

Dear Editor,
Small bowel bleeding accounts for 5% of all gastrointestinal bleeding cases. Vascular lesions of the gastrointestinal tract include hemangioma, telangiectasia, angiodysplasia and phlebectasia1 and they account for 5-10% of all benign neoplasms of the small bowel.2 The diagnosis of small bowel hemangioma is not easy and different modalities with different diagnostic accuracy could be used. Considering the scarcity of information on small bowel hemangiomas, the present case report is unique as it underlines the perplexity of relying on a single diagnostic method. Written informed consent was obtained from the patient to publish this case and accompanying images in scientific journals for research and educational purposes.
In September 2014, a 40-year-old male patient referred to a physician due to fatigue and palpitation. Laboratory studies showed low hemoglobin level (Hb: 9.9 g/dl, MCV: 76 fL), low serum level of ferritin and iron, normal hemoglobin electrophoresis, and positive stool occult blood tests. The patient had no history of melena, hematochezia, or maroon color stool. Upper GI endoscopy and colonoscopy were performed and multiple biopsies including duodenal mucosa were taken, all of which were normal and inconclusive. Video capsule endoscopy for the assessment of small bowel mucosa3 revealed no abnormal finding. Subsequently, the patient was referred to our center for further investigations. Red blood cell GI bleeding scintigraphy revealed active GI bleeding, most likely from the jejunum. CT enterography study with contrast injection in the arterial phase showed a suspicious soft tissue lesion containing multiple tiny spots of calcification and vascular components in the proximal part of the jejunum (figure 1). Due to increased risk of bleeding by endoscopic sampling, the patient was referred for laparoscopic surgery. The laparoscopic finding was in favor of a small bowel hemangioma. The lesion was resected and the diagnosis of cavernous type hemangioma was confirmed by pathology studies. Microscopic examination revealed large and cavernous vascular spaces, which were partially filled with blood (figure 2). The patient did not show any evidence of GI bleeding, such as anemia and positive stool occult blood tests after the 3 and 6 months follow-up visits.
Figure 1.
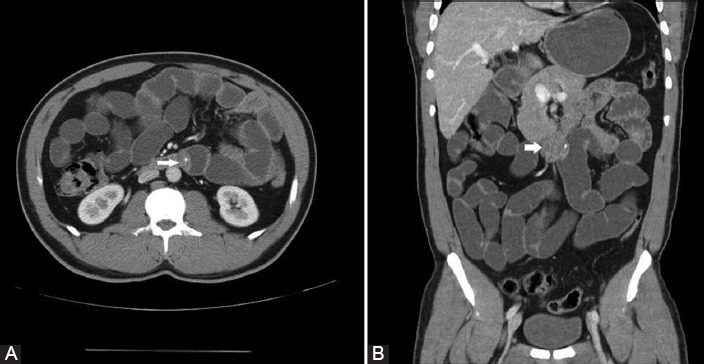
CT enterography revealed a soft tissue lesion measuring 26×12 mm with multiple tiny spots of calcifications in the proximal jejunum (white arrow) in coronal (A) and sagittal sections (B).
Figure 2.
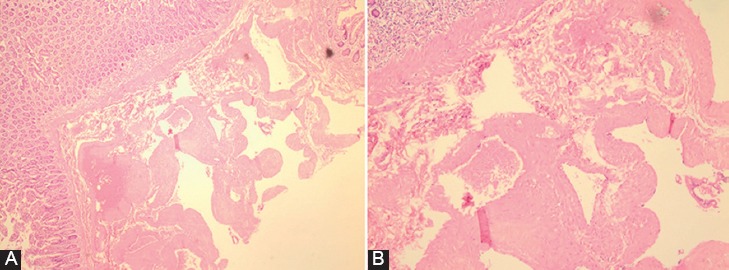
Irregular spongy mass 2×1×1 mm in the wall of the small bowel. Microscopic examination shows large and cavernous vascular spaces in submucosal layer. H&E staining ×40 (A) and H&E staining ×100 (B).
Small bowel bleeding is infrequent and accounts for 5% of all cases. Common causes include vascular lesions, neoplasia, NSAID ulcer, and inflammatory bowel diseases. Hemangioma, telangiectasia, angiodysplasia, and phlebectasia are typical forms of small bowel vascular lesions. Hemangiomas of the small bowel are generally rare and most commonly found in the jejunum.2,4 The types of hemangiomas include capillary type, cavernous type, and mixed type. The cavernous type has the highest frequency followed by the mixed type. Clinical manifestation includes bleeding presentation and surgical consequences. Chronic occult blood loss and iron deficiency anemia are the most common types of presentation,4 however, cavernous hemangioma might be large in size5 and could cause severe bleeding. Surgical complications include obstruction, intussusceptions, perforation, and intramural hematoma. The diagnosis of small intestinal hemangioma is difficult. Small bowel barium study, angiography, and RBC scan scintigraphy are useful in diagnosing 25% of cases.2 CT enterography and MRI enterography have additional diagnostic accuracy. Wireless capsule endoscopy and balloon-assisted enteroscopy are innovational diagnostic tools in this era.2,4 The diagnostic rate of wireless capsule endoscopy and balloon-assisted enteroscopy in the diagnosis of obscure GI bleeding is similar and about 38-93%. However, wireless capsule endoscopy has the highest diagnostic yield (90%) near the bleeding episode and it drops to less than 10% after two weeks. Surgery is an accepted treatment for solitary lesions in the small intestine and laparoscopy with complete resection is a procedure of choice.2
In the context of GI bleeding, bleeding of small bowel lesions is rare. However, when the upper and lower sources of bleeding have been excluded, the main culprit is the small bowel. Innovative techniques have their own limitations and a sole reliance on the negative result of each technique could be misleading. The present case report demonstrates the importance of clinical suspicion, particularly based on inconclusive results from one or two studies and if a high index of suspicion persists.
Conflict of Interest: None declared.
References
- 1.Ersoy O, Akin E, Demirezer A, Koseoglu H, Balci S, Kiyak G. Cavernous haemangioma of small intestine mimicking gastrointestinal stromal tumour. Arab J Gastroenterol. 2013;14:139–40. doi: 10.1016/j.ajg.2013.08.008. [DOI] [PubMed] [Google Scholar]
- 2.Pera M, Marquez L, Dedeu JM, Sanchez J, Garcia M, Ramon JM, et al. Solitary cavernous hemangioma of the small intestine as the cause of long-standing iron deficiency anemia. J Gastrointest Surg. 2012;16:2288–90. doi: 10.1007/s11605-012-1991-6. [DOI] [PubMed] [Google Scholar]
- 3.Gerson LB, Fidler JL, Cave DR, Leighton JA. ACG Clinical Guideline: Diagnosis and Management of Small Bowel Bleeding. Am J Gastroenterol. 2015;110:1265–87. doi: 10.1038/ajg.2015.246. quiz 88. [DOI] [PubMed] [Google Scholar]
- 4.Elias G, Toubia N. Hemangioma of the small intestine presenting with recurrent overt, obscure gastrointestinal bleeding. Clin Gastroenterol Hepatol. 2010;8(A18):Ae1. doi: 10.1016/j.cgh.2009.03.036. [DOI] [PubMed] [Google Scholar]
- 5.Fernandes D, Dionisio I, Neves S, Duarte P. Cavernous hemangioma of small bowel: a rare cause of digestive morrhage. Rev Esp Enferm Dig. 2014;106:214–5. [PubMed] [Google Scholar]