

Abstract
Aims and Objectives:
Nowadays, the material that offers the best sealing characteristic in the field of endodontic treatment is the mineral trioxide aggregate (MTA), nevertheless, this material necessities an adhesive bonding agent to perfectly join to the dental surface. The aim of this study was to analyze using a scanning electron microscope (SEM) the possible microgap between the adhesive, MTA, and the dental surface.
Material and Methods:
Fourteen extracted molars were divided into two groups – group A was prepared with MTA-component adhesive and group B was prepared with MTA and composite dual etching. The observations were carried out with a SEM Phenom G2 Pro mode S.E.I. JMP® software was used for statistical analysis, and a t-test was used for evaluating the difference between the two groups.
Results:
The gap of the areas at higher magnification (1000×) with a size greater than 5 microns in width and 20 microns in length were considered significant, and only group A recorded significant data.
Conclusions:
The SEM analysis performed in the group A with interposition of adhesive and flow between the dental pulp chamber and MTA demonstrates the presence of a marginal gap of considerable amplitude in the all of the samples investigated.
KEYWORDS: Bonding agents, dental interface, endodontic material, MTA
INTRODUCTION
Modern dentistry has set as its goal the preservation of teeth. The improvement of conservative therapies and increased attention to the oral health conditions give the patients the opportunity of maintaining their natural teeth for a long time. This has been achieved with a significant reduction of tooth extraction number with an increase in teeth subjected to an endodontic treatment.
Today, even in the presence of perforations of the pulp chamber floor, it is possible to treat and save the teeth by using modern materials widely studied in the literature that have shown an ideal behavior in different clinical situations.
Among the materials available today, the mineral trioxide aggregate (MTA) is the material of choice for endodontic treatments.[1] To seal a dental perforation, it is essential to obtain a dry field. Torabinejad et al. developed a cement called MTA, which has all the features required of an ideal material to seal the communication between the root canal system and the oral cavity.[2] The MTA can be classified as an extremely biocompatible cement capable of stimulating healing and osteogenesis with its hydrophilic chemical features.[2] It consists of a powder of fine trioxide (tricalcium oxide, silicon oxide, bismuth oxide) and other hydrophilic particles (tricalcium silicate and tricalcium aluminate, responsible for the chemical and physical properties of this aggregate), which hardens in the presence of moisture. Hydration of the powder results in the formation of a colloidal gel with a pH of 12.5, which solidifies into a hard structure in approximately 3–4 hours.[3] This cement differs from all the other materials available on trade for its biocompatibility and antibacterial properties. Marginal adaptation and the sealing ability of MTA are features not present in the other materials used for endodontic treatment. In terms of biocompatibility, several recently published papers demonstrated the absence of cytotoxicity of the material in contact with fibroblasts and osteoblasts.[4,5,6] When MTA is applied on the dental surface, it produces the formation of a dentin bridge when the material is used to cover and directly protect the dental pulp.[7,8,9,10,11] Other researchers have demonstrated how there is a growth of cementum, periodontal ligament, and bone tissue when the MTA is applied for sealing a perforation. In addition, the marginal adaptation and the sealing ability of this new material are superior to those of the amalgam, glass cement, and to the reinforced zinc oxide cements based on a mixture of 32% eugenol and 68% ethoxy benzoic acid (Super EBA).[12,13,14,15] The characteristic that distinguishes MTA is its hydrophilic properties. The materials used to repair perforations or to protect the pulp tissue in direct pulp capping are usually in contact with blood or other tissue fluids. Dental cavity moisture can definitely be an important factor for its potential effects on the physical properties and sealing ability of the endodontic materials.[9,15]
As is demonstrated by Torabinejad,[9] MTA is the only material not affected by moisture or by blood contamination; the presence or absence of blood, in fact, seems to have no effect on sealing ability of MTA. In fact, MTA sets only in the presence of water.[16]
MTA restoration is applied through the use of conventional adhesive systems. The sublayer adhesive-MTA determines opposed forces to those adhesive, which should guarantee an intimate contact between the material and tooth substrate with the appearance of delamination and cracks at the interface tooth-restoration. The direct consequence of “micro-leakage” could be the cause of failure conservative restoration because of detachment caused by poor adhesion between these two materials that are chemically so different.[17,18]
The purpose of this research is to compare the efficiency of different adhesive systems interposed between the MTA and the restorative material, considering which is more reliable from the point of view of clinical microscope through the analysis of any microleakage between the various interfaces analyzed. The presence and quantification of the gap was performed using a scanning electron microscope (SEM).
MATERIAL AND METHODS
The investigation has been performed following the trade indication for the mixing of MTA (Aureoseal, Ogna LAB, Italy) cement proportions recommended by the manufacturer of liquid powder (1 g powder and 0.33 mL of saline). The research was carried out on 14 molars extracted for periodontal reasons. Each dental element was stored in saline solution for 1 month. Glutaraldehyde and sodium hypochlorite were not used as disinfectants and fixatives. Each tooth was sectioned by using an ISO 016 round bar mounted on high-speed handpiece. The cut was performed in the sagittal half tooth portion and was later made up of pulp floor covering with the MTA cement [Figure 1]. The size of the preparation was the same for each tooth by using a standard model empty ring placed on the tooth measuring 5 mm in diameter.
Figure 1.
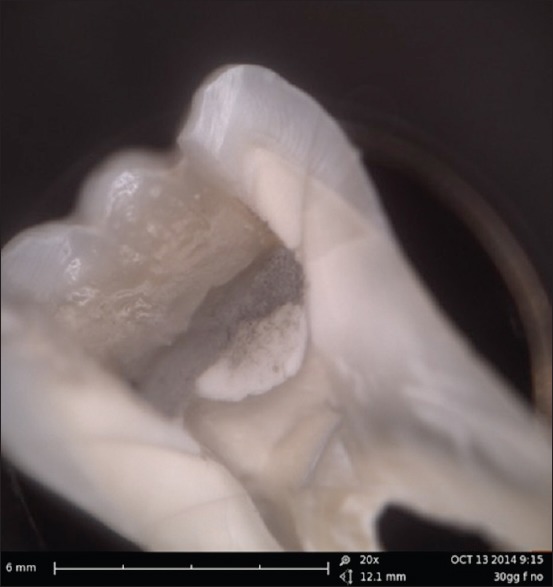
Representative image of a prepared tooth. It is possible to underline the different areas in which the MTA have been fixed and analyzed
An application of MTA was done with a thickness of 3 mm left in a humid environment for a week with a cotton pellet soaked in water up to complete hardening of the MTA, as suggested by the manufacturer.
The examined interfaces were divided the 2 groups – Group A was prepared with MTA-component adhesive (Scotchbond Universal 3M and 3M Filtek composite flow, 3M ESPE, St. Paul, MN, USA) (etching with 37% phosphoric acid for 30 seconds the surface was washed and kept moist for approximately 6–8 seconds, until the application of a single-component adhesive (Scotch Bond, 3M ESPE, St. Paul, MN, USA) and its polymerization for 20''); Group B was prepared with MTA and composite dual etching (Unicem 3M ESPE, St. Paul, MN, USA). The adhesive enamel-dentin and composites were used according to the manufacturer.
In both the groups, the observations were carried out with a SEM Phenom G2 Pro (25-nanometer resolution) mode SEI (Scanning electron direct), and then measured with a M2® software after cutting with a hard tissue microtome (Leica SP 1600).
The samples were analyzed at low magnification along the interface to detect the presence of possible marginal cracks. A rotation of the sample was made in the course of observations to avoid artifacts related to overlapping margins. The gap areas of the areas at higher magnification (1000×) with a size greater than 5 microns in width and 20 microns in length were considered significant. JMP® software (JMP ®, SAS Institute, Milan, Italia) was used for statistical analysis. A t-test was applied to evaluate differences between two groups with same size (P <0.05).
RESULTS
The preliminary analysis of the data shows a gap between the interface MTA–adhesive–composite of the examined cases in group A. In group B, in which the seal was obtained exclusively with dual-etching system, there was no significant gap [Figures 1–3]. Seven samples of group A showed the gap at the interface MTA–composite on range approximately of 18 microns by electronic measurement using the same microscope used for the survey. Seven samples of group B showed no gap at the interface composite. The average of the group A was recorded as 13.42 microns while group B recorded an average value of 6.71 microns [Graph 1].
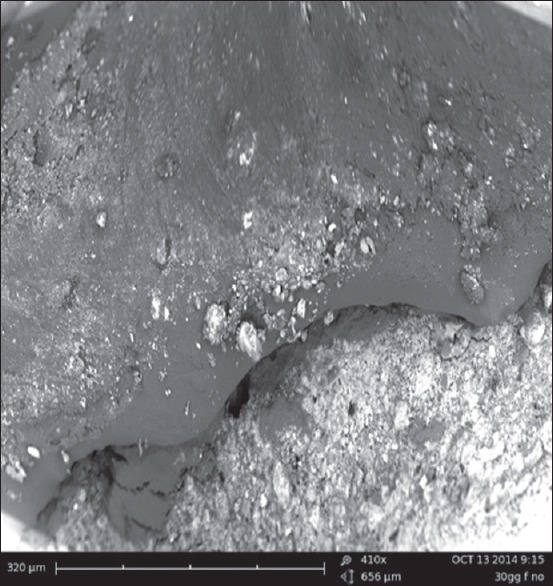
Figure 3.
The group B sample recorded a gap on average 6.42 μm. The SEM image gives the opportunity of underlining the excellent adhesion between the dual and MTA
Graph 1.
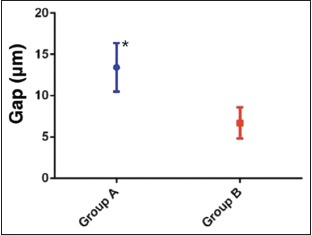
Gap values in µm of two groups. * (P <0.05) indicates significant statistical differences between groups A and B
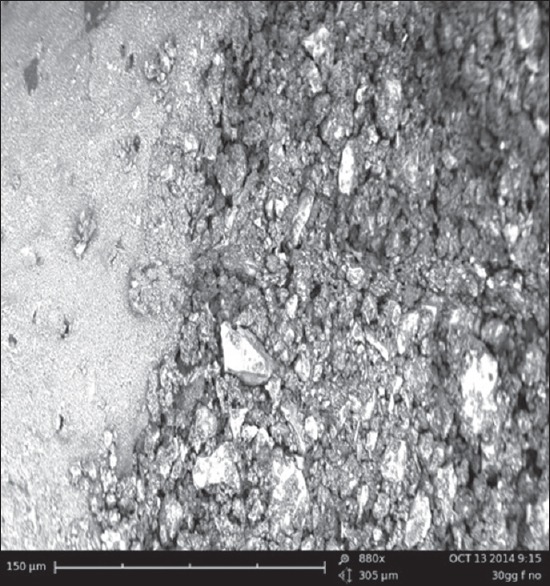
Figure 2.
The group A sample recorded a gap on average 13.42 μm. The SEM image gives the opportunity of underlining this gap
DISCUSSION
An ideal pulp covering material should guarantee the healthy radicular pulp tissue, should be highly biocompatible, should prevent bacterial microleakage, and should preserve a perfect adhesion between the tooth surface and the reconstructive materials.[19,20,21]
Analyzing the recent international literature regarding the material used in the conservative dentistry,[18,19,20,21,22] the problem of the material used in the conservative dentistry is related to their capacity of adhesion as well as regarding the avoidance of microlinkage and microgap in the restoration. The rationale of the study is to discover the optimal material for avoiding microgap on placing MTA on restorative dentistry.[19,20] The primary outcome of the study underlined good adhesion of both the materials used in the investigated groups. Therefore, the secondary outcome evidenced how one material, group B, better responded in the microscopic evaluation of the adhesion.
MTA can be considered the new gold standard for vital pulp therapies. It offers long-term seal, acceptable biocompatibility, and dentinal bridge formation demonstrated by several investigations both in animal as well as human teeth. As is well documented, the biocompatibility of MTA is based on its high pH and calcium ion release. However, this chemical phenomenon seems to be the principal parameter involving the repair. It has been recorded in several in-vivo researches how when great amounts of calcium ions are available, it could activate adenosine triphosphate, which plays a significant role in the mineralization and reparative process.[22,23,24,25]
The calcium ions specifically modulated osteopontin and bone morphogenetic protein-2 levels during pulp calcification. When mixed with water, the calcium oxide powder of MTA gets converted to CH, which dissociates to hydroxyl and calcium ions when it contacts the tissue fluids, which guarantees the possibility of high working on humidity. However, even though the high potential of MTA is well demonstrated, it is not easy to utilize the adhesive material to have a perfect fit between the MTA and the tooth surface.[21,24,26]
Within the limitation due to the size of the sample, the in-vitro research and the problems related to the tooth preparation, the results of the presents study give the opportunity of evaluating two different systems of adhesion. The SEM investigation underlined how the dual etching system resulted in low microgap between the MTA applied and the tooth surface, probably due to the interposition of the adhesive enamel dentine. This study confirms what was recently evidenced in the field of conservative dentistry; the dental materials' bonding mechanism to enamel and dentine is related to a chemical process in which minerals removed from the dental hard tissues are replaced with resin monomers. Then, the polymerization process fixes the placed material in the created porosities.[16,17,18,19,20]
There are two different effective adhesion systems that can be currently utilized over the MTA reconstruction which are well accepted in conservative dentistry. A first etching moment, followed by a compulsory rinsing procedure, which is responsible for the complete removal of smear layer and smear plugs is typical of the etch and rinse adhesives systems. On the other hand, an other cementation using dual-polymerizing resin luting cements can be widely used to bond MTA restorations because of their low solubility, low viscosity, clinically consistent thickness, high performance mechanical properties than conventional adhesives, ability to bond tooth to restorative material when used with bonding agents, and lower microleakage related to other materials.
Several researches on conservative dentistry about MTA have been recently published regarding the predictable and safe features of the adhesion materials. Analyzing the recent literature, controversies about the in-vitro researches are related to the nature and the type of dentin bridge formed between adhesive material and restorative ones. Therefore, future investigations should be focused on highlighting the quality of the filled microgap using large sample size, extended time period, and evaluating the pulp response on carious affected teeth. Long-term fixation is a fundamental step in the process of retention, marginal seal, and durability of indirect restorations.[22,24,27,28,29,30] Since the past two decades, resin cements continue to evolve with advancements in adhesive dentistry. The data from this investigation indicated how the dual adhesive cement works better then the traditional adhesive systems. However, the limitation of the present study is related with the in-vitro experimentation. Human saliva and humidity of the oral cavity may often influence the final results and may influence the cementation and the relation of bonding agents with MTA.
CONCLUSIONS
The microscopic observations, performed in group A with interposition of adhesive and flow between the chamber floor and MTA, demonstrates the presence of a marginal gap of considerable amplitude in 100% of the samples. The adopted technique in the study seems to be useful for the use of dental adhesives and it has proved to be very efficient and effective. In restoration with composite materials' self-etching primer without the use of mordants and adhesives results obtained demonstrate that the adhesive techniques ensure an adequate marginal seal in all the samples used. The presence of adhesive in the intermediate layer between the resin and MTA probably increases shrinkage stress, decreasing the effectiveness adhesive. Moreover, the presence of water in the MTA could inhibit adhesion due to high hydrophobicity of the resin materials; therefore, the use of the adhesive seems to be discouraged. All these analyses seem to suggest that the major achievements in cases where the MTA is used as the substrate. Extensive research should be performed to guarantee the long-term results in each therapy performed in conservative dentistry.
The optimization of the results of composite restorations MTA should therefore envisage the use of multiple materials with a common resinous base but with different chemical-physical characteristics with the aim to compensate for any gap, which results from polymerization shrinkage.
FINANCIAL SUPPORT AND SPONSORSHIP
Nil.
CONFLICTS OF INTEREST
There are no conflicts of interest.
REFERENCES
- 1.Purra AR, Ahangar FA, Chadgal S, Farooq R. Mineral trioxide aggregate apexification: A novel approach. J Conserv Dent. 2016;19:377–80. doi: 10.4103/0972-0707.186443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Torabinejad M, Pitt Ford TR, Mckendry DJ, Abedi HR. Histologic assessment of mineral trioxide aggregate as root-end filling material in monkeys. J Endod. 1997;23:225–8. doi: 10.1016/S0099-2399(97)80051-9. [DOI] [PubMed] [Google Scholar]
- 3.Asgary S, Ahmadyar M. Vital pulp therapy using calcium-enriched mixture: An evidence-based review. J Conserv Dent. 2013;16:92–8. doi: 10.4103/0972-0707.108173. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Koh ET, Mcdonald F, Pitt Ford TR, Torabinejad M. Cellular Response To Mineral Trioxide Aggregate. J Endod. 1998;24:543–7. doi: 10.1016/S0099-2399(98)80074-5. [DOI] [PubMed] [Google Scholar]
- 5.Koh ET, Torabinejad M, Pitt Ford TR, Brady K. Mineral Trioxide Aggregate Stimulates A Biological Response In Human Osteoblasts. J Biomed Mater Res. 1997;37:432–9. doi: 10.1002/(sici)1097-4636(19971205)37:3<432::aid-jbm14>3.0.co;2-d. [DOI] [PubMed] [Google Scholar]
- 6.Ford TR, Torabinejad M, Abedi HR, Bakland LK, Kariyawasam SP. Using Mineral Trioxide Aggregate As A Pulp-Capping Material. J Am Dent Assoc. 1996;127:1491–4. doi: 10.14219/jada.archive.1996.0058. [DOI] [PubMed] [Google Scholar]
- 7.Qureshi A, Soujanya E, Nandakumar, Pratapkumar Sambashivarao Recent advances in pulp capping materials: An overview. J Clin Diagn Res. 2014;8:316–21. doi: 10.7860/JCDR/2014/7719.3980. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Holland R, De Souza V, Nery MJ, Otoboni Filho JA, Bernabe PF, Dezan Junior E. Reaction of rat connective tissue to implanted dentin tubes filled with mineral trioxide aggregate or calcium hydroxide. J Endod. 1999;25:161–6. doi: 10.1016/s0099-2399(99)80134-4. [DOI] [PubMed] [Google Scholar]
- 9.Polineni S, Bolla N, Mandava P, Vemuri S, Mallela M, Gandham VM. Marginal adaptation of newer root canal sealers to dentin: A SEM study. J Conserv Dent. 2016;19:360–3. doi: 10.4103/0972-0707.186453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Torabinejad M, Pitt Ford TR, McKendry DJ, Abedi HR, Miller DA, Kariyawasam SP. Histologic assessment of mineral trioxide aggregate as a root-end filling in monkeys. J Endod. 1997;23:225–8. doi: 10.1016/S0099-2399(97)80051-9. [DOI] [PubMed] [Google Scholar]
- 11.Barbizam JV, Trope M, Tanomaru-Filho M, Teixeira EC, Teixeira FB. Bond strength of different endodontic sealers to dentin: Push-out test. J Appl Oral Sci. 2011;19:644–7. doi: 10.1590/S1678-77572011000600017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Adamo HL, Buruiana R, Schertzer L, Boylan RJ. A comparison of MTA, SuperEBA, composite and amalgam as root-end filling materials using a bacterial microleakage model. Int Endod J. 1999;32:197–203. doi: 10.1046/j.1365-2591.1999.00214.x. [DOI] [PubMed] [Google Scholar]
- 13.Gurgel-Filho ED, Martins F. Comparative evaluation of push-out bond strength of a MTA based root canal sealer. Braz J Oral Sci. 2014;13:114–7. [Google Scholar]
- 14.Al-Haddad A, Abu Kasim NH, Che Ab Aziz ZA. Interfacial adaptation and thickness of bioceramic-based root canal sealers. Dent Mater J. 2015;34:516–21. doi: 10.4012/dmj.2015-049. [DOI] [PubMed] [Google Scholar]
- 15.Wu MK, Kontakiotis EG, Wesselink PR. Long term seal provided by some root-end filling materials. J Endod. 1998;24:557–60. doi: 10.1016/S0099-2399(98)80077-0. [DOI] [PubMed] [Google Scholar]
- 16.Gade VJ, Belsare LD, Patil S, Bhede R, Gade JR. Evaluation of push-out bond strength of endosequence BC sealer with lateral condensation and thermoplasticized technique: An in vitro study. J Conserv Dent. 2015;18:124–7. doi: 10.4103/0972-0707.153075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Borkowski K, Kotousov A, Kahler B. Effect of material properties of composite restoration on the strength of the restoration–dentine interface due to polymerization shrinkage, thermal and occlusal loading. Med Eng Phys. 2007;29:671–6. doi: 10.1016/j.medengphy.2006.07.009. [DOI] [PubMed] [Google Scholar]
- 18.Lee IB, Cho BH, Son HH, Um CM. A new method to measure the polymerization shrinkage kinetics of light cured composites. J Oral Rehabil. 2005;32:304–14. doi: 10.1111/j.1365-2842.2004.01414.x. [DOI] [PubMed] [Google Scholar]
- 19.Karadas M, Cantekin K, Gumus H, Ateş SM, Duymuş ZY. Evaluation of the bond strength of different adhesive agents to a resin-modified calcium silicate material (TheraCal LC) Scanning. 2016;38:403–11. doi: 10.1002/sca.21284. [DOI] [PubMed] [Google Scholar]
- 20.Perdigão J, Geraldeli S. Bonding characteristics of self-etching adhesives to intact versus prepared enamel. J Esthet Restor Dent. 2003;15:32–41. doi: 10.1111/j.1708-8240.2003.tb00280.x. [DOI] [PubMed] [Google Scholar]
- 21.Lee IB, Um CM. Thermal analysis on the cure speed of dual cured resin cements under porcelain inlays. J Oral Rehabil. 2001;28:186–97. doi: 10.1046/j.1365-2842.2001.00639.x. [DOI] [PubMed] [Google Scholar]
- 22.Lee IB, An W, Chang J, Um CM. Influence of ceramic thickness and curing mode on the polymerization shrinkage kinetics of dual-cured resin cements. Dent Mater. 2008;24:1141–7. doi: 10.1016/j.dental.2008.03.015. [DOI] [PubMed] [Google Scholar]
- 23.Pashley DH, Tay FR. Aggressiveness of contemporary self-etching adhesives. Part II: Etching effects on unground enamel. Dent Mater. 2001;17:430–44. doi: 10.1016/s0109-5641(00)00104-4. [DOI] [PubMed] [Google Scholar]
- 24.Osorio R, Monticelli F, Moreira MA, Osorio E, Toledano M. Enamel-resin bond durability of self-etch and etch and rinse adhesives. Am J Dent. 2009;22:371–5. [PubMed] [Google Scholar]
- 25.Erhardt MC, Osorio E, Aguilera FS, Proença JP, Osorio R, Toledano M. Influence of dentin acid-etching and NaOCl-treatment on bond strengths of self-etch adhesives. Am J Dent. 2008;21:44–8. [PubMed] [Google Scholar]
- 26.Bastos LA, Sousa AB, Drubi-Filho B, Panzeri Pires-de-Souza Fde C, Garcia Lda F. Microtensile bond strength of silorane-based composite specific adhesive system using different bonding strategies. Restor Dent Endod. 2015;40:23–9. doi: 10.5395/rde.2015.40.1.23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hajizadeh H, Nemati-Karimooy A, Nasseh A, Rahmanpour N. Evaluating the shear bond strength of enamel and dentin with or without etching: A comparative study between dimethacrylate-based and silorane-based adhesives. J Clin Exp Dent. 2015;7:e563–8. doi: 10.4317/jced.52322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Lo Giudice G, Cutroneo G, Centofanti A, Artemisia A, Bramanti E, Militi A, et al. Dentin morphology of root canal surface: A quantitative evaluation based on a scanning electronic microscopy study. Biomed Res Int. 2015;27:ID164065. doi: 10.1155/2015/164065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Lo Giudice G, Cicciù M, Cervino G, Lizio A, Visco AM. Flowable resin and marginal gap on tooth third medial cavity involving enamel and radicular cementum: A SEM evaluation of two restoration techniques. Indian J Dent Res. 2012;23:763–9. doi: 10.4103/0970-9290.111256. [DOI] [PubMed] [Google Scholar]
- 30.Lo Giudice G, Lipari F, Lizio A, Cervino G, Cicciù M. Tooth fragment reattachment technique on a pluri traumatized tooth. J Conserv Dent. 2012;15:80–3. doi: 10.4103/0972-0707.92613. [DOI] [PMC free article] [PubMed] [Google Scholar]