focused on determining workflow (task switching) patterns in the healthcare setting, which utilized Excel spreadsheets to record observed data. This method required observers to enter an activity ID into the Excel template. All other cells populate automatically with time stamp, duration, and full task ID name. Graphical visualizations include pie and bar charts generated from Excel for the percentages in terms of time spent on tasks in each task category. Although user friendly, this data collection method failed to identify the complex details associated with task switching. Also, because of the automatic timestamp (associated in a one-to-one manner with one task), task switching and multitasking failed to be captured, thus limiting the interpretability of nursing activities from the data.
Non-electronic methods of measuring multitasking and task switching have also been used, although considerably less reliable due to manual recording processes necessitating time away from the observation. For instance, traditional stopwatch and paper methods have been used to record multitasking and task switching of clinicians. In a time motion study conducted by Edwards (2009),30 observers shadowed clinicians for two to four hour periods using real time stopwatches and a paper/pencil observational tool system. Another study focused on the changes in communication tasks rather than patient care functions, in which written documentation and audio recordings were used to record communication events.31 The audio recordings were used to accurately monitor interruptions and were later analyzed and transcribed.31 Although effective in recording communication, multitasking, and task switching activities, observers were responsible for both timing the duration of events and providing detailed written accounts. Observation accuracy was limited because of time necessary for paper/pencil documentation. Additionally, non-verbal communications failed to be captured. Lastly, Berg (2013)32 utilized interviews along with hand written documentation of observations to obtain clinicians’ perspectives on their experiences with workflow interruptions. In this study, the observers - experienced nurses - documented six categories (type of activity, duration of the activity, location, persons, interruptions, whether the clinician was the recipient cause of the interruption, and continuation of activity after interruption), which were recorded in written form on a semi structured template.32 While audio recordings and post-observation interviews may be useful adjunct methods to an electronic time-motion methods, handwritten documentation methods lack reliable because of the time required of the observer to record data rather than fully observing clinicians behavior.
In summary, studies using a time motion method to study clinical workflow were inconsistency in their approaches. Zheng (2011)34 proposed Suggested Time And Motion Procedures (STAMP) to standardize research for time motion studies. Following STAMP, we designed a time motion study to understand and visualize nursing workflow on multitasking and task switching activities. We used TimeCaT,35,36 a comprehensive electronic time capture tool to capture data for our time-motion study. TimeCaT is a web based application, optimized for tablets and iPads developed by the Department of Biomedical Informatics at The Ohio State University. It is a fully customizable, web-based, time capture tool designed for time motion studies. TimeCaT can be used to evaluate multitasking, task switching, and interobserver reliability,37 and can be used on any internet capable device. TimeCaT has also been optimized to support data capture using touch enabled devices. We loaded selected nursing activities on TimeCaT (Figure 1), trained student observers, and validated the data capture process using the inter-observer reliability module included in TimeCaT.
Figure 1.
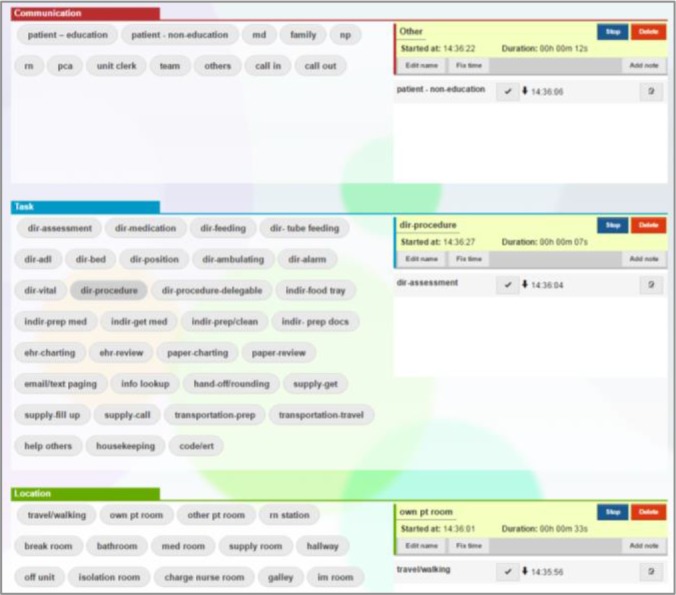
TimeCaT screenshot
Our study was a pilot project for a larger study aiming to understand top of license nursing practice. The purpose of this pilot project was to establish the rigor of the time motion method. With the preliminary data, we were able to describe nursing workflow in three activity dimensions: communication, task and location. Communication includes with whom nurses are interacting; hands-on tasks include tasks requiring nurses to physically touch to perform a task (i.e. start an IV); and location includes where nursing activities take place. We explored these three activity dimensions, across the continuum of time to understand the phenomena of multitasking and task switching in nursing practice.
Methods
Setting and Sample
After obtaining IRB approval, the study was conducted on a medical-surgical unit at The Ohio State University Wexner Medical Center (OSUWMC). The observations occurred in the general patient care areas including the nursing station, hallway, medication room, patient room, and supply areas. This was a pilot study in which we used a convenience sample of registered nurses. The nurses met the following inclusion criteria: (1) full-time staff Registered Nurses (RNs) working at OSUWMC with more than two years of acute care nursing work experience and (2) greater than or equal six months of work experience on the study unit. Informed consent was obtained for this observational study at the time of recruitment.
Observed nursing activities
We observed all nursing activities including anticipated nursing activities and activities which may be classified as non-value added. Anticipated activities include but are not limited to; hand-off (shift reporting), direct patient care (patient assessment, medication administration, patient treatment), discharge planning and admission, documentation (charting), interprofessional communication, care planning, call light response, administrative responsibilities, and communication with patient and family. The observable nursing activities list was finalized during the training phase of the data collection process. In total, we identified and defined 12 types of communication, 30 hands-on tasks, and 14 locations. See representative examples in Table 1.
Table 1.
Selected activities definition table
| Category | Name | Definition | Start-time | End-time |
|---|---|---|---|---|
| Comm. | Patient Education | Planned patient education; direct communication with patient | RN starts talking about education content | RN stops talking about education content or switches to another topic |
| Comm. | Patient Noneducation | Direct communication with patient not concerning planned education; any communication other than planned education. | RN or patient starts talking | Both RN and patient stop talking |
| Comm. | M.D. | Direct communication (verbal and non-verbal) between nurse and physicians | RN or MD starts talking | Both RN and MD stop talking |
| Comm. | Call In | RN answers a call on her OSUMC mobile phone. | RN says hello; starts talking to person calling | RN hangs up the phone |
| Comm. | Call Out | RN calls someone on her OSUMC mobile phone | RN hits green call out button on phone | RN hangs up the phone |
| Hands-on Task | Direct - Assessment | RN performs direct physical assessment | Places hands and/or stethoscope on patient | Removes hands and/or stethoscope |
| Hands-on Task | Direct - Procedure | RN performs treatment or procedure that cannot be delegated (top of license tasks) | RN places hands on pt. or supplies to begin procedure | RN removes hands or switches to another direct task |
| Hands-on Task | Direct - Procedure - delegable | Direct patient care that may be delegated to a PCA or other unlicensed persons | RN places hands on pt. or supplies to begin procedure | RN removes hands or switches to another direct task |
| Hands-on Task | Transportation-prep | Get patient prepared to travel for procedure | Initiate travel preparation, gathering supplies for transport only | patient begins to transport (no longer preparing for transport) |
| Hands-on Task | EHR-Charting | Recording, entering or updating data in the EHR | RN logs on to EHR and starts typing in EHR | RN stops typing or logs off computer |
| Location | Travel/Walking | Time spent walking/traveling in between destinations | Leaves destination and begins traveling | Reaches destination and stops traveling |
| Location | Own Patient Room | In nurses’ assigned patient rooms | Enters assigned patient room and crosses doorway | Leaves assigned patient room and crosses the doorway |
| Location | Hallway | In hallway as a destination | Stops walking in hallway | Continues to walk |
Student observers
In order to obtain quality observational data, we recruited three nursing student as our observers, including one nursing PhD student and two undergraduate senior nursing students. With their background and clinical experience, they were familiar with nursing workflow and were able to recognize and distinguish various nursing activities. All observers understood the study purpose, and were required to participate in research meetings in which of the nursing activities definitions were established. Observers were trained with trial observations for at least 12 hours, and three rounds of inter-observer reliability assessment to ensure study fidelity and data validity prior to beginning actual research observations. All trial observations occurred in the study site which allowed student observers to be familiar with the environment as well as the on-site observation. This also helped introduce the study and study personnel to the nurse participates.as well as other unit personnel.
Inter-observer reliability assessment (IORA)
The establishment of IORA protocols and guidelines is the priority in validating a time motion study. We used the IORA provided in TimeCaT,35 a robust, comprehensive method for inter-observer reliability assessment.37 It considers four types of agreements on the workflow observation: 1) proportion-kappa (P-K): evaluates the naming agreement on virtually created one-second activity, based on the Kappa statistic. P-K provides a global assessment of the agreement over time; 2) naming-kappa (N-K): a systematic pairing approach based on time-overlap, and provides a Kappa statistic representing the agreement on activity naming; 3) duration-concordance correlation coefficient (DCCC): agreement on the duration of an activity. It is the concordance correlation coefficient and intends to provide a means to evaluate the correlation concerning activity duration; and 4) sequence-Needleman-Wunsch (S-NW): agreement of the sequence of activities. It is an assessment focusing specifically on the order of activities recorded. Based on the Needleman-Wunsch sequence alignment algorithm from bioinformatics, the proposed method returns a normalized score that represents an overall sequence agreement. Table 2 presents three IORA training results from two observers. Their performance was improved over time. The IORA provided useful information for observers’ training and a meaningful quantitative IORA report. In addition, we visualized clinical workflow by their sequence and duration, as presented in Figure 2. Each colored band represents an activity; the width of the band represents the duration of the activity. For example, EHR charting and EHR review are two activities which occurred more frequently and longer in duration than other activities. We were also able to compare the activities observed by Observer A against to the activities observed by Observer B. The side-by-side workflow visualization (Figure 2) in TimeCaT allowed us to offer immediate feedback to our observers after the training sessions.
Table 2.
Sample IORA training results from two observers
| Communication | Hands-On Task | Location | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| P-K | N-K | D-CCC | S-NW | P-K | N-K | D-CCC | S-NW | P-K | N-K | D-CCC | S-NW | |
| IORA1 | 83.41% 0.71K | 73.97% 0.65 K | 0.257P | 0.78 | 85.16% 0.78K | 66.73% 0.59K | 0.966p | 0.66 | 95.02% 0.94K | 77.41% 0.69K | 0.99p | 0.79 |
| IORA2 | 85.51% 0.7K | 61.31% 0.46K | 0.98p | 0.79 | 85.14% 0.73K | 56.8% 0.46K | 0.897p | 0.7 | 87.3% 0.85K | 60.14% 0.49K | 0.987 | 0.71 |
| IORA3 | 93.34% 0.8K | 71.03% 0.59K | 0.954p | 0.82 | 88.87% 0.79K | 73.21% 0.67K | 0.992p | 0.78 | 97.46% 0.97K | 84.85% 0.79K | 0.998p | 0.9 |
P-K= proportion-kappa; N-K= naming-kappa; D-CCC= duration-concordance correlation coefficient; S-NW= Sequence-Needleman-Wunsch
Figure 2.
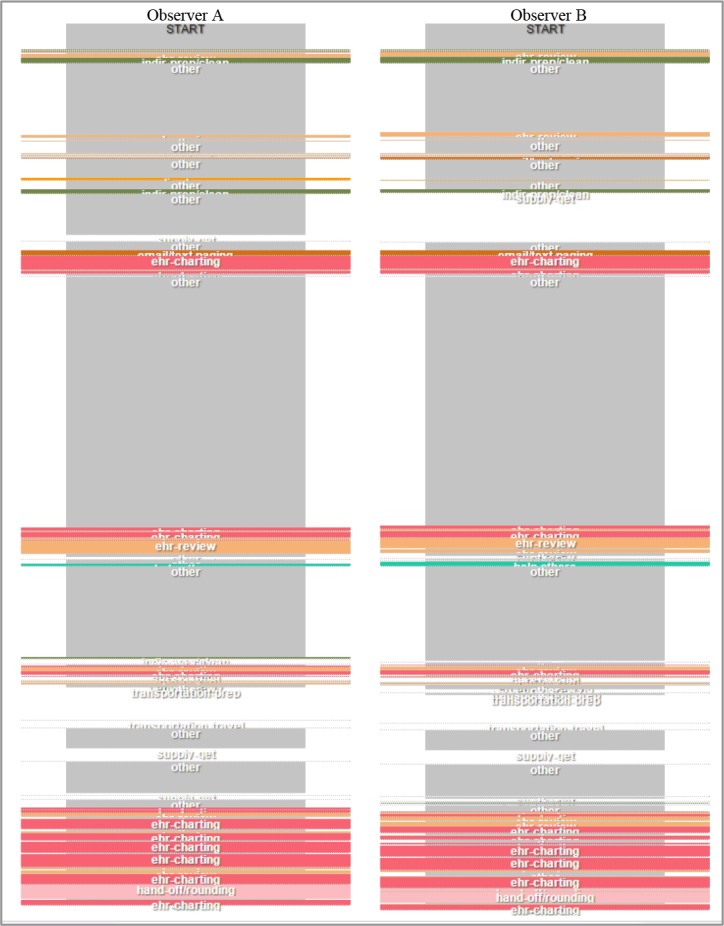
Side-by-Side IORA3 workflow visualization on hands-on tasks
Procedure
Student observers obtained informed consent from the observed nurse as well as permission from patients for observing their care. Each observation lasted for four hours over preset time periods: 7am to 11am, 11am to 3pm, or 3pm to 7pm, depending on availability arrangement. No identifiable information or health records were collected. The study was approved by the Institutional Review Board (IRB) at The Ohio State University.
Results
We completed a total of 56 hours (fourteen valid 4-hour observations) with 10 registered nurses, including eight observations from 11am to 3pm, five observations from 3pm to 7pm, and one observation from 7am to 11am. Among the 14 observations, three were on Monday, one on Tuesday, one on Wednesday, five on Thursday, and three on Friday.
Multi-tasking
In a 4-hour observation time block, nurses had 124 communications and 208 hands-on tasks on average. We considered that nurses were multitasking when they were engaged in communication and hands-on tasks simultaneously. We found that nurses were multitasking 131 times on average, which is 39.48% of all times; the total multitask duration ranges from 14.6 minutes to 109 minutes, 44.98 minutes (18.63%) on average. Multitasking duration seemed higher from 7am to 11am, but because we had only one observation during that time frame, we were not able to be conclusive.
Table 3 shows more details for each observation and the proportion of multitasking in frequency and duration (second). For example, Observation 1 occurred from 11am to 3pm, a 4-hour observation. During the observation, the nurse communicated 132 times with others and performed 171 hands-on tasks. The nurse multitasked (having communication and hands-on task simultaneously) 105 times, which is about 34.65% of all times. The duration of multitasks is 37.97 minutes, 15.76% of the total duration.
Table 3.
Observations
| ID | time | total duration (sec.) | Frequency | no. of multitasks | proportion | duration of multitasks (sec.) | proportion | |
|---|---|---|---|---|---|---|---|---|
| total no. of comm. | total no. of hands-on tasks | |||||||
| 1 | 11-3 | 14455 | 132 | 171 | 105 | 34.65% | 2278 | 15.76% |
| 2 | 3-7 | 14431 | 59 | 166 | 59 | 26.22% | 880 | 6.10% |
| 3 | 11-3 | 14459 | 108 | 261 | 125 | 33.88% | 1703 | 11.78% |
| 4 | 11-3 | 14433 | 156 | 248 | 199 | 49.26% | 3794 | 26.29% |
| 5 | 11-3 | 14374 | 78 | 161 | 51 | 21.34% | 1031 | 7.17% |
| 6 | 3-7 | 14659 | 170 | 248 | 194 | 46.41% | 3404 | 23.22% |
| 7 | 11-3 | 14372 | 154 | 164 | 111 | 34.91% | 2430 | 16.91% |
| 8 | 3-7 | 14678 | 140 | 231 | 131 | 35.31% | 2981 | 20.31% |
| 9 | 3-7 | 14461 | 167 | 247 | 144 | 34.78% | 2463 | 17.03% |
| 10 | 11-3 | 14581 | 109 | 212 | 152 | 47.35% | 3174 | 21.77% |
| 11 | 11-3 | 14413 | 149 | 189 | 153 | 45.27% | 4196 | 29.11% |
| 12 | 11-3 | 14409 | 102 | 227 | 126 | 38.30% | 1507 | 10.46% |
| 13 | 7-11 | 14733 | 161 | 240 | 228 | 56.86% | 6547 | 44.44% |
| 14 | 3-7 | 14413 | 54 | 152 | 60 | 29.13% | 1400 | 9.71% |
| Average | 14490.79 = 4.03 hours | 124.21 = 2.07 mins | 208.36 = 3.43 mins | 131.29 = 2.19 min | 39.48% | 2699.14 = 44.99 mins | 18.58% | |
| Total | 202871 = 56.35 hours | 1739 = 28.98 mins | 2917 = 48.62 mins | 1838 = 30.63 mins | 37788 = 629.8 mins | |||
Workflow visualization
We also examined workflow visualization (Figure 3) to explore the location of nursing activities occurred. We presented the workflow in three activity dimensions: communication, hands-on task, and location. We visualized these three activity dimensions across the continuum of time with colored bands representing different activities; the width of the band represents the duration of an activity. The activities on the three activity dimensions, and at the same horizontal position, represent multitasking. The workflow visualization can be interpreted as who the nurse was talking to, while doing what, and at what location. We found that nurses usually charted at the nursing station or on the hallway. They sometimes charted while they were traveling/walking to another destination. When they were reviewing or charting on the electronic health record, they were often talking to their patients or to other professions. Nurses usually called out when reviewing or charting, but could receive phone calls at anytime and anywhere. Task switching often occurred between related activities, such as reviewing and charting electronic health records, switching between direct patient care activities (e.g. procedure, vital sign, medication administration). Another example of related activities was calling out and electronic health record review. Calling out required looking up pager or phone numbers using the electronic health record, so these two activities were often closely linked.
Figure 3.

A Snapshot of nursing workflow visualization
Discussion
Self-created multitasking vs. unexpected interruption
During this pilot study, we observed that multitasking and task switching could be self-directed, such as consulting with other professions while reviewing patient records, talking to patients for assessment and documenting results simultaneously, charting while walking, and assessing patients while administering medications. Self-directed multitasking and task switching were considered being more efficient at work and are likely contributing to their job satisfaction.38 Conversely, we also observed unexpected multitasking or interruptions, such as receiving phone calls anytime and anywhere, or mini-conversations with others while preparing medications. Some interruptions are important as they could be reminders, alerts, or another higher priority task.39 However, interruptions also increase cognitive load,40 decrease the speed of information processing in human prefrontal cortex,41 and result in errors. While multitasking is necessary and an important skill in healthcare systems, it is important to assess and recognize its impact on patient care. For example, allowing patients direct contact with nurses, through the use of pagers, could increase patient satisfaction, but it may also increase unexpected interruptions. Such interruptions could potentially contribute to safety issues, particularly if nurses are performing critical procedures or preparing complex medication regimens.
Visualizing nursing workflow: communications, hands-on tasks, and locations of nursing activities
Currently, no model exists to evaluate multitasking. Multitasking could be self-directed or not, and could increase or decrease efficiency.42 To help explicate these workflow nuances, we used a workflow visualization method to understand the phenomena. We defined multitasking and task switching and designed the time motion study to capture observable nursing activities from three activity dimensions: communication, hands-on tasks, and location over the continuum of time. Using TimeCaT, we were able to analyze nursing workflow from the timing and frequency of the three activity dimensions and investigate the context and rationale via workflow visualization. Our study design and method provides a practical and reliable approach to conducting and analyzing time motion studies from both quantitative and qualitative perspectives.
Study limitations
Observing nurses in one unit in one hospital within one academic health system limits generalizability of our study. Data collection occurred over a two-month period which may introduce bias due to seasonal variations in hospital admissions. Participation bias was also a limitation, as nurses volunteered to participate in the study. Also, observations could be limited due to that humans may not be able to accurately record every action that is occurring, especially in a high stress clinical situation.43 We may have missed collection of data, particularly in rapidly changing hands-on tasks, communications or locations/movements of nurses. To minimize observational bias, all our observers were required to establish IORA before their observation data could be considered as valid thus also insuring study fidelity. We could not guarantee 100% accuracy, but we minimized the inconsistency between observers through rigorous training and clearly defining definitions of communications, hands-on tasks, and locations.
Future direction
In our study, we only recorded nursing activities that were observable. However, nurses often multitask and task switch in their thinking – critical thinking – which is unobservable. For example, nurses may juggle various needs of patients, family, and co-workers. Future research should investigate the impact of multitasking by assessing perceived workload at the end of observation to strengthen study findings. In addition, working within the complex healthcare environment of today, nurses must provide care that is efficient and effective. There is a growing body of literature that describes the workflow of nurses in an acute care environment.44–52 It has been found that nurses spend a considerable amount of non-value added time on activities that could potentially be delegated to other team members who could accomplish the care safely and with greater cost effectiveness. Inefficiencies in organizational systems also contribute to non-value added time.53,54 To date, there has been no empirical work that has aligned nursing practices and workflow or examined these practices relative to the notion of “top of licensure”. Top of license nursing practice addresses how nurses spend their time across the care continuum and examines “non-valued-added” work which could be executed safely by other healthcare personnel.53,54 As this is a pilot project under a larger nursing practice study, our ongoing and future research will explore top of license nursing activities and provide a strategic solution for providing higher quality and more efficient care.
Conclusion
We conducted a time motion study to capture communications, hands-on tasks, and locations of nursing activities. We also described our methodology in detail, and demonstrated a practical and reliable approach for other researchers. With the observational data, we were able to identify the amount of multitasking being carried out by nurses in their daily work, and provide a vivid pictures of nurses’ activities via a workflow visualization. Even though multitasking sometimes cannot be avoided, it has been noted that “Multitasking, a media-driven bias toward dramatic scenarios, and an emphasis on meeting institutional goals in the form of documentation have led to a culture of action-based practice, which interferes with nurses’ability to simply be with patients. In order for nurses to be fully present with their patients, the cultural norm of multitasking and the emphasis on doing must be reexamined within the context of patient care.”55 We plan to continue the time motion study with a larger sample of nurses to observe their workflows and activities, with the hope of providing a quantitative observational study with statistically rigorous evidences to describe the work of nurses. Future research also includes applying the approach and methodology to investigate the workflow change before and after the implementation of a new practice model or a new technology.
References
- 1.Zheng K, Haftel HM, Hirschl RB, O'Reilly M, Hanauer DA. Quantifying the impact of health IT implementations on clinical workflow: a new methodological perspective. J Am Med Inform Assoc. 2010;17(4):454–461. doi: 10.1136/jamia.2010.004440. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kalisch BJ, Aebersold M. Interruptions and multitasking in nursing care. Jt Comm J Qual Patient Saf. 2010;36(3):126–132. doi: 10.1016/s1553-7250(10)36021-1. [DOI] [PubMed] [Google Scholar]
- 3.Weaver SM, Arrington CM. The effect of hierarchical task representations on task selection in voluntary task switching. J Exp Psychol Learn Mem Cogn. 2013;39(4):1128–1141. doi: 10.1037/a0031677. [DOI] [PubMed] [Google Scholar]
- 4.Walter SR, Li L, Dunsmuir WT, Westbrook JI. Managing competing demands through task-switching and multitasking: a multi-setting observational study of 200 clinicians over 1000 hours. BMJ Qual Saf. 2014;23(3):231–241. doi: 10.1136/bmjqs-2013-002097. [DOI] [PubMed] [Google Scholar]
- 5.van Rensen EL, Groen ES, Numan SC, et al. Multitasking during patient handover in the recovery room. Anesth Analg. 2012;115(5):1183–1187. doi: 10.1213/ANE.0b013e31826996a2. [DOI] [PubMed] [Google Scholar]
- 6.Westbrook JI, Duffield C, Li L, Creswick NJ. How much time do nurses have for patients? A longitudinal study quantifying hospital nurses’ patterns of task time distribution and interactions with health professionals. BMC Health Serv Res. 2011;11:319. doi: 10.1186/1472-6963-11-319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Skaugset LM, Farrell S, Carney M, et al. Can You Multitask? Evidence and Limitations of Task Switching and Multitasking in Emergency Medicine. Ann Emerg Med. 2015 doi: 10.1016/j.annemergmed.2015.10.003. [DOI] [PubMed] [Google Scholar]
- 8.Janssen CP, Gould SJJ, Li SYW, Brumby DP, Cox AL. Integrating knowledge of multitasking and interruptions across different perspectives and research methods. Int. J. Hum.-Comput. Stud. 2015;79(C):1–5. [Google Scholar]
- 9.Walter SR, Dunsmuir WTM, Westbrook JI. Studying interruptions and multitasking in situ. Int. J. Hum.- Comput. Stud. 2015;79(C):118–125. [Google Scholar]
- 10.Lamar M, Craig M, Daly EM, et al. Acute tryptophan depletion promotes an anterior-to-posterior fMRI activation shift during task switching in older adults. Hum Brain Mapp. 2014;35(2):712–722. doi: 10.1002/hbm.22187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Orr JM, Banich MT. The neural mechanisms underlying internally and externally guided task selection. Neuroimage. 2014;84:191–205. doi: 10.1016/j.neuroimage.2013.08.047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Poljac E, Koch I, Bekkering H. Dissociating restart cost and mixing cost in task switching. Psychol Res. 2009;73(3):407–416. doi: 10.1007/s00426-008-0151-9. [DOI] [PubMed] [Google Scholar]
- 13.Rogers RD, Monsell S. Costs of a Predictable Switch between Simple Cognitive Tasks. J Exp Psychol Gen. 1995;124(2):207–231. [Google Scholar]
- 14.Rubinstein JS, Meyer DE, Evans JE. Executive control of cognitive processes in task switching. J Exp Psychol Human. 2001;27(4):763–797. doi: 10.1037//0096-1523.27.4.763. [DOI] [PubMed] [Google Scholar]
- 15.Monsell S. Task switching. Trends Cogn Sci. 2003;7(3):134–140. doi: 10.1016/s1364-6613(03)00028-7. [DOI] [PubMed] [Google Scholar]
- 16.Alavash M, Thiel CM, Giessing C. Dynamic coupling of complex brain networks and dual-task behavior. Neuroimage. 2016;129:233–246. doi: 10.1016/j.neuroimage.2016.01.028. [DOI] [PubMed] [Google Scholar]
- 17.Rodrigue M, Son J, Giesbrecht B, et al. Spatio-Temporal Detection of Divided Attention in Reading Applications Using EEG and Eye Tracking; Proceedings of the 20th International Conference on Intelligent User Interfaces; Atlanta, Georgia, USA. 2015. [Google Scholar]
- 18.Du JTN, Spink A. Toward a Web Search Model: Integrating Multitasking, Cognitive Coordination, and Cognitive Shifts. J Am Soc Inf Sci Tec. 2011;62(8):1446–1472. [Google Scholar]
- 19.Wendt M, Kiesel A, Mathew H, Luna-Rodriguez A, Jacobsen T. Irrelevant Stimulus Processing When Switching Between Tasks. Z Psychol. 2013;221(1):41–50. [Google Scholar]
- 20.Yin SH, Wang T, Pan WG, Liu YJ, Chen AT. Task-switching Cost and Intrinsic Functional Connectivity in the Human Brain: Toward Understanding Individual Differences in Cognitive Flexibility. Plos One. 2015;10(12) doi: 10.1371/journal.pone.0145826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Draheim C, Hicks KL, Engle RW. Combining Reaction Time and Accuracy: The Relationship Between Working Memory Capacity and Task Switching as a Case Example. Perspect Psychol Sci. 2016;11(1):133–155. doi: 10.1177/1745691615596990. [DOI] [PubMed] [Google Scholar]
- 22.Salvucci DD, Taatgen NA, Borst JP. Toward a Unified Theory of the Multitasking Continuum: From Concurrent Performance to Task Switching, Interruption, and Resumption. Chi2009; Proceedings of the 27th Annual Chi Conference on Human Factors in Computing Systems; 2009. pp. 1819–1828. [Google Scholar]
- 23.Lopetegui M, Yen PY, Lai A, Jeffries J, Embi P, Payne P. Time motion studies in healthcare: what are we talking about? J Biomed Inform. 2014;49:292–299. doi: 10.1016/j.jbi.2014.02.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Medicine NLo. MeSH: Time and Motion Studies. 1991. http://www.ncbi.nlm.nih.gov/mesh?term=Time+and+Motion+Studies.
- 25.Qian S, Yu P, Hailey D. Nursing staff work patterns in a residential aged care home: a time?motion study. Aust Health Rev. 2015. [DOI] [PubMed]
- 26.Tuinman A, de Greef MH, Krijnen WP, Nieweg RM, Roodbol PF. Examining Time Use of Dutch Nursing Staff in Long-Term Institutional Care: A Time-Motion Study. J Am Med Dir Assoc. 2016;17(2):148–154. doi: 10.1016/j.jamda.2015.09.002. [DOI] [PubMed] [Google Scholar]
- 27.Li L, Hains I, Hordern T, Milliss D, Raper R, Westbrook J. What do ICU doctors do? A multisite time and motion study of the clinical work patterns of registrars. Crit Care Resusc. 2015;17(3):159–166. [PubMed] [Google Scholar]
- 28.Cady RG, Finkelstein SM. Task-technology fit of video telehealth for nurses in an outpatient clinic setting. Telemed J E Health. 2014;20(7):633–639. doi: 10.1089/tmj.2013.0242. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Bastian ND, Munoz D, Ventura M. A Mixed-Methods Research Framework for Healthcare Process Improvement. J Pediatr Nurs. 2016;31(1):e39–51. doi: 10.1016/j.pedn.2015.09.003. [DOI] [PubMed] [Google Scholar]
- 30.Edwards A, Fitzpatrick LA, Augustine S, et al. Synchronous communication facilitates interruptive workflow for attending physicians and nurses in clinical settings. Int J Med Inform. 2009;78(9):629–637. doi: 10.1016/j.ijmedinf.2009.04.006. [DOI] [PubMed] [Google Scholar]
- 31.Spencer R, Coiera E, Logan P. Variation in communication loads on clinical staff in the emergency department. Ann Emerg Med. 2004;44(3):268–273. doi: 10.1016/j.annemergmed.2004.04.006. [DOI] [PubMed] [Google Scholar]
- 32.Berg LM, Kallberg AS, Goransson KE, Ostergren J, Florin J, Ehrenberg A. Interruptions in emergency department work: an observational and interview study. BMJ Qual Saf. 2013;22(8):656–663. doi: 10.1136/bmjqs-2013-001967. [DOI] [PubMed] [Google Scholar]
- 33.Westbrook JI, Ampt A, Williamson M, Nguyen K, Kearney L. Methods for measuring the impact of health information technologies on clinicians’ patterns of work and communication. Stud Health Technol Inform. 2007;129(Pt 2):1083–1087. [PubMed] [Google Scholar]
- 34.Zheng K, Guo MH, Hanauer DA. Using the time and motion method to study clinical work processes and workflow: methodological inconsistencies and a call for standardized research. J Am Med Inform Assoc. 2011;18(5):704–710. doi: 10.1136/amiajnl-2011-000083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Lopetegui M, Yen PY, Lai AM, Embi PJ, Payne PR. Time Capture Tool (TimeCaT): development of a comprehensive application to support data capture for Time Motion Studies. AMIA Annu Symp Proc. 2012;201(2):596–605. [PMC free article] [PubMed] [Google Scholar]
- 36.TimeCaT: Time Capture Tool. 2015. Apr 30th, timecat.org.
- 37.Lopetegui MA, Bai S, Yen PY, Lai A, Embi P, Payne PR. Inter-observer reliability assessments in time motion studies: the foundation for meaningful clinical workflow analysis; AMIA Annu Symp Proc; 2013. pp. 889–896. [PMC free article] [PubMed] [Google Scholar]
- 38.Forsberg HH, Muntlin Athlin A, von Thiele Schwarz U. Nurses’ perceptions of multitasking in the emergency department: effective, fun and unproblematic (at least for me) - a qualitative study. Int Emerg Nurs. 2015;23(2):59–64. doi: 10.1016/j.ienj.2014.05.002. [DOI] [PubMed] [Google Scholar]
- 39.Hall LM, Ferguson-Pare M, Peter E, et al. Going blank: factors contributing to interruptions to nurses’ work and related outcomes. J Nurs Manag. 2010;18(8):1040–1047. doi: 10.1111/j.1365-2834.2010.01166.x. [DOI] [PubMed] [Google Scholar]
- 40.Coiera EW, Jayasuriya RA, Hardy J, Bannan A, Thorpe ME. Communication loads on clinical staff in the emergency department. Med J Aust. 2002;176(9):415–418. doi: 10.5694/j.1326-5377.2002.tb04482.x. [DOI] [PubMed] [Google Scholar]
- 41.Dux PE, Tombu MN, Harrison S, Rogers BP, Tong F, Marois R. Training improves multitasking performance by increasing the speed of information processing in human prefrontal cortex. Neuron. 2009;63(1):127–138. doi: 10.1016/j.neuron.2009.06.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Alkahtani M, Aziz T, Ahmad A, Darmoul S. Multitasking in Healthcare Systems. Paper presented at: The 2015 Industrial and Systems Engineering Research Conference 2015; Tenessee; USA. [Google Scholar]
- 43.Vankipuram M, Kahol K, Cohen T, Patel VL. Toward automated workflow analysis and visualization in clinical environments. J Biomed Inform. 2011;44(3):432–440. doi: 10.1016/j.jbi.2010.05.015. [DOI] [PubMed] [Google Scholar]
- 44.Benner P, Sheets V, Uris P, Malloch K, Schwed K, Jamison D. Individual, practice, and system causes of errors in nursing: a taxonomy. J Nurs Adm. 2002;32(10):509–523. doi: 10.1097/00005110-200210000-00006. [DOI] [PubMed] [Google Scholar]
- 45.Clarke SP, Aiken LH. Failure to rescue. Am J Nurs. 2003;103(1):42–47. doi: 10.1097/00000446-200301000-00020. [DOI] [PubMed] [Google Scholar]
- 46.Ebright PR, Patterson ES, Chalko BA, Render ML. Understanding the complexity of registered nurse work in acute care settings. J Nurs Adm. 2003;33(12):630–638. doi: 10.1097/00005110-200312000-00004. [DOI] [PubMed] [Google Scholar]
- 47.Higuchi KA, Donald JG. Thinking processes used by nurses in clinical decision making. J Nurs Educ. 2002;41(4):145–153. doi: 10.3928/0148-4834-20020401-04. [DOI] [PubMed] [Google Scholar]
- 48.Potter P, Wolf L, Boxerman S, et al. An Analysis of Nurses’ Cognitive Work: A New Perspective for Understanding Medical Errors Advances in Patient Safety: From Research to Implementation (Volume 1: Research Findings); Rockville MD; 2005. [PubMed] [Google Scholar]
- 49.Wolf LD, Potter P, Sledge JA, Boxerman SB, Grayson D, Evanoff B. Describing nurses’ work: combining quantitative and qualitative analysis. Hum Factors. 2006;48(1):5–14. doi: 10.1518/001872006776412289. [DOI] [PubMed] [Google Scholar]
- 50.Tang Z, Mazabob J, Weavind L, Thomas E, Johnson TR. A time-motion study of registered nurses’ workflow in intensive care unit remote monitoring; AMIA Annu Symp Proc; 2006. pp. 759–763. [PMC free article] [PubMed] [Google Scholar]
- 51.Capuano T, Bokovoy J, Halkins D, Hitchings K. Work flow analysis: eliminating non-value-added work. J Nurs Adm. 2004;34(5):246–256. doi: 10.1097/00005110-200405000-00008. [DOI] [PubMed] [Google Scholar]
- 52.Blay N, Duffield CM, Gallagher R, Roche M. A systematic review of time studies to assess the impact of patient transfers on nurse workload. Int J Nurs Pract. 2014;20(6):662–673. doi: 10.1111/ijn.12290. [DOI] [PubMed] [Google Scholar]
- 53.Storfjell JL, Ohlson S, Omoike O, Fitzpatrick T, Wetasin K. Non-value-added time: the million dollar nursing opportunity. J Nurs Adm. 2009;39(1):38–45. doi: 10.1097/NNA.0b013e31818e9cd4. [DOI] [PubMed] [Google Scholar]
- 54.Storfjell JL, Omoike O, Ohlson S. The balancing act: patient care time versus cost. J Nurs Adm. 2008;38(5):244–249. doi: 10.1097/01.NNA.0000312771.96610.df. [DOI] [PubMed] [Google Scholar]
- 55.de Ruiter HP, Demma JM. Nursing: the skill and art of being in a society of multitasking. Creat Nurs. 2011;17(1):25–29. doi: 10.1891/1078-4535.17.1.25. [DOI] [PubMed] [Google Scholar]