

Abstract
Background:
Although anesthesiology has grown tremendously and although anesthesiologists play a crucial role in the perioperative management of patients and also outside operating theater (OT) such as critical care, pain clinic, and labor analgesia, they do not get due recognition. We conducted a study to assess the awareness about the role of anesthesia and anesthesiologists among patients scheduled to undergo surgery in a Government Tertiary Care Teaching Women and Children Hospital.
Designs:
A prospective cross-sectional survey with a sample size of 100 patients.
Materials and Methods:
Patients scheduled to undergo elective surgery in the age group of 18–65 years with the American Society of Anesthesiologists (ASA) Grades 1 and 2, who are willing to participate and given written informed consent. Patients whose age <18 years and more than 65 years, ASA health status Class 3 and above were excluded.
Analysis:
Statistical analysis was done by calculating percentages using Chi-square test.
Results:
Twenty percent of the participants were illiterate and of the educated, none were graduates or postgraduates. Patients with higher level of education had better knowledge of anesthesiology and role of an anesthesiologist with P < 0.05 than those with lesser education. Forty-eight percent of the participants had no idea about anesthesia despite the majority (62%) having previous surgery with no statistically significant difference (P > 0.05) between those with previous surgery and those without previous surgery regarding their knowledge of anesthesiology and anesthesiologist. Ninety percent did not know the complications, types of anesthesia and 44% did not know that anesthesiologist is a doctor.
Conclusion:
Most of the participants were not aware of the role of anesthesia and anesthesiologists inside and outside OT. Although this could be attributed to their lower level of education, the fraternity of anesthesiologists has to educate patients and surgeons about the role of anesthesia.
Keywords: Anesthesia, anesthesiologist, awareness
INTRODUCTION
Anesthesiology as a specialty has evolved tremendously over the last few decades following its first successful public demonstration way back in 1846. Anesthesiologists play a very crucial role in perioperative care, intensive care, labor analgesia, and pain clinic. The role of anesthesiology and anesthesiologists has traditionally been viewed as behind the screen specialty, and it is only in the last few decades, this specialty has grown beyond the four walls of the operation theater and the role of anesthesiologists is being increasingly appreciated in pain clinic, labor analgesia, accident and emergency, and in Intensive Care Unit (ICU).
Anesthesiology is the art and science of relieving pain during surgery and safety is the most important priority achieved through eternal vigilance.[1] The anesthesiologists play a very important role during and after surgery by protecting the patients from any adverse events during surgery through better management of vital functions, by providing good pain relief, and providing optimum surgical conditions to the surgeon and keep the patients safe by close monitoring.[1,2]
However, despite clearly playing a very crucial role in the perioperative management of patients and also in other areas such as pain clinic, labor analgesia, and critical care, it is still felt that anesthesiologist does not get the due he deserves, both in the eyes of the public and also fellow medical professionals.[1,2,3]
Although there have been surveys conducted before to assess knowledge of anesthesia and anesthesiologists before, these surveys were either conducted on general public[1,2,3,4,5] or on rural population[6] and on nonspecific groups of hospital patients.[7,8,9,10] There have been no previous surveys conducted specifically among patients scheduled to undergo surgeries in a Government Tertiary Care Women and Children Hospital.
The present study was conducted specifically to assess the level of awareness about the role of anesthesia and anesthesiologists among patients scheduled to undergo elective surgery in a Government Tertiary Care Women and Children Hospital.
MATERIALS AND METHODS
After Institutional Ethical Committee approval, this cross-sectional observational study was conducted at Vani Vilas Hospital (VVH) which is a Government Tertiary Teaching Women and Children Hospital affiliated to Bangalore Medical College and Research Institute, Bengaluru, Karnataka, India.
The survey was conducted by distributing questionnaires [Figure 1] to 100 patients scheduled to undergo elective surgery at VVH from August 2015 to November 2015 over a period of 3 months.
Figure 1.

Preoperative questionnaire.
Inclusion criteria
Adults in the age group of 18–65 years with the American Society of Anesthesiologists (ASA) Grades 1 and 2, undergoing elective surgeries and who are willing to participate and given written informed consent for this survey.
Exclusion criteria
Patients not willing to take part in the study, age <18 years and >65 years, ASA Grade 3 and above, and patients posted for emergency surgery were excluded from the study.
After confirming their willingness to take part in the questionnaire, patients were explained about the pattern of questions. Questionnaire was available in two languages – Kannada and English. Patients could opt for language of their preference. Illiterate and patients with vernacular other than Kannada and English had an interpreter to help in explaining question. Interpreter was a preoperative nurse who was not involved in the study. Literate patients were given questionnaire forms and asked to tick the answer of their choice. Survey was conducted in the preoperative period. Preoperative survey was conducted on patients who have not had a preanesthesia checkup. Survey was carried out by anesthesia postgraduate students posted in VVH. After a period of 3 months, survey questionnaires were collected and analyzed. Statistical analysis was done by calculating percentages using Chi-square test and correlation studies.
The questionnaire was a predesigned and pretested questionnaire and consisted of three sections. The first section was demographic data, second section had questions about anesthesiology, and the third section included questions about the role of an anesthesiologist. There were 21 questions in this questionnaire.
RESULTS
A total of 100 patients participated in this survey. All of them were women and most of them were aged between 21 and 30 years. Age distribution of the participants is depicted in Figure 2.
Figure 2.
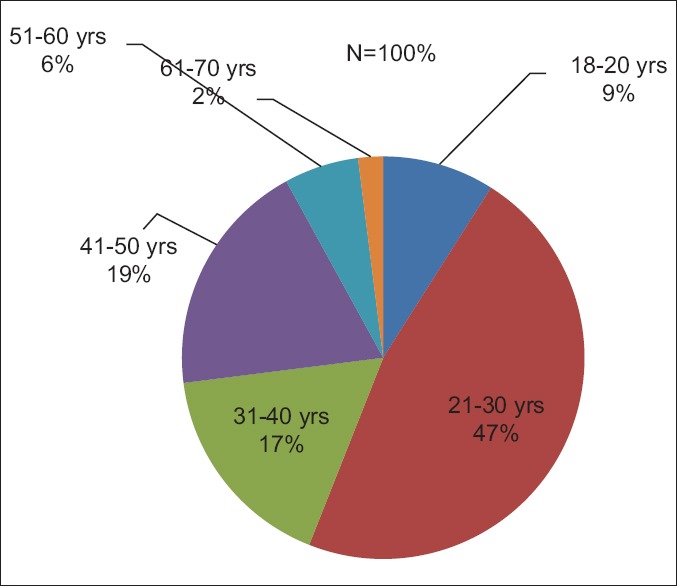
Age distribution of survey participants.
The vast majority (62%) were from Bengaluru and remaining 38% were from outside Bengaluru and most of the participants (62%) were gynecology patients and remaining 38% were obstetric patients.
Eighty percent of the participants were educated and 20% were illiterate. Of the educated, 50% had completed primary school, 28% high school, and 2% intermediate; however, none of the participants were graduates/postgraduates. Distribution of participants as per their education is depicted in Figure 3.
Figure 3.
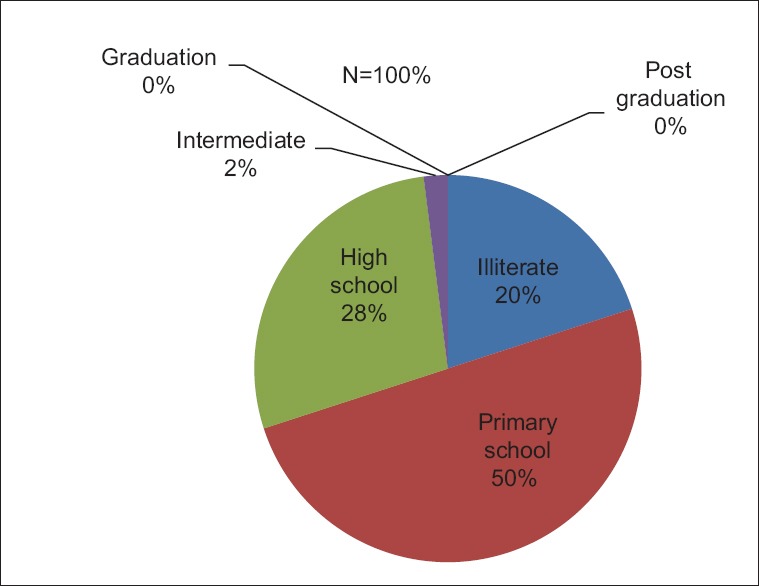
Education distribution of the participants.
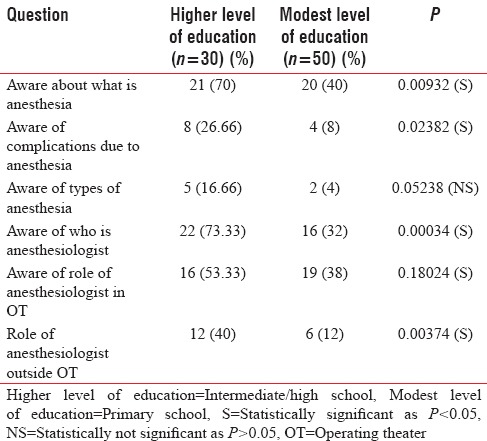
There was a statistically significant difference with P < 0.05 between the participants with higher level of education (intermediate and high school) having a greater knowledge of anesthesia, types, complications, and role of anesthesiologist inside and outside operating theater (OT) than the patients with medium level of education (primary school) as shown in Table 1.
Table 1.
Correlation studies of patient's level of education on their response to questions
All of them were homemakers.
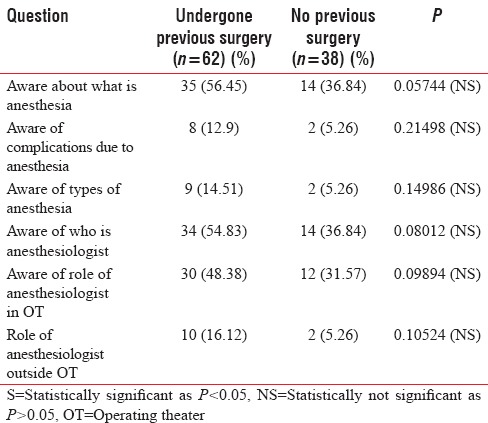
Majority of the participants (62%) had prior exposure to surgery and 38% had no previous surgery. Regarding their knowledge of anesthesiology, 48% had no idea about anesthesiology despite the majority (62%) having had prior exposure to surgery. There was statistically no significant difference between patients who had previous surgery and those who did not undergo previous surgery regarding their knowledge about anesthesia, types, complication, and the role of anesthesiologist both inside and outside OT as depicted in Table 2.
Table 2.
Correlation studies of patient's previous surgery experience on their response to questions
Twenty-nine percent felt it involved making area numb, 8% thought anesthesia was putting patients to sleep, and 15% thought it was to make patient unconscious. This is depicted in Figure 4.
Figure 4.
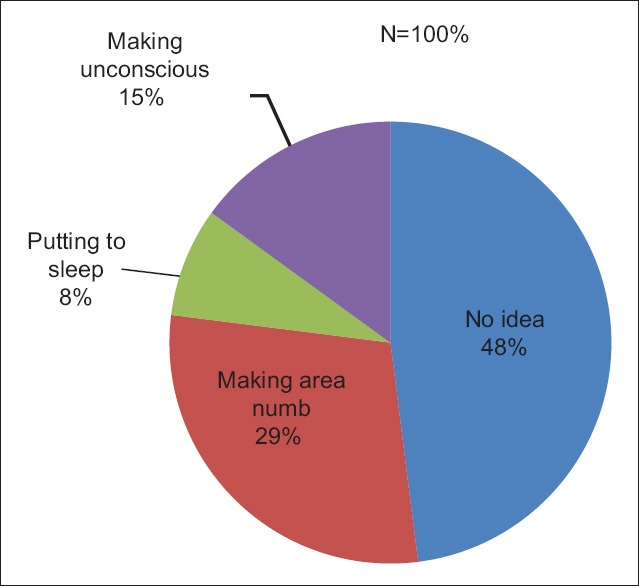
Distribution of participants regarding their idea about anesthesiology.
Specifically with regards to prior exposure to anesthesia, 50% said that they did have prior exposure to anesthesia and remaining 50% had no prior exposure to anesthesia. Of those 50% who said they had previous exposure to anesthesia, 32% were not sure whether they received general anesthesia (GA) or regional anesthesia (RA) and 18% were sure they had received local anesthesia. As far as their source of information about anesthesia, 14% had self-exposure, 16% were informed by the surgeon, 8% from a friend, 5% from a relative, 2% from the nurse, and 5% had multiple sources of information.
When asked about their fears/concerns about anesthesia, 43% did not know, 38% feared feeling pain during surgery, 15% feared being unconscious, 2% feared not waking up, and 2% feared not able to move.
The overwhelming majority (90%) of the participants said that they had no idea about complications due to anesthesia. Of the 10% who were aware about anesthesia complications, 5% felt not waking up was a complication of GA and 5% said that backache was a complication of RA.
Regarding consent for anesthesia, majority (57%) was not aware about the need for anesthesia consent and 43% were aware about the need for anesthesia consent.
When asked about different types of anesthesia, the overwhelming majority (94%) had no idea and only 6% knew about types of anesthesia, with 4% stating they knew about spinal anesthesia and 2% said they knew about local anesthesia.
Regarding their knowledge about who is an anesthesiologist, 48% said that anesthesiologist is a doctor, 44% had no idea, 7% answered specialist, and 1% answered technician. This response is depicted in Figure 5.
Figure 5.
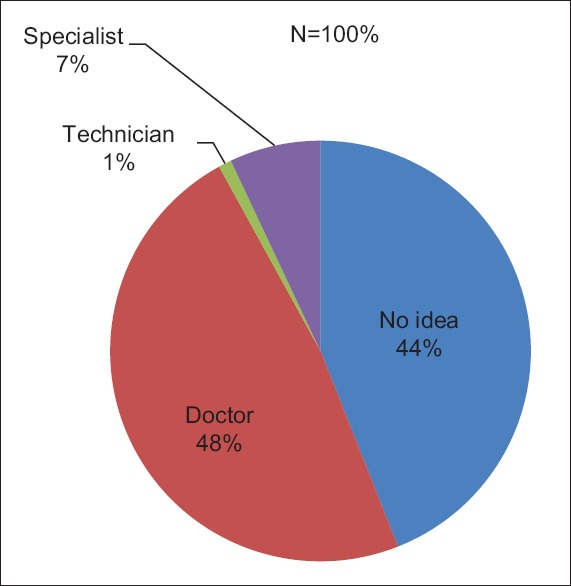
Distribution of participants regarding their perception of who is anesthesiologist.
When participants were asked specifically about the role of an anesthesiologist in OT, 57% had no idea, 31% answered he administers drugs, and 12% answered anesthetist anesthetizes patients and also monitors them. When asked whether they were actually aware that anesthetist was present in the OT, 59% had no idea, 22% said definitely yes, and 19% answered may be present. Regarding their knowledge about methods employed by the anesthesiologist to anesthetize patients, 66% answered by means of an injection and 34% had no idea.
The participants were then asked about who was looking after pain relief during and after surgery. Forty-four percent answered it was a surgeon, 36% had no idea, 6% answered it was a nurse, only 5% answered anesthetist, and remaining 9% answered all the above. This is highlighted in Figure 6.
Figure 6.
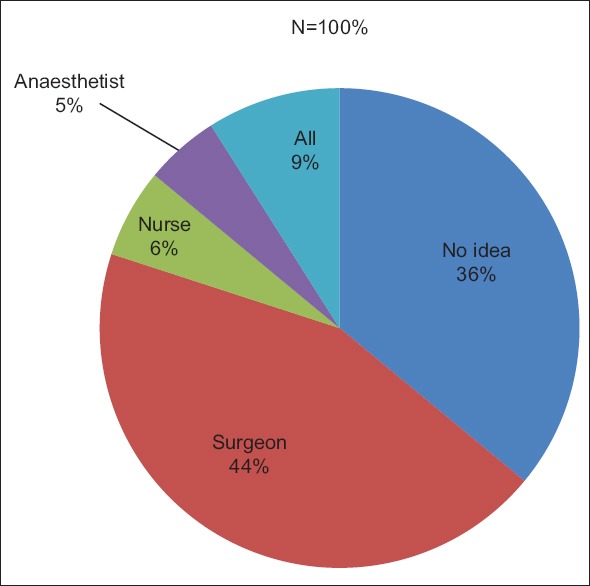
Response of participants regarding who looks after pain relief during and after surgery.
Regarding willingness to meet anesthesiologist before surgery, 41% were willing, 41% had no idea, and remaining 18% were not willing. When asked whether anesthetist was responsible for recovery after surgery, 69% had no idea, 22% answered yes, and 9% answered no. Regarding workplace of the anesthesiologist, 83% had no idea, 15% answered only OT, and remaining 2% answered OT, ICU, and preanesthesia clinic.
DISCUSSION
Our study was conducted to assess the knowledge about anesthesia among the patients scheduled for surgery in a Government Tertiary Care Teaching Women and Children Hospital, to study the awareness about the role of anesthesiologists in the perioperative management of patients scheduled to undergo operations and to analyze the perspective of patients about anesthesia as a specialty.
In our study, although most of the patients (62%) had previous exposure to surgery, overall their awareness about anesthesia and different techniques of anesthesia were poor. This could well be due their lack of education as 20% of the participants were illiterate and among the educated, none of them were graduates/postgraduates. This poor level of knowledge is similar to other surveys conducted in our country,[1,2,3,4] especially in the survey conducted on the rural population by Singh et al.[6] However, this is in sharp contrast to a very high level of awareness (80%) about anesthesia and the role of anesthetist among the UK population as reported in a study by Swinhoe and Groves.[7] This probably reflects the higher literacy rate in Western countries such as the UK and also a better interaction between anesthetist and patients during preanesthetic evaluation (PAE) as reported by Naithani et al.[3] In many of the previous surveys, especially by Naithani et al. and Singh et al.[3,6] there is a clear-cut correlation between the level of education and the level of awareness about anesthesia and anesthesiologist, and this could possibly explain the overall poor knowledge about anesthesia and role of anesthesiologist among our survey participants.
This is further established in our survey as there is a statistically significant difference with P < 0.05 between patients with higher level of education and those with medium level of education regarding their knowledge about anesthesia, types, complications, who is anesthesiologist and the role of anesthesiologist inside and outside OT as demonstrated in Table 1 (correlation studies of patient's level of education on their responses).
In our study, 48% of the patients were aware that anesthesiologist was a doctor and only 7% knew that anesthesiologist is a specialist. This is in agreement with previous studies when most of the patients are not even aware that anesthesiologist is a doctor, and most of the people are not aware that anesthesiologists are specialists like surgeons or physicians as reported by Uma and Hanji, Mathur et al., Naithani et al., and Irwin et al.[1,2,3,8] However, in a survey conducted by Prasad and Suresh,[4] much higher percentage (75%) of participants knew anesthesiologist is a doctor.
Most of our patients (57%) had no idea about the role of anesthetist in the OT, and only 12% were aware that anesthetist not only anesthetizes but also monitors them throughout the procedure. Other studies by Uma and Hanji, Mathur et al., and Naithani et al.[1,2,3] reported similar figures. This is in contrast to 80% of patients knowing about the role of the anesthesiologist in OT as reported by Swinhoe and Groves[7] from the UK, once again highlighting the role of education and higher literacy rate in the knowledge of patients.
It was extremely disappointing to note that only 2% of the patients were aware about the role played by anesthetist outside the OT. This lack of knowledge has been found in earlier studies by Gurunathan and Jacob and Herman,[5,9] and there has been no improvement over the years as reported in surveys by Uma and Hanji, Mathur et al., and Naithani et al.[1,2,3]
Although fear of feeling pain during surgery was the biggest concern/fear among 38% of the patients, yet only 5% knew it was the anesthetist who will provide pain relief during and after surgery, re-emphasizing their ignorance about the role of anesthesia and anesthesiologist. This was in contrast with the Western studies where awareness under anesthesia and failure to wake up were the biggest anesthesia concerns among patients as reported by Herman and Shevde and Panagopoulos.[9,10]
Informed consent before surgery is a very crucial document, and it was disappointing to know that 57% of the participants were not aware of the need to give informed consent for anesthesia. This is in contrast to 77% of patients being aware and 23% not aware of the need to give informed consent in a survey conducted by Prasad and Suresh.[4] In our survey, this could reflect both the lack of awareness about the importance of anesthesia but also highlights the importance of attending PAE clinic where the patients can be educated about anesthesia, different techniques of anesthesia, benefits and expected complications/side effects of anesthesia, and at the same time obtaining informed anesthesia consent.
Overall, it is disappointing that most of the patients in this study had poor knowledge about anesthesia, types and techniques of anesthesia, and role of anesthesiologist inside and outside OT. Although this is in agreement with most studies conducted in India as reported by Uma and Hanji, Mathur et al., and Naithani et al.,[1,2,3] it still is disappointing, especially in a tertiary teaching women hospital where anesthesiology and anesthesiologists play a very important role as seen in the study conducted by Bajwa and Bajwa[11] in the OT providing a safe, pain-free intraoperative and postoperative experience for all patients undergoing surgeries and also outside the OT where anesthesiologists provide labor analgesia services for pain-free delivery, educate patients in PAE clinics, and also play a crucial role in critical care of the very sick patients in ICU.
This study shows that although anesthesiologists play a very important role both in and outside the OT, not many patients are aware about anesthesiology as a specialty and the role of anesthesiologists. Although this may be partially attributed to the low level of education of our patients [Table 1], much needs to be done by the fraternity of anesthesiologists in educating the patients.
Anesthesiologists need to spend more time in PAE clinics in explaining to patients the role of anesthesia, types of anesthesia, techniques, benefits and potential complications/side effects with each technique, labor analgesia, informed anesthesia consent, and clearly highlighting their role to the patients both inside and outside OT. The familiar face of anesthetist goes a long way in relieving the anxiety of the patient in an unfamiliar environment of the OT as clearly proven in a study conducted by Klopfenstein et al.[12]
Anesthesiologists need to highlight their role in media, conduct health melas to educate patients about anesthesia and role of anesthesiologists, and also educate the surgeons who in turn can help improve the knowledge of this specialty among patients.
CONCLUSION
Most of the patients in our study were not aware of the role of anesthesia, types and techniques of anesthesia, and the role of anesthesiologists inside and outside OT despite the fact that most of them had previous surgery. Although this could be attributed to their lower level of education, the fraternity of anesthesiologists has a very important responsibility to educate patients and surgeons about the role of anesthesia, types, techniques, benefits, and also the very crucial role played by anesthesiologists inside and outside OT. This can be achieved by spending more time in PAE clinics, more interaction with patients, and with the help of print, electronic media, public health melas, and familiarizing themselves with the patients before surgery.
This could go a long way in improving the image of anesthesiologist with the patients and also the public at large.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Uma BR, Hanji AS. “Anaesthesia and Anaesthesiologists: How Famous are We among the General Population?” – A Survey. J Clin Diagn Res. 2013;7:2898–900. doi: 10.7860/JCDR/2013/7084.3788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mathur SK, Dube SK, Jain S. Knowledge about anaesthesia and anaesthesiologist amongst general population in India. Indian J Anaesth. 2009;53:179–86. [PMC free article] [PubMed] [Google Scholar]
- 3.Naithani U, Purohit D, Bajaj P. Public awareness about anaesthesia and anaesthesiologist: A survey. Indian J Anaesth. 2007;51:420–6. [Google Scholar]
- 4.Prasad CG, Suresh G. A survey on public awareness about the role of anesthesiologists. Ain -Shams J Anaesthesiol. 2014;7:456–9. [Google Scholar]
- 5.Gurunathan U, Jacob R. The public's perception of anaesthesiologists-Indian attitudes. Indian J Anaesth. 2004;48:456–60. [Google Scholar]
- 6.Singh P, Kumar A, Trikha A. Rural perspective about anesthesia and anesthesiologist: A cross-sectional study. J Anaesthesiol Clin Pharmacol. 2013;29:228–34. doi: 10.4103/0970-9185.111729. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Swinhoe CF, Groves ER. Patients’ knowledge of anaesthetic practice and the rôle of anaesthetists. Anaesthesia. 1994;49:165–6. doi: 10.1111/j.1365-2044.1994.tb03380.x. [DOI] [PubMed] [Google Scholar]
- 8.Irwin MG, Fung SK, Tivey S. Patients’ knowledge of and attitudes towards anaesthesia and anaesthetists in Hong Kong. Hong Kong Med J. 1998;4:16–22. [PubMed] [Google Scholar]
- 9.Herman CR. An appraisal of the anaesthetist-patient relationship. Anaesthesia. 1978;33:45–8. doi: 10.1111/j.1365-2044.1978.tb08278.x. [DOI] [PubMed] [Google Scholar]
- 10.Shevde K, Panagopoulos G. A survey of 800 patients’ knowledge, attitudes, and concerns regarding anesthesia. Anesth Analg. 1991;73:190–8. doi: 10.1213/00000539-199108000-00013. [DOI] [PubMed] [Google Scholar]
- 11.Bajwa SJ, Bajwa SK. Anaesthetic challenges and management during pregnancy: Strategies revisited. Anesth Essays Res. 2013;7:160–7. doi: 10.4103/0259-1162.118945. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Klopfenstein CE, Forster A, Van Gessel E. Anesthetic assessment in an outpatient consultation clinic reduces preoperative anxiety. Can J Anaesth. 2000;47:511–5. doi: 10.1007/BF03018941. [DOI] [PubMed] [Google Scholar]