

Abstract
Dentistry has undergone significant advancement and has seen several changing concepts over a decade. One such novel innovation is piezosurgery. Piezoelectric bone surgery or otherwise known as piezosurgery is a novel technique invented by Professor Vercellotti in 1988 to overcome the limitations of traditional instrumentation in oral bone surgery by modifying and improving conventional ultrasound technology. It is a promising, meticulous, and soft tissue sparing system for bone cutting based on low frequency ultrasonic microvibrations. The absence of macrovibration makes the instrument more manageable and allows greater intraoperative control with a significant increase in cutting safety in the more difficult anatomical cutting zone. The present review compares piezosurgery with the traditional tools and emphasizes on its mechanism of action, instruments, biologic effects, advantages, and limitations, as well as its various applications in the field of dentistry.
KEYWORDS: Cavitation, piezoelectric device, piezosurgery
INTRODUCTION
Over the last few decades, there has been rapid development in various dental surgical techniques, evolving a world of painless dentistry. Traditionally, osseous surgery was performed using hand instruments and various rotary instruments with different burs, which required external copious irrigation because of the production of heat using these instruments. In addition to heat, considerable pressure was also exerted in osseous surgeries, with a limitation in the case of fractured or brittle bones.[1] To overcome the above mentioned limitations, a novel surgical technique was introduced based on ultrasonic microvibration for precise and selective cut on the bone, without injuring the surrounding tissues.[2] This new alternative method, introduced in dentistry for bone related surgeries, was termed piezosurgery.
Piezosurgery, a relatively novel technique invented by Professor Vercelloti in 1988, offers advantages and overcomes the limitations of traditional instrumentation in oral bone surgery by modifying and improving conventional ultrasound technology. The basic principle of piezoelectricity discovered by Jacque and Pierre curie in late 19th century for bone cutting is based on ultrasonic microvibrations.[3] These microvibrations are created by the piezoelectric effect wherein certain ceramics and crystals deform on passing electric current through them, resulting in oscillations of ultrasonic frequency.[4]
The device consists of a cutting edge piezoelectric ultrasonic transducer mechanized by an ultrasonic generator competent of driving a range of resonant cutting inserts, a hand piece, and a foot switch connected to the main unit which supplies power and has holders for the hand piece and irrigation fluids. It contains a peristaltic pump for cooling with a jet of solution that discharge from the inserts and also helps in removing rubble from the cutting area. The device has a control panel with a digital display to set the power and frequency modulation. They also have several autoclavable tool-tips called inserts, which are titanium or diamond coated in various grades and move by microvibrations created in piezoelectric hand piece.[5] This device is widely used in dentistry serving various applications such as root planing, removal of supra and subgingival deposits and stains from teeth, crown lengthening, atraumatic tooth extraction, ridge augmentation, sinus floor elevation, bone graft harvesting, lateralization of inferior alveolar nerve, implant surgery, and ridge expansion.[6]
HISTORY
The term “piezo” originates from the Greek word piezein, which means, “to press tight, squeeze.” Jacques and Pierre Curie first discovered piezoelectricity in the year 1880 who found that applying pressure on various crystals, ceramics, or bone created electricity. This piezo effect is based on physical interactions and phenomena of basic electric and mechanical dimensions such as electric field strength, polarization, tension, and extension in the crystalline field, which states that deformation in crystals on passing electric current results in oscillations of ultrasonic frequency. The vibrations obtained are amplified and transferred to a vibration tip which when applied with slight pressure on bone tissue results in cavitation phenomena, which is a cutting effect exclusively on mineralized tissue.[4]
Gabriel Lippmann in 1881 found the converse piezoelectric effect, which was further investigated by various scientists. Catuna in 1953 developed an ultrasonic drill for cavity preparation on human teeth and published an article on the effects of ultrasound on dental hard tissues.[7] In 1957, Richman was the first to report the surgical use of an ultrasonic chisel without slurry to remove bone and resect roots in apicoectomies.[8] Mazzarow in 1960 reported evidence of an ultrasonic scalpel-like blade to directly cut osseous tissue.[9]
Mcfall et al., in 1961, evaluated the distinction of healing by comparison of rotating instruments and oscillating scalpel blade and found slow healing with no severe complication by use of these scalpel blades.[10] In 1980, Horton et al. stated that bone regeneration was better using ultrasonic device.[11] One year later, he evaluated the clinical utility of ultrasonic instrumentation in surgical removal of bone and observed mineralized tissue removal with ease and efficiency along with good acceptance by patients without any complications.[12]
In 1998, Torella reported the better use of ultrasonic generator compared to magnetostrictive device because of its greater efficiency of cutting with less bone destruction.[13] In 1999, Dr. Thomas Vercelloti invented piezoelectric bone surgery in collaboration with Mectron Spa and published in the year 2000.[14]
In 2001, piezosurgery® was introduced.
In 2002, the device was approved for commercial use in Germany.
In 2003, Vercelloli discovered the ideal frequency method for endodontic, orthopedic, neurologic, periodontal, and oral and maxillofacial surgeries.[15,16]
In 2005, the US Food and Drug Administration extended the use of ultrasonics in dentistry to include bone surgery.[17]
MECHANISM OF ACTION
Ultrasonics is a branch of acoustics dealing with sound vibrations in a frequency that ranges above the audible level i.e., >20 kHz where sonic is an ultrasound wave of high amplitude produced by three different methods.
Mechanical Method – up to 100 kHz
Magnetostatic Method – 18–25 kHz
Piezoelectric effect – 25–50 kHz
In piezosurgery, piezoelectric effect is used where mechanical energy in the form of tension and compression is converted into electric energy.[18]
Piezoelectric ultrasonic frequency is created by compelling an electric current from a generator over piezo-ceramic rings, which leads to their deformation. The ultrasonic frequency usually ranges 24–36 kHz, capable of cutting mineralized tissue in dental applications. Thus, the accruing movement from the deformation of ring sets up a vibration in the transducer, which creates the ultrasound output. These waves are transmitted to the hand piece tip, also called an insert, where longitudinal movement occurs resulting in the cutting of osseous tissue by microscopic shattering of bone.[19] The transducer is a very important part of the instrument system because it incorporates a piezoelectric element, which converts electric signals into mechanical vibrations and finally mechanical vibrations into electric signals.
Cavitation is the microboiling phenomenon occurring in liquids on any solid–liquid interface vibrating to an intermediate frequency, corresponding to a rupture of the molecular cohesion in liquids and the appearance of zones of depression that fill up with vapor until they form bubbles that are about to implode. In case of detartrating tools, cavitation occurs when the water spray contacts the insert vibrating to intermediate frequency.[20]
In ultrasonic osteotomy procedures, this phenomenon maintains good visibility in the field of operation by dispersing coolant as an aerosol and providing hemostasis.[21] The cavitation effect also shows an antibacterial property by fragmenting bacterial cell wall, which helps in obtaining high predictability and low morbidity in bone surgery.[6,22]
INDICATIONS
(1) Soft tissue debridement, (2) smoothening of root surfaces, (3) bone grafting, (4) implant site preparation, (5) removing an implant, (6) sinus lifting procedure, (7) retrograde root canal preparation, (8) apicectomy, (9) cystectomy, (10) extraction of ankylozed teeth, and (11) orthodontic surgeries.[23]
CONTRAINDICATIONS
No absolute contraindications
(1) Cardiopathy, (2) patients with uncontrolled diabetes mellitus, (3) patient receiving radiotherapy, (4) patients with metal/ceramic crowns, (5) patients with pacemakers.
PIEZOELECTRIC DEVICE
The device consists of a hand piece and a foot switch that are connected to a main unit, which supplies power and has holder for hand piece and irrigation fluids. The main unit comprises a platform and a control panel along with a digital display and keypad. Frequency of 25–29 kHz is present with a series of inserts of different form along with a linear vibration ranging from 60–200 µm. The power of the device is approximately 5 W.[24] The unit offers three different power levels from a clinical point of view. Low mode for orthodontic surgery and apico endocanal cleaning; high mode for cleaning and smoothing the radicular surface; and boosted mode in osseous surgery for performing osteotomy and osteoplasty.
PARTS OF THE INSTRUMENT
CONTROL PANEL
The piezosurgery unit is solely controlled by an interactive keyboard, which has two basic programs, the BONE and ROOT. In the BONE program, it is possible to adapt the power to any four levels depending upon the quality of the bone. In the ROOT program, the power can be set to either PERIO or ENDO. With this system, any interference present in the unit, hand piece, or electronics are recognized and highlighted on the display. The surgical tray contains all the components necessary for surgery utilizing this unit [Figure 1].
Figure 1.
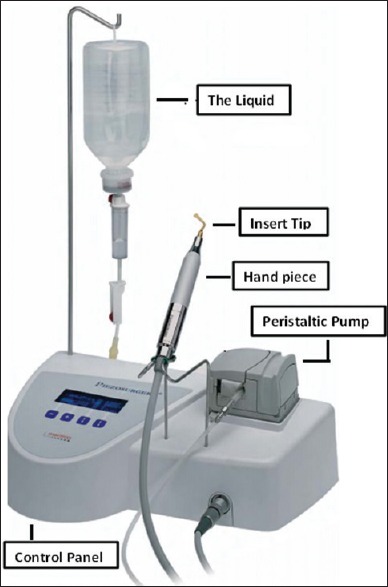
Piezosurgery unit
Dynamometric wrench
Insert tips are tightened to the hand piece using a dynamometric wrench which applies a predefined force to obtain energy transmission.
Hand piece
Each piezosurgery unit comes with two hand pieces and is permanently connected to a hand piece cord, which can be sterilized together.
The peristaltic pump
Contains irrigating solution which discharges from the insert with an adjustable flow of 0–60 ml/min for cooling and removal of detritus from cutting area. For a cooling effect, the solution is refrigerated at 4°C and the quantity of liquid may be adjusted using + and – buttons. The liquid is drawn from the bottle, which hangs from the rod provided, passing in hand piece through a cord.
Insert tips
Insert available can be classified as:
Titanium nitrate coating
They are effective for osteoplasty technique or for harvesting bone chips because they have the maximum cutting efficiency, avoid corrosion, and increase working life.
Diamond coating
Used in case of thin bone osteotomy or for complete osteotomy close to anatomical structures offering clinically less efficacious cut, histologically are more traumatic than cutting inserts, but much safer. They may be classified as:
Sharp insert tips
For effective treatment in bony structures such as in the osteoplasty techniques or for harvesting bone chips.
Smooth insert tips
For precise and controlled work on the bone structure. These are used in osteotomy when it is necessary to prepare difficult and delicate structure such as those preparing for sinus window or access to nerve.
Blunt insert tips
Used for preparing soft tissues. For e.g. elevating Schneider's membrane or lateralizing nerve. In periodontics, these tips are used for root planning [Figure 2].
Figure 2.
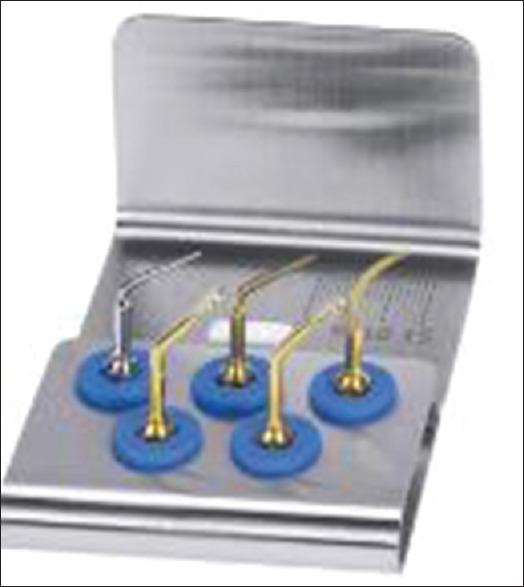
Perio kit
BASED ON INSERT TIP COLOR
Gold
All tips used to treat bone. This gold color is obtained by applying a coating of titanium nitride to improve the surface hardness for a longer working life [Figure 3].
Figure 3.
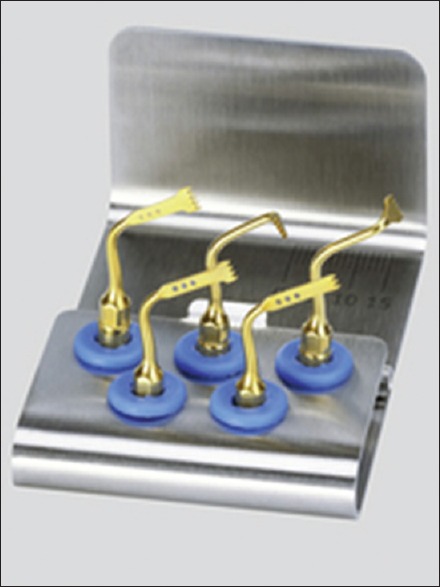
Gold insert tips
Steel
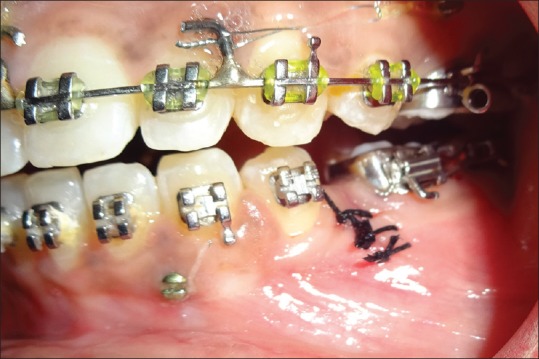
Used for soft tissue or delicate structures such as the roots of teeth [Figure 4].[20,25]
Figure 4.

Steel insert tips
BIOLOGICAL EFFECTS ON BONE CUT BY PIEZOELECTRIC DEVICE
The effect on cortical and cancellous bone and the surface roughness produced by different osteotomy technique have a strong biological effect on the bone and healing of the bone.[8] For piezoelectric osteotomy, the comparatively low amplitude of the cutting tool as opposed to that of an oscillating saw yield more precise cutting in clinical practice.[25] Blood free surgical site is another advantage because it provides a better intraoperative view. Local overheating, cavitation effects, and flow of cooling fluid by use of piezoelectric tools may serve as possible explanations for absence of blood at osteotomy site [Figures 5–7].[26]
Figure 5.

Preoperative piezosurgery for osteotomy
Figure 7.
Postoperative piezosurgery
Figure 6.

Operative site of osteotomy
The process is a prospect for extension in a spectrum of minimally invasive surgery using peizosurgery. Primary goal is to access the defective site without raising much of the mucoperiosteal flap. Bone swaging is done by peizo leading to minimal exposure. Though the advantage of peizosurgery is to avoid any soft tissue damage, precision drift of bone is done in few exceptional cases [Figure 8].
Figure 8.
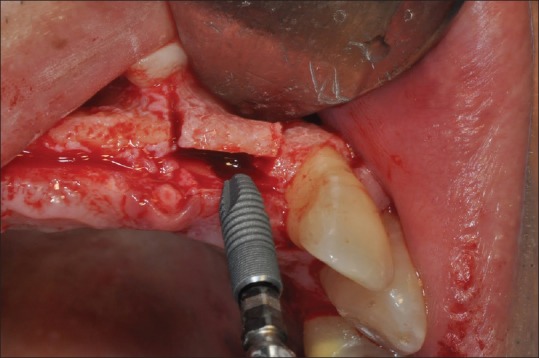
Ridge split done using piezosugery
In a previous study, rate of postoperative wound healing in a dog model following ostectomy and osteoplasty was used to compare the efficacy of piezoelectric instrument with a commonly used carbide burs (CB) or a diamond bur (DB). The surgical site treated by CB or DB lost bone in comparison to baseline measurements, by 14th day, while surgical sites treated by PS revealed a bone gain level. By the 28th day, the surgical site treated by all three instruments demonstrated an increased bone level and regeneration of cementum and periodontal ligament. However, by day 56, the surgical site treated by CB or DB evidenced a loss of bone versus a bone gain in the PS-treated sites. Thus, it appears that PS provided more favorable osseous repair and remodeling than CB or DB when surgical procedures were performed. Therefore, PS could be regarded as being efficacious for use in osseous surgery.[27]
GonzalezGarcia et al. conducted a study of 17 vertical alveolar distractions in the posterior region of the mandible, 7 on the right side, and 10 on the left side and compared the results between two approaches, i.e. conventional and piezoelectric technique. After analyzing several criteria, they concluded that the use of piezoelectric osteotomy in osteogenic distraction to increase the alveolar ridge height prior to the installation of dental implants is easier and less prone to intraoperative complications compared to conventional osteotomy procedures.[28]
Esteves et al. conducted a study and compared the differences of osteotomies performed with piezosurgery and a conventional drill with regard to “histomorphometrical, immunohistochemical and molecular analysis” and showed that, histologically and histomorphometrically, the bone healing showed no differences between the two groups, except for a slight higher amount of newly formed bone observed 30 days after the use of the piezosurgery device.[29]
Applications of piezosurgery in medicine include cranial osteoplasty, ENT surgery, neurosurgery, pediatric surgery, orthopedics, rhinoplasty and otologic surgeries.
APPLICATIONS IN DENTISTRY
ORTHODONTIC APPLICATIONS
Osteotomy, corticotomy, orthodontic traction of third molars, orthodontic closure of edentulous spaces, surgical cortical microincisions, and surgically assisted rapid maxillary expansion (SARME). Le Fort I osteotomy and orthodontic microsurgery can be effectively performed with the help of piezosurgery.[22,30] Blood loss decreased from an average 772 ml in conventional orthognathic surgery to an average 537 ml during orthognathic surgery using piezosurgery.[31]
ORAL AND MAXILLOFACIAL SURGERY
The most important indications are sinus lift, bone graft harvesting, osteogenic distraction, ridge expansion, endodontic surgery, periodontal surgery, inferior alveolar nerve decompression, cyst removal, dental extraction, unilateral condylar hyperplasia, and impacted tooth removal.[3] The risk of perforating Schneiderian membrane is reduced from 30% to 7% during the osteotomy procedure for bone window confection or during membrane lifting.[32]
PERIODONTOLOGY APPLICATIONS
Supragingival and subgingival scaling
Removal of supra and subgingival calculus, stains, and debris by placing the inserts vertically parallel to the long axis of the tooth and moving continuously.[33]
Curettage
By debriding epithelial lining of the pocket wall which results in microcauterization,[34] crown lengthening where bone is reduced effectively preserving root surface integrity,[35] regenerative surgeries for obtaining autogenous grafts in the form of bone chips or monocortical blocks.[18]
IMPLANTOLOGY
Harvesting block graft
Piezosurgery provides high precision and operating sensitivity and easy differentiation between cortical and cancellous bone while removing blocks of monocortical cancellous bone.[36] Osteotomy procedure where piezosurgery decreases the risk of bone fracture, making bones more elastic after osteotomy with ultrasonic intermediate vibration, thereby minimizing complications. Distraction osteogenesis followed by implant placement, for retrieval of blade implants, in ridge expansion, maxillary sinus elevation, drilling holes in bone for implant placement, for insertion of implant.[37]
Endodontics
Osteotomy, root-end resection, and root-end preparation preventing damage to soft tissues.[38]
ADVANTAGES
Has optimal vibration frequency for the mineralized tissue required during cutting and maintaining the bone constantly clean, avoiding excessive temperature.
Using of a modulated ultrasonic frequency allows highly precise and safe cutting of hard tissue, whereas adjacent soft tissue and nerve remain unharmed making it superior compared to conventional rotating instruments.
Strength required to make cuts is far less compared to that with drill or with oscillating saws making surgical control with piezosurgery maximum.
Offers direct visibility during osteotomy procedure minimizing risk to adjacent oral soft tissues.[39]
Piezosurgery units are three times more powerful than conventional ultrasonic units, which make it possible to cut highly mineralized tissue.
Minimal intraoperative bleeding seen as it does not traumatize bone thermally, with rapid postoperative wound healing.
Using piezosurgery tips, the harvested bone can be modified and shaped to fit accurately to the recipient.
Cavitation effect created by interaction between the irrigant solution and the oscillating tips makes surgical site clear during osteotomy.
Possibility to adapt the frequency of the vibrations of piezoelectric ceramics produces an efficacious and efficient cutting action on the bone of different quality.[40]
LIMITATIONS
Adequate dexterity and gentle touch is required for this type of procedure with a different learning curve.
Increase in working pressure above a certain limit impedes the vibrations of insert, transforming the energy into heat. Thus, the most effective way is to use piezosurgery hand piece with higher speed and a lower pressure.
Increase in operative time compared to traditional cutting instrument.
Difficulties encountered in deeper osteotomies sites because lack of insert of appropriate length and thickness to avoid the increasing pressure of the hand preventing microvibration of the insert.
Inserts get worn away very rapidly, and hence, it is recommended not to go beyond ten uses in bone surgery because it may break or cause damage to tissues by uncontrolled heat.[19]
Not cost effective.
CONCLUSION
Piezosurgery is relatively new surgical technique, which can be used in a variety of surgical procedure to complement traditional oral surgical procedures, and in some cases, replace traditional procedures. It also had been found to have additional effects regarding bone healing, minimal intraoperative bleeding, etc., and seems to be more efficient in first phases of bone healing.
In addition to its limitations, when used with their variable frequency and power, it serves as a platform for range of applications in periodontology, implantology, and various other oral surgical procedures, making it a highly effective tool in clinical practice.
FINANCIAL SUPPORT AND SPONSORSHIP
Nil.
CONFLICTS OF INTEREST
There are no conflicts of interest.
REFERENCES
- 1.Rashad A, Kaiser A, Prochnow N, Schmitz I, Hoffmann E, Haurer P. Heat Production during different Ultrasonic and conventional osteotomy preparation for dental Implants. Clin Oral Implant Res. 2011;22:1361–5. doi: 10.1111/j.1600-0501.2010.02126.x. [DOI] [PubMed] [Google Scholar]
- 2.Chopra P, Chopra P. Piezosurgery and its applications in Periodontology and Implantology. Int J Contemp Dent. 2011;2:16–24. [Google Scholar]
- 3.Pavlikova G, Foltan R, Horka M, Hanzelka T, Brounska H, Sedy J. Piezosurgery in oral and maxillofacial surgery. Int J Oral Maxillofac Surg. 2011;40:451–7. doi: 10.1016/j.ijom.2010.11.013. [DOI] [PubMed] [Google Scholar]
- 4.Labanca M, Azzola F, Vinci R, Rodella LF. Piezoelectric surgery: Twenty years of use. Br J Oral Maxillofac Surg. 2008;46:265–9. doi: 10.1016/j.bjoms.2007.12.007. [DOI] [PubMed] [Google Scholar]
- 5.Georg E, Klein J, Bank J, Hassfeld S. Piezosurgery: An ultrasound device for cutting bone and its use and limitations in maxillofacial surgery. Br J Oral Maxillofac Surg. 2004;42:451–3. doi: 10.1016/j.bjoms.2004.04.006. [DOI] [PubMed] [Google Scholar]
- 6.Nalbandian S. Piezosurgery techniques in implant dentistry. Aust Dent Pract. 2011:116–26. [Google Scholar]
- 7.Catuna MC. Sonic Surgery. Ann Dent. 1953;12:100–29. [Google Scholar]
- 8.Richman MJ. The use of ultrasonics in root canal therapy and root resection. Med Dent J. 1957;12:12–8. [Google Scholar]
- 9.Mazarow HB. Bone repair after experimentally produced defects. J Oral Surg. 1960;18:107–15. [Google Scholar]
- 10.Mcfall TA, Yamane GM, Burnett GW. Comparison of cutting effect on bone of ultrasonic cutting device and rotary burs. J Oral Surg. 1961;19:200–9. [PubMed] [Google Scholar]
- 11.Horton JE, Tarpley TM, Wood LD. The healing of surgical defects in alveolar bone produced with ultrasonic instrumentation, chisel and rotary bur. Oral Surg. 1975;39:536–46. doi: 10.1016/0030-4220(75)90192-9. [DOI] [PubMed] [Google Scholar]
- 12.Horton JE, Tarpley TM, Jr, Jacoway JR, Chapel Hill NC. Clinical applications of ultrasonic instrumentation in the surgical removal of bone. Oral Surg Oral Med Oral Pathol. 1981;51:236–42. doi: 10.1016/0030-4220(81)90051-7. [DOI] [PubMed] [Google Scholar]
- 13.Torrella F, Pitarch J, Cabanes G, Aniuta E. Ultrasonic osteotomy for surgical approach of maxillary sinus: A technical note. Int J Oral Maxillofac Implants. 1998;13:697–700. [PubMed] [Google Scholar]
- 14.Vercellotti T. Piezoelectric surgery in implantology: A case report – A new piezoelectric ridge expansion technique. Int J Periodont Restorative Dent. 2000;20:359–65. [PubMed] [Google Scholar]
- 15.Walsh LJ. Piezosurgery: An increasing role in dental hard tissue surgery. Aust Dent Pract. 2007;18:52–6. [Google Scholar]
- 16.Pereira CC, Gealh WC, Meorin-Nogueira L, Garcia-Júnior IR, Okamoto R. Piezosurgery Applied to Implant Dentistry: Clinical and Biological Aspects. J Oral Implantol. 2014;40:401–8. doi: 10.1563/AAID-JOI-D-11-00196. [DOI] [PubMed] [Google Scholar]
- 17.Thomas J. piezoelectric ultrasonic bone surgery: Benefits for the interdisciplinary team and patients. Dent India. 2008;2:20–4. [Google Scholar]
- 18.Kshirsagar JT, Prem KK, Yashodha SR, Nirmmal MT. Piezosurgery: Ultrasonic bone surgery in periodontics and oral implantology- Review. Int J Appl Dent Sci. 2015;1:19–22. [Google Scholar]
- 19.Leclercq P, Zenati C, Amr S, Dohan DM. Ultrasonic bone cut part 1: State-of-art technologies and common applications. J Oral Maxillofac Surg. 2008;66:177–82. doi: 10.1016/j.joms.2005.12.054. [DOI] [PubMed] [Google Scholar]
- 20.Aro H, Kallioniemi H, Aho AJ, Kellokumpu-Lehtinen P. Ultrasonic Device in Bone Cutting. A Histological and Scanning Electron Microscopical Study. Acta Orthop Scand. 1981;52:5–10. doi: 10.3109/17453678108991750. [DOI] [PubMed] [Google Scholar]
- 21.Mani AM, Marawar PP, Shubhangi Amit, Dalvi A. Piezosurgery – A Review. Pravara Med Rev. 2014;6:8–11. [Google Scholar]
- 22.Agarwal E, Masamatti SS, Kumar A. Escalating Role of Piezosurgery in Dental Therapeutics. J Clin Diagn Res. 2014;8:ZE08–11. doi: 10.7860/JCDR/2014/9161.4988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Devi S, Swaminathan M, Karthikeyan I, Anitha K. Piezosurgery in Periodontics. Int J Prosthodont Restorative Dent. 2015;5:51–5. [Google Scholar]
- 24.Schlee M. Piezosurgery – A precise and safe new oral surgery technique. Aust Dent Pract. 2009;2009:144–8. [Google Scholar]
- 25.Lands CA, Stubinger S, Laudemann K, Rieger J, Sader R. Bone harvesting at the anterior iliac crest using piezoosetotmy versus conventional open harvesting: A pilot study. Oral Surg Oral Med Oral Pathol Oral Radio Endod. 2008;105:19–28. doi: 10.1016/j.tripleo.2007.09.025. [DOI] [PubMed] [Google Scholar]
- 26.Chiriac G, Herten M, Schwarz F, Rothamel D, Becker J. Autogenous bone chips: Influence of a new piezoelectric device (Piezosurgery®) on chips morphology, cell viability and differentiation. J Clin Periodontol. 2005;32:994–9. doi: 10.1111/j.1600-051X.2005.00809.x. [DOI] [PubMed] [Google Scholar]
- 27.Vercellotti T, Nevins ML, Kim DV, Nevins M, Wada K, Schenk Rk, et al. Osseous response following respective therapy with a piezosurgery. Int J Periodont Restorative Dent. 2005;25:543–9. [PubMed] [Google Scholar]
- 28.GonzálezGarcía A, DinizFreitas M, SomozaMartín M, GarcíaGarcía A. Piezoelectric and conventional osteotomy in alveolar distraction osteogenesis in a series of 17 patients. Int J Oral Maxillofac Implants. 2008;23:8916. [PubMed] [Google Scholar]
- 29.Esteves JC, Marcantonio E, Jr, de Souza Faloni AP, Rocha FR, Marcantonio RA, Wilk K, et al. Dynamics of bone healing after osteotomy with piezosurgery or conventional drilling – histomorphometrical, immunohistochemical, and molecular analysis. J Transl Med. 2013;11:221. doi: 10.1186/1479-5876-11-221. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Stübinger S, Stricker A, Berg BI. Piezosurgery in implant dentistry. Clin Cosmet Investig Dent. 2015;7:115–24. doi: 10.2147/CCIDE.S63466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Anuroopa P, Kishan Panicker G, Nalini MS, Reddy BC. Piezosurgery in Dentistry: A Versatile Tool In Bone Management. Research And Reviews. J Dent Sci. 2014;2:32–7. [Google Scholar]
- 32.Flemmig TF, Petersilka GJ, Mehl A, Hickel R, Klaiber B. The effect of working parameters on root substance removal using a piezoelectric ultrasonic scaler in vitro. J Clin Periodontol. 1998;25:158. doi: 10.1111/j.1600-051x.1998.tb02422.x. [DOI] [PubMed] [Google Scholar]
- 33.Walmsley AD, Laird WR, Williams AR. Dental plaque removal by cavitational activity during ultrasonic scaling. J Clin Periodontol. 1988;15:539–43. doi: 10.1111/j.1600-051x.1988.tb02126.x. [DOI] [PubMed] [Google Scholar]
- 34.Hema S, Kranti K, Sameer Z. Piezosurgery in periodontology and oral implantology. J Indian Soc Periodontol. 2009;13:155–6. doi: 10.4103/0972-124X.60229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Sherman JA, Davies HT. Ultracision: The harmonic scalpel and its possible uses in maxillofacial surgery. Br J Oral Maxillofac Surg. 2000;38:530–2. doi: 10.1054/bjom.2000.0502. [DOI] [PubMed] [Google Scholar]
- 36.Sohn DS, Ahn MR, Lee WH. Piezoelectric osteotomy of intraoral harvesting of bone blocks. Int J Periodontics Restorative Dent. 2007;27:3–7. [PubMed] [Google Scholar]
- 37.Stefano S, Mario B, Marino S, Francesca M, Franco M. Autogenous particulate bone collected with a piezo-electric surgical device and bone trap: A microbiological and histomorphometric study. Arch Oral Biol. 2006;51:883–91. doi: 10.1016/j.archoralbio.2006.04.001. [DOI] [PubMed] [Google Scholar]
- 38.Abella F, de Ribot J, Doria G, Duran-Sindreu F, Roig M. Applications of Piezoelectric Surgery in Endodontic Surgery: A Literature Review. J Endod. 2014;40:325–32. doi: 10.1016/j.joen.2013.11.014. [DOI] [PubMed] [Google Scholar]
- 39.Schlee M, Steigmann M, Bratu E, Garg AK. Piezosurgery: Basics and possibilities. Implant Dent. 2006;15:334–40. doi: 10.1097/01.id.0000247859.86693.ef. [DOI] [PubMed] [Google Scholar]
- 40.Crosetti E, Battiston B, Succo G. PIezosurgery in head and neck oncological and reconstructive surgery: Personal experience on 127 cases. Acta Otorhinolaryngol Ital. 2009;29:1–9. [PMC free article] [PubMed] [Google Scholar]