

Abstract
Cardiac computed tomography (CCT) has become an invaluable cross-sectional imaging modality in congenital heart disease (CHD) patients. However, altered anatomical connections and cardiovascular physiology makes CHD arguably the most challenging area in CCT imaging, which remains a complimentary modality to cardiac magnetic resonance and echocardiography. A bespoke CT protocol is often required to achieve a diagnostic examination; this can be achieved through careful consideration of the basic principles of image acquisition and contrast administration. This article reviews these principles and demonstrates how they can be applied to CCT in CHD using the Fontan circulation as an example.
Keywords: Computed tomography (CT), congenital cardiac disease, bespoke acquisition protocol design, iodinated contrast haemodynamics, Fontan circuit
Introduction
The use of cardiac computed tomography (CCT) in congenital heart disease (CHD) has enhanced the applicability of cross sectional anatomical imaging. CHD is arguably the most challenging area of imaging in cardiac CT and is ideally performed by those with appropriate training and experience. However, when the general radiologist is faced with a CHD case, bespoke protocols can be formulated for the specific system and indication through applying general principles in CT acquisition and contrast administration. This article uses the Fontan circuit as an example of how CT imaging in complex CHD can be approached with reference to our experience in a tertiary referral centre.
Individual modalities have specific attributes for assessment of CHD but no single imaging method is comprehensive in any given patient. Therefore, referrers and cardiac imagers must recognize the limitations of each imaging technique and endeavor to use a multi-modality approach.
Whilst echocardiography is the most widely used imaging modality in CHD, image quality can be suboptimal due to poor acoustic windows. There is often the need to examine extra cardiac structures and previous surgical procedures (1) and anatomy may remain undefined or uncertain.
Catheter cardiac angiography has long been the mainstay imaging tool. However as an invasive modality, it has a higher complication rate compared with CT (2,3). It may require higher doses of contrast medium (2), more frequently general anaesthesia (2), often imparts greater radiation dose (4,5) and provides limited information on the extra vascular structures. It does have the advantage of invasive haemodynamic assessment e.g., pressure measurements, shunt calculations and oxygen saturations.
MRI is frequently and widely used for the long-term monitoring of complex CHD patients but is contraindicated in patients with non-MRI compatible pacemakers and devices, which may be present. Additionally, metallic devices cause magnetic resonance artefacts. Figure 1 demonstrates how significant metallic artefact from a stainless steel coil in the ductus arteriosus essentially renders a MRI study non-diagnostic.
Figure 1.
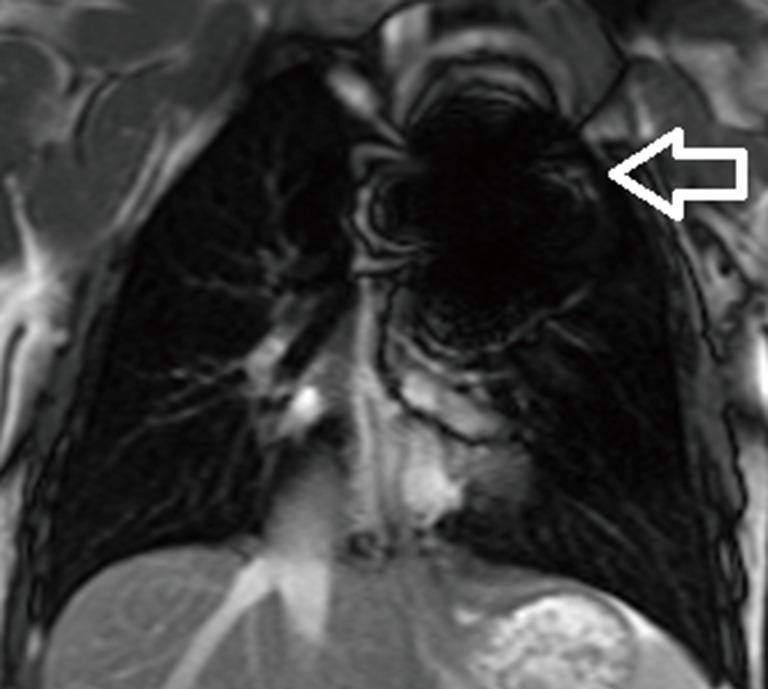
Metallic artefact from a stainless steel coil in the ductus arteriosus (white arrow) resulting in a non-diagnostic CMR study.
Whilst ionising radiation is a consideration, modern CT scanners have significantly reduced radiation dose which in turn reduces the number of invasive catheter studies and thus the reduction in overall patient radiation burden (6). Importantly, CT can facilitate a more focused approach to the catheter angiographic study.
CCT imaging in the context of CHD requires appropriate knowledge of the expected anatomical connections, the potentially complex physiology and haemodynamics and vitally, the specific clinical question(s) to be answered. This is of particular importance in the context of the Fontan circuit, which, in the authors’ opinion, presents one of the more difficult challenges to cardiac CT and probably one of the better examples to illustrate this.
The Fontan circuit
Anatomical review
The Fontan circulation is a series of palliative surgical procedures performed in patients with cardiac anomalies that preclude achieving a successful bi-ventricular repair (Table 1) (7). It results in diversion of systemic venous return directly to the pulmonary arteries, without passing through a ventricle resulting in a single ventricular physiology.
Table 1. Conditions precluding a successful biventricular repair.
| Tricuspid atresia |
| Pulmonary atresia with intact ventricular septum |
| Mitral atresia |
| Hypoplastic left heart syndrome |
| Various univentricular hearts |
The procedure was proposed by Francois Fontan and Eugene Baudet in 1971 for tricuspid atresia but has since undergone several revisions (8). The initial circuit involved a classical Glenn shunt between the superior vena cava (SVC) and right pulmonary artery (RPA). The SVC was ligated at the SVC/right atrium (RA) confluence with division of the RPA from the main pulmonary artery (MPA) bifurcation (7). A connection between the RA and MPA was formed to complete a bypass of the ventricle (7). There have been several modifications of this technique, collectively known as the atriopulmonary Fontan (Figure 2) (9).
Figure 2.

Volume rendered computed tomography (CT) of original Fontan circuit—the atriopulmonary connection. The right atrial auricle is anastomosed to the pulmonary artery (white arrows). The tricuspid valve is sealed, allowing blood to flow directly from the right atrium (RA) to the pulmonary circuit.
Due to the emergence of late complications, the atriopulmonary circuit technique has been modified by a bidirectional Glenn (SVC to RPA shunt with the anastomosis formed to direct flow to the RPA and LPA) followed by channelling of blood from the inferior vena cava (IVC) to the RPA via a baffle within the RA [total cavo-pulmonary connection (TCPC) or lateral tunnel] or an extra cardiac prosthetic conduit connecting IVC to PA (Figure 3). Note if the IVC or SVC were to be left-sided, a left-sided connection to the pulmonary arteries is required.
Figure 3.
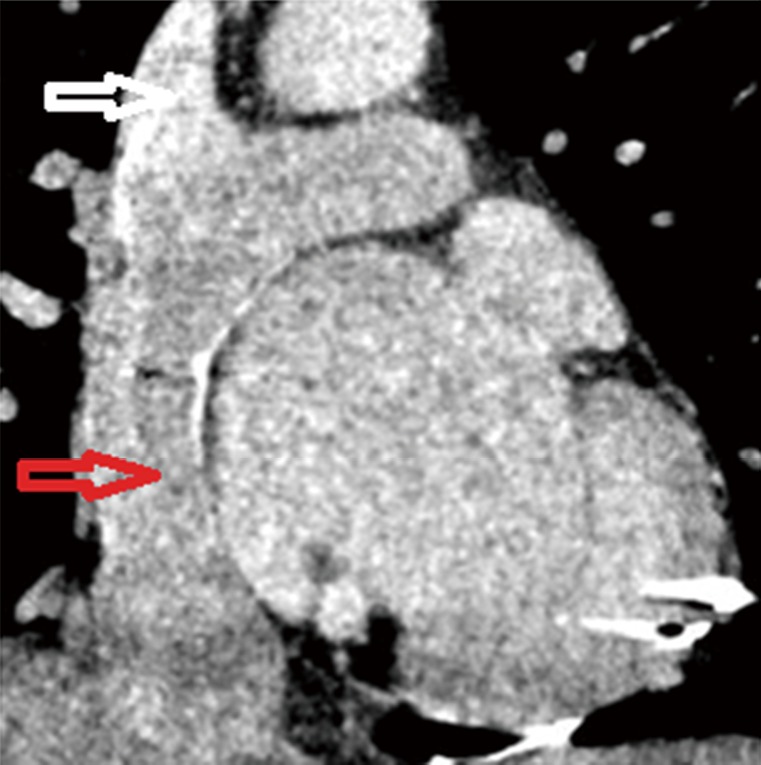
Coronal computed tomography (CT) demonstrating an extra-cardiac Fontan with a prosthetic conduit connecting the inferior vena cava (IVC) to the pulmonary arteries (red arrow). The conduit usually has a fenestration to the right atrium (RA). The SVC is anastomosed to the right pulmonary artery (RPA) (white arrow).
CT contrast haemodynamics
In terms of contrast haemodynamics in a Fontan circuit, peripheral venous contrast injection in the right arm enter the SVC, then to the pulmonary arteries, typically opacifying the RPA more than the LPA (with a right SVC). This then opacifies the right pulmonary veins first with relatively delayed left pulmonary venous opacification (Figure 4A). After flowing through the pulmonary veins and the systemic ventricle to the systemic arterial circulation, contrast returns from the lower body via the IVC (Figure 4B) to the RPA anastomosis with flow preferentially directed towards the LPA. Contrast is also recirculated via the SVC. Thus knowledge of the underlying anatomy informs the timing of the CT to answer the posed clinical question and avoid an inadequate examination.
Figure 4.
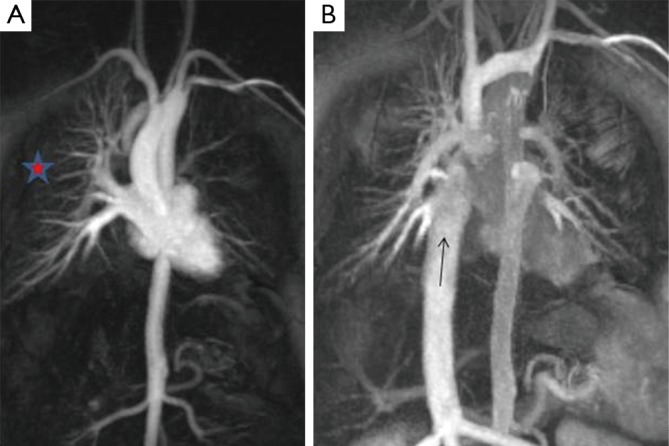
Cardiac MR angiogram with early (A) and late (B) phase acquisitions. (A) Contrast flows down the right sided SVC to preferentially fill the right pulmonary artery (RPA). There is unilateral opacification of the right pulmonary veins (red star). After contrast has circulated and returns to the heart via the inferior vena cava (IVC) (B), it preferentially fills the left pulmonary artery.
The intravenous contrast administration protocol (contrast flux and length of bolus), field of view and timing of the CCT scan will vary depending on the clinical question. The implications of renal dysfunction are beyond the scope of this paper.
Common problems encountered are:
Suboptimal anatomical opacification—not enough contrast, wrong timing, wrong anatomy opacified;
Pseudothrombus or pseudoembolism—caused by mixing of unopacified with opacified blood as a consequence of timing and haemodynamics;
Insufficiently imaged field of view.
Principles in contrast administration and CT acquisition
As discussed, patients with CHD and Fontan circuits have variable shunts, cardiac connections and variably impaired haemodynamics which all influence intra-vascular physiology, again, emphasising the importance of this clinical detail prior to the CT. We suggest that the CT protocol has to be tailored to the individual and the specific clinical indication. There are important generic factors to consider when formulating a bespoke protocol for CHD patients, which can broadly be broken down into patient, contrast and CT scanning parameters.
Patient factors: weight and cardiac output
The most important patient-related factor affecting the magnitude of vascular contrast enhancement is patient weight (10). Larger patients have larger blood volumes and therefore dilute any given contrast volume more than smaller patients, resulting in lower contrast enhancement. This is demonstrated in Figure 5, where for a given concentration and volume of contrast injected at a given rate, patients with a lower body weight have higher enhancement curves. Weight based protocols ensure contrast dose is optimised for the patients predicted blood volume. As patients with Fontan circuits can be imaged at any age with CT, tailoring contrast dose to the patient’s weight is clearly important.
Figure 5.
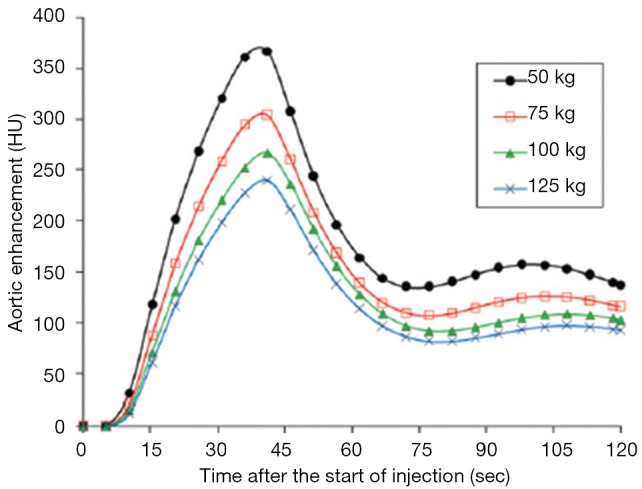
Simulated contrast enhancement curves (10). Simulated contrast enhancement curves of the aorta on hypothetical adults of varying body weights who underwent an injection of 125 mL iodinated contrast at 4 mL/s. Higher body weights require higher doses of contrast at faster rates to achieve the same enhancement.
A critical patient related factor affecting the timing of contrast enhancement is cardiac output and cardiovascular circulation (10). In patients with impaired left ventricular function, for a fixed volume and flow rate of contrast, there is a delay in peak enhancement and lower attenuation than patients with normal left ventricular function (11). The cardiac output of patients with Fontan circuits is often impaired and consequently a test bolus or bolus tracking can help understand patient specific haemodynamics (see below).
Contrast medium factors: injection rate, duration and pattern (uniphasic versus biphasic contrast injection)
Consideration of contrast injection rate and duration is particularly relevant to Fontan circuits. The superior and inferior section of the Fontan connections opacify at different times post injection, but often each need to be adequately imaged. A fast injection rate will increase the magnitude of enhancement and cause earlier opacification, but narrows the potential temporal window for acquisition, as demonstrated in Figure 6 (10). The injection duration is defined as the contrast volume divided by the injection rate. As shown in Figure 7, for a fixed flow rate, longer contrast boluses cause a higher magnitude of opacification and higher total volume of contrast with constant cardiac output (10). Both injection rate and duration can be manipulated in two phases (“biphasic”) to ensure equal and optimal SVC and IVC opacification in a single acquisition (“biphasic contrast, single acquisition”—see Table 2 for an example).
Figure 6.
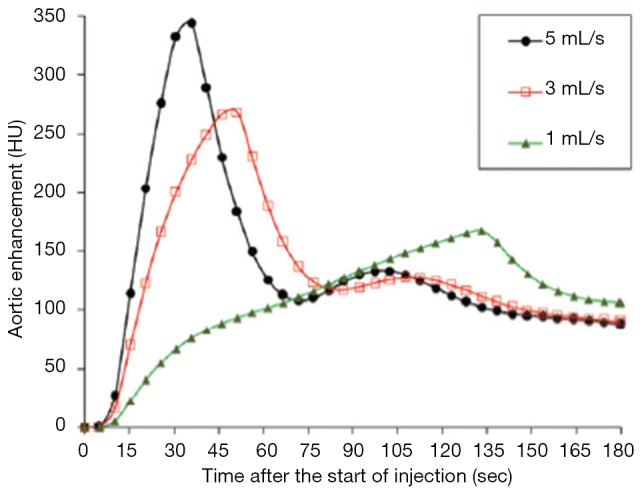
Simulated contrast enhancement curves (10). Simulated contrast enhancement curves of the aorta on a hypothetical adult of 70 kg who underwent a fixed injection volume of 125 mL iodinated contrast at varying injection rates. Faster injection rates increase the magnitude of enhancement and cause earlier opacification, but narrow the temporal window for acquisition.
Figure 7.
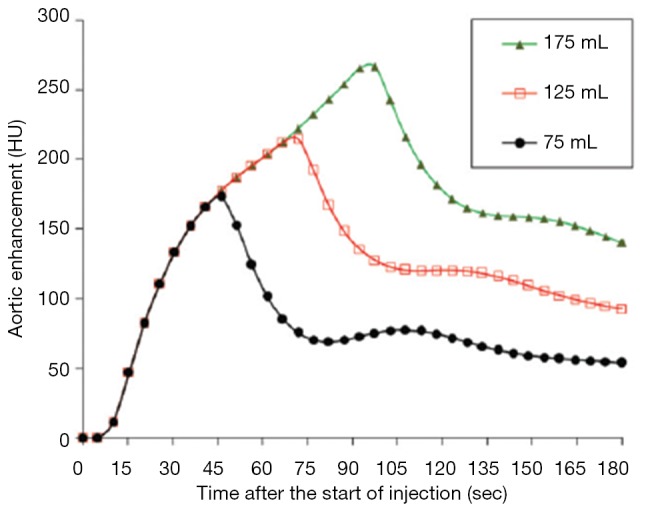
Simulated contrast enhancement curves (10). Simulated contrast enhancement curves of the aorta on a hypothetical adult of 70 kg subjected to three volumes of iodinated contrast at 2 mL/s.
Table 2. Examples of three different protocols used in our institution.
| Weight (kg) | Diagnosis | Fontan/shunt type | Indication/question | Contrast injection rate | Contrast volume (mL) | Contrast injection duration (s) | Contrast phase | Acquisition (s) | Acquisition phase |
|---|---|---|---|---|---|---|---|---|---|
| 62 | Pulmonary atresia. RV-coronary arterial fistula | Right modified Blalock Taussig. Bidirectional Glenn. Lateral tunnel TCPC | Coronary angiogram showed RCA/LAD fistula connecting to the RV | 6 mL/s | 100 | 17 | Single | 30 | Single |
| 63 | Tricuspid atresia. Pulmonary stenosis. Sinus of Valsalva aneurysm with LVOT obstruction | Extra-cardiac Fontan | Calcified mass in LVOT on TTE, failed TOE | 50 mL at 3 mL/s, 30 mL at 1 mL/s | 80 | 47 | Biphasic | 65 | Single |
| 60 | Right atrial isomerism total anomalous pulmonary venous drainage. Double outlet RV | Extra-cardiac Fontan | Pulmonary venous obstruction or systemic venous to pulmonary venous collaterals. Raised Fontan pressures on catheter angiography | 3 mL/s | 146 | 49 | Single | 55 and 110 | Biphasic |
RV, right ventricle; TCPC, total cavo-pulmonary connection; RCA, right coronary artery; LAD, left anterior descending coronary artery; LVOT, left ventricular outflow tract; TTE, trans-thoracic echocardiogram; TOE, trans-oesphageal echocardiogram.
CT scanning factors: timing (fixed, test bolus, bolus tracking) and uniphasic versus biphasic scanning acquisition
Effective scan timing can either be at a fixed delay or predicted from bolus tracking or test bolus injection. In bolus tracking, a region of interest in placed over the target vessel. After contrast injection, the scan triggers once a HU (typically 150) has been reached and the CT is performed several seconds later, allowing for breath holding instructions. A test bolus involves injecting a small volume (usually 20 mL) of contrast and acquiring multiple low radiation dose sequential images. A time enhancement curve can be calculated to determine the contrast haemodynamics of the individual. Figure 8 demonstrates enhancement patterns for different organs in a normal cardiovascular system (10). For Fontan circuits with different cardiac connections and altered haemodynamics, a test bolus may be preferable for aortic and coronary imaging, but is impractical for IVC conduit imaging as the subject may accrue a large radiation dose while waiting for IVC opacification, even with a scan delay, which itself will be very poor because of the low dose of contrast that will have been administered. An alternatively is to use a biphasic acquisition (“single contrast phase, biphasic acquisition”—see Table 2 for an example). The patient is scanned twice—once in optimal systemic opacification and once in caval/delayed or second-phase pulmonary arterial opacification.
Figure 8.
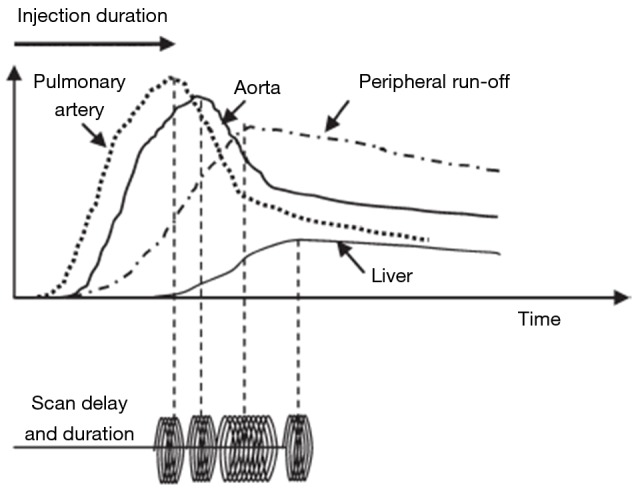
Test bolus method (10). Time enhancement curve and scan delay for organs of different circulatory paths. Computed tomography (CT) scan acquisition can be delayed appropriately from the start or completion of contrast injection.
Specific indications in Fontan circuits with proposed bespoke protocols
Coronary imaging
Either the test bolus or the bolus racking technique can obtain good aortic/coronary enhancement. An iodine flux of 20–24 mg/kg/s (lower dose suggested for 100 kV imaging, higher doses for 120 or 140 kV) will produce excellent arterial opacification. Bolus length (usually 15–20 s) will be dependent on the speed of the CT system. ECG gating is ideally applied prospectively and in mid diastole, though other modes may be required.
Systemic arterial, venous and coronary imaging
To ensure optimal coronary opacification in addition to superior and inferior Fontan connections, the single contrast phase, biphasic scanning (systemic arterial and delayed) acquisition protocol is suggested. A standard dose of contrast (at 100 kV 400 mg/kg iodine over 20 seconds = 20 mg/kg/s) is initially administered to ensure optimal arterial opacification. A second delayed image acquisition allows for contrast recirculation and opacification of the central veins (Figure 4B).
Pulmonary embolism and thrombus in the Fontan circuit
If a standard CT pulmonary angiographic protocol is performed in this patient group, it is almost certainly going to be either non-diagnostic or demonstrate a pseudoembolism or pseudothrombus (11). With an arm injection, contrast will usually flow preferentially into the RPA, very little in the left pulmonary artery and unopacified blood will be entering from below via the IVC or right atrial connection to the central pulmonary circulation (Figures 9,10). The usual result is hyperdense contrast layering in the RPA and inadequate enhancement of the LPA with unopacified blood causing pseudothrombus. The same effect occurs in the IVC to PA connection which may be dilated and behaving like a sump but contains slow-flowing, turbulent blood.
Figure 9.

Single contrast phase, single acquisition [as for standard computed tomography (CT) pulmonary angiogram protocol]. (A,B) Unopacified blood enters from the inferior Fontan connection causing mixing with contrast; (C) which causes pseudo-thrombi in the main pulmonary arteries.
Figure 10.

Single contrast phase, single acquisition [as for standard computed tomography (CT) pulmonary angiogram protocol]. (A) The column of unopacified blood (white arrow) entering the Fontan inferiorly; (B,C) the streaming effect and creation of “pseudo emboli” (red arrows).
Simultaneous homogeneous enhancement of the SVC, IVC and pulmonary arteries is needed. If renal function is normal the contrast dose can be increased to 600–800 mg/kg. Low kV, high mAs scanning can help to optimise image contrast in the conduits and PA circulation as a standard contrast dose (400 mg/kg) will not provide high HU enhancement (Figure 6). Using a single delayed phase acquisition (80–100 s) allows for contrast recirculation and opacification in the central veins and pulmonary arteries (Figure 11). Some operators may prefer to bolus track from the distal descending thoracic aorta with an appropriate additional delay (e.g., of 40–60 s).
Figure 11.

Sagittal and coronal computed tomography (CT) of the extra-cardiac Fontan circuit. Increased contrast dose with a delayed acquisition at 80 s. Both superior and inferior Fontan circuits are opacified.
Alternatively a biphasic contrast, single acquisition ensures simultaneous opacification of superior and inferior Fontan circuits. Optimal timing is around 55–65 s after contrast injection starts. A large volume of contrast (600–800 mg/kg) with an initial rapid flow rate/or high contrast “flux dump” (to optimise the delayed phase IVC enhancement) continued at a lower flow rate “tail” (to maintain optimal SVC and PA enhancement) such that the total contrast injection time is about 60 s. As the rapid flow rate of contrast switches to the lower flow rate, overall opacification remains high and stable, especially if low kV imaging can be used. Figure 12 demonstrates how this protocol can adequately opacify the Fontan, allowing for identification of a large clot.
Figure 12.

Atriopulmonary Fontan connection in tricuspid atresia. (A) The connection between right atrium (RA) and main pulmonary artery (MPA) (star); (B) how a biphasic contrast rate; single acquisition creates adequate opacification of the Fontan, allowing identification of a large clot (arrow).
Systemic arterial and Fontan/pulmonary imaging
This can be achieved with a single phase acquisition (as per point 3). However if coronary detail is also needed, a 2 phase acquisition (as per points 2 and 3) is required.
Fontan leak
This is problematic with CT as it is not usually possible to opacify the IVC conduit without contrast also being in the heart, thereby not allowing small jets of contrast to be appreciated easily. If desirable a leg injection with early imaging may be helpful, though streaming artefact will usually remain a problem and this is not routinely performed in our institution.
Some authorities (12) have had success with simultaneous contrast power injections via arm and common femoral venous cannulation; hand injection via a femoral vein will not be powerful enough and will result in streaming artefact given that unopacified blood is still entering the IVC from the contralateral iliac veins, the renal and hepatic veins. Power injection may not prevent this either. This method is also somewhat more impractical in the usual CT clinical setting and not routinely used in our institution.
General advice
Consider the use of prospective ECG-gated CT acquisition technique to reduce radiation dose and minimise motion artefact; consider whether a uni- or biphasic scan is required;
-
Adhere to a weight-based contrast protocol to aid optimal enhancement. Use low kV scanning if tube mAs output allows (to increase vascular enhancement with the necessary delayed imaging);
Increase the contrast dose if 120 or 140 kV scanning used. Consider giving more contrast volume at higher flow rates with dilated chambers, impaired ventricular function or severe volume loading due to valve dysfunction; this needs an adequately sized and positioned cannula (ideally an 18-gauge in the right antecubital fossa); consider whether a uni- or biphasic contrast injection is required;
Consider using a “test bolus” technique rather than a bolus tracking technique to get a feel for the cardiac haemodynamics;
Consider renal reduction regimes; low kV scanning to reduce contrast dose, low risk contrast agent, adequate intravenous pre-hydration and nephrotoxic drug optimisation or elimination.
Conclusions
CHD is probably the most challenging patient group to optimally image with CT and the Fontan circuit is particularly complex. A consistent and structured approach is required. A detailed knowledge of the haemodynamics and anatomical connections helps to tailor the study appropriately. Bespoke protocolling for each patient ensures the specific clinical indication is addressed.
Acknowledgements
The authors thank Dr. KT Bae (USA) for giving them permission to use several graphs (Figures 5-8) used in his publication.
Footnotes
Conflicts of Interest: The authors have no conflicts of interest to declare.
References
- 1.Prakash A, Powell AJ, Geva T. Multimodality noninvasive imaging for assessment of congenital heart disease. Circ Cardiovasc Imaging 2010;3:112-25. 10.1161/CIRCIMAGING.109.875021 [DOI] [PubMed] [Google Scholar]
- 2.Hollingsworth CL, Yoshizumi TT, Frush DP, Chan FP, Toncheva G, Nguyen G, Lowry CR, Hurwitz LM. Pediatric cardiac-gated CT angiography: assessment of radiation dose. AJR Am J Roentgenol 2007;189:12-8. 10.2214/AJR.06.1507 [DOI] [PubMed] [Google Scholar]
- 3.Mehta R, Lee KJ, Chaturvedi R, Benson L. Complications of pediatric cardiac catheterization: a review in the current era. Catheter Cardiovasc Interv 2008;72:278-85. 10.1002/ccd.21580 [DOI] [PubMed] [Google Scholar]
- 4.Gaca AM, Jaggers JJ, Dudley LT, Bisset GS, 3rd. Repair of congenital heart disease: a primer-part 1. Radiology 2008;247:617-31. 10.1148/radiol.2473061909 [DOI] [PubMed] [Google Scholar]
- 5.Dillman JR, Hernandez RJ. Role of CT in the evaluation of congenital cardiovascular disease in children. AJR Am J Roentgenol 2009;192:1219-31. 10.2214/AJR.09.2382 [DOI] [PubMed] [Google Scholar]
- 6.Walsh MA, Noga M, Rutledge J. Cumulative radiation exposure in pediatric patients with congenital heart disease. Pediatr Cardiol 2015;36:289-94. 10.1007/s00246-014-0999-y [DOI] [PubMed] [Google Scholar]
- 7.Lewis G, Thorne S, Clift P, Holloway B. Cross-sectional imaging of the Fontan circuit in adult congenital heart disease. Clin Radiol 2015;70:667-75. 10.1016/j.crad.2015.02.011 [DOI] [PubMed] [Google Scholar]
- 8.Fontan F, Baudet E. Surgical repair of tricuspid atresia. Thorax 1971;26:240-8. 10.1136/thx.26.3.240 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.de Leval MR, Deanfield JE. Four decades of Fontan palliation. Nat Rev Cardiol 2010;7:520-7. 10.1038/nrcardio.2010.99 [DOI] [PubMed] [Google Scholar]
- 10.Bae KT. Intravenous contrast medium administration and scan timing at CT: considerations and approaches. Radiology 2010;256:32-61. 10.1148/radiol.10090908 [DOI] [PubMed] [Google Scholar]
- 11.Prabhu SP, Mahmood S, Sena L, Lee EY. MDCT evaluation of pulmonary embolism in children and young adults following a lateral tunnel Fontan procedure: optimizing contrast-enhancement techniques. Pediatr Radiol 2009;39:938-44. 10.1007/s00247-009-1304-8 [DOI] [PubMed] [Google Scholar]
- 12.Sandler KL, Markham LW, Mah ML, Byrum EP, Williams JR. Optimizing CT angiography in patients with Fontan physiology: single-center experience of dual-site power injection. Clin Radiol 2014;69:e562-7. 10.1016/j.crad.2014.09.011 [DOI] [PubMed] [Google Scholar]