

Abstract
Systemic fungal infections pose insidious challenges in neonatal intensive care settings. We present the case of a 9-day-old male term neonate admitted for polymicrobial sepsis and hepatic dysfunction who later developed candidemia superinfection. Despite broad antifungal therapy, the fungemia was complicated by progressive growth of a fungus ball in the right ventricular outflow tract that threatened cardiac function. Surgical excision of the mass was undertaken by right atriotomy and histologic examination confirmed Candida albicans.
Keywords: fungemia, Candida albicans, human herpesvirus 1, acute liver failure
Introduction
Fungal infections are common in very low birth weight neonates, with the Candida albicans (C. albicans) species accounting for 75% of these.1 Cardiac manifestations of fungemia in neonates can present as valvular vegetations, perivalvular abscesses, or intracardiac masses.2 We present a term neonate who developed a right ventricular (RV) fungal mass in the setting of herpes simplex virus (HSV-1)-induced liver failure.
Case Report
A 9-day-old male term neonate of normal birth weight and uncomplicated delivery initially presented with fever and poor feeding. Possible maternal HSV infection prompted empiric acyclovir therapy. Broad-spectrum antibiotic therapy was started empirically due to concerns for meningitis and urine cultures that were later found positive for methicillin-sensitive Staphylococcus aureus (MSSA) and group B Streptococcus (GBS). A positive DNA test confirmed the diagnosis of HSV-1. This was complicated by HSV-induced liver failure. A central venous catheter was placed 6 days after admission. One week after insertion of the central line, blood cultures grew C. albicans, and antifungal therapy was initiated.
Echocardiogram revealed a 25-mm × 4-mm echogenic, mobile pedunculated mass attached to the anterior RV wall and interventricular septum, with a 1-cm satellite lesion positioned inferiorly. Mild RV outflow tract (RVOT) gradient and mild RV dilatation were also noted (Figure 1). A multidisciplinary team determined that surgical excision of the intracardiac mass was indicated for infectious source control and prevention of cardiopulmonary compromise.
Figure 1.
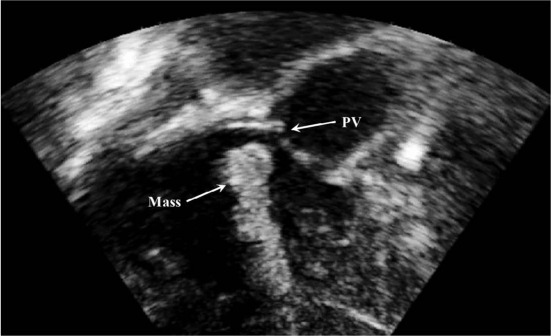
Transesophageal echocardiogram reveals an echodense structure in the right ventricular outflow tract (arrow). PV: pulmonary valve.
The patient was placed on cardiopulmonary bypass utilizing bicaval cannulation. An aortic cross-clamp was placed, and antegrade cardioplegia was administered. The right atrium was opened and the RV was approached through the tricuspid valve. Two distinct masses, both composed of friable yellow-brown material consistent with infectious vegetations, were completely removed from the RVOT. One located adjacent to the pulmonary valve annulus measured 2 cm in its largest diameter, and the other found near the moderator band measured 1 cm in diameter. Meticulous inspection of the RV cavity confirmed that the masses were removed in their entirety, with no residual fragments or additional vegetations. The excised masses were sent for microbiological cultures, which grew C. albicans. Histopathologic examination demonstrated the composition of a fungus ball containing acute inflammatory cells and fibrin deposition. Gomori methenamine silver (GMS) stain highlighted numerous budding yeast and pseudohyphae (Figure 2). Postoperatively, amphotericin B, acyclovir, and broad-spectrum antibiotics were continued.
Figure 2.
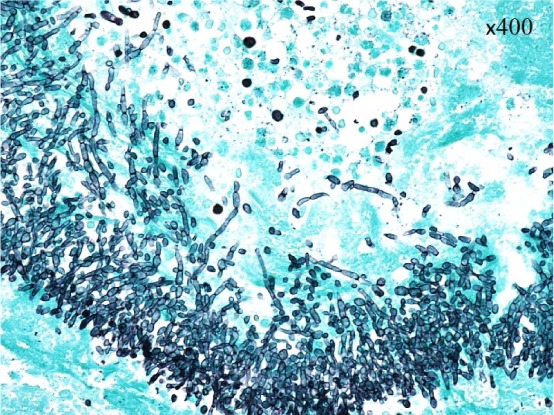
Photomicrograph of the resected right ventricular mass revealing numerous budding yeast and pseudohyphae (GMS × 400).
Postoperative echocardiogram identified no residual vegetations within the RV or RVOT. Serial cranial ultrasound examinations revealed multiple punctate hemorrhagic foci throughout the deep white matter and deep gray nuclei 5 days postoperatively. Due to the progressive multiorgan failure, the baby eventually developed disseminated intravascular coagulopathy and died on postoperative day 33.
Discussion
Over the past decade, diagnosis of neonatal Candida septicemia has increased to the current incidence ranging from 1.6% to 4.5%.3 Of these cases, 5% progress to endocarditis, and the vast majority of cases present in preterm low birth weight neonates.4,5 By contrast, Candida endocarditis in term neonates with normal birth weight, such as our patient, is extremely rare, with only a single case of Candida endocarditis documented in the literature.3 Fungal endocarditis in children is most frequently attributed to the Candida species, which account for 63% of reported cases. This infection usually affects the right side of the heart, most often the RV.4
Echocardiographic characteristics of intracardiac fungal lesions include bright, smooth borders and a homogenous echogenicity. Most involve the ventricular apex, atrial appendages, or intravascular catheters. Clinical signs of cardiac involvement depend on the size, site, and consistency of the mass. Small intracardiac thrombi often produce no clinical symptoms,6,7 and because standard microbiologic studies take approximately 3 days to establish a diagnosis of fungemia, clinical suspicion can be delayed. Echocardiographic findings of intracardiac vegetations associated with candidemia and negative bacterial blood cultures are highly suggestive of Candida endocarditis.8
In our patient, the development of Candida endocarditis was likely multifactorial. Empiric antibiotic coverage may have altered the microbial milieu in favor of fungal infection. The central venous catheter introduced a potential source. In addition, the patient's cellular immune response was suppressed by a disseminated HSV infection that led to fulminant liver failure. Although the antifungal therapy was initiated immediately upon discovery of positive fungal cultures, the progressive multisystem failure and polymicrobial sepsis impaired adequate fungal clearance.
Conclusion
The diagnosis of systemic fungal infection should be considered in any neonate who presents with fever associated with significant comorbidities in the setting of intravascular devices. Fungal cultures, echocardiography, and abdominal and brain ultrasound are essential for diagnosis and management of neonatal fungemia in the intensive care unit.
Conflict of Interest Disclosure
The authors have completed and submitted the Methodist DeBakey Cardiovascular Journal Conflict of Interest Statement and none were reported.
References
- 1. Butler KM, Baker CJ.. Candida: an increasingly important pathogen in the nursery. Pediatr Clin North Am. 1988. June; 35( 3): 543– 63. [DOI] [PubMed] [Google Scholar]
- 2. Mayayo E, Moralejo J, Camps J, Guano J.. Fungal endocarditis in premature infants: case report and review. Clin Infect Dis. 1996; 22: 366– 8. [DOI] [PubMed] [Google Scholar]
- 3. Brecht M, Clerihew L, McGuire W.. Prevention and treatment of invasive fungal infection in very low birthweight infants. Arch Dis Child Fetal Neonatal Ed. 2009. January; 94( 1): F65– 9. [DOI] [PubMed] [Google Scholar]
- 4. Levy I, Shalit I, Birk E, . et al. Candida endocarditis in neonates: report of five cases and review of the literature. Mycoses. 2006. January; 49( 1): 43– 8. [DOI] [PubMed] [Google Scholar]
- 5. Benjamin DK Jr, Poole C, Steinbach WJ, Rowen JL, Walsh TJ.. Neonatal candidemia and end-organ damage: a critical appraisal of the literature using meta-analytic techniques. Pediatrics. 2003. September; 112( 2 Pt 1): 634– 40. [DOI] [PubMed] [Google Scholar]
- 6. Tanke RB, van Megen R, Daniëls O.. Thrombus detection on central venous catheters in the neonatal Intensive care unit. Angiology. 1994. June; 45( 6): 477– 80. [DOI] [PubMed] [Google Scholar]
- 7. Beardsley DS. Venous thromboembolism in the neonatal period. Semin Perinatol. 2007. August; 31( 4): 250– 3. [DOI] [PubMed] [Google Scholar]
- 8. Heydarian M, Werthammer JW, Kelly PJ.. Echocardiographic diagnosis of Candida mass of the right atrium in a premature infant. Am Heart J. 1987. February; 113( 2 Pt 1): 402– 4. [DOI] [PubMed] [Google Scholar]