

Abstract
Objective:
Ischemia-modified albumin (IMA) is a sensitive biomarker of myocardial ischemia. However, data on IMA levels in acute heart failure (HF) are still lacking. In this study, we aimed to evaluate serum IMA levels in acute decompensated HF and the effects of dobutamine and levosimendan treatments on IMA levels.
Methods:
This was a prospective, multicenter study that included 70 patients hospitalized with acute decompensated HF and left ventricular ejection fraction <35%. Blood samples for IMA measurements were obtained on admission and 24-48 h after the initiation of HF therapy. Twenty-nine patients were treated with standard HF therapy, 18 received levosimendan, and 23 received dobutamine in addition to standard of care. A single serum specimen was also collected from 32 healthy individuals each. IMA concentrations were measured by the albumin cobalt binding colorimetric assay, and the results were given in absorbance units (AU). Independent and paired sample t-tests, Mann-Whitney U test, and Wilcoxon signed-rank test were used for the analysis.
Results:
In patients with acute decompensated HF, the serum concentration of IMA was significantly higher than those of healthy subjects (0.894±0.23 AU vs. 0.379±0.08 AU, p<0.001). Overall, the IMA levels significantly decreased after 24-48 h of HF therapy (0.894±0.23 AU and 0.832±0.18 AU, p=0.013). Furthermore, the IMA levels were also found to significantly decrease with standard HF therapy (1.041±0.28 vs. 0.884±0.15 AU, p=0.041), with levosimendan (0.771±0.18 vs. 0.728±0.18 AU, p=0.046) and also with dobutamine (0.892±0.18 vs. 0.820±0.13 AU, p=0.035).
Conclusion:
Patients with acute decompensated HF had elevated IMA levels, and appropriate HF therapy significantly reduced the serum IMA levels. Dobutamine or levosimendan did not increase the IMA levels, suggesting a lower potential in inducing myocardial ischemia when used in recommended doses.
Keywords: ischemia modified albumin, heart failure, acute
Introduction
Ischemia-modified albumin (IMA) is a highly sensitive biomarker of transient myocardial ischemia, arising before the development of myocardial necrosis; therefore, it is referred to as an early marker of ischemia rather than myocardial cell damage (1-5). It has been widely studied in the assessment of patients presenting with suspected acute coronary syndrome (ACS). IMA has also been found to be elevated in the setting of oxidative stress, acidosis, hypoxia, inflammatory state, and sodium and calcium pump disruptions (5-9). These conditions are also involved in the pathophysiological process of heart failure (HF). In several studies, reactive oxygen species have been shown to be produced in the failing myocardium and oxidative stress has been demonstrated to be implicated in the pathogenesis of HF (6-8). However, data about IMA levels specifically in patients with acute HF are still lacking.
The most widely used inotropic agent dobutamine has been reported to increase myocardial oxygen consumption and oxidative stress, and therefore, it may lead to precipitate ischemia and cause myocardial cell damage as has been shown in animal models (10, 11). In contrast to dobutamine, levosimendan has been shown not to increase myocardial oxygen consumption and oxidative stress and is therefore presumed to have cardioprotective properties (12, 13). However, it is not clear whether dobutamine induces myocardial ischemia when used in clinically recommended dosages and whether levosimendan shows a better profile over dobutamine in terms of inducible ischemia or oxidative stress. IMA appears to be an ideal biomarker to evaluate inducible myocardial ischemia or oxidative stress.
The aim of this study was to evaluate the serum IMA levels in patients admitted to a hospital with the diagnosis of acute decompensated HF, serial changes in the IMA concentrations in response to appropriate HF therapy during hospital stay, and the effects of dobutamine and levosimendan on serum IMA levels.
Methods
Study population
Seventy patients, aged 18 years or older, were admitted to participating centers (Eskişehir Osmangazi University, Cardiology Department, Eskişehir, Turkey; Ufuk University, Cardiology Department, Ankara, Turkey; Kilis State Hospital, Cardiology Clinic, Kilis, Turkey; Türkiye Yüksek İhtisas Hospital, Cardiology Clinic, Ankara, Turkey; and Cumhuriyet University, Cardiology Department, Sivas, Turkey) and hospitalized with the diagnosis of acutely decompensated HF defined as a rapid onset or progressive deterioration in the symptoms and signs of congestion and/or low cardiac output (e.g., increasing breathlessness, orthopnea, jugular venous distension, peripheral edema, weight gain, pulmonary crepitations, tachycardia, cold extremities, and hypotension), which were considered to be due to a precipitant or trigger (e.g., an arrhythmia, discontinuation of diuretic treatment, non-adherence to diet/drug therapy, and uncontrolled hypertension), New York Heart Association functional class III-IV, and left ventricular ejection fraction (LVEF) <35% as measured by transthoracic echocardiography were included in this multicenter study. ACS defined by progressive angina or chest pain at rest or new ECG changes and/or serial increase in cardiac troponin levels, recent percutaneous coronary interventions (PCI), cardiogenic shock, hypertrophic cardiomyopathy, severe valvular heart disease, severe renal failure, chronic obstructive pulmonary disease, pregnancy, hypo/hyperthyroidism, recent infection history, and abnormal albumin levels (<3.5 g/dL and >5.5 g/dL) were the exclusion criteria. A single serum specimen was also collected from aged-matched 32 apparently healthy individuals (mean age 68±7 years, 20 males and 12 female) as a control reference population. The control group must also have met the exclusion criteria and was similar with the main study population in terms of age (68±7 vs. 66±10 years, p=0.302), gender (62.5% vs. 70% males, p=0.370), and serum albumin levels (4.0±0.2 mg/dL vs. 3.8±0.6 mg/dL, p=0.270).
Study design and protocol
The present study was a multicenter, prospective study conducted in the cardiology department of five hospitals from four different cities (14). The study protocol was approved by the institutional Ethics Committee, and the study was performed in accordance with the guidelines of the Declaration of Helsinki. All patients gave written informed consent before enrollment.
After hospital admission, all patients were treated with guidelines-recommended medical therapy for acute HF including oxygen, intravenous diuretic, and vasodilator therapy on top of their background oral medication such as angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, beta-blockers, or mineralocorticoid receptor antagonists. The patients’ background therapy, including beta-blockers, was continued during the hospital stay if tolerated. Digoxin was used for rate control in the presence of atrial fibrillation. In addition, patients who did not respond to optimal pharmacological therapy as evidenced by persistent dyspnea or congestion, those with clinical evidence of organ hypoperfusion such as worsening renal or liver functions as evidenced by oliguria, increase in creatinine and liver transaminase levels, and evidence of elevated cardiac filling pressures received inotropic therapy. The decision of inotropic support and type of inotropic agent was left at the discretion of the physician. Among all patients, 29 were treated with standard HF therapy with oxygen, diuretics, vasodilators (standard therapy group); 18 received an additional 24 h infusion of levosimendan with a loading dose of 6-12 pg/kg over 10 min followed by a continuous infusion of 0.1-0.2 pg/kg/min (levosimendan group), and 23 received dobutamine with a continuous infusion of 5-10 pg/kg/min for 24 h in addition to the standard HF therapy (dobutamine group).
The serum concentrations of IMA were measured from blood samples collected after diagnosis and before the initiation of HF therapy, and additionally, a second specimen was collected after 24-48 h of the initiation of HF therapy. Baseline demographic data and medications were documented in all subjects (Table 1). N-terminal pro-brain natriuretic peptide (NT-proBNP), hemoglobin, serum potassium, sodium, creatinine, blood urea nitrogen (BUN), albumin, and cardiac troponin-I (cTnI) levels were measured during admission and after 24-48 h of the initiation of HF therapy. Also, LVEF and systolic pulmonary arterial pressure (sPAP) were obtained from transthoracic echocardiography. In addition to the IMA levels, changes in other laboratory variables were also analyzed.
Table 1.
Patient demographics on admission
| Study population (n=70) | |
|---|---|
| Age, years | 66±10 |
| Male gender, n | 49 (70%) |
| Diabetes, n | 28 (40%) |
| Hypertension, n | 52 (74%) |
| Hyperlipidemia, n | 40 (57%) |
| Smoker, n | 22 (31%) |
| Ischemic heart failure, n | 62 (88%) |
| Medication | |
| ACEI/ARB, n | 52 (74%) |
| Beta blocker, n | 49 (70%) |
| MRA, n | 29 (42%) |
| Diuretic, n | 39 (56%) |
| Digoxin, n | 26 (37%) |
ACEI - angiotensin converting enzyme inhibitor; ARB - angiotensin receptor blocker; MRA - mineralocorticoid receptor antagonist
IMA measurement
Blood samples for the measurement of the IMA level were centrifuged within 1 h of collection for 15 min at 3000 rpm. The serum specimens were frozen at -70°C on site before being sent for central lab analysis to determine the IMA concentration. The IMA concentrations were measured by the albumin cobalt binding colorimetric assay by the addition of a known amount of cobalt to the serum specimen and by further measurement of the unbound cobalt by colorimetric assay using dithiothreitol, as previously described by Bar-Or et al. (15) The analysis in the Human Humalyzer 2000 spectrophotometer (Human Diagnostics, Weisbaden, Germany) were performed at 470 nm, and the results were given in absorbance units (AU).
Statistical analysis
The statistical analysis was performed using the Statistical Package for Social Sciences software 20.0 (IBM SPSS 20, SPSS Inc, Chicago, USA), Medcalc 11.3.0 (MedCalc 11.3-MedCalc Software bvba, Mariakerke, Belgium). The variables were expressed as mean±standard deviation and median (25-75 percentiles). Data were tested for normal distribution with the Shapiro-Wilks test. Independent and paired sample t-tests were used for the analysis of normally distributed variables. Mann-Whitney U test and Wilcoxon signed-rank test were used for the analysis of non-normally distributed variables. The diagnostic performance of IMA was assessed by receiver operating characteristic (ROC) curve analysis. From the ROC curve, the optimum diagnostic cutoff point for the present study population was chosen to maximize clinical sensitivity and specificity. Categorical data were presented as frequencies and percentages. p-values <0.05 were considered to be statistically significant.
Results
IMA levels on admission
In the patients with acute decompensated HF, the mean serum concentration of IMA was found to be significantly higher than those of the control healthy subjects (0.894±0.23 AU vs. 0.379±0.08 AU, p<0.001) (Fig. 1). The area under the ROC curve (AUC) was 0.97 (95% CI, 0.90-0.99, p=0.0001) for the diagnosis of acute decompensated HF with a diagnostic cutoff point of 0.578 AU (Fig. 2). The sensitivity and specificity were 92.8% (95% CI, 0.84-0.97) and 100% (95% CI, 0.89-100), respectively, and the positive and negative predictive values were found to be 100% (95% CI, 0.94-100) and 86.5% (95% CI, 0.710.95), respectively, for the present study population.
Figure 1.
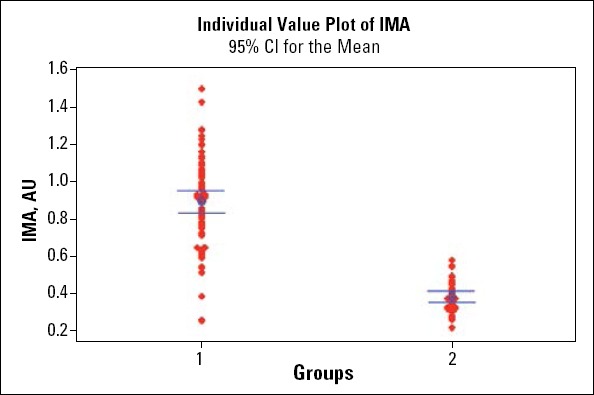
Ischemia-modified albumin (IMA) levels in patients with acute decompensated heart failure (1) and control healthy subjects (2) on hospital admission (0.894±0.23 AU vs. 0.379±0.08 AU, p<0.001)
Figure 2.
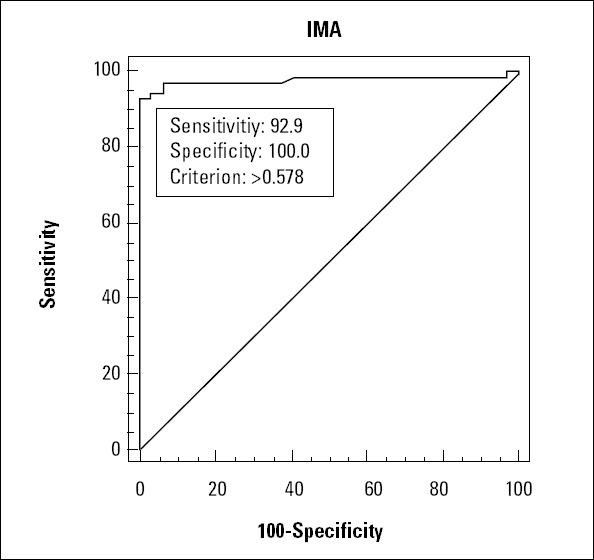
ROC curve of IMA for the diagnosis of acute decompensated heart failure with a diagnostic cutoff point of 0.578 AU. The area under the curve (AUC) was 0.97 (95% CI, 0.90-0.99, p=0.0001)
Changes in IMA levels following appropriate HF therapy
Overall, no statistically significant changes were observed in the serum sodium, creatinine, albumin, cTnI, and hemoglobin levels during HF therapy (Table 2). As expected, the NT-proBNP and sPAP levels were found to significantly decrease and LVEF to significantly increase following appropriate HF therapy (Table 2). A slight increase in the BUN levels and a slight decrease in the serum potassium levels were identified, probably as a result of the side effects of loop diuretic treatment.
Table 2.
Changes in clinical and laboratory variables following heart failure therapy
| Admission | After HF therapy | P | |
|---|---|---|---|
| Systolic BP mm Hg* | 113±20 | 109 ± 15 | 0.121 |
| Diastolic BP mm Hg* | 68±14 | 66±10 | 0.290 |
| Heart rate, bpm* | 83±16 | 80±13 | 0.189 |
| Hemoglobin, gr/dL* | 12.5±2.3 | 12.1±2.1 | 0.061 |
| Sodium, mg/dL* | 137±6.1 | 136±5.2 | 0.210 |
| Potassium, mg/dL* | 4.5±0.6 | 4.3±0.4 | 0.002 |
| BUN, mg/dL * | 29.8±19.3 | 32.6±19.9 | 0.022 |
| Creatinine, mg/dL* | 1.15±0.4 | 1.21 ± 0.4 | 0.193 |
| Albumin, mg/dL* | 3.8±0.6 | 3.7±0.5 | 0.077 |
| NT-proBNP pg/mL** | 4343 (1730-9858) | 3298 (1030-9528) | 0.001 |
| cTnI, ng/mL** | 0.030 (0.010-0.077) | 0.030 (0.010-0.067) | 0.408 |
| LVEF, %* | 25.4±6.1 | 26.5±6.3 | 0.001 |
| sPAP mm Hg* | 43.4±19 | 39.2±11 | 0.001 |
mean±SD, Paired t test,
median(Quartiles), Wilcoxon signed-rank test
BP - blood pressure; BUN - blood urea nitrogen; cTn - cardiac troponin-I; LVEF - left ventricular ejection fraction; NT-proBNP - N-terminal pro-brain natriuretic peptide; sPAP - systolic pulmonary arterial pressure
Furthermore, when compared with the admission levels, the serum IMA concentrations significantly decreased following 24-48 h of the initiation of appropriate HF therapy (0.894±0.23 AU and 0.832±0.18 AU, respectively, p=0.013). In the subgroup analysis in terms of inotropic therapy, the serum IMA levels were found to significantly decrease in the standard therapy group (1.041±0.28 vs. 0.884±0.15 AU, p=0.041) and also in the levosimendan group (0.771±0.18 vs. 0.728±0.18 AU, p=0.046) and also significantly reduced in the dobutamine group (0.892±0.18 vs. 0.820±0.13 AU, p=0.035) following appropriate in-hospital HF therapy (Fig. 3). The magnitude of serum IMA reduction was not significantly different between the levosimendan and dobutamine groups (0.043±0.13 vs. 0.071±0.15 AU, p=0.541), levosimendan and standard therapy groups (0.043±0.13 vs. 0.15±0.27 AU, p=0.155), and also dobutamine and standard therapy groups (0.071±0.15 vs. 0.15±0.27 AU, p=0.280).
Figure 3.
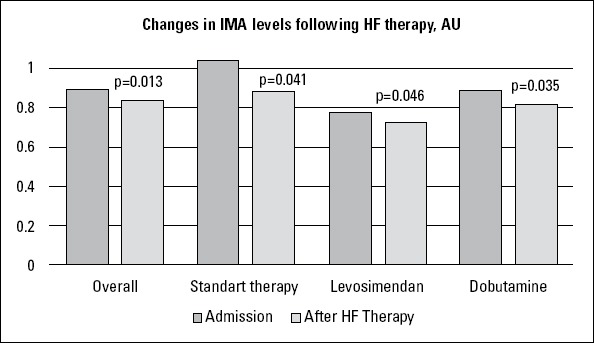
Changes in serum IMA concentrations 24-48 h after the initiation of appropriate heart failure therapy. The magnitude of IMA reduction was not different among the subgroups
Most probably because of the rapid hemodynamic response to inotropic agents, the NT-proBNP levels were found to significantly reduce after 24-48 h of HF therapy in the levosimendan group [4357 (1321-7910) vs. 2390 (813-10155) pg/mL, p=0.005] and also in the dobutamine group [5743 (2745-12991) vs. 4195 (208210002) pg/mL, p=0.022]. The magnitude of reduction in the NT-proBNP levels was similar between the levosimendan and dobutamine groups [302 (194-4279) vs. 683 (221-5636) pg/mL, p=0.610]. However, the NT-proBNP levels did not significantly change in the standard therapy group [2044 (1337-13243) vs. 2654 (236-12158), p=0.655]. Also, the cTnI levels did not significantly change after 24-48 h of HF therapy in the levosimendan group [0.025 (0.01-0.057) vs. 0.03 (0.01-0.05) ng/mL, p=0.893], in the dobutamine group [0.04 (0.01-0.2) vs. 0.035 (0.01-0.3) ng/mL, p=0.407], and also in the standard therapy group [0.02 (0.0170.05) vs. 0.03 (0.02-0.07) ng/mL, p=0.713].
Discussion
The results of this multicenter study mainly demonstrated that the patients presenting with acute decompensated HF had elevated serum IMA concentrations when compared with those of the healthy controls and that appropriate in-hospital HF therapy significantly reduced the serum IMA levels. The findings of the present study also showed that the serum IMA levels did not increase during treatment with dobutamine or levosimendan, suggesting lower potential of these inotropic agents in inducing myocardial ischemia and increasing oxidative stress when used in clinically recommended doses.
Ischemia and oxidative stress structurally alter the N-terminal portion of serum albumin and thereby reduce the metal-binding capacity of the protein resulting in IMA formation. Ischemia in any organ before infarction can lead to IMA elevation within 6-10 min, which returns to baseline values within 6 h (4, 16). IMA has mostly been studied in coronary events (2-5) and is reported to be a strong predictor of long-term outcome in patients with ACS (17). Because of the lack of tissue specificity, elevated IMA levels have also been identified in many clinical conditions, such as systemic sclerosis (18), rheumatoid arthritis (19), pulmonary embolism (20), chronic liver disease (21), or exposure to trauma (22). In these clinical conditions, IMA elevation does not only result from tissue ischemia, but also from oxidative stress or chronic inflammation. In a recent study in patients with slow coronary flow, the antioxidant level was reported to be negatively correlated with serum IMA levels (23).
Heart failure is associated with myocardial oxidative stress, inflammatory activation, and thereby endothelial dysfunction, which all contribute significantly to the pathophysiology and progression of this clinical syndrome (6-24). In HF, myocardial oxidative stress leads to myocyte apoptosis, cardiac remodeling, and progressive deterioration of the failing myocardium (25). Reactive oxygen species mediate the activation of apoptotic cell death pathways in response to hemodynamic overload and beta-adrenergic stimulation (26). Hemodynamic overload and adrenergic activation are very high in an acute HF setting, and therefore, oxidative stress is expected to be much more pronounced in patients with acute decompensated HF. Moreover, c orona ry hea rt d isea se is a c ommon c omorbi d c ond iti on in patients with HF, which is also one of the reasons for oxidative stress. However, little is known about IMA levels in HF.
In a very recent paper, serum IMA and oxidative stress levels have been reported to be significantly higher in chronic ischemic HF patients than in healthy individuals (27). The results of our study further verified the highly significant elevation of serum IMA levels in the setting of acute decompensated HF. Dominguez-Rodriguez et al studied the relation of IMA levels with left ventricular systolic function in patients presenting with myocardial infarction (MI) who underwent primary PCI and found a significant inverse correlation between IMA levels and LVEF and also a close relation with the occurrence of HF (28). Different from our study, which included acute HF patients and excluded ACS or recent PCI, they studied in patients with acute MI treated with primary PCI in which ACS and PCI themselves lead to a significant increase in IMA levels that make it difficult to interpret the reason for IMA elevation. In their study, the sensitivity and specificity of IMA for HF were 93.3% and 37.7%, respectively, at 0.31 AU (28). Furthermore, our findings demonstrated a significant reduction in the IMA levels in response to HF therapy, suggesting reduction in oxidative stress with the treatment of HF.
There is a link between oxidative stress and adrenergic stimulation in HF as increased plasma catecholamine levels are reported to be a strong stimulus for the generation of reactive oxygen species (8, 26). The commonly used beta-adrenergic inotropic agent dobutamine increases myocardial contractility at the expense of increased myocardial oxygen consumption (29, 30). In animal models, dobutamine has been shown to reduce subendocardial blood flow and may cause myocardial injury (10). Therefore, there is some concern about dobutamine in precipitating myocardial ischemia or oxidative stress. In contrast, levosimendan, a novel calcium-sensitizing inotropic agent with vasodilatory and cardioprotective properties, does not increase myocardial oxygen demand and oxidative stress and also shows antioxidant and anti-inflammatory effects (31, 32).
The subgroup analysis of our study showed that the serum IMA levels significantly decreased with not only treatment with levosimendan but also treatment with dobutamine used in clinically recommended doses.
Study limitations
Several limitations of the present study should be emphasized. A relatively small patient population is one of the limitations of this present study, which make it difficult to interpret subgroup findings. The lack of correlation of IMA with any parameters studied might be due to the small sample size. In our study population, the sensitivity and specificity of IMA for acute decompensated HF were 92.8% and 100%, respectively, at 0.578 AU, in which the specificity of IMA was much higher than expected when taking into account the lack of tissue specificity for IMA. The sensitivity and specificity largely depend on the patient population selected. From the diagnostic standpoint, it would be best to include all patients presenting with dyspnea of unknown etiology in order to determine the diagnostic potential of IMA for acute HF. However, the primary objective of our study was not to determine the diagnostic performance of IMA but rather to evaluate the IMA levels and treatment effects on IMA in acute HF. Our findings at least showed that the serum IMA level was a highly sensitive marker for acute decompensated HF.
Conclusion
This study suggested for the first time that patients presenting with acute decompensated HF had elevated levels of IMA when compared with healthy controls and also suggested that in-hospital acute HF therapy significantly reduced the serum IMA levels. The findings of this study also demonstrated that levosimendan and dobutamine did not increase the IMA levels, suggesting a lower potential of these inotropic agents in inducing myocardial ischemia or increasing oxidative stress when used in clinically recommended doses. IMA, as a highly sensitive marker, may have some diagnostic potential for the assessment of acute decompensated HF; however, further studies designed to specifically assess its diagnostic ability are necessary for this patient population.
Footnotes
Conflict of interest: None declared.
Peer-review: Externally peer-reviewed.
Authorship contributions: Concept - Y.Ç.; Design - Y.Ç., M.B.Y., Ş.K., E.G., S.D.; Supervision - H.Ş., F.M., H.G., U.K.M., S.Ö., S.K.; Resource - Y.Ç., S.D., E.G., S.K., H.Ş.; Materials - S.D., M.B.Y.; Data collection &/or processing - H.G., U.K.M., S.Ö., S.K., E.G.; Analysis &/or interpretation - Y.Ç., F.M.; Literature search - Y.Ç., S.D.; Writing - Y.Ç., M.B.Y., S.D., E.G., Ş.K.; Critical review - S.D., H.Ş., E.G., Ş.K., M.B.Y.
References
- 1.Cho DK, Choi JO, Kim SH, Choi J, Rhee I, Ki CS, et al. Ischemia-modified albumin is a higly sensitive serum marker of transient myocardial ischemia induced by coronary vasospasm. Coron Artery Dis. 2007;18:83–7. doi: 10.1097/MCA.0b013e328010a49f. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 2.Sinha MK, Roy D, Gaze DC, Collinson PO, Kaski JC. Role of “ischemia modified albumin,“a new biochemical marker of myocardial ischemia, in the early diagnosis of acute coronary syndromes. Emerg Med J. 2004;21:29–34. doi: 10.1136/emj.2003.006007. [CrossRef] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sinha MK, Gaze DC, Tippins JR, Collinson PO, Kaski JC. Ischemia modified albumin is a sensitive marker of myocardial ischemia after percutaneous coronary intervention. Circulation. 2003;107:2403–5. doi: 10.1161/01.CIR.0000072764.18315.6B. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 4.Bar-Or D, Winkler JV, VanBenthysen K, Harris L, Lau E, Hetzel FW. Reduced albumin-cobalt binding with transient myocardial ischemia after elective percutaneous transluminal coronary angioplasty: a preliminary comparison to creatinine kinase-MB, myoglobin, and troponin I. Am Heart J. 2001;141:985–91. doi: 10.1067/mhj.2001.114800. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 5.Quiles J, Roy D, Gaze D, Garrido IP, Avanzas P, Sinha M, et al. Relation of ischemia modified albumin (IMA) levels following elective angioplasty for stable angina pectoris to duration of balloon induced myocardial ischemia. Am J Cardiol. 2003;92:322–4. doi: 10.1016/s0002-9149(03)00638-6. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 6.Josephson RA, Silverman HS, Lakatta EG, Stern MD, Zweier JL. Study of the mechanisms of hydrogen peroxide and hydroxyl free radical induced cellular injury and calcium overload in cardiac myocytes. J Biol Chem. 1991;266:2354–61. [PubMed] [Google Scholar]
- 7.Ide T, Tsutsui H, Kinugawa S, Utsumi H, Kang D, Hattori N, et al. Mitochondrial electron transport complex I is a potential source of oxygen free radicals in the failing myocardium. Cir Res. 1999;85:357–63. doi: 10.1161/01.res.85.4.357. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 8.Nakamura K, Kusano K, Nakamura Y, Kakishita M, Ohta K, Nagase S, et al. Carvedilol decreases elevated oxidative stress in human failing myocardium. Circulation. 2002;105:2867–71. doi: 10.1161/01.cir.0000018605.14470.dd. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 9.Cobbe SM, Poole-Wilson PA. The time of onset and severity of acidosis in the myocardial ischemia. J Mol Cell Biol. 1980;12:74560. doi: 10.1016/0022-2828(80)90077-2. [DOI] [PubMed] [Google Scholar]
- 10.Schulz R, Rose J, Martin C, Brodde OE, Heusch G. Development of short-term myocardial hibernation. Its limitation by the severity of ischemia and inotropic stimulation. Circulation. 1993;88:684–95. doi: 10.1161/01.cir.88.2.684. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 11.Krell MJ, Kline EM, Bates ER, Hodgson JM, Dilworth LR, Laufer N, et al. Intermittent, ambulatory dobutamine infusion in severe congestive heart failure. Am Heart J. 1986;112:787–91. doi: 10.1016/0002-8703(86)90475-8. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 12.Michaels AD, Mckeown B, Kostal M, Vakharia KT, Jordan MV, Gerber IL, et al. Effects of intravenous levosimendan on human coronary vasomotor regulation, left ventricular wall stress, and myocardial oxygen uptake. Circulation. 2005;111:1504–9. doi: 10.1161/01.CIR.0000159252.82444.22. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 13.Ukkonen H, Saraste M, Akkila J, Knuuti J, Karanko M, Lida H, et al. Myocardial efficiency during levosimendan infusion in congestive heart failure. Clin Pharmacol Ther. 2000;68:522–31. doi: 10.1067/mcp.2000.110972. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 14.Çavuşoğlu Y, Korkmaz Ş, Demirtaş S, Gencer E, Şasmaz H, Mutlu F, Yılmaz MB. Ischemia-Modified Albumin levels in patients with acute decompansated heart failure treated with dobutamine or levosimendan: IMA-HF Study. ESC Congress 2013, 31 August-4 September Amsterdam Netherlands. European Heart Journal. 2013;34(Abstract Suppl):P5711. doi: 10.5152/akd.2015.6156. 1064-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Bar-Or D, Lau E, Winkler JV. A novel assay for cobalt-albumin binding and its potential as a marker for myocardial ischemia-a preliminary report. J Emerg Med. 2000;19:311–5. doi: 10.1016/s0736-4679(00)00255-9. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 16.Christenson RH, Duh SH, Sanhai WR, Wu AH, Holtman V, Painter P, et al. Characteristics of an albumin cobalt binding test for assessment of acute coronary syndrome patients: a multicenter study. Clin Chem. 2001;47:464–70. [PubMed] [Google Scholar]
- 17.Belle EV, Dallongeville J, Vicaut E, Degrandsart A, Baulac C, Montalescot G. Ischemia-modified albumin levels predict long-term outcome in patients with acute myocardial infarction. The French Nationwide OPERA study. Am Heart J. 2010;159:570–6. doi: 10.1016/j.ahj.2009.12.026. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 18.Montagnana M, Lippi G, Volpe A, Salvagno GL, Biasi D, Caramaschi P, et al. Evaluation of cardiac laboratory markers in patients with systemic sclerosis. Clin Biochem. 2006;39:913–7. doi: 10.1016/j.clinbiochem.2006.03.016. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 19.Leitemperguer MR, Tatsch E, Kober H, De Carvalho JA, Moresco RN, Da Silva JE. Assessment of ischemia-modified albumin levels in patients with rheumatoid arthritis. Clin Lab. 2014;60:1065–70. doi: 10.7754/clin.lab.2013.130143. [DOI] [PubMed] [Google Scholar]
- 20.Türedi S, Gündüz A, Menteşe A, Karahan SC, Yılmaz SE, Aroğlu O, et al. Value of ischemia-modified albumin in the diagnosis of pulmonary embolism. Am J Emerg Med. 2007;25:770–3. doi: 10.1016/j.ajem.2006.12.013. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 21.Chen CY, Tsai WL, Lin PJ, Shiesh SC. The value of serum ischemia-modified albumin for assessing liver function in patients with chronic liver disease. Clin Chem Lab Med. 2011;49:1817–21. doi: 10.1515/CCLM.2011.675. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 22.Can M, Demirtaş S, Polat O, Yıldız A. Evaluation of effects of ischemia on the albumin cobalt binding (ACB) assay in patients exposed to trauma. Emerg Med J. 2006;23:537–9. doi: 10.1136/emj.2005.030486. [CrossRef] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Koç F, Erdem S, Altunkaş F, Özbek K, Gül EE, Kurban S, et al. Ischemia-modified albumin and total antioxidant status in patients with slow coronary flow: a pilot observational study. Anatol J Cardiol. 2011;11:582–7. doi: 10.5152/akd.2011.159. [DOI] [PubMed] [Google Scholar]
- 24.Fischer D, Rossa S, Landmesser U, Spiekermann S, Engberding N, Hornig B, et al. Endothelial dysfunction in patients with chronic heart failure is independently associated with increased incidence of hospitalization, cardiac transplantation, or death. Eur Heart J. 2005;26:65–9. doi: 10.1093/eurheartj/ehi001. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 25.Sorescu D, Griendling KK. Reactive oxygen species, mitochondria, and NAD(P)H oxidases in the development and progression of heart failure. Congest Heart Fail. 2002;8:132–40. doi: 10.1111/j.1527-5299.2002.00717.x. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 26.Castro PF, Greig D, Perez O, Moraga F, Chiong M, Diaz-Araya G, et al. Relation between oxidative stress, catecholamines, and impaired chronotropic response to exercise in patients with chronic heart failure secondary to ischemic or idiopathic cardiomyopathy. Am J Cardiol. 2003;92:215–8. doi: 10.1016/s0002-9149(03)00543-5. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 27.Ellidağ HY, Eren E, Yılmaz N, Çekin Y. Oxidative stress and ischemia-modified albumin in chronic ischemic heart failure. Redox Rep. 2014;19:118–23. doi: 10.1179/1351000213Y.0000000083. [CrossRef] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Dominguez-Rodriguez A, Abreu-Gonzales P, Garcia-Gonzales MJ, Samimi-Fard S, Kaski JC. Relation of ischemia-modified albumin levels and left ventricular systolic function in patients with ST-segment elevation myocardial infarction treated with primary percutaneous coronary intervention. Clin Chim Acta. 2008;388:196–9. doi: 10.1016/j.cca.2007.10.030. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 29.Gross R, Strain J, Greenberg M, LeJemtel TH. Systemic and coronary effects of intravenous milrinone and dobutamine in congestive heart failure. J Am Coll Cardiol. 1986;7:1107–13. doi: 10.1016/s0735-1097(86)80231-5. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 30.Pacold I, Kleinman B, Gunnar R, Loeb HS. Effects of low-dose dobutamine on coronary hemodynamics, myocardial metabolism and anginal threshold in patients with coronary artery disease. Circulation. 1983;68:1044–50. doi: 10.1161/01.cir.68.5.1044. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 31.Ukkonen H, Saraste M, Akkila J, Knuuti MJ, Lehikoinen P, Nagren K, et al. Myocardial efficiency during calcium sensitization with levosimendan: a noninvasive study with positron emission tomography and echocardiography in healthy volunteers. Clin Pharmacol Ther. 1997;61:596–607. doi: 10.1016/S0009-9236(97)90139-9. [CrossRef] [DOI] [PubMed] [Google Scholar]
- 32.Parissis JT, Andreadou I, Bistola V, Paraskevaidis I, Flippatos G, Kresmastinos DT. Novel biologic mechanisms of levosimendan and its effect on the failing heart. Expert Opin Investig Drugs. 2008;17:1143–50. doi: 10.1517/13543784.17.8.1143. [CrossRef] [DOI] [PubMed] [Google Scholar]