

Abstract
How does empathic physiology unfold as a dynamic process, and which aspect of empathy predicts children’s kindness? In response to empathy induction videos, 4–6 year-old children (N = 180) showed an average pattern of dynamic respiratory sinus arrhythmia (RSA) change characterized by early RSA suppression followed by RSA recovery, and modest subsequent suppression during positive resolution of the empathic event. Children’s capacity for this pattern of flexible RSA change was associated with their subjective empathic feelings, which were concurrently associated with more sympathetic and prosocial responses to others. Conversely, only children’s dynamic RSA change longitudinally predicted prosocial behavior two years later. These findings have implications for understanding the dynamic and multifaceted nature of empathy, and its relation with prosocial development.
Keywords: empathy, sympathy, prosocial behavior, dynamic RSA, subjective feelings, emotion
Empathy, the vicarious sharing of the emotions of others, is widely regarded as one of the main psychological motivators of kindness (de Waal, 2008; Eisenberg, Spinrad, & Morris, 2014). Empathizing with the suffering of another can provide the emotional impulse to engage in helpful acts meant to alleviate the other person’s suffering, and can also lead to sympathetic feelings of sorrow and concern for the person’s well-being (Eisenberg & Eggum, 2009). In theory, empathy is likely both dynamic, in the sense that it is a process that rapidly unfolds over time, and multifaceted, involving verbal and nonverbal emotional expressions (e.g. facial, vocalic, posture, body movement), subjective feelings (i.e., affective experience), and physiological changes (Hastings, Miller, Kahle, & Zahn-Waxler, 2014). Despite this rich theory, empirical work that focuses on the dynamic and multifaceted nature of children’s empathy is lacking. We know very little regarding 1) how children’s empathy unfolds as a dynamic process over time, and 2) which of empathy’s multiple facets is most closely tied to children’s kindness. This study was conducted to address these gaps in our knowledge.
Empathy as Multifaceted
Emotional processes, like empathy, are believed to involve coordinated changes in experiential, behavioral, and physiological response systems (Ekman, 1992). Simulation theories propose that, in early childhood, conscious representations of one’s own emotions (i.e., subjective empathic feelings) are particularly important for gaining information about others’ emotional states (Decety & Meyer, 2008). Empathy is also an embodied response involving changes in somatic and autonomic systems (Hastings et al., 2014; Preston & de Waal, 2002). These physiological changes contribute to subjective feelings as well as other aspects of empathic responding that can be outside of conscious awareness, like evaluation of risk and safety in the environment (Porges, 2011), which are important for maintaining social engagement and avoiding personal distress. From a functionalist perspective on emotion (Thompson, 2011), these subjective and physiological components of empathy help people to adapt to environmental demands and accomplish personal and social goals. Empathy, therefore, serves as a mechanism for facilitating one person’s positive engagement with another person who is in need (Preston & de Waal, 2002).
Well-regulated empathic responses characterized by moderate arousal rather than intense discomfort, in turn, can foster prosocial emotions and behaviors, including sympathy, an emotional state of concern and sorrow for another (Eisenberg & Eggum, 2009), and prosocial behavior meant to assist others or alleviate others’ distress. Past research has supported the perspective that empathy is a proximate mechanism of children’s sympathy and prosocial behavior (Eisenberg et al., 2014), but it is unclear whether the specific components of empathic responses differ in their importance for motivating the various aspects of prosociality. One goal of this project was to examine whether subjective empathic feelings – that is, the recognized experience of feelings that mirror the emotions of another – or bottom-up, physiological aspects of empathy are more closely linked to children’s prosocial behavior and sympathy.
Although there are many physiological changes that take place when children empathize with others, the autonomic nervous system, particularly the parasympathetic branch, is believed to play an important role in children’s empathy, sympathy, and prosocial behavior (Hastings & Miller, 2014; Miller, Kahle, & Hastings, 2015). Parasympathetic influence over cardiac activity decreases physiological arousal (e.g., lower heart rate) and promotes restorative processes in the body. Respiratory sinus arrhythmia (RSA) refers to heart rate variability that corresponds with breathing. RSA is mainly under the control of the myelinated vagus nerve, suggesting that RSA is a good proximal measure of parasympathetic nervous system (PNS) activity. RSA suppression (i.e., withdrawal of PNS influence) supports adaptive orienting and coping in response to emotionally challenging events (Porges, 2011). Conversely, in safe social contexts, RSA maintenance or augmentation (i.e., increasing PNS influence) may support calm, social engagement (Hastings et al., 2008; Porges, 2011). Given the role of RSA in orienting, emotion regulation, and social engagement, all of which are theoretically important for empathic and prosocial responding, the current study focuses on RSA as a physiological component of empathy.
Empathic Physiology as Dynamic
In addition to being multifaceted, empathy is also theorized to be a dynamic process that involves rapid changes in emotional systems over time in response to rapidly changing events in the environment (Hastings & Miller, 2014). Physiology is an important component of emotion that might correspond with or underlie other emotional processes, like subjective experience and behavior (Ekman, 1992). Contrary to viewing emotion as a dynamic process that unfolds over time, traditional techniques of quantifying PNS reactivity rely on static measures of mean change between non-affective and affective conditions (e.g., arithmetic change scores or standardized residuals). These methods have produced inconsistent findings (Hastings & Miller, 2014; Hastings et al., 2014), with both RSA suppression (Liew et al., 2011), and RSA maintenance or augmentation (Gill & Calkins, 2003: Stellar, Cohen, Oveis, & Keltner, 2015) being associated with empathy-related responding. By not effectively modeling empathy as a dynamic process, interesting and important questions have gone unaddressed in prior work. For example, how does physiology during empathy change as a process that unfolds over time? What is the direction and magnitude of change at different points in time during an empathic event?
A static change score presumes that the average RSA level during a proscribed period of time captures the most meaningful information for “state physiology”, and that only the differences in averages need to be examined. Measures of dynamic change allow for an ongoing pattern of fluctuations in PNS influence over cardiac activity during an empathic event. Thus, there have been calls for models that are more sensitive to temporal aspects of emotion to better reflect the dynamic nature of physiology (Brooker & Buss, 2010; Burt & Obradovic, 2012; Fortunato, Gatzke-Kopp, & Ram, 2013; Miller et al., 2013). For example, Miller and colleagues (2013) found that a pattern of initial decreasing RSA followed by RSA recovery during an anger-themed video stimulus predicted children’s self-control of aggression. In the present study, we built on this work by using latent growth curve analysis to model children’s dynamic RSA during an empathy induction that involved sadness-themed video stimuli.
Current Study
The current study had two main goals. First, we sought to model empathy-related RSA change as a dynamic process that unfolds over the course of viewing another person experience sadness. Second, we examined whether subjective empathic feelings or physiological reactivity during empathy, as indexed by dynamic RSA, would predict children’s kindness (prosocial behavior and sympathy) both concurrently in early childhood and longitudinally two years later. We predicted that children who shared in the emotional experiences of others (i.e., subjective empathic feelings) would be more prosocial and sympathetic. Tentatively, we hypothesized that children’s well-regulated empathic physiological responses to others’ sadness might be similar to the pattern of dynamic RSA change observed by Miller and colleagues (2013). Thus, children who demonstrated more dynamic RSA flexibility in the form of more RSA suppression followed by RSA augmentation during empathy induction were expected to be more sympathetic and prosocial toward others.
Method
Participants
Time 1
180 children were recruited for this study (95 boys, 85 girls). Children were aged 4.0 – 4.9 years (n = 98) or 6.0 – 6.9 years (n = 82) at recruitment, but four younger and eight older children turned 5 or 7 years old prior to testing. Children with identified cognitive delays or physical difficulties that would interfere with their ability to complete procedures were excluded from the study. Children were tested in the language primarily spoken in their homes (n = 146 tested in English; n = 34 tested in French). Families were predominantly Caucasian (78.7%) and middle to upper-middle socieoeconomic status in terms of annual family income (M = $79,700 CND, SD = $43,470, range from less than $10,000 to over $220,000) and mother education (M = 14.79 years, SD = 2.30). Families were recruited by direct mailing, local advertisements, and letters distributed to preschool and elementary schools.
Time 2
A follow-up assessment took place 2 years later and included 155 children (83 boys, 72 girls) from the original assessment (86.1% retention). The average age at the follow-up assessment was 7.09 years (SD = 1.13, range 6 – 9.58). Families who participated at T2 were not significantly different from families who dropped out of the study in terms of children’s age at T1, sex, ethnicity, family income, maternal education (all χ2(1) < .55; all t(178) < 1.76), or T1 measures of physiology (all t(152) < .82), empathy, and prosociality (all t(177) < 1.88).
Procedure
Children were tested in the laboratory at both time points. Data were collected from 2006 through 2009. At T1, approximately one hour into the visit, electrodes attached to an ambulatory autonomic monitor (Minilogger 2000; Mini-Mitter Inc., 1999) were placed on the child’s chest to record inter-beat intervals (IBI). Approximately 10 minutes later, children were instructed to sit quietly and watch a 7.5 minute mood induction video showing a child experiencing 5 emotional events. Following the video, children were asked to label how they felt while watching the different emotion induction vignettes. At T1 and T2, children were exposed to scripted accident simulations performed by an examiner and by the child’s mother. The mother’s accident simulation occurred approximately 100 minutes into the visit, and the examiner’s accident simulation occurred approximately 40 minutes after the mother’s simulation. Children’s responses to these accident simulations were video recorded for later coding of sympathetic concern and prosocial behavior.
Empathy induction video at T1
IBI data were recorded while children watched the Mood Induction Stimulus for Children (MISC; Hastings, Zahn-Waxler, Robinson, Usher, & Bridges, 2000; Miller et al., 2013). The MISC presented emotionally evocative stories on video, including two sadness-themed vignettes intended to induce empathy. The sadness vignettes lasted 90-seconds each, and both included six 15-sec epochs. For both vignettes, children first saw a 15-s distractor scene (first epoch) of non-emotional material (shimmering stars and soothing music). Then, children saw a 1-min narrated story that included four still images presented for 15-s each. Each story presented a child and mother experiencing sadness; the first story involved the child’s dog running away and the second story involved the child’s grandfather being very sick. For each story, the first image (second epoch) began the story and was neutral in emotional content. The second image (third epoch) introduced the sadness eliciting event, and included evocative music and both the mother and child being depicted with sad expressions, saying they were sad, and speaking in sad vocal tones. The third image (fourth epoch) was visually identical to the second, but the narration and music intensified the sad content, including the child beginning to cry. The fourth image (fifth epoch) ended the narrated story with a positive resolution. Both vignettes then concluded as they began, with the same 15-s distractor scene (sixth epoch) of non-emotional material. The MISC included two other stories between the sadness-themed stories, such that the children did not view the two scenes back-to-back.
Respiratory sinus arrhythmia
IBI data collected during the empathy inductions were edited for artifacts and outliers. RSA was computed using Porges’ algorithm (1985). The high-frequency band-pass for quantifying RSA was set to range from .24 to 1.04 Hz. Sampling rate was set at 250 Hz. RSA was calculated for each 15-s epoch corresponding with the four different sections of the sadness vignettes (neutral and emotional) and two distractor scenes that preceded and followed each vignette. 15-s is a common epoch length for developmental studies (Miller et al., 2013), and Porges’ algorithm can estimate RSA in shorter epochs both reliably and without violating statistical assumptions of nonstationarity of the IBI time series (Lewis, Furman, McCool, & Porges, 2012; Porges, 1985).
Subjective empathic feelings
Following the video, children were shown the image depicting sad content from the vignettes and were asked to report what had happened. If children did not respond, the examiner verbally described the primary event of the vignette, without identifying the emotional content (i.e., “They thought the dog had run away”; “The grandpa was very sick”). The examiner then asked children how they felt while watching the video. If children did not say a specific emotion, they were presented with a drawing of five emotional facial expressions (sad, happy, angry, scared, and neutral) and asked to point to the face that best matched how they felt during the empathy induction. Children who reported feeling neutral or another emotion other than sadness were scored as 0, those who reported feeling sadness by pointing to the sad face were scored as 1, and those who verbally reported that they felt sad during the vignette were scored as 2 (κ = .98). Children’s scores for both vignettes were averaged (r = .51, p < .001) to form a measure of subjective feelings of empathy.
Accident simulation at T1 and T2
Children’s prosocial behaviors and expressions of sympathetic concern were observed in response to 90-s accident simulations in which an adult feigned injury (Hastings et al., 2000). At T1 and T2, both an examiner and the child’s mother simulated distress and pain after pretending to injure themselves and dropping several small objects.
Prosocial behavior
Each child’s engagement in prosocial acts was coded on a 0 to 3 scale: a score of 0 reflected “none”; a score of 1 reflected “brief assistance (one pat or verbalization)”; a score of 2 reflected “moderate assistance (more than one prosocial verbalization or helping for 3–5 seconds)”; and a score of 3 reflected “prolonged assistance (more than 5 seconds of helping).” Inter-coder reliability was α = .98 and .91 for mother and examiner simulations at T1, respectively, and α = 1.00 and 1.00, respectively, at T2. Observed prosocial behavior in response to the examiner and mother accident simulations were positively correlated at both time points (r = .30, p < .001 and r = .31, p = .001 at T1 and T2, respectively). The prosocial behavior ratings were aggregated across accident simulations (mother and examiner) to form single indices of prosocial behavior at T1 and T2.
Expressions of sympathetic concern
In the first 30-s of the accident stimulations, children’s observed facial, vocal, and gestural/postural expressions of sympathetic concern were coded on a 1 to 5 scale, ranging from “absent” to “great concern, sadness clearly expressed, and sympathetic face.” Inter-coder reliability was α = .71 and .83 for mother and examiner simulations at T1, respectively, and α = .88 and .89, respectively, at T2. Observed sympathetic concern in response to the examiner and mother accident simulations were positively correlated at both time points (r = .39, p < .001 and r = .32, p < .001 at T1 and T2, respectively). The sympathy codes were aggregated across accident simulations (mother and examiner) to form single indices of sympathetic concern at T1 and T2.
Language competence at T1
The verbal subset of the Kaufman Brief Intelligence Test (KBIT; Kaufman & Kaufman, 2004) was used as a measure of children’s language development (M = 103.20, SD = 14.49). Considering that language skills might help children to verbally express subjective empathic feelings and prosociality, children’s KBIT verbal scores were included as a covariate in analyses.
Analyses
We used second-order latent growth curve (Hancock, Kuo, & Lawrence, 2001) to model children’s dynamic RSA change as a process that unfolded over the course of the sadness videos. Second-order growth curve models include latent variables at each time point (i.e., first-order factors) with multiple indicators (see Miller et al., 2013, for a similar analysis of a single video). Each empathy induction video was composed of six 15-s epochs (i.e., distractor scene, intro scene, sadness scene, intensification of sadness scene, resolution scene, distractor scene). Thus, our model included six first-order latent factors to represent each 15-s epoch of the video induction. Each first-order factor included two RSA values as manifest indicators (one for each sadness vignette). We estimated change in children’s RSA by modeling the six first-order factors (time points) as dependent on two second-order factors (intercept and slope). We estimated and compared the fit of different second-order latent growth curve models to examine which might best explain the change in children’s RSA over the course of the vignettes. We used several indices to assess model fit, including χ2, the Comparative Fit Index (CFI), the Tucker-Lewis Index (TLI), and the root mean square error of approximation (RMSEA) with a 90% confidence interval. Good model fit is indicated by low χ2 values, CFI and TLI values higher than .95, and RMSEA values lower than .06 (Hu & Bentler, 1999).
In addition to identifying how children’s RSA changed over the course of the sadness videos, we were interested in examining 1) the concurrent associations at T1 between empathy related physiology, empathic feelings, sympathetic concern, and prosocial behavior, and 2) the longitudinal relations between T1 empathy variables and T2 sympathetic concern and prosocial behavior. We used a structural equation model to allow the second-order factors explaining children’s dynamic change in RSA (i.e., intercept and slope), reported empathic feelings, T1 sympathetic concern, T1 prosocial behavior, sex, age, and KBIT verbal scores, to all covary with each other. In addition, we included all of these T1 variables as predictors of T2 sympathetic concern and T2 prosocial behavior.
At T1, there were incomplete data for 36 children due to experimenter or mother error during the accident simulations, experimenter error during the collection of children’s reported subjective empathic feelings, or lack of useable cardiac data. At T2, there were incomplete data for 27 children due to experimenter or mother error during the accident simulations. Thus, there were 144 children with complete data at T1 and 128 children with complete data at T2. For our structural equation models, full information maximum likelihood estimation (FIML) was used to estimate all model parameters and treat missing data.
Results
Descriptive Statistics
The descriptive statistics for RSA during each empathy induction video are presented in Table 1. Children showed more observed sympathetic concern at T2 (M = 2.65, SD = .84) than T1 (M = 2.08, SD = .94), t(154) = 6.65, p < .001. Children’s prosocial behavior at T1 (M = 1.76, SD = .1.11) and T2 (M = 1.89, SD = .1.12) did not differ, t(154) = 1.20, p = .23. Regarding subjective empathic feelings at T1, the mean score was 1.08 (SD = .81), with 25.7% of children not reporting sadness in response to either video (M = 0.0), 36.6% of children verbally reporting feeling sad in response to both videos (M = 2.0), and 37.7% of children having mixed responses to the two videos (M = 0.5 – 1.5).
Table 1.
Descriptive Statistics for Respiratory Sinus Arrhythmia (RSA) During the Empathy Induction Videos
| Video 1 (Lost Dog) | Video 2 (Sick Grandfather) | |||||
|---|---|---|---|---|---|---|
|
| ||||||
| Epoch | M | SD | Range | M | SD | Range |
| 1. Stars | 6.47 | 1.34 | 3.16–9.07 | 6.33 | 1.67 | 1.97–10.71 |
| 2. Intro | 6.34 | 1.49 | 2.61–9.97 | 6.37 | 1.58 | 2.60–10.38 |
| 3. Sad 1 | 6.11 | 1.51 | 2.19–9.22 | 6.27 | 1.51 | 2.46–9.48 |
| 4. Sad 2 | 6.50 | 1.38 | 3.12–9.57 | 6.40 | 1.60 | 3.01–10.38 |
| 5. End | 6.21 | 1.32 | 3.06–9.64 | 6.26 | 1.58 | 2.09–10.09 |
| 6. Stars | 6.35 | 1.58 | 2.39–10.12 | 6.20 | 1.53 | 2.26–9.88 |
Modeling Physiological Empathy
We compared second-order linear, no-growth, and latent basis models to determine which model best explained change in RSA over the course of the sadness videos. Attempting to fit the linear model (second-order latent slope factor loadings: 0, 1, 2, 3, 4, 5) produced an error message that the covariance matrix was not positive definite. The no-growth model, without a second-order latent slope factor, provided acceptable fit to the data, χ2(70, N = 180) = 130.64, p = .000, CFI = .96, TLI = .95, RMSEA = .07 (90% confidence interval: .05, .09). The second-order latent basis model provided good overall fit to the data, χ2(63, N = 180) = 96.44, p = .004, CFI = .98, TLI = .97, RMSEA = .05 (90% confidence interval: .03, .08), and showed significantly better fit than the no-growth model according to a chi-square difference test, χ2(7, N = 180) = 34.21, p < .001. The epochs from the first sadness video (lost dog) were selected as the scale indicators for each first-order factor (loadings constrained to 1), and we freely estimated the first-order factor loadings for the second sadness video (sick grandfather). The loadings ranged from .97 to 1.01. Thus, to present a more parsimonious model, these loadings were constrained to 1; this model did not differ significantly from a model with freely estimated loadings for the first-order factors, χ2(6, N = 180) = 10.18, p = .12.
This model was used to define children’s dynamic RSA change during the sadness videos and is presented in Figure 1. To fit a latent basis model, two time points must be assigned slope factor loadings. The intercept was set to represent children’s RSA during the first distractor scene (epoch 1) by setting the slope factor loading for the first time point to 0. Examining the RSA means for each epoch of the sadness videos, children’s RSA was significantly lower during the 15-s scene introducing the sad material (epoch 3) than during the other epochs. Thus, we constrained the slope factor loading for the third time point to −1 to represent RSA suppression from the distractor scene (epoch 1) to the introduction of sadness scene (epoch 3). The slope factor loadings for the other time points (epochs 2, 4, 5, and 6) were freely estimated to allow the modeling of a potential nonlinear shape trajectory of RSA change over the course of the videos. This second-order latent basis model was used in subsequent analyses.
Figure 1.
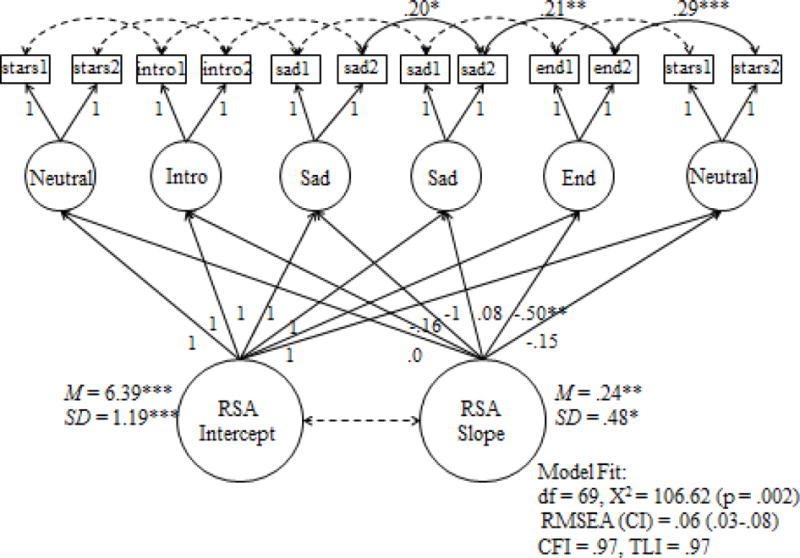
Second-order latent basis growth curve model defining children’s dynamic RSA during the empathy induction videos.
Note. ***p < .001, **p < .01, *p < .05.
The estimated means of the intercept and slope were significant. The intercept (M = 6.39, p < .001) represents the average RSA value during the first distractor scene (epoch 1). The slope value (M = .24, p = .001), multiplied by each slope loading for each time point (0, −.16, −1, .08, −.50, −.15), represents the average RSA trajectory over the course of the sadness videos. The intercept and slope were not correlated (r = .15, p = .35). The average RSA trajectory (see Figure 2) revealed a pattern of nonlinear RSA change characterized by early RSA suppression during the introduction of sad content (epoch 3), followed by RSA recovery during the continuation of sad content (epoch 4), then modest RSA suppression during the resolution of the sad event (epoch 5), and a return to initial levels during the second distractor scene (epoch 6). There was also significant variance in the intercept (SD = 1.19, p < .001) and slope (SD = .48, p = .02) factors, demonstrating that there were meaningful individual differences in children’s RSA level at the beginning of the empathy induction, and in how children’s RSA changed over the course of the empathy induction. Children with stronger slopes showed a more pronounced pattern of initial RSA suppression, recovery, and subsequent suppression during positive resolution, whereas children with weaker slopes may have had either flatter curves with less change, or patterns of change that deviated in other ways.
Figure 2.
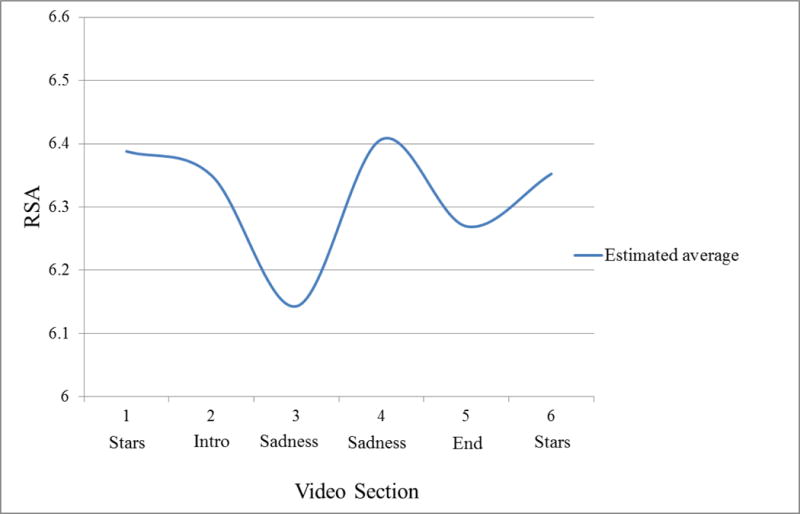
Average trajectory of dynamic RSA change over the course of the empathy induction videos.
Predicting Prosocial Behavior and Sympathetic Concern
The intercept and slope of RSA, and children’s reported subjective empathic feelings, were used as predictors and covariates in a second model examining the concurrent relations at T1 between physiology, sympathetic concern, and prosocial behavior, and the predictive relations between T1 variables and T2 sympathetic concern and prosocial behavior at T2 (see Figure 3). Age, sex, and KBIT verbal scores were also included in the model as concurrent covariates and longitudinal predictors; although they are not shown in Figure 3 in order to improve clarity of the focal paths, significant links between age, sex, and verbal ability are described in the text. Additionally, RSA intercept was not significantly related to any other measures and is not depicted in Figure 3, although it was included in the statistical model. This model showed good fit to the data, χ2(150, N = 180) = 192.23, p = .011, CFI = .97, TLI = .96, RMSEA = .04 (90% confidence interval: .02, .06).
Figure 3.
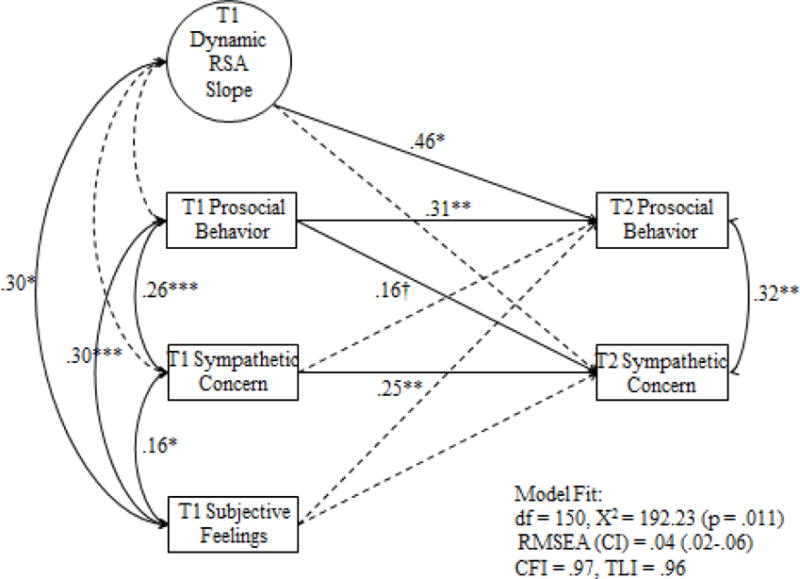
Model with concurrent and longitudinal associations between T1 RSA slope during empathy, T1 subjective empathic feelings, and T1 and T2 observed sympathetic concern and prosocial behavior.
Note. ***p < .001, **p < .01, *p < .05, †p < .10. Standardized beta weights are presented for the significant paths. Dotted lines are non-significant paths. Paths for RSA intercept, sex, age, and KBIT verbal were included in the statistical model but are not presented in the figure.
Effects for sex, age, and verbal ability
Concurrently at T1, girls were more likely to report experiencing sadness during the empathy induction (r = .25, p < .001), scored higher on the KBIT verbal test (r = .20, p = .02), and tended to show more prosocial behavior at T1 (r = .14, p = .06) than boys. Older children were also more likely to report feeling sad (r = .23, p = .003) and showed more prosocial behavior (r = .19, p = .01) at T1 than younger children. Children who scored higher on the KBIT verbal test were more likely to report experiencing sadness (r = .22, p = .008). There were no significant associations between sex, age, and verbal ability with RSA, T2 prosocial behavior, or sympathetic concern at T1 or T2.
Concurrent links between empathic and prosocial measures
The latent slope of RSA was significantly correlated with subjective empathic feelings (r = .30, p = .04). Children who showed more flexible RSA change in the form of more initial RSA suppression, more subsequent RSA augmentation, followed by more RSA suppression during the positive resolution, were more likely to report having felt sad. Subjective reports of sadness were linked to more sympathetic concern (r = .16, p = .04) and prosocial behavior (r = .30, p < .001) in response to the accident simulations. Children who expressed more sympathetic concern also engaged in more prosocial behaviors (r = .26, p < .001).
Because these results raised the possibility that children’s subjective empathic feelings may have acted as a mediator between the more instantaneous dynamic RSA responses and the T1 prosocial measures, we examined these potential indirect effects in a supplementary model. This differed from the preceding model in that the Time 1 measures were modeled as direct paths, rather than correlations. The direct effects of the latent slope of RSA on prosocial behavior and sympathetic concern were not significant before or after controlling for subjective empathic feelings (all ps > .18), and were therefore dropped from the model. The latent slope of RSA predicted subjective empathic feelings at the trend level (β = .30, p = .067). In turn, subjective empathic feelings positively predicted T1 prosocial behavior (β = .30, p < .001) and sympathetic concern (β = .16, p = .030). The indirect effects were computed as the product of the path coefficients linking dynamic RSA to subjective empathic feelings and linking subjective empathic feelings to prosocial behavior and sympathetic concern. We used the Sobel test to test the statistical significance of the indirect effects. Given our expectation of positive indirect effects – seeing that the physiological and subjective responses are positively interrelated facets of the experience of empathy – we used one-tailed hypothesis testing. The latent slope of RSA indirectly predicted prosocial behavior (β = .09, p = .047) and tended to indirectly predict sympathetic concern (β = .05, p = .081) through children’s subjective empathic feelings. Children with higher RSA slope values were more likely to report having felt sad and, in turn, were observed to be more prosocial and sympathetic.
Predictive links between T1 empathic and T2 prosocial measures
The individual differences in children’s observed responses to the accident simulations were stable. Children who showed more sympathetic concern and prosocial behavior at T1 were likely to show more concern and prosocial behavior at T2 (β = .25, p = .002 and β = .31, p = .002, respectively). Prosocial behavior at T1 also tended to predict more sympathetic concern at T2 (β = 16, p = .07), and at T2, children who were more sympathetic were also more prosocial (r = .32, p = .007). Over and above the stability of prosocial behavior, the latent slope of RSA at T1 predicted more prosocial behavior at T2 (β = .46, p = .04).
What parts of the dynamic RSA slope mattered most?
In a follow up analysis, we tested whether RSA change during specific parts of the sadness videos were particularly important for subjective empathic feelings and observed responses. In SEM, we replaced the latent growth curve with standardized residuals to represent epoch to epoch changes in RSA (i.e., epoch 1 to 2, epoch 2 to 3, epoch 3 to 4, epoch 4 to 5, and epoch 5 to 6). Greater RSA augmentation from epoch 3 to 4 (i.e., during intensification of sadness in videos) was associated with more subjective empathic feelings at T1 (r = .19, p = .02) and predicted more prosocial behavior at T2 (β = .29, p = .002). Greater RSA suppression from epoch 4 to 5 (i.e., during positive resolution in videos) was associated with more observed sympathetic concern at T1 (r = −.18, p = .03) and tended to predict more sympathetic concern at T2 (β = −.15, p = .09). No other change components, including the initial RSA suppression from epoch 2 to 3 (i.e., beginning of sad content), were uniquely associated with the subjective empathic feelings, sympathetic concern and prosocial measures. It is worth noting that the associations between RSA and other variables were generally stronger in the model including dynamic RSA slope than were evident in the model including epoch to epoch changes using standardized residuals.
Discussion
Studying the dynamic and multifaceted nature of empathy can better our understanding of how it contributes to children’s development of kindness. The use of traditional static measures of physiological reactivity in previous research has overlooked how children’s empathy may quickly unfold over brief periods in response to the sadness of others. Furthermore, empathic arousal has been hypothesized to promote sympathy and prosocial actions, but it has been unclear which aspect of empathy is most predictive of children’s concern and care for others. Our findings indicate that children’s empathy related RSA changes can be modeled as a dynamic process, characterized by increasing and decreasing RSA at different points in time during an empathic event. Furthermore, we found that the subjective feelings component of empathic sadness was linked to children’s concurrent observed sympathetic concern and prosocial behavior in early childhood, but that specific patterns of dynamic, flexible RSA changes in response to sadness in others were longitudinally predictive of the development of prosocial behavior into middle childhood.
By using a latent basis growth curve approach, we were able to model an average pattern of children’s dynamic RSA change over the course of empathy induction videos. The pattern of change for our sample was nonlinear in shape; on average, children showed strong decreasing RSA during the initial introduction of sadness, followed by strong RSA recovery during the intensification of sadness, followed by a more modest decrease during the positive resolution, and then recovery such that they returned to initial RSA levels by the end of the video stimuli. Previous research on the autonomic psychophysiology of children’s prosocial development relied on measures of mean RSA change from a baseline (Gill & Calkins, 2003; Liew et al., 2011). These measures assume that physiological reactivity is linear, and that its meaningful relation with children’s prosociality is represented in the mean level changes in PNS activity. In comparison, our method provided a more nuanced picture of dynamic RSA activity during an empathic experience that is closer to theoretical depictions of emotion as rapidly changing in response to salient events as they unfold in the environment (Thompson, 2011). Thus, our findings provide support for an alternative view of physiological reactivity that focuses on a more fine-grained level of temporal analysis. Physiological reactivity during empathy, as well as in other kinds of emotional contexts, may be best characterized by nonlinear change.
At T1, children who reported matching the sadness displayed in the videos were concurrently observed to be more sympathetic and prosocial, and also had stronger dynamic RSA changes. These findings suggest that a specific pattern of flexible PNS reactivity while viewing sadness in others supports children’s subjective empathic experience, and that this subjective aspect of empathy may be a proximal motivator of young children’s preparedness to engage in prosocial behavior and show sympathy for others. Indeed, our mediation model partially supported this inference, as there was an indirect path between children’s dynamic RSA slopes and their prosocial behaviors via their subjective empathy. The indirect path predicting children’s sympathetic expressions was in the same direction, but fell short of significance. Young children’s conscious awareness of their own feelings of empathic sadness might be an important step in transforming empathically-aroused neurobiological responses into other-oriented sympathetic concern and helping (de Waal, 2008). This echoes prior research showing that empathy mediates the link between such factors as parenting behavior and children’s prosocial behavior (Padilla-Walker & Christensen, 2011). However, given the time that passed between the video empathy induction technique and the accident simulation procedure, it should be noted that our measures of empathic sadness could not have been the direct and proximal causes of prosocial behavior and sympathy. Rather, we are interpreting the earlier physiological and subjective empathy measures as indicators of the children’s likely empathic responses in the context of the later accident simulation. In addition, given that the measure of sympathy may have included children’s displays of empathic mirroring of the adults’ distressed emotions, more clearly distinguishing empathy from sympathy will be an important challenge for future observational studies.
Children’s subjective empathy did not appear to make a lasting contribution to their kind responses over the subsequent two years. Conversely, their early flexible disengagement and reengagement of the PNS during empathy predicted their prosocial development into middle childhood. The literature on RSA in relation to prosociality is mixed, with studies linking either RSA suppression or RSA augmentation to empathy-related responding (Gill & Calkins, 2003; ; Liew et al., 2011; Stellar et al., 2015), depending to an extent on the contexts or procedures used to elicit RSA responses (Miller & Hastings, in press). Our study helps to bridge past discrepant findings by showing that both decreasing and increasing RSA are important for children’s empathy, but at different points in time during an empathic event. To the extent that RSA suppression reflects orienting upon a salient stimulus and preparing to mobilize resources for coping (Porges, 2011), children’s initial decrease in RSA during empathy may support attending to the distress of others as emotionally salient stimuli and increasing empathic physiological arousal. Subsequent RSA recovery as the sadness cues persist could promote children’s evaluation of the environment as not personally threatening (either consciously or non-consciously), thus allowing for calm, prosocial engagement (Porges, 2011). The modest RSA suppression observed during the positive resolution section of the empathy induction videos may reflect children’s sensitivity to and recognition of the alleviation of the others’ distress, followed by a recovery to initial RSA levels when presented with a neutral slide. This sequence suggests that the parasympathetic component of empathy for sadness unfolds as a process that supports early orienting, attending, and arousal, then calm, social engagement with the distress of others, followed by attention to the positive resolution of others’ distress and their recovery of well-being as a salient event. This is a marked departure from the inferences that have been drawn from the use of traditional RSA change scores, which have constrained earlier thinking about empathy as being a function of either increasing or decreasing RSA, rather than both.
Adopting this nonlinear perspective on positive physiological response to emotionally evocative events suggests that healthy physiological reactivity might be better re-conceptualized as healthy patterns of physiological flexibility. The observed pattern of flexibility (i.e., early RSA suppression, followed by RSA recovery, and modest subsequent RSA suppression) may tap into children’s ability to effectively adjust their physiology to meet the changing demands of changing environments (Berntson & Cacioppo, 2007). It is exciting to note that a very recent publication from another laboratory also found that a similar pattern of dynamic RSA change (i.e., early RSA suppression followed by RSA recovery) to a video stimulus was associated with adolescents’ prosocial behavior (Cui et al., 2015). But, in our study, why would physiology at T1 be concurrently associated with feelings, but longitudinally predictive of behavior? The capacity to demonstrate this pattern of dynamic RSA change in childhood may represent effective emotion regulation that promotes the development of prosocial behavior over time. In early childhood, emotion sharing and imitation processes (e.g., subjective empathic feelings) are foundational mechanisms for understanding and affiliating with others (Decety & Meyer, 2008), such that mirroring the sad feelings of others might be the primary motivator for feeling concern and providing care for others. With maturation, children may come to rely on other aspects of empathy for motivating prosociality. From this perspective, our measure of dynamic and flexible RSA changes may characterize a well-regulated experience of empathic emotion that older children can effectively act upon to engage positively with others. This may presume that the patterns of dynamic RSA change were stable over time, which would need to be confirmed in future studies. Given that similar patterns have been observed and related to prosocial behavior in adolescents (Cui et al., 2015), this is a reasonable expectation.
It should be noted that children’s RSA recovery during the intensification of sadness (i.e., RSA augmentation from epoch 3 to 4) was the most salient aspect of RSA change for predicting children’s concurrent subjective empathic feelings and subsequent prosocial behavior. Thus, although the dynamic slope of RSA accounted for more variance in children’s future prosociality than did the epoch to epoch changes, our findings are in line with the perspective that RSA augmentation plays an important role in fostering calm, social engagement that is important for providing help to others (Hastings & Miller, 2014; Porges, 2011). It is also noteworthy that the most emotionally evocative epochs of the videos were the strongest contributors to the shape of dynamic RSA change, supporting our contention that empathy-related physiological changes drove the significant associations between the RSA slope and children’s subjective empathic feelings and prosocial behavior. Of course, physiological and subjective responses to video depictions of events may not exactly parallel the reactions that children have when directly interacting with others. Greater support for our interpretation could come from future research examining RSA and subjective feelings in contexts in which children have the opportunity to directly help others they see in distress.
Whereas dynamic RSA was measured during the sadness video stimuli, children’s subjective empathic feelings were measured in retrospect after the video had ended and we’re not measured in a dynamic fashion; this may have detracted from the predictive utility of subjective feelings. Studying children’s subjective feelings as an unfolding process could be an interesting direction for future research. As well, although repeated observations of behavior allowed us to predict the development of prosociality, physiology and subjective feelings were only measured once. Future longitudinal research with repeated measures of physiology, feelings, and prosociality will be necessary to clearly illustrate any developmental changes in the empathic underpinnings of prosocial responses.
Conclusions
We examined multiple aspects of empathy (i.e., subjective feelings and physiology) as motivators of children’s observed kindness (i.e., sympathetic concern and prosocial behavior), both concurrently and longitudinally. Empathy was assessed across multiple videos, and kindness was observed across multiple partners, such that the associations we documented cannot be attributed to specific elements of the stimuli children saw or their relationships with the distressed adults. We also used a novel methodology to model multiple physiological states at different points during an empathic episode as a single physiological process underlying empathy. Our findings should serve to resolve notable discrepancies and gaps in the literature on prosocial development. Specifically, we showed that different facets of empathy are more predictive of young children’s concurrent versus future kindness, and that effective PNS reactivity during empathy is not simply a function of RSA suppression or augmentation, but can instead be better captured by the concept of dynamic PNS flexibility – showing specific kinds of RSA changes at different points in time during an empathic event.
In theory, a dynamic and multifaceted experience of empathy should represent an important step in a cascade of events that can lead to sympathy and prosocial behavior. However, few researchers have empirically studied the widely hypothesized link between empathy and kindness using methods that allow for consideration of both multiple components of empathy, and empathic physiology as a dynamic process that unfolds over time. Our study provides a promising step towards narrowing the gap between theory and research on empathy and prosociality. We found children’s dynamic RSA during empathy to be characterized by both RSA suppression and augmentation at different points in time, perhaps reflecting orientation to the distress of others, followed by calm social engagement, followed by attention to the resolution of others’ distress. Children who showed more of this pattern of flexible and dynamic RSA reported feeling more empathic sadness and demonstrated more prosocial behavior two years later in response to adults in distress. Conversely, children’s empathic matching of subjective feelings of sadness was concurrently linked to their displays of sympathetic concern and acts of kindness. These findings provide a nuanced and rich understanding of the nature of children’s empathy and prosocial development. Improving our ability to assess and model emotions as multifaceted and dynamic processes will continue to be an important avenue of future work.
Acknowledgments
This research was supported by a Canadian Institutes of Health Research grant to Paul D. Hastings and National Institute of Mental Health Predoctoral Fellowship T32-MH20006 to Jonas G. Miller.
References
- Berntson GG, Cacioppo JT. Integrative physiology: Homeostasis, allostasis, and the orchestration of systematic physiology. In: Cacioppo JT, Tassinary LG, Berntson GG, editors. Handbook of psychophysiology. 3rd. Cambridge, England: Cambridge University Press; 2007. pp. 433–452. [Google Scholar]
- Brooker RJ, Buss KA. Dynamic measures of RSA predict distress and regulation in toddlers. Developmental Psychobiology. 2010;52:372–382. doi: 10.1002/dev.20432. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burt KB, Obradovic J. The construct of psychophysiological reactivity: Statistical and psychometric issues. Developmental Review. 2013;33:29–57. doi: 10.1016/j.dr.2012.10.002. [DOI] [Google Scholar]
- Cui L, Morris AS, Harrist AW, Larzelere RE, Criss MM, Houltberg BJ. Adolescent RSA responses during an anger discussion task: Relations to emotion regulation and adjustment. Emotion. 2015;15:360–372. doi: 10.1037/emo0000040. [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Waal FBM. Putting the altruism back into altruism: The evolution of empathy. Annual Review of Psychology. 2008;59:279–300. doi: 10.1146/annurev.psych.59.103006.093625. [DOI] [PubMed] [Google Scholar]
- Decety J, Meyer M. From emotion resonance to empathic understanding: A social developmental neuroscience account. Development and Psychopathology. 2008;20:1053–1080. doi: 10.1017/S0954579408000503. [DOI] [PubMed] [Google Scholar]
- Eisenberg N, Eggum ND. Empathic responding: Sympathy and personal distress. In: Decety J, Ickes W, editors. The social neuroscience of empathy. Cambridge, MA: MIT press; 2009. pp. 63–88. [Google Scholar]
- Eisenberg N, Spinrad T, Morris A. Empathy-related responding in children. In: Killen M, Smetana J, editors. Handbook of moral development. 2nd. New Jersey: Lawrence Erlbaum; 2014. pp. 184–207. [Google Scholar]
- Ekman P. An argument for basic emotions. Cognition and Emotion. 1992;6:169–200. doi: 10.1080/02699939208411068. [DOI] [Google Scholar]
- Fortunato CF, Gatzke-Kopp LM, Ram N. Associations between respiratory sinus arrhythmia reactivity and internalizing and externalizing symptoms are emotion specific. Cognitive and Affective Behavioral Neuroscience. 2013;13:238–251. doi: 10.3758/s13415-012-0136-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gill KL, Calkins SD. Do aggressive toddlers lack concern for others? Behavioral and physiological indicators of empathic responding in 2-year-old children. Development and Psychopathology. 2003;15:55–71. doi: 10.1017/s095457940300004x. [DOI] [PubMed] [Google Scholar]
- Hancock GR, Kuo WL, Lawrence FR. An illustration of second-order latent growth models. Structural Equation Modeling. 2001;8:470–489. doi: 10.1207/S15328007SEM0803_7. [DOI] [Google Scholar]
- Hastings PD, Miller JG. Autonomic regulation, Polyvagal Theory, and children’s prosocial development. In: Padilla-Walker L, Carlo G, editors. Prosocial development: A multidimensional approach. New York: Oxford University Press; 2014. pp. 112–127. [Google Scholar]
- Hastings PD, Miller JG, Kahle S, Zahn-Waxler C. The neurobiological bases of empathic concern for others. In: Killen M, Smetana J, editors. Handbook of moral development. 2nd. New Jersey: Lawrence Erlbaum; 2014. pp. 411–434. [Google Scholar]
- Hastings PD, Nuselovici JN, Utendale WT, Coutya J, McShane KE, Sullivan C. Applying the polyvagal theory to children’s emotion regulation: Social context, socialization, and adjustment. Biological Psychology. 2008;79:299–306. doi: 10.1016/j.biopsycho.2008.07.005. [DOI] [PubMed] [Google Scholar]
- Hastings PD, Zahn-Waxler C, Robinson J, Usher B, Bridges D. The development of concern for others in children with behavior problems. Developmental Psychology. 2000;36:531–546. doi: 10.1037/0012-1649.36.5.531. [DOI] [PubMed] [Google Scholar]
- Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling. 1999;6:1–55. doi: 10.1080/10705519909540118. [DOI] [Google Scholar]
- Kaufman AS, Kaufman NL. Manual for the Kaufman Brief Intelligence Test-Second edition (KBIT-2) Circle Pines, MN: American Guidance Service; 2004. [Google Scholar]
- Lewis GF, Furman SA, McCool MF, Porges SW. Statistical strategies to quantify respiratory sinus arrhythmia: Are commonly used metrics equivalent? Biological Psychology. 2012;89:349–364. doi: 10.1016/j.biopsycho.2011.11.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Liew J, Eisenberg N, Spinrad TL, Eggum ND, Haugen RG, Kupfer A, Baham ME. Physiological regulation and fearfulness as predictors of young children’s empathy-related reactions. Social Development. 2011;20:111–134. doi: 10.1111/j.1467-9507.2010.00575.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller JG, Chocol C, Nuselovici JN, Utendale WT, Simard M, Hastings PD. Children’s dynamic RSA change during anger and its relations with parenting, temperament, and control of aggression. Biological Psychology. 2013;92:417–425. doi: 10.1016/j.biopsycho.2012.12.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller JG, Kahle S, Hastings PD. Roots and benefits of costly giving: Children who are more altruistic have greater autonomic flexibility and less family wealth. Psychological Science. 2015;26:1038–1045. doi: 10.1177/0956797615578476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miller JG, Hastings PD. Biopsychosocial models of prosociality: Compassionate love, vagal regulation, and children’s altruism. In: Narvaez D, Braungart-Rieker J, Miller L, Gettler L, Hastings PD, editors. Contexts for Young Child Flourishing: Evolution, Family and Society. New York: Oxford University Press; in press. [Google Scholar]
- Mini-Mitter Company, Inc. Mini-logger series 2000. Sunriver, OR: Author; 1999. [Google Scholar]
- Padilla-Walker LM, Christensen KJ. Empathy and self-regulation as mediators between parenting and adolescents’ prosocial behavior toward strangers, friends, and family. Journal of Research on Adolescence. 2011;21:545–551. doi: 10.1111/j.1432-7795.2010.00695.x. [DOI] [PubMed] [Google Scholar]
- Porges SW. patent number; 4,510,944. Washington, DC: US Patent Office; Method and apparatus for evaluating rhythmic oscillations in periodic physiological response systems. 1985
- Porges SW. The polyvagal theory. New York: Norton & co; 2011. [Google Scholar]
- Preston SD, de Waal FBM. Empathy: Its ultimate and proximate bases. Behavioral and Brain Sciences. 2002;25:1–72. doi: 10.1017/S0140525X02000018. [DOI] [PubMed] [Google Scholar]
- Stellar JE, Cohen A, Oveis C, Keltner D. Affective and physiological responses to the suffering of others: Compassion and vagal activity. Journal of Personality and Social Psychology. 2015;108:572–585. doi: 10.1037/pspi0000010. [DOI] [PubMed] [Google Scholar]
- Thompson RA. Emotion and emotion regulation: Two sides of the developing coin. Emotion Review. 2011;3:53–61. doi: 10.1177/1754073910380969. [DOI] [Google Scholar]