

Abstract
Introduction
Solid facial edema (SFE) is a rare complication of acne vulgaris. To examine the clinical features of acne patients with solid facial edema, and to give an overview on the outcome of previous topical and systemic treatments in the cases so far published.
Methods
We report two cases from Switzerland, both young men with initially papulopustular acne resistant to topical retinoids.
Results
Both cases responded to oral isotretinoin, in one case combined with oral steroids. Our cases show a strikingly similar clinical appearance to the cases described by Connelly and Winkelmann in 1985 (Connelly MG, Winkelmann RK. Solid facial edema as a complication of acne vulgaris. Arch Dermatol. 1985;121(1):87), as well as to cases of Morbihan’s disease that occurs as a rare complication of rosacea.
Conclusion
Even 30 years after, the cause of the edema remains unknown. In two of the original four cases, a potential triggering factor was identified such as facial trauma or insect bites; however, our two patients did not report such occurrencies. The rare cases of solid facial edema in both acne and rosacea might hold the key to understanding the specific inflammatory pattern that creates both persisting inflammation and disturbed fluid homeostasis which can occur as a slightly different presentation in dermatomyositis, angioedema, Heerfordt’s syndrome and other conditions.
Keywords: Adrenergic receptors, Brimonidine, Erythema, Rosacea, Vasoconstriction, Worsening of erythema
Introduction
Acne vulgaris is a disorder of the pilosebaceous unit, namely the sebaceous gland and the hair follicle it is attached to. Some 85% of people have acne at some point in their life, especially during puberty [1], and therefore it could be considered the most common inflammatory skin disease. Due to disfiguration and scarring, the disease has major effects on the patient’s quality of life [2], eliciting depression, social withdrawal, anxiety and a higher rate of unemployment [3, 4].
The pathogenesis includes several components whose interplay is only partially known. The androgen surge in puberty stimulates the sebocytes and follicular keratinocytes that proliferate and obstruct the outflow tract of the hair follicle. This leads to a hyperplasia of the sebaceous glands and the seborrhea that is characteristic for acne. Propionibacterium acnes, an opportunistic grampositive anaerobic strain found in the seborrheic areas of the skin, breaks down fatty acids. These compounds are believed to elicit inflammation and chemotaxis of neutrophil granulocytes and adaptive immune cells to the follicular epithelium. This ends in the rupture and release of sebum, microorganisms and keratin into the dermis. Accumulation of neutrophils, lymphocytes and foreign-body giant cells leads to the characteristic erythematous papules, pustules, nodules and cysts of inflammatory acne [1, 5].
In very rare cases, however, the primary acne lesions occur together with a wooden, solid facial edema (SFE). Typically, the acne lesions are moderate to severe but in no way extreme, hence this phenomenon cannot be explained by simple edema due to inflammation. It was first observed and published by Connelly and Winkelmann in 1985 [6]. Although we believe we have understood more about acne pathogenesis since then, solid facial edema remains a mystery. It has been suggested that chronic inflammation, comparable to other body regions such as the legs, damages the lymphatic system and leads to fibrosis, which is further supported by mast cells. Accordingly, early treatment before damage is irreversible seems sensible. Here, we report two Swiss cases of SFE in acne vulgaris and summarize the clinical features and treatment responses of SFE cases in the literature.
Case Report
A 18-year old carpenter presented with numerous papules and pustules on the forehead and cheeks compatible with acne. Initially, he had been fruitlessly treated with topical retinoids. Instead, after 6 months of therapy, the patient developed a localized, symmetric, wooden, non-pitting edema over the cheeks and infraorbital regions, the lower front and glabella. All edematous areas were beset with multiple comedones and papulopustules (Fig. 1). A punch biopsy revealed some dermal edema and fibrosis as well as moderate infiltrates composed of lymphocytes and neutrophils granulocytes around the pilo-sebaceous unit (Fig. 2). Treatment with 2 mg/kg oral prednisone for 12 days in combination with 20 mg isotretinoin for 2 months resulted in a complete regression of the edema.
Fig. 1.
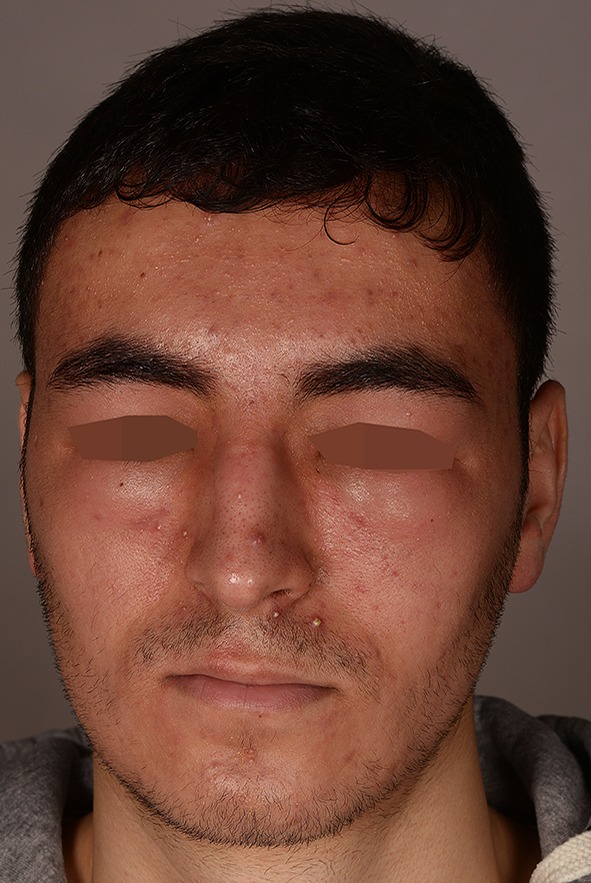
Diffuse papules and pustules with facial wooden edema in the periorbital area
Fig. 2.

Biopsy of case 1 revealing dermal edema and fibrosis as well as mixed cellular infiltrate around the pilo-sebaceous unit
The second case was an otherwise healthy 20-year-old student, who consulted for a persisting edematous reaction of the left upper and lower eyelid and cheek that had developed 5 months earlier. It had started during treatment with topical retinoids for erythematous papules and pustules interpreted as acne vulgaris that had arisen on the forehead, cheeks, chin and pre-sternal area. Shortly after commencing the treatment, the indurated edema developed. No comedones nor teleangiectasias were present. A biopsy showed a spongiotic dermatitis, probably due to local treatment, as well as acne of a typical mixed cellular and mixed perifollicular inflammation. Further, fibrosis in the middle and dermis was quite prominent. After 8 months treatment with isotretinoin 20 mg per day and an antihistamine, the facial edema slowly cleared.
Compliance with Ethics Guidelines
Informed consent was obtained from the patients prior to publication.
Discussion
A total of 20 similar cases have been reported so far in the medical literature (Table 1). Multiple strategies were used in attempts to treat the edema. The first therapy attempt, with elastic facial stockings for several months as reported by Connelly and Winkelmann, failed [6]. In 8 cases, 0.5–1 mg/kg per day isotretinoin was reported as an effective treatment of the facial edema in acne vulgaris [7–10]. There were two reported cases of treatment failure after 3 and 4 months of therapy with isotretinoin, which corresponds with our experience, as in the second case, we observed improvement only after 8 months of treatment [11, 12]. Therapy attempts with oral prednisone alone showed no improvement of the facial edema, in contrast to successes by a combination with isotretinoin [13]. Surgical therapy after failure of conventional treatment, as reported in one case, led to complete resolution [14]. It remains unknown whether the result was aesthetically satisfying. In the related condition called Morbihan disease, isotretinoin monotherapy and combination therapies of isotretinoin with either ketotifen or clofazimine all produced good results [12, 15].
Table 1.
Cases of SFE reported in the literature
| Case No. | Location | Age (years) | Sex | History of acne | Acne lesions | Trigger of edema | Delay until presentation (years) | Treatment | Success | References |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Face | 20 | M | For 8 years | Papulopustules, nodules, hemorrhagic crusts, comedones and atrophic scars confined to the face | Unknown | 2 | 4 months of isotretinoin (0.5 mg/kg/day) and 4 months of ketotifen (2 mg/day) | Complete resolution | [10] |
| 2 | Face | 18 | M | For 6 months | Papules and pustules on the forehead and cheeks | Topical retinoids | 0.1825 | Oral prednisone 2 mg/kg/day for 12 days in combination with isotretinoin 20 mg for 2 months | Complete resolution | This report |
| 3 | Face | 20 | M | For 8 months | Papules and pustules on the forehead, cheeks and chin | Topical retinoids | 0.125 | 8 months treatment with isotretinoin 20 mg/day and antihistamine | Complete resolution | This report |
| 4 | Face | 65 | M | Acne as a child and “cysts all his life” | Facial biopsy compatible with sebaceous hyperplasia and rosacea | Unknown | 4 | Surgery (debulking of the affected tissue) after failure of conventional treatment | Complete resolution | [14] |
| 5 | Face | 20 | M | For 3 years, no treatment | Moderate juvenile polymorphic acne | Unknown | 2 | 8 months of isotretinoin 1 mg/kg/day | 50% reduction | [7] |
| 6 | Face | 15 | F | Unknown | Nodular pustules in the right nasolabial fold | Unknown | 1 | 6 months of isotretinoin 1 mg/kg/day | 80% reduction | [7] |
| 7 | Face | 17 | M | Moderate papulocystic acne for 3 years | Facial lesions consisting of inflammatory papules and scattered pustules and cysts | Unknown | 1 | 20 weeks of isotretinoin (40 mg/twice a day = 1.0 mg/kg/day) | Moderate reduction | [9] |
| 8 | Face | 20 | F | Acne vulgaris for 4 years | Unknown | Unknown | 0.33 | 20 weeks of isotretinoin (30 mg/day) and clofazimine (100 mg four times a week), manual lymph drainage once a week for 15 times | Moderate reduction | [8] |
| 9 | Face | 18 | M | Acne for 4 years | Numerous inflammatory acne lesions | Unknown | 0.75 | Isotretinoin (50 mg/day for 12 weeks, 40 mg/day for 12 weeks), manual lymph drainage for two weeks | Moderate reduction | [8] |
| 10 | Face | 21 | W | Nodulocystic acne for 5 years | Erythematous, solid, edematous plaques and firm, deep-seated nodules on the cheeks and forehead | Unknown | NA | Injections of hot water into the indurated areas, typhoid fever therapy and X-ray treatment | Moderate reduction | [6] |
| 11 | Face | 18 | M | Papulopustular acne vulgaris | Unknown | Unknown | NA | Systemic steroid therapy | Moderate reduction | [20] |
| 12 | Mid-face | 24 | M | For 10 years | Erythematous papules with few pustules across the cheeks and nose | Unknown | 1.5 | 3 months of isotretinoin 1 mg/kg/day and 1 month of prednisone | No | [21] |
| 13 | Face | 25 | M | For 11 years | Multiple pitting scars on the whole face but no inflammatory acne lesions | Unknown | 4 | 2 months of oral tetracyclines 500 mg and 4 months isotretinoin (40 mg/day = 0.5 mg/kg) | No | [11] |
| 14 | Face | 18 | M | Papulopustular acne for 3 years | Excoriated papular acne lesions on the forehead and upper part of the back | Unknown | 0.75 | 15 months of elastic facial stockings | No | [6] |
| 15 | Face | 20 | M | For 3 years | Papular acne on the chin, acne scarring on the forehead | Motor vehicle accident | 2 | 15 months of elastic facial stockings | No | [6] |
| 16 | Face | 20 | M | For 2 years | Papulopustular acne on the forehead | Gnat bite | 0.5 | 6 weeks of oral corticosteroids | No | [6] |
| 17/18 | Face | 14 | M | For 1 year | Severe papulopustular acne, primarily involving the face, associated with pronounced centrofacial edema | Unknown | 0.25 | Betamethasone 1.5 mg/day, stopped after 2 weeks due to inefficacy. Oral and topical antibiotics | Persistence of edema, resolution of acne | [22] |
| 19 | Face | 18 | M | Unknown | Intense papulopustular acne without scarring and seborrheic dermatitis | Unknown | NA | Prednisone (20 mg/day) | Unknown | [13] |
| 20 | Face | 17 | M | Unknown | Seborrheic dermatitis and papulopustular acne | Unknown | 2 | Prednisone (15 mg/day) | Unknown | [13] |
These two cases illustrate this typical, almost unmistakable, disease of solid facial edema which produces a striking facies. This condition does not stand alone—clinically closely comparable to the initial report of Connelly and Winkelmann [6], quite similar reports of SFE as a rare complication of rosacea (Morbihan disease) were published in 1957 [15]. Morbihan disease also produces solid facial edema with histopathologic features of granulomatous rosacea that can occur at any stage of the disease [15]. The pathogenesis of Morbihan disease also remains unclear [15, 16], the two main hypotheses being lymph vessel abnormalities or the edema representing an inflammatory effect [12, 15]. This peculiar edema is not reduced when standing, nor does it show variation during the day. Interestingly, a number of other facial dermatoses can produce similar effects, including dermatomyositis, angiedema, Melkersson–Rosenthal and Heerfordt’s syndrome [17–19].
We believe a common inflammatory pattern may be underlying all these conditions. A number of mediators are directly involved in induction of edema, including bradykinin, interleukin 1 beta, histamine and others. These are produced by cells both of the innate (mast cells, granulocytes, monocytes/macrophages) as well as of the adaptive immune system (T cells). We have therefore undertaken comparative studies that are currently ongoing. Once the pathogenesis of persisting edema is better understood, more targeted and effective therapies might be within our reach.
Acknowledgements
No funding or sponsorship was received for this study or publication of this article. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval for the version to be published.
Disclosures
Sarah Kuhn-Régnier, Joanna Mangana, Katrin Kerl, Jivko Kamarachev, Lars E. French, Antonio Cozzio and Alexander A. Navarini have nothing to disclose.
Compliance with Ethics Guidelines
Informed consent was obtained from the patients prior to publication.
Data Availability
All data generated or analyzed during this study are included in this published.
Open Access
This article is distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 International License (http://creativecommons.org/licenses/by-nc/4.0/), which permits any noncommercial use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
Footnotes
Enhanced content
To view enhanced content for this article go to http://www.medengine.com/Redeem/B687F0603931CB7A.
References
- 1.James WD. Clinical practice. Acne. N Engl J Med. 2005;352(14):1463–1472. doi: 10.1056/NEJMcp033487. [DOI] [PubMed] [Google Scholar]
- 2.Al-Shidhani A, Al-Rashdi S, Al-Habsi H, Rizvi S. Impact of acne on quality of life of students at Sultan Qaboos University. Oman Med J. 2015;30(1):42–47. doi: 10.5001/omj.2015.08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Koo J. The psychosocial impact of acne: patients’ perceptions. J Am Acad Dermatol. 1995;32(5):S26–S30. doi: 10.1016/0190-9622(95)90417-4. [DOI] [PubMed] [Google Scholar]
- 4.Cunliffe WJ. Acne and unemployment. Br J Dermatol. 1986;115(3):386. doi: 10.1111/j.1365-2133.1986.tb05757.x. [DOI] [PubMed] [Google Scholar]
- 5.Ramanathan S, Hebert AA. Management of acne vulgaris. J Pediatr Health Care. 2011;25(5):332–337. doi: 10.1016/j.pedhc.2011.05.007. [DOI] [PubMed] [Google Scholar]
- 6.Connelly MG, Winkelmann RK. Solid facial edema as a complication of acne vulgaris. Arch Dermatol. 1985;121(1):87. doi: 10.1001/archderm.1985.01660010091026. [DOI] [PubMed] [Google Scholar]
- 7.Humbert P, Delaporte E, Drobacheff C, Piette F, Blanc D, Bergoend H, et al. Solid facial edema associated with acne. Therapeutic efficacy of isotretinoin. Ann Dermatol Venereol. 1990;117(8):527–532. [PubMed] [Google Scholar]
- 8.Helander I, Aho HJ. Solid facial edema as a complication of acne vulgaris: treatment with isotretinoin and clofazimine. Acta Derm Venereol. 1987;67(6):535–537. [PubMed] [Google Scholar]
- 9.Friedman SJ, Fox BJ, Albert HL. Solid facial edema as a complication of acne vulgaris: treatment with isotretinoin. J Am Acad Dermatol. 1986;15(2):286–289. doi: 10.1016/S0190-9622(86)70168-0. [DOI] [PubMed] [Google Scholar]
- 10.Jungfer B, Jansen T, Przybilla B, Plewig G. Solid persistent facial edema of acne: successful treatment with isotretinoin and ketotifen. Dermatology. 1993;187(1):34–37. doi: 10.1159/000247194. [DOI] [PubMed] [Google Scholar]
- 11.Kilinc I, Gencoglan G, Inanir I, Dereli T. Solid facial edema of acne: failure of treatment with isotretinoin. Eur J Dermatol. 2003;13(5):503–504. [PubMed] [Google Scholar]
- 12.Veraldi S, Francia C, Persico M. Morbihan syndrome. Indian Dermatol Online J. 2013;4(2):122. doi: 10.4103/2229-5178.110639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Camacho-Martinez F, Winkelmann RK. Solid facial edema as a manifestation of acne. J Am Acad Dermatol. 1990;22(1):129–130. doi: 10.1016/S0190-9622(08)80014-X. [DOI] [PubMed] [Google Scholar]
- 14.Méndez-Fernández MA. Surgical treatment of solid facial edema. Ann Plastic Surg. 1997;39(6):620–623. doi: 10.1097/00000637-199712000-00011. [DOI] [PubMed] [Google Scholar]
- 15.Hu SW, Robinson M, Meehan SA, Cohen DE. Morbihan disease. Dermatol Online J. 2012;18(12):27. [PubMed] [Google Scholar]
- 16.Wohlrab J, Lueftl M, Marsch WC. Persistent erythema and edema of the midthird and upper aspect of the face (morbus morbihan): evidence of hidden immunologic contact urticaria and impaired lymphatic drainage. J Am Acad Dermatol. 2005;52(4):595–602. doi: 10.1016/j.jaad.2004.08.061. [DOI] [PubMed] [Google Scholar]
- 17.Powell RJ, Leech SC, Till S, Huber PAJ, Nasser SM, Clark AT. BSACI guideline for the management of chronic urticaria and angioedema. Clin Exp Allergy. 2015;45(3):547–565. doi: 10.1111/cea.12494. [DOI] [PubMed] [Google Scholar]
- 18.Chappity P, Kumar R, Sahoo AK. Heerfordt’s syndrome presenting with recurrent facial nerve palsy: case report and 10-year literature review. Sultan Qaboos Univ Med J. 2015;15(1):e124–e128. [PMC free article] [PubMed] [Google Scholar]
- 19.Findlay AR, Goyal NA, Mozaffar T. An overview of polymyositis and dermatomyositis. Muscle Nerve. 2015;51(5):638–656. doi: 10.1002/mus.24566. [DOI] [PubMed] [Google Scholar]
- 20.Mahajan PM. Solid facial edema as a complication of acne vulgaris. Cutis. 1998;61(4):215–216. [PubMed] [Google Scholar]
- 21.Patel AB, Harting MS, Hsu S. Solid facial edema: treatment failure with oral isotretinoin monotherapy and combination oral isotretinoin and oral steroid therapy. Dermatol Online J. 2008;14(1):14. [PubMed] [Google Scholar]
- 22.Tosti A, Guerra L, Bettoli V, Bonelli U. Solid facial edema as a complication of acne vulgaris in twins. J Am Acad Dermatol. 1987;17(5 Pt 1):843–844. doi: 10.1016/S0190-9622(87)80281-5. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
All data generated or analyzed during this study are included in this published.