

Abstract
Purpose:
The purpose of this study was to evaluate conventional acupuncture therapy in the management of clinical outcomes for temporomandibular disorders (TMD) in adults.
Methods:
The electronic databases PubMed, EMBASE, Cochrane Central Register of Controlled Trials, and Clinical Trails.gov were searched for reports published until March 31, 2016.
Results:
Nine eligible studies from 8 publications involving 231 patients were included in the meta-analysis. A comparison of the main outcome of visual analog scale (VAS) values of pain between the acupuncture group and control group showed a significant decrease (MD = −0.98, 95% CI [−1.62, −0.34], I2=54%, P = 0.003) in the VAS following acupuncture treatment. However, subgroup analysis according to the type of sham control group indicated that there were significant differences in the results when sham acupuncture was used as the control group (MD = −1.54, 95% CI [−2.63, −0.45], I2=58%, P = 0.006) as well as when sham laser treatment was used as the control group (MD = −1.29, 95% CI [−2.32, −0.27], I2 = 0%, P = 0.01). However, there was no significant difference when the splint treatment group was used as the control group (MD = −0.09, 95% CI [−0.69, 0.50], I2 = 0%, P = 0.76). Subgroup analyses of VAS for pain by the classification of diseases indicated that the myogenous TMD subgroup demonstrated a significant difference (MD = −1.49, 95% CI [−2.45, −0.53], I2 = 47%, P = 0.002), and TMD showed no statistically significant difference (MD = −0.42, 95% CI [−1.14, 0.30], I2 = 46%, P = 0.25). Subgroup analysis according to whether the subgroup penetrated the skin showed that nonpenetrating sham acupuncture as the control group showed a significant difference (MD = −1.56, 95% CI [−2.70, −0.41], I2 = 58%, P = 0.008) compared with the conventional acupuncture as the treatment modality, while penetrating sham acupuncture as the control group showed no significant difference (MD = −1.29, 95% CI [−3.40, 0.82], I2 = not applicable, P = 0.23). No publication bias was observed considering the symmetry of the funnel plots.
Conclusions:
Our results indicate that conventional acupuncture therapy is effective in reducing the degree of pain in patients with TMD, especially those with myofascial pain symptoms.
Keywords: acupuncture, meta-analysis, temporomandibular disorders, VAS of pain
1. Introduction
Temporomandibular disorder (TMD) is a nonspecific diagnosis that represents a group of often painful and/or dysfunctional conditions involving the muscles of mastication and/or the temporomandibular joint (TMJ).[1] Epidemiological studies have shown that approximately 10% of the population is affected, and 30-year-old women are most likely to be affected by TMD.[2,3] The main signs and symptoms of TMD include TMJ clicking, acute or chronic myofascial or oral masticatory muscle pain, tenderness of the masticatory muscles, and abnormal jaw movements.[4–6]
The exact etiology of TMD is difficult to identify, but some studies have found the following contributing factors: occlusal abnormalities, psychological stress, orthodontic treatment, microtrauma, poor health and nutrition, joint laxity, and exogenous estrogen.[7,8] The American Academy of Orofacial Pain[9] classification system divides TMD into 2 groups: myogenous TMD, which is related to masticatory muscle disorders, and arthrogenous TMD, which is related to the TMJ itself. Epidemiological studies have shown that most TMD patients are diagnosed with myofascial pain.[10]
Currently, there is a lack of consensus regarding the most efficacious treatment approach for TMD because of its multifactorial nature. Various treatments have been implemented for the treatment of TMD, including pharmacological therapy, psychological therapy, occlusal therapy, physical therapy, cognitive therapy, acupuncture therapy, and surgical interventions.[11–14] In cases of myofascial pain, strategies often target muscle relaxation.[5] Acupuncture is a commonly used strategy for pain relief in these cases, in which an acupuncture needle or, more often, multiple needles are inserted at the appropriate acupuncture points.[15–17] Therefore, we performed this meta-analysis to elucidate the properties of acupuncture by comparing the clinical effects of acupuncture for the treatment of TMD through combining all of the relevant clinical studies.[18] This meta-analysis was conducted according to the Preferred Reporting items for Systematic Reviews and Meta-analysis statement.[19]
2. Materials and methods
2.1. Search strategy
We conducted a search of 4 electronic databases, namely PubMed, EMBASE, the Cochrane Central Register of Controlled Trials, and Clinical Trails.gov, from the building database until March 31, 2016, for eligible randomized or parallel-group design clinical trials that evaluated the effectiveness of acupuncture therapy in patients with TMD. The following Medical Subject Headings (MeSH) and text words were used: “temporomandibular,” “temporomandibular disorders,” “TMD,” “temporomandibular joint disorders,” “TMJ,” and “acupuncture.”
2.2. Literature selection and exclusion
All of the studies were selected in accordance with the following inclusion criteria: randomized or parallel-group design clinical trial, including only TMD patients older than 18 years, comparing the effectiveness of acupuncture therapy, including only patients diagnosed with TMD (including but not limited to: osteoarthritis, TMJ clicking or anterior disc displacement with or without reduction), including patients who have not received any TMD treatment prior to the study, and investigating one of the following outcomes: ① a change in the visual analog scale measurement (VAS) for pain, ② a change in maximum mouth opening (MMO) without examiner intervention, ③ a change in the VAS of masseter muscle tenderness upon palpation, or ④ a change in the VAS of functional impairment. The change in the VAS score for pain was the main outcome investigated, and the others were secondary outcomes.
Studies were excluded in accordance with the following criteria: if pain at rest was used as the pain score, the study was a duplicate, the data cannot be extracted or obtained through contact with the author, and too little information to calculate the missing standard deviations (SD) was provided.
2.3. Data extraction
The relevant information, including the study design, patient characteristics, interventions, comparisons, and outcomes, was independently extracted and entered into a database by 2 of the investigators. When the relevant research information was missing, particularly the study design or outcome information, we contacted the original authors for clarification.
Disagreements between the 2 authors regarding data extraction were resolved by discussion. If the dispute persisted, other senior investigators were consulted to attain a consensus.
2.4. Statistical analysis
When describing all of the outcomes based on continuous data under a unified measurement standard, we used the weighted mean difference (MD),[20] 95% confidence interval (CI) and P≤0.05; otherwise, the standardized mean difference (SMD), 95% confidence interval (CI) and P≤0.05 were employed. All of the outcome data were processed using RevMan 5.3 (Cochran Collaboration, London, UK) software. All of the missing SDs were estimated from the relevant P values.[21] We performed a statistical test for heterogeneity[22] and adopted an I2 greater than 50% as evidence for heterogeneity according to the Cochrane handbook.[20] If the data were homogeneous under a fixed-effects model, the 3 confounding factors, including the type of sham control group, classification of diseases, and the control group according to whether to penetrate the skin, were identified as the key sources of heterogeneity in the main outcomes.[22] Heterogeneity was then dealt with using subgroups according to these modifiers. If the data were still heterogeneous, we performed a random-effects model.[22]
The symmetry of a funnel plot was used to qualitatively determine whether there was publication bias.[23] In a funnel plot, larger studies that provide a more precise estimate of an intervention's effect form the spout of the funnel, whereas smaller studies with less precision form the cone end of the funnel. Asymmetry in the funnel plot indicates potential publication bias.
3. Results
3.1. Study selection and data collection
We identified 382 potentially relevant publications in the electronic databases (Fig. 1). Employing the selection criteria, we obtained quantitative data for our meta-analysis after reading all titles, abstracts, and full texts. Nine eligible studies from 8 publications[24–31] were included in our final analysis.
Figure 1.
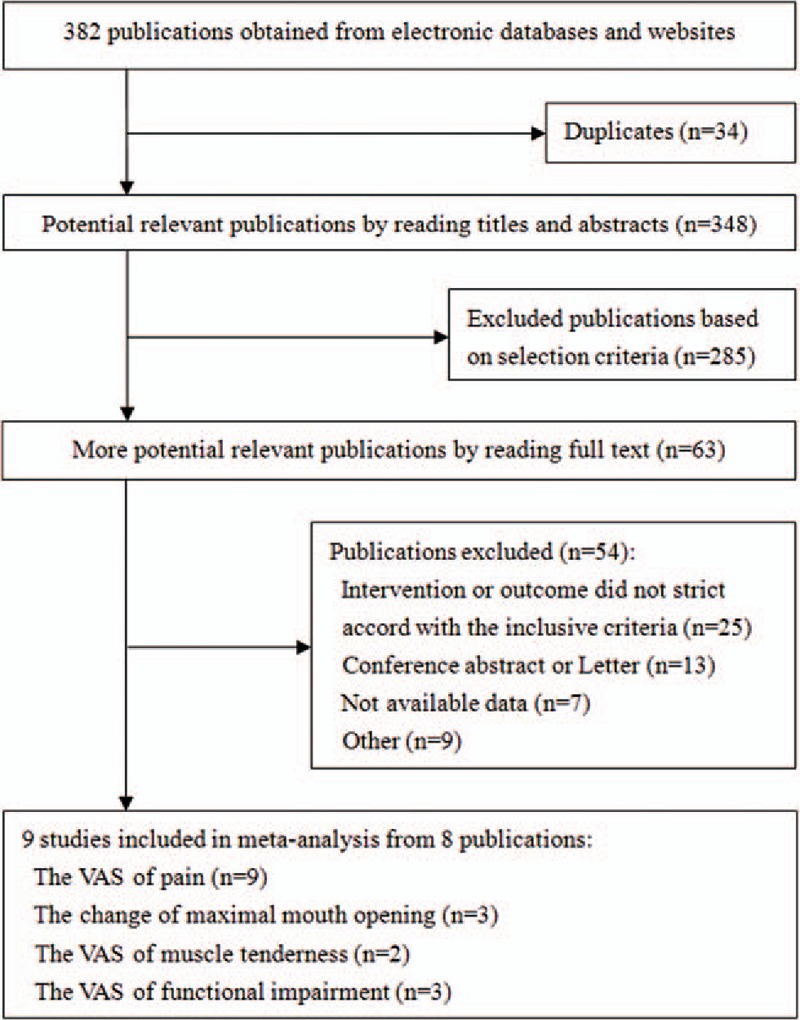
Summary of trial identification and selection.
3.2. Study characteristics
We investigated the 9 eligible studies from 8 publications [24–31] involving 231 patients. The VAS of pain was determined for all patients from these 9 studies.[24–31] The change in MMO was blended in 100 patients of 3 studies.[24,27,29] The VAS of muscle tenderness was involved in 46 patients of 2 studies.[25,29] The VAS of functional impairment included 74 patients of 3 studies.[27,31]Table 1 describes the clinical characteristics of all 9 studies.
Table 1.
Characteristics information of included studies.

3.3. VAS of pain
A comparison of the VAS of pain between the acupuncture group and control group indicated a significant decrease (MD = −0.98, 95% CI [–1.62,–0.34], I2=54%, P = 0.003) under the random-effects model.
Subgroup analysis of VAS for pain according to the type of control group under the random-effects model, as shown in Fig. 2, indicated that sham acupuncture as the control group (MD=−1.54, 95% CI [−2.63, −0.45], I2=58%, P = 0.006) and sham laser treatment as the control group (MD=−1.29, 95% CI [−2.32, −0.27], I2=0%, P = 0.01) showed a significant difference, but splint treatment as the control group (MD = −0.09, 95% CI [−0.69, 0.50], I2=0%, P = 0.76) showed no statistically significant difference.
Figure 2.
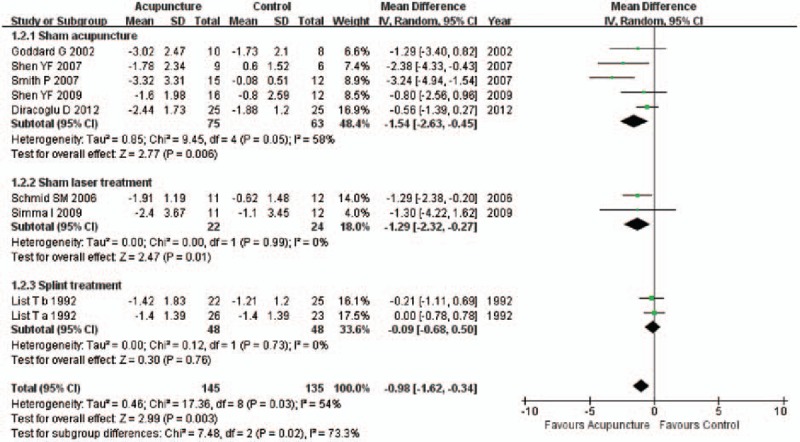
Forest plot of subgroup analysis of VAS for pain according to the type of sham control group. VAS = visual analog scale.
Subgroup analysis of VAS for pain by the classification of diseases under the random-effects model, shown in Fig. 3, indicated that myogenous TMD showed a significant difference (MD = −1.49, 95% CI [−2.45, −0.53], I2=47%, P = 0.002), while TMD showed no statistically significant difference (MD=−0.42, 95% CI [−1.14, 0.30], I2=46%, P = 0.25).
Figure 3.

Forest plot of subgroup analysis of VAS for pain according to the classification of diseases. VAS = visual analog scale.
The control subgroups were compared according to whether the control group treatment penetrated the skin (Fig. 4). Using the random-effects model, the overall results measuring the VAS of pain (MD=−1.49, 95% CI [−2.45, −0.53], I2=47%, P = 0.002) and nonpenetrating sham acupuncture as the control group (MD=−1.56, 95% CI [−2.70, −0.41], I2=58%, P = 0.008) showed significant differences, while penetrating sham acupuncture as the control group (MD=−1.29, 95% CI [−3.40, 0.82], I2= not applicable, P = 0.23) showed no significant difference.
Figure 4.
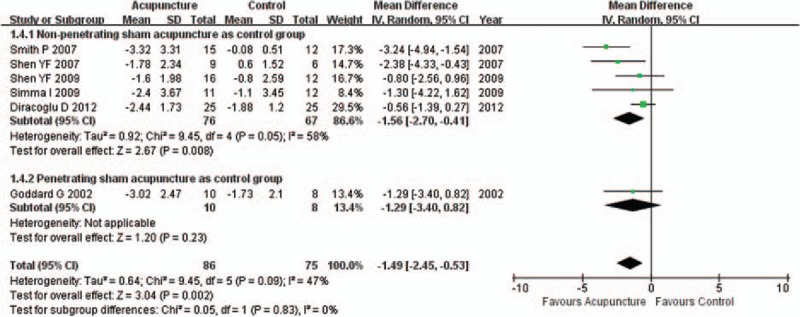
Forest plot of subgroup analysis of VAS for pain according to whether to penetrate the skin in control group. VAS = visual analog scale.
3.4. Change in MMO
A comparison of the change in MMO between the acupuncture group and control group, shown in Fig. 5, indicated no statistically significant difference (MD=3.44, 95% CI [−2.71, 9.58], I2=91%, P = 0.27]) under the random-effects model. When analyzed by subgroup according to the classification of diseases, the myogenous TMD (or the sham acupuncture groups) showed no statistically significant difference in the change of MMO (MD=3.23, 95% CI [−5.65, 12.12], I2=95%, P = 0.48), and the TMD (or the sham laser treatment groups) showed no statistically significant difference in the change of MMO (MD=4.00, 95% CI [−0.53, 8.53], I2=not available, P = 0.08).
Figure 5.
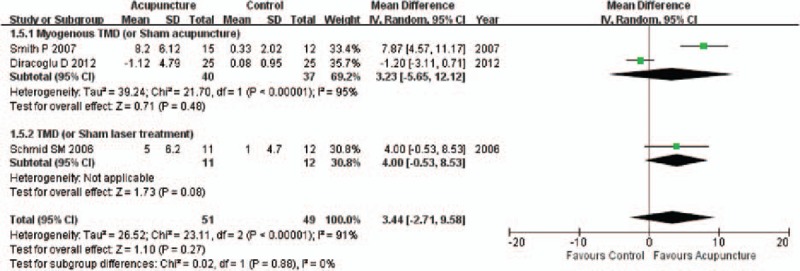
Forest plot of subgroup analysis of the change in MMO according to the classification of diseases. MMO = maximum mouth opening.
3.5. VAS of muscle tenderness
Using the fixed-effects model, a comparison of the VAS of muscle tenderness between the acupuncture group and control group (Fig. 6) showed a significant difference (SMD=−1.07, 95% CI [−1.70, −0.43], I2=37%, P = 0.001).
Figure 6.

Forest plot of the VAS of muscle tenderness. VAS = visual analog scale.
3.6. VAS of functional impairment
Using the random-effects model, a comparison of the VAS of functional impairment between the acupuncture group and control group (Fig. 7) showed no statistically significant difference (MD=−1.15, 95% CI [−3.26, 0.96], I2=74%, P = 0.29).
Figure 7.

Forest plot of the VAS of functional impairment. VAS = visual analog scale.
3.7. Publication bias
No publication biases were observed based on the symmetry of the funnel plots in all outcomes. The plot for the main outcome from the subgroup analysis of the VAS of pain according to the classification of diseases is shown in Fig. 8.
Figure 8.
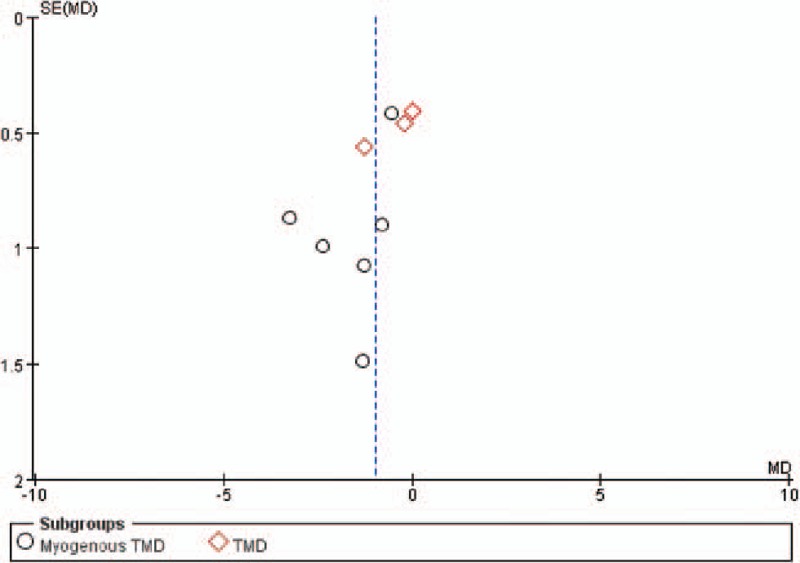
Funnel plot of subgroup analysis of the VAS of pain according to the classification of diseases. VAS = visual analog scale.
4. Discussion
Within this review, we developed explicit eligibility criteria using the Participants, Intervention, Comparison, Outcome, Study design format. We performed extensive and rigorous literature searches to identify potentially suitable articles in electronic databases. We also conducted meta-analyses to determine the overall treatment effect sizes. These ensured that our review could serve as a comprehensive summary of the available evidence at present. This meta-analysis evaluated 9 clinical trials that included TMD patients aged older than 18 years. In this study, acupuncture therapy was found to be superior to control therapy when measured by the VAS of pain and muscle tenderness. The specific subgroup results helped to refine the results and reveal parameters that may be helpful in the clinical practice of acupuncture for the management of pain in patients with TMD.
These results show that acupuncture was more effective than either sham acupuncture treatment or sham laser treatment, indicating that acupuncture is an effective tool for the management of pain in patients with TMD. Our results found no difference between acupuncture and splint treatment, but rather both of these treatments resulted in equivalent pain relief. Subgroup analysis, according to the classification of diseases, indicated that patients with myogenous TMD were more likely to benefit from acupuncture therapy than those with joint disorders. In 2009, Shen et al[26] found that a single acupuncture session reduced most myofascial pain endpoints of TMD. The results provided that penetrating sham acupuncture was shown to be more effective than nonpenetrating sham acupuncture for the relief of pain in this study and indicated that penetrating the skin was one of the key factors for the efficiency of acupuncture. However, Enblom et al and Ernst[32,33] in 2006 and 2008 reported that it was not penetrating versus nonpenetrating acupuncture per se, but rather the difference in the technique between different therapists, that may result in different requirement perceptions and blinding patterns. In 2011, Langevin et al[34] reported that there were few systematic investigations concerning which components of an acupuncture session may be important for any therapeutic effect, including needle placement and depth, and MacPherson et al,[35] in 2013, found little evidence that the effectiveness of acupuncture on pain was modified by the location of the needles. Additionally, Enck et al,[36] in 2010, deemed that real acupuncture and sham acupuncture produce similar effects. In the case of both MMO and functional impairment, our results showed that acupuncture had poor efficacy.
Several theses have been proposed to explain the mechanism of action of acupuncture. According to traditional Chinese medicine[37] (TCM), the human body contains a form of energy (qi) that flows throughout the body along clearly defined channels (meridians). When this sophisticated interconnected inner system is unbalanced, pain and disease will result. However, by inserting appropriate needles into specific points, the channels can be blocked, and the qi can once again flow fluently, and the rebalancing of the energy flow will both relieve the pain and eliminate the disease/disorder.[38,39] From the perspective of analgesic mechanism, some researchers have found that acupuncture can reduce the release of endogenous opiates (such as β-endorphin, enkephalin, endomorphin, and dynorphin[40–43] from the pituitary gland into the plasma, thereby resulting in analgesia in the central nervous system). In addition to the opioids, 5-HT (5-hydroxytryptamine [serotonin]) is believed to play an important role in acupuncture analgesia.[44] Tsai et al[45] found 5-HT release upon the activation of enkephalin-containing interneurons, which presynaptically inhibit the primary sensory neurons in the spinal cord. When the body is in a state of persistent inflammation, peptides can reduce the accompanying hyperalgesia, and immune cells will produce endogenous opiates.[46–48] Sekido et al[46] found that peripheral opioid receptors are involved in acupuncture analgesia during inflammatory conditions via local blockade rather than via systemic blockade of opioid receptors.
Some limitations in our manuscript should be addressed. First, only a few clinical trials met all of the inclusion and exclusion criteria; therefore, more clinical studies are required to confirm our results.[20] Second, some clinical trials had missing data on basic characteristics, possibly falsely increasing the heterogeneity owing to the failure to perform metaregression for confounding factors.[49,50] Although we estimated the missing SD from P values, this issue could lead to errors.[21]
5. Conclusion
This study compared the clinical effectiveness of acupuncture therapy in TMD patients through the meta-analysis of published results. Our results indicate that acupuncture therapy penetrating the skin has greater effectiveness and reduces the pain degree to a greater extent, especially myofascial pain symptoms, compared with both sham nonpenetrating acupuncture and sham laser therapy.
Footnotes
Abbreviations: 5-HT = 5-hydroxytryptamine, CI = confidence interval, MD = difference in means, MeSH = medical subject headings, MMO = maximum mouth opening, PRISMA = preferred reporting items for systematic reviews and meta-analysis, SD = standard deviations, SMD = standardized mean difference, TCM = traditional Chinese medicine, TMD = temporomandibular disorders, TMJ = temporomandibular joint, VAS = visual analog scale.
J-YW and Y-MN had full access to all of the data in the study, and take responsibility for the integrity of the data and the accuracy of the data analysis. J-YW, CZ, and Y-MN designed the study. Y-PX and Y-YY developed and tested the data collection forms. W-DL, LP, and J-YW acquired the data. M-HD and J-YW conducted the analysis and interpreted the data. J-YW and Y-MN drafted the manuscript. All authors critically revised the manuscript. Y-MN and M-HD had guarantor.
The authors have no conflicts of interest to disclose.
References
- [1].Goldstein BH. Temporomandibular disorders: a review of current understanding. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999;88:379–85. [DOI] [PubMed] [Google Scholar]
- [2].Magnusson T, Egermark I, Carlsson GE. Treatment received, treatment demand, and treatment need for temporomandibular disorders in 35-year-old subjects. Cranio 2002;20:11–7. [DOI] [PubMed] [Google Scholar]
- [3].Al-Jundi MA, John MT, Setz JM, et al. Meta-analysis of treatment need for temporomandibular disorders in adult nonpatients. J Orofac Pain 2008;22:97–107. [PubMed] [Google Scholar]
- [4].Dworkin SF, Huggins KH, LeResche L, et al. Epidemiology of signs and symptoms in temporomandibular disorders: clinical signs in cases and controls. J Am Dent Assoc 1990;120:273–81. [DOI] [PubMed] [Google Scholar]
- [5].Chen YW, Chiu YW, Chen CY, et al. Botulinum toxin therapy for temporomandibular joint disorders: a systematic review of randomized controlled trials. Int J Oral Maxillofac Surg 2015;44:1018–26. [DOI] [PubMed] [Google Scholar]
- [6].Armijo-Olivo S, Pitance L, Singh V, et al. Effectiveness of manual therapy and therapeutic exercise for temporomandibular disorders: systematic review and meta-analysis. Phys Ther 2016;96:9–25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Sharma S, Gupta DS, Pal US, et al. Etiological factors of temporomandibular joint disorders. Natl J Maxillofac Surg 2011;2:116–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [8].Gage JP. Collagen biosynthesis related to temporomandibular joint clicking in childhood. J Prosthet Dent 1985;53:714–7. [DOI] [PubMed] [Google Scholar]
- [9].Buescher JJ. Temporomandibular joint disorders. Am Fam Physician 2007;76:1477–82. [PubMed] [Google Scholar]
- [10].Winocur E, Steinkeller-Dekel M, Reiter S, et al. A retrospective analysis of temporomandibular findings among Israeli-born patients based on the RDC/TMD. J Oral Rehabil 2009;36:11–7. [DOI] [PubMed] [Google Scholar]
- [11].Zhang Y, Montoya L, Ebrahim S, et al. Hypnosis/Relaxation therapy for temporomandibular disorders: a systematic review and meta-analysis of randomized controlled trials. J Oral Facial Pain Headache 2015;29:115–25. [DOI] [PubMed] [Google Scholar]
- [12].Conti PC, de Alencar EN, da Mota Correa AS, et al. Behavioural changes and occlusal splints are effective in the management of masticatory myofascial pain: a short-term evaluation. J Oral Rehabil 2012;39:754–60. [DOI] [PubMed] [Google Scholar]
- [13].Shedden Mora MC, Weber D, Neff A, et al. Biofeedback-based cognitive-behavioral treatment compared with occlusal splint for temporomandibular disorder: a randomized controlled trial. Clin J Pain 2013;29:1057–65. [DOI] [PubMed] [Google Scholar]
- [14].Chen J, Huang Z, Ge M, et al. Efficacy of low-level laser therapy in the treatment of TMDs: a meta-analysis of 14 randomised controlled trials. J Oral Rehabil 2015;42:291–9. [DOI] [PubMed] [Google Scholar]
- [15].Adams D, Cheng F, Jou H, et al. The safety of pediatric acupuncture: a systematic review. Pediatrics 2011;128:e1575–87. [DOI] [PubMed] [Google Scholar]
- [16].Ernst E, Lee MS, Choi TY. Acupuncture: does it alleviate pain and are there serious risks? A review of reviews. Pain 2011;152:755–64. [DOI] [PubMed] [Google Scholar]
- [17].Lee MS, Ernst E. Acupuncture for pain: an overview of Cochrane reviews. Chin J Integr Med 2011;17:187–9. [DOI] [PubMed] [Google Scholar]
- [18].Borenstein M, Hedges LV, Higgins JP, et al. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res Synth Methods 2010;1:97–111. [DOI] [PubMed] [Google Scholar]
- [19].Moher D, Liberati A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 2009;339:b2535. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Higgins J, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011; Available at: www.cochrane-handbook.org Accessed October 1, 2011. [Google Scholar]
- [21].Furukawa TA, Barbui C, Cipriani A, et al. Imputing missing standard deviations in meta-analyses can provide accurate results. J Clin Epidemiol 2006;59:7–10. [DOI] [PubMed] [Google Scholar]
- [22].Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med 2002;21:1539–58. [DOI] [PubMed] [Google Scholar]
- [23].Copas J, Shi JQ. Meta-analysis, funnel plots and sensitivity analysis. Biostatistics 2000;1:247–62. [DOI] [PubMed] [Google Scholar]
- [24].Diracoglu D, Vural M, Karan A, et al. Effectiveness of dry needling for the treatment of temporomandibular myofascial pain: a double-blind, randomized, placebo controlled study. J Back Musculoskelet Rehabil 2012;25:285–90. [DOI] [PubMed] [Google Scholar]
- [25].Simma I, Gleditsch JM, Simma L, et al. Immediate effects of microsystem acupuncture in patients with oromyofacial pain and craniomandibular disorders (CMD): a double-blind, placebo-controlled trial. Br Dent J 2009;207:E26. [DOI] [PubMed] [Google Scholar]
- [26].Shen YF, Younger J, Goddard G, et al. Randomized clinical trial of acupuncture for myofascial pain of the jaw muscles. J Orofac Pain 2009;23:353–9. [PMC free article] [PubMed] [Google Scholar]
- [27].Smith P, Mosscrop D, Davies S, et al. The efficacy of acupuncture in the treatment of temporomandibular joint myofascial pain: a randomised controlled trial. J Dent 2007;35:259–67. [DOI] [PubMed] [Google Scholar]
- [28].Shen YF, Goddard G. The short-term effects of acupuncture on myofascial pain patients after clenching. Pain Pract 2007;7:256–64. [DOI] [PubMed] [Google Scholar]
- [29].Schmid-Schwap M, Simma-Kletschka I, Stockner A, et al. Oral acupuncture in the therapy of craniomandibular dysfunction syndrome—a randomized controlled trial. Wien Klin Wochenschr 2006;118:36–42. [DOI] [PubMed] [Google Scholar]
- [30].Goddard G, Karibe H, McNeill C, et al. Acupuncture and sham acupuncture reduce muscle pain in myofascial pain patients. J Orofac Pain 2002;16:71–6. [PubMed] [Google Scholar]
- [31].List T, Helkimo M. Acupuncture and occlusal splint therapy in the treatment of craniomandibular disorders: II. A l-year follow-up study. Acta Odontol Scand 1992;50:375–85. [DOI] [PubMed] [Google Scholar]
- [32].Enblom A, Hammar M, Steineck G, et al. Can individuals identify if needling was performed with an acupuncture needle or a non-penetrating sham needle? Complement Ther Med 2008;16:288–94. [DOI] [PubMed] [Google Scholar]
- [33].Ernst E. Acupuncture—a critical analysis. J Intern Med 2006;259:125–37. [DOI] [PubMed] [Google Scholar]
- [34].Langevin HM, Wayne PM, Macpherson H, et al. Paradoxes in acupuncture research: strategies for moving forward. Evid Based Complement Alternat Med 2011;2011:180805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].MacPherson H, Maschino AC, Lewith G, et al. Characteristics of acupuncture treatment associated with outcome: an individual patient meta-analysis of 17,922 patients with chronic pain in randomised controlled trials. PLoS One 2013;8:e77438. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Enck P, Klosterhalfen S, Zipfel S. Acupuncture, psyche and the placebo response. Auton Neurosci 2010;157:68–73. [DOI] [PubMed] [Google Scholar]
- [37].Chan E, Tan M, Xin J, et al. Interactions between traditional Chinese medicines and Western therapeutics. Curr Opin Drug Discov Devel 2010;13:50–65. [PubMed] [Google Scholar]
- [38].Unschuld PU, Huang Di Nei Jing Su Wen: Nature, Knowledge, Imagery in an Ancient Chinese Medical Text, University of California Press, London, UK, 2003. [Google Scholar]
- [39].Unschuld PU, Tessenow H, Jinsheng Z, et al. An Annotated Translation of Huang Di's Inner Classic—Basic Questions, University of California Press, London, UK, 1st edition, 2011. [Google Scholar]
- [40].Pomeranz B, Chiu D. Naloxone blockade of acupuncture analgesia: endorphin implicated. Life Sci 1976;19:1757–62. [DOI] [PubMed] [Google Scholar]
- [41].Pomeranz B, Cheng R, Law P. Acupuncture reduces electrophysiological and behavioral responses to noxious stimuli: pituitary is implicated. Exp Neurol 1977;54:172–8. [DOI] [PubMed] [Google Scholar]
- [42].Mendelson G. The possible role of enkephalin in the mechanism of acupuncture analgesia in man. Med Hypotheses 1977;3:144–5. [DOI] [PubMed] [Google Scholar]
- [43].Han Z, Jiang YH, Wan Y, et al. Endomorphin-1 mediates 2 Hz but not 100 Hz electroacupuncture analgesia in the rat. Neurosci Lett 1999;274:75–8. [DOI] [PubMed] [Google Scholar]
- [44].Cheng RS, Pomeranz B. Electroacupuncture analgesia could be mediated by at least two pain-relieving mechanisms; endorphin and non-endorphin systems. Life Sci 1979;25:1957–62. [DOI] [PubMed] [Google Scholar]
- [45].Tsai HY, Lin JG, Inoki R. Further evidence for possible analgesic mechanism of electroacupuncture: effects on neuropeptides and serotonergic neurons in rat spinal cord. Jpn J Pharmacol 1989;49:181–5. [DOI] [PubMed] [Google Scholar]
- [46].Sekido R, Ishimaru K, Sakita M. Differences of electroacupuncture-induced analgesic effect in normal and inflammatory conditions in rats. Am J Chin Med 2003;31:955–65. [DOI] [PubMed] [Google Scholar]
- [47].Huang C, Hu ZP, Long H, et al. Attenuation of mechanical but not thermal hyperalgesia by electroacupuncture with the involvement of opioids in rat model of chronic inflammatory pain. Brain Res Bull 2004;63:99–103. [DOI] [PubMed] [Google Scholar]
- [48].Hokfelt T. Neuropeptides in perspective: the last ten years. Neuron 1991;7:867–79. [DOI] [PubMed] [Google Scholar]
- [49].Higgins JP, Thompson SG. Controlling the risk of spurious findings from meta-regression. Stat Med 2004;23:1663–82. [DOI] [PubMed] [Google Scholar]
- [50].Thompson SG, Higgins JP. How should meta-regression analyses be undertaken and interpreted? Stat Med 2002;21:1559–73. [DOI] [PubMed] [Google Scholar]