

Abstract
Child burn mortality differs widely between regions and is closely related to material deprivation, but reports on their global distribution are few. Investigating their country level distribution in light of economic level and income inequality will help assess the potential for macro-level improvements. We extracted data for child burn mortality from the Global Burden of Disease study 2013 and combined data into 1–14 years to calculate rates at country, region and income levels. We also compiled potential lives saved. Then we examined the relationship between country level gross domestic product per capita from the World Bank and income inequality (Gini Index) from the Standardized World Income Inequality Database and child burn mortality using Spearman coefficient correlations. Worldwide, the burden of child burn deaths is 2.5 per 100,000 across 103 countries with the largest burden in Sub-Saharan Africa (4.5 per 100,000). Thirty-four thousand lives could be saved yearly if all countries in the world had the same rates as the best performing group of high-income countries; the majority in low-income countries. There was a negative graded association between economic level and child burns for all countries aggregated and at regional level, but no consistent pattern existed for income inequality at regional level. The burden of child burn mortality varies by region and income level with prevention efforts needed most urgently in middle-income countries and Sub-Saharan Africa. Investment in safe living conditions and access to medical care are paramount to achieving further reductions in the global burden of preventable child burn deaths.
Keywords: Child, Burn, Mortality, Income inequality
Highlights
-
•
Burden of child burn deaths is 2.5/100,000, largest burden in Sub-Saharan-Africa.
-
•
34,000 lives could be saved yearly from burns if all countries had similar rates.
-
•
Globally child burns decrease as economic wealth increases.
-
•
Prevention efforts needed urgently in middle-income countries, Sub-Saharan-Africa.
1. Introduction
The Millennium Developmental Goals document the remarkable achievements towards a 50% reduction in deaths for under-fives since 1990 (GBD 2013 Mortality and Causes of Death Collaborators, 2015) due to interventions focused on targeting infectious and communicable diseases and improving access to essential child health services. Yet, many countries are now facing the double burden of infectious and non-communicable diseases combined (Global Burden of Disease Study 2013 Collaborators, 2015). Child injuries contribute to a high share of non-communicable diseases in children, but they have received limited attention in spite of their preventability (Byass et al., 2013, Alonge and Hyder, 2014). Injuries as a whole and burns in particular are, in fact, major causes of both death and social inequalities in child health (Laflamme et al., 2009). Children have an inherently higher risk of sustaining burn injuries due to their physical size and skin sensitivity (Peden et al., 2008) and those living in deprived and densely populated environments have a greater exposure to a range of hazardous products (Peck, 2011, Burrows et al., 2010, Othman and Kendrick, 2010).
Historically, gross domestic product (GDP) and gross national income (GNI) have been used as a summary measure to compare living standards between countries and it is now established that population health is significantly higher and better in richer countries than in poorer ones (Bell et al., 2013, Commission on Social Determinants of Health, 2008). This relationship has also been established in the injury field for children under five (Khan et al., 2015) and in the 1–19 age group globally (Peden et al., 2008). For child burns, 2004 data at the global level showed that mortality was nearly 11 times higher in low-income countries than in high-income countries (Peden et al., 2008).
Another factor of interest when investigating macro-determinants of child health and safety is country level income inequality, which is associated with a range of worse child health outcomes in resource rich and poor nations (Pickett & Wilkinson, 2015a), including injuries (Sengoelge et al., 2014). In the case of burns, it is reasonable to expect greater mortality where income inequality is higher, as a consequence of lower investments in the provision of minimal living standards and adequate housing conditions for the poorest segments of the population, as well as limited access to universal health care services (Peck, 2011, Bell et al., 2013, Sengoelge et al., 2013). Against this background we provide an update of the geographical distribution of child burn mortality rates worldwide and investigate the association between country level economic development and income inequality and the mortality burden.
2. Materials and methods
This was a cross-sectional register-based ecological study at country level.
2.1. Data sources and linkage
We used four online open access databases linked together in a four-stage process. The first stage consisted of extracting country-specific child mortality data from the Global Burden of Diseases (GBD) 2013 study expressed as number of deaths for the age groups 1–4, 5–9, and 10–14 years. A full protocol detailing the data collection, treatment and estimations can be consulted elsewhere but in brief incompleteness, under-reporting, and misclassification corrections are individualised for each data source, country or subnational site, and year (IHME Protocol, 2013).
A total of 103 countries were identified with child burn mortality data with burn classified as an external cause-of-injury due to fire, heat and hot substances by the GBD (IHME Protocol, 2013). The second stage involved matching mortality rates by country with two measures of economic development accessed from the World Bank: GNI per capita for classification of world economies (high income (≥$US 12,616), ii) middle income ($US 1036–12,615) and iii) low income (≤$US 1035)) and GDP per capita as an indicator of wealth (The World Bank, n.d.). The third stage consisted of linking to the Gini index of net income inequality within countries from the Standardized World Income Inequality Database, used for cross-national research on income inequality due to its extensive coverage and comparability (Solt, 2016). The final stage included linking the total population for each age group from the Department of Economic and Social Affairs at the United Nations (United Nations, 2015) to the total number of deaths in each country. This was necessary as the GBD 2013 study only shows mortality rates for the three separate age groups at country level and not for combined ages 1–14, and provides no rates at regional or income level.
2.2. Data treatment
The 103 countries were first stratified into seven regions using the GDB 2013 classification: Sub-Saharan Africa; South Asia; Latin America and the Caribbean; Eastern Europe/Central Asia; Asia-East; South East and Pacific; Middle East and North Africa; Organization for Economic Cooperation and Development (OECD). Then countries were stratified into high, middle and low-income economies at country and regional level based on the GNI classification.
Child burn mortality rates per 100,000 were compiled for ages 1–14 combined at country level (see Supplement 1 Table), followed by rates at regional and income level. We then used these mortality data to further compile the number of potential lives saved by subtracting the burn mortality rate in each income category from the reference (lowest) burn mortality rate in the same category. This result was multiplied by the total population aged 1–14 years and divided by 100,000. The formula reads as follow: [(Child burn mortality rate per income category) − (Reference child burn mortality rate) × (Total N population 1–14 years) / 100,000]. Next we examined the relationship between child burn mortality rates and GDP and income inequality by region and income level using Spearman coefficient correlations (r). Countries were then plotted on scatter plot diagrams to provide a visualization of these relationships using the log transformation of the GDP to make the data less skewed. Data analysis was performed using Stata/SE 12.1 (StataCorp, 2011) and the geographical map was developed using Google Maps Maker.
3. Results
In 2013 the overall burn mortality rate among children aged 1–14 years was 2.5 per 100,000 across 103 countries and wide regional variation exists in country rates ranging from 0 to 9.5 per 100,000 (see Fig. 1). The burden is most remarkable in Asia, particularly Mongolia, and certain parts of Africa (e.g. Rwanda, Malawi, Togo).
Fig. 1.

Geographical distribution of child burn mortality per 100,000 in 2013.
When examining the relationship between burn mortality rates and world economies, there is a graded increase in rates with decreasing country economic level globally and in the two regions where the overall burden is highest, Sub-Saharan Africa and Eastern Europe and Central Asia (see Table 1). This pattern was not present in the five other regions as three regions have the highest child burn rates in the middle income countries compared to three regions with rates highest in the high-income group. Furthermore, the low income countries of the Sub-Saharan region have the majority of preventable deaths at 13,671 potential lives saved from 25,857 lives saved in all low income countries combined (53%) and 41% from the total preventable deaths globally.
Table 1.
Distribution of child burn mortality rate and potential lives saved by region and income level.
| Region and income level (N countries) | Deaths 1–14 y |
Population 1–14 y |
Mortality rate per 100,000 (min–max) |
Potential lives savedb |
|---|---|---|---|---|
| All (N = 103)a | 43,992 | 1,740,000,000 | 2.5 (0–9.5) | 33,081 |
| High income (N = 39) | 1069 | 176,000,000 | 0.6 (0–2.1) | Reference |
| Middle income (N = 49) | 13,052 | 903,000,000 | 1.4 (0.2–8.1) | 7224 |
| Low income (N = 15) | 29,871 | 663,000,000 | 4.5 (0.1–9.5) | 25,857 |
| Sub-Saharan Africa (N = 15) | 30,655 | 685,000,000 | 4.5 (1.0–9.5) | 13,671 |
| High income (N = 0) | – | – | – | |
| Middle income (N = 5) | 873 | 34,000,000 | 2.5 (1.2–4.5) | Reference |
| Low income (N = 10) | 29,782 | 651,000,000 | 4.6 (0.9–9.5) | 13,671 |
| South Asia (N = 8) | 9190 | 364,000,000 | 2.5 (0.3–2.6) | – |
| High income (N = 0) | – | – | – | |
| Middle income (N = 5) | 9104 | 353,000,000 | 2.6 (0.3–2.6) | – |
| Low income (N = 3) | 86 | 10,300,000 | 0.8 (0.3–0.9) | – |
| Latin America and the Caribbean (N = 18) | 526 | 75,700,000 | 0.6 (0.2–4.9) | 297 |
| High income (N = 2) | 2 | 961,989 | 0.2 (0.2–0.2) | Reference |
| Middle income (N = 15) | 522 | 73,900,000 | 0.6 (0.2–4.9) | 296 |
| Low income (N = 1) | 2.5 | 855,187 | 0.3 | 1 |
| Eastern Europe/Central Asia (N = 18) | 721 | 41,900,000 | 1.8 (0–3.1) | 121 |
| High income (N = 6) | 402 | 21,700,000 | 1.4 (0–2.1) | Reference |
| Middle income (N = 12) | 319 | 20,200,000 | 2.0 (0.2–3.1) | 121 |
| Low income (N = 0) | – | – | – | – |
| Asia East, South East and Pacific (N = 12) | 1712 | 374,000,000 | 0.5 (0–8.1) | – |
| High income (N = 4) | 15 | 3,698,756 | 0.3 (0–0.5) | – |
| Middle income (N = 7) | 1697 | 369,000,000 | 0.5 (0.2–0.4) | – |
| Low income (N = 1) | 1 | 791,218 | 0.1 (0.3–8.1) | – |
| Middle East and North Africa (N = 4) | 7 | 3,135,905 | 0.2 (0.2–0.3) | 1 |
| High income (N = 1) | 4 | 1,978,422 | 0.2 | Reference |
| Middle income (N = 3) | 3 | 1,157,483 | 0.3 (0.2–0.3) | 1 |
| Low income (N = 0) | – | – | – | – |
| Organization for Economic Cooperation and Development (OECD) (N = 33) | 1185 | 200,900,000 | 0.6 (0.1–2.5) | 356 |
| High income (N = 30 | 650 | 150,000,000 | 0.4 (0.1–1.2) | Reference |
| Middle income (N = 3) | 535 | 50,900,000 | 1.1 (0.2–2.5) | 356 |
Certain countries may fall under different categories, so the total n countries may not add up to 103.
This was calculated using the lowest child burn mortality rate in each region which showed a graded relationship between income level and burn deaths, therefore the analysis was not conducted in South Asia and Asia East, South East and Pacific.
When comparing burn rates with country level economic wealth at global level, there is a significant negative correlation between GDP (r = − 0.69, p < 0.01) and burn mortality rates and a positive correlation with income inequality (r = 0.44, p < 0.001) (see Table 2). At regional level significant negative correlations are observed in three out of seven regions for GDP – Latin America and the Caribbean, Eastern Europe/Central Asia and Asia East, South East and Pacific – and a positive one for income inequality only in Eastern Europe/Central Asia. At country income level, significant (and negative) associations appear only in the case of GDP for middle-income and high-income countries. A positive but not significant association exists between child burn deaths and income inequality for all three income levels.
Table 2.
Correlation between gross domestic product (GDP) and income inequality and child burn mortality at regional and income level, 2013.
| Country grouping | GDP and burn mortality rate (N = 101) |
Income inequality and burn mortality rate (N = 103) |
||
|---|---|---|---|---|
| r | p | r | p | |
| All | − 0.69 | < 0.01 | 0.44 | < 0.001 |
| Geographic region | ||||
| Sub-Saharan Africa (N = 15) | − 0.26 | 0.34 | 0.15 | 0.59 |
| South Asia (N = 8) | − 0.29 | 0.49 | 0.09 | 0.82 |
| Latin America and the Caribbean (N = 18) | − 0.55 | 0.02 | 0.21 | 0.40 |
| Eastern Europe/Central Asia (N = 26) | − 0.61 | < 0.01 | 0.49 | 0.01 |
| Asia East, South East and Pacific (N = 13) | − 0.59 | 0.03 | 0.01 | 1.00 |
| Middle East and North Africa (N = 4) | 0.4 | 0.6 | 0.40 | 0.60 |
| Organization for Economic Cooperation and Development (OECD) (N = 33) | − 0.10 | 0.58 | 0.28 | 0.12 |
| Country income level | ||||
| High-income (N = 39) | − 0.11 | 0.54 | 0.26 | 0.11 |
| Middle-income (N = 49) | − 0.31 | 0.03 | 0.13 | 0.36 |
| Low-income (N = 14) | − 0.60 | 0.02 | 0.17 | 0.54 |
Fig. 2a and b provide a visualization of this relationship for all countries combined whereby child burn rates decrease as GDP increases, and increase as income inequality increases. The slope of the regression is steeper for GDP compared to income inequality, but with more dispersion within compared to between countries. When stratifying by region there is no consistent or statistically significant pattern present.
Fig. 2.

Association between GDP and income inequality and child burn mortality rate stratified by region, 2013.
a) GDP
Total (R2 = 0.36; p < 0.001); Sub-Saharan Africa (R2 = 0.11; p = 0.22); South Asia (R2 = 0; p = 0.98); Latin America and the Caribbean (R2 = 0.23; p = 0.05); Eastern Europe/Central Asia (R2 = 0.21; p = 0.03); Asia East, South East and Pacific (R2 = 0.11; p = 0.29); Middle East and North Africa (R2 = 0.03; p = 0.82); and OECD (R2 = 0.22; p = 0.01)
b) income inequality
Total R2 = 0.10; p = 0.01; Sub-Saharan Africa R2 = 0.01; p = 0.77; South Asia R2 = 0.46; p = 0.06; Latin America and the Caribbean R2 = 0.02; p = 0.54; Eastern Europe/Central Asia R2 = 0.10; p = 0.12; Asia East, South East and Pacific R2 = 0.06; p = 0.42; Middle East and North Africa R2 = 0.22; p = 0.53; and OECD R2 = 0.09; p = 0.09.
We illustrate this for income levels as well showing a stronger association between GDP versus income inequality and child burn rates (see Fig. 3a and b). Also, for both economic measures there is a high level of dispersion for all countries combined and low- and middle-income countries compared to high income countries.
Fig. 3.
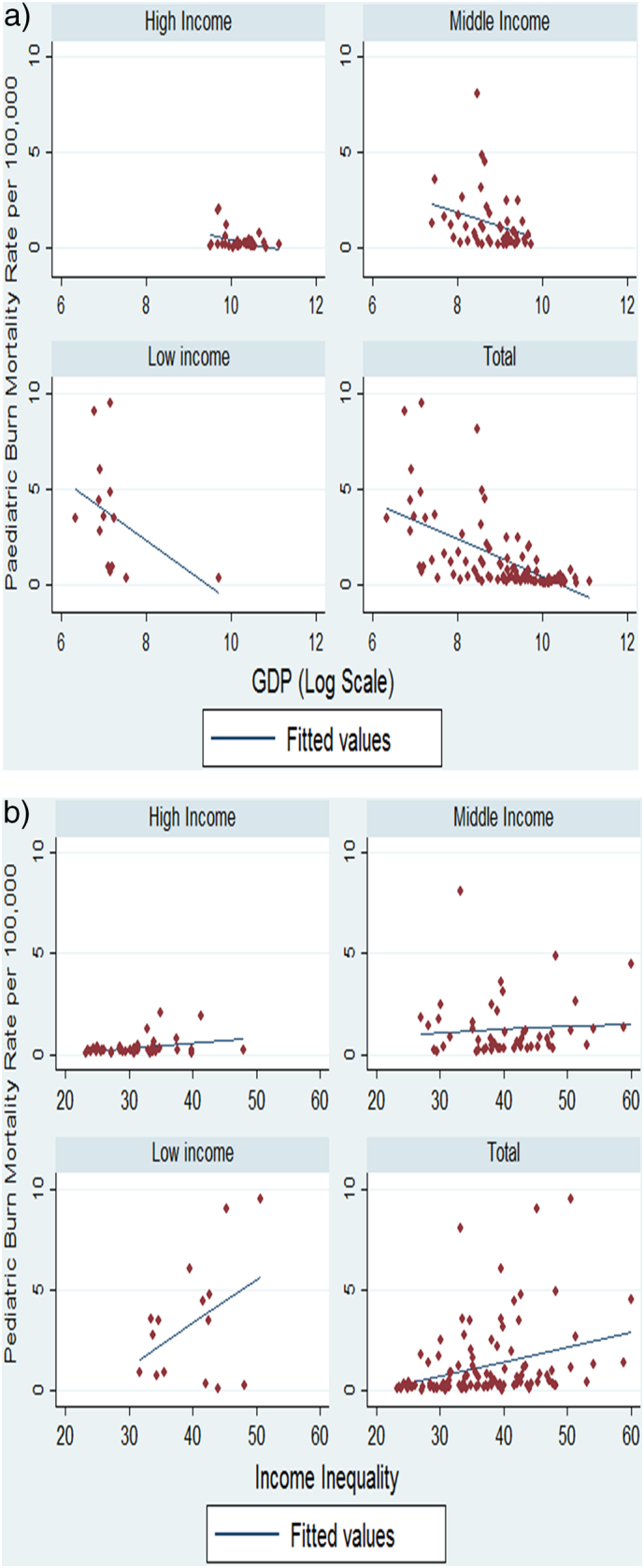
Association between GDP, and income inequality, and child burn mortality stratified by income level, 2013.
a) GDP Total (R2 = 0.36; p < 0.001); high income (R2 = 0.12; p = 0.04); middle income (R2 = 0.08; p = 0.05); low income (R2 = 0.17; p = 0.15).
b) income inequality
Total (R2 = 0.10; p = 0.001); high income (R2 = 0.11; p = 0.04); middle income (R2 = 0.01; p = 0.61); low income (R2 = 0.18; p = 0.12).
4. Discussion
4.1. Main findings
In this study we present the most recent global estimates of child burn mortality due to burn injuries, 2.5 per 100,000 and show the wide regional and country level variations. Sub-Saharan Africa has almost double the mortality rates and the majority of preventable deaths are found in the low income countries of this region, showing how burns are closely linked to poverty–both a source and a consequence of burns. Furthermore, there exists a negative graded association between GDP between countries and child burns for all countries combined and at regional level. But no consistent pattern for income inequality within countries is found at regional level. This may be due to the increase worldwide in within-country inequality that is wider now compared to before, as well as the fact that income inequality continues to have wide variations in levels and trends across regions (World Bank, 2016).
As is the case for a range of injury outcomes (Haagsma et al., 2016) the burden of burn mortality has decreased in the past decade, specifically for children and by as much as 36% globally. The 2004 data found child burns were 11 fold higher in low and middle income countries compared to high income countries, and in the 2013 the gap has narrowed to 7.5 times higher. This may be related to the decreasing trend of extreme poverty levels globally and particularly in East Asia/Pacific and South Asia, but only a marginal decrease in Sub-Saharan Africa which has more poor than all other regions combined (World Bank, 2016). It also reflects the harsh reality of global child poverty as children up to 14 years of age today comprise 44% of the ‘extremely poor’ (Newhouse et al., 2016). These inequalities in progress towards shared prosperity signify a call for action globally and region-specific. This study supports the notion that an essential element in addressing child burn inequalities is the link with economic development, as low income countries continue to bare the largest burden of burn mortality rates in children (Nthumba, 2016). Barriers to care in resource poor settings include limited knowledge of first aid for burns, long distances to reach these services and poor transport systems from the rural to the urban areas where specialized burn care is available; if accessed there is then the issue of limited supplies, beds and staff in burn centers (Ndiritu et al., 2006). Multi-pronged community-based interventions were found to be most effective in child burn prevention programmes, in both low and high resource settings, and adapting effective hazard reduction programs to informal settlements was particularly important in South Africa (Parbhoo et al., 2010).
In South Asia, South East and Pacific, Latin American and the Caribbean and Asia East the higher mortality rates in the middle income group may reflect the epidemiological shift to development issues that are detrimental to child home safety (e.g. migration to urban environments with high population density and precarious living conditions, not least for heating and cooking food), as well differential access to health care. A recent systematic review of burn management capacity found that hospitals in low and middle income countries have the competence and infrastructure for initial burn management and resuscitation, but lack infrastructure and capacity to deliver burn care (Parbhoo et al., 2010). Burn management criteria and strategies are needed to guide practitioners in countries with limited resources for advanced burn care, particularly innovative solutions for pain management in child burns (Gupta et al., 2014, Atiyeh et al., 2009). In the African region research at the individual level found no clear association was found between burn injuries and socioeconomic factors (e.g. number of children, place of residence, occupation, income, types of fuels/appliances in the home) (Atiyeh et al., 2010). Region-specific research is therefore needed that can shed light on the macro-level mechanisms at play in the high risk countries and possibly also clarify why country level income inequality is associated with rates of burn mortality overall but not at regional level.
4.2. Study strengths and limitations
This study provides the most recent global update of the global distribution of child burn mortality, and to the best of our knowledge, this study is the first to assess how both country economic level and income inequality relate to child burn mortality. The Global Burden of Disease 2013 data provide robust mortality estimates and their strengths and limitations are discussed elsewhere (IHME Protocol, 2013). As is the case for global studies of the like, data from several countries are missing, mainly low and middle income ones, which weakens the strengths of our conclusions. Another issue is that the countries that do provide data may have numerator and denominator information of different quality but how this affects our comparisons for groups of countries is uncertain. Furthermore, no comparisons could be made regarding the downward trend and reduction in the differences between high and low income countries with other data sources, such as the World Health Organization (WHO) Mortality Database, as the WHO injury codes for burns do not include contact with heat and hot substances, which are classified under ‘all other external causes of death.’
4.3. Implications
The gap in the rates of child burn mortality between low-middle income and high-income countries, although reduced in the past decade is unnecessarily high and the excess rates found in middle income countries in some – rapidly developing – regions of the world is worrying. Burn injury is highly preventable, as shown by the low mortality rates in high-income countries in this study, and the means are to be found in measures that contribute to reduce child exposure to fire hazards – most importantly in the home environment, to protect when danger is present (e.g. fire blankets, non-flammable clothing, etc.) and to provide good quality health care rapidly (Laflamme et al., 2009). Still today the child mortality burden of burns and potential for lives saved is high, particularly in Sub Saharan Africa region where low income countries are far more affected. There is an urgent need for regional and national injury prevention action plans in Sub-Saharan Africa as expected, but also in middle income countries which show larger rates in certain regions. These plans have to combine a range of micro and macro level strategies at the local, national and regional level to benefit all children, and targeted efforts tailored to the most vulnerable areas and households.
How higher levels of country economic development is associated with improvements in children's reduced burn risk appears region specific. Furthermore, it is unclear why GDP as an economic measure between countries seems to offer a better explanation at regional level than income inequality within a country as found in other research (Rybarczyk et al., 2017). Country level analyses on low and middle income countries did not find an association between income inequality and a wider health gap between rich and poor, suggesting that improving the wealth of poor households may be more effective for improving overall health than measures to reduce inequality (Pickett & Wilkinson, 2015b). Improved wealth would lead to better living conditions, nutrition and access to medical services, markers of key social determinants of health (Peden et al., 2008, Peck, 2011, Bell et al., 2013, Commission on Social Determinants of Health, 2008, van Deurzen et al., 2014, Jutz, 2015). Due to the high burn rates in Sub-Saharan Africa, this is especially relevant for these countries. In addition, the quality of governance in Sub-Saharan Africa must be addressed as public spending on health has been found to be twice as effective in reducing under-five mortality in the Sub-Saharan African countries with good quality of governance compared to the countries with poor quality of governance (Semyonov et al., 2013, Kipp et al., 2016, Makuta and O'Hare, 2015).
5. Conclusion
Global inequalities exist in child burn injuries with the highest death rates in Sub-Saharan Africa and the mortality rate almost eight-fold higher in low and middle income countries compared to high income countries. Investment in safe living conditions and equitable access to medical care are a priority for achieving further reductions in the global burden of preventable child burn deaths.
The following is the supplementary data related to this article.
Child burn mortality rate by country from the Global Burden of Disease Study 2013.
Conflict of interest statement
The authors declare that there are no conflicts of interest.
Contributor Information
Mathilde Sengoelge, Email: mathilde.sengoelge@ki.se.
Ziad El-Khatib, Email: ziad.el-khatib@ki.se.
Lucie Laflamme, Email: lucie.laflamme@ki.se.
References
- Alonge O., Hyder A.A. Reducing the global burden of childhood unintentional injuries. Arch. Dis. Child. 2014;99:62–69. doi: 10.1136/archdischild-2013-304177. [DOI] [PubMed] [Google Scholar]
- Atiyeh B.S., Costagliogla M., Hayek S.N. Burn prevention mechanisms and outcomes: pitfalls, failures and successes. Burns. 2009;35:181–193. doi: 10.1016/j.burns.2008.06.002. [DOI] [PubMed] [Google Scholar]
- Atiyeh B.S., Masellis A., Conte F. Optimizing burn treatment in developing low-and middle-income countries with limited health care resources (part 3) Ann. Burns Fire Disasters. 2010;XXIII(1):13–18. [PMC free article] [PubMed] [Google Scholar]
- Bell R., Donkin A., Marmot M. Florence; UNICEF: 2013. Tackling Structural and Social Issues to Reduce Inequities in Children's Outcomes in Low- to Middle-income Countries. [Google Scholar]
- Burrows S., van Niekerk A., Laflamme L. Fatal injuries among urban children in South Africa: risk distribution and potential for reduction. Bull. World Health Organ. 2010;88(4):267–272. doi: 10.2471/BLT.09.068486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Byass P., de Courten M., Graham W.J. Reflections on the global burden of disease 2010 estimates. PLoS Med. 2013;10(7) doi: 10.1371/journal.pmed.1001477. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Commission on Social Determinants of Health . World Health Organization; Geneva: 2008. Closing the Gap in a Generation: Health Equity Through Action on the Social Determinants of Health. [DOI] [PubMed] [Google Scholar]
- van Deurzen I., van Oorschot W., van Ingen E. The link between inequality and population health in low and middle income countries: policy myth or social reality? PLoS One. 2014;9(12) doi: 10.1371/journal.pone.0115109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- GBD 2013 Mortality and Causes of Death Collaborators Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;385(9963):117–171. doi: 10.1016/S0140-6736(14)61682-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Global Burden of Disease Study 2013 Collaborators Global, regional, and national disability-adjusted life years (DALYs) for 306 diseases and injuries and healthy life expectancy (HALE) for 188 countries, 1990–2013: quantifying the epidemiological transition. Lancet. 2015;386(9995):743–800. doi: 10.1016/S0140-6736(15)61340-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gupta S., Wong E.G., Mahmood U., Charles A.G., Nwomeh B.C., Kushner A.L. Burn management capacity in low and middle income countries: A systematic review of 458 hospitals across 14 countries. Int. J. Surg. 2014;12(10):1070–1073. doi: 10.1016/j.ijsu.2014.08.353. [DOI] [PubMed] [Google Scholar]
- Haagsma J.A., Graetz N., Bolliger I. The global burden of injury: incidence, mortality, disability-adjusted life years and time trends from the global burden of disease study 2013. Inj. Prev. 2016;22(1):3–18. doi: 10.1136/injuryprev-2015-041616. [DOI] [PMC free article] [PubMed] [Google Scholar]
- IHME Protocol GBD 2013: Global Burden of Diseases, Injuries, and Risk Factors. 2013. http://www.healthdata.org/sites/default/files/files/GBD_2013_Protocol.pdf Available: (Date of access 23 December 2015)
- Jutz R. The role of income inequality and social policies on income-related health inequalities in Europe. Int. J. Equity Health. 2015;14(1):117. doi: 10.1186/s12939-015-0247-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khan U.R., Sengoelge M., Zia N., Razzak J.A., Hasselberg M., Laflamme L. Country level economic disparities in child injury mortality. Arch. Dis. Child. 2015;100(Suppl. 1):S29–S33. doi: 10.1136/archdischild-2013-305847. Feb. [DOI] [PubMed] [Google Scholar]
- Kipp A.M., Blevins M., Haley C.A. Factors associated with declining under-five mortality rates from 2000 to 2013: an ecological analysis of 46 African countries. BMJ Open. 2016;6(1) doi: 10.1136/bmjopen-2015-007675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Laflamme L., Sethi D., Burrows S., Hasselberg M., Racioppi F., Apfel F. World Health Organization; Copenhagen: 2009. Addressing the Socioeconomic Safety Divide: A Policy Briefing. [Google Scholar]
- Makuta I., O'Hare B. Quality of governance, public spending on health and health status in Sub Saharan Africa: a panel data regression analysis. BMC Public Health. 2015;15:932. doi: 10.1186/s12889-015-2287-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ndiritu S., Ngumi Z.W.W., Nyaim O. Burns: the epidemiological pattern, risk and safety awareness at Kenyatta National Hospital, Nairobi. East Afr. Med. J. 2006;83(8):455–460. doi: 10.4314/eamj.v83i8.9462. [DOI] [PubMed] [Google Scholar]
- Newhouse D., Suarez-Becerra P., Evans M.C. Policy Research Working Paper 7845. World Bank; Washington, DC: 2016. New estimates of extreme poverty for children. [Google Scholar]
- Nthumba P.M. Burns in sub-Saharan Africa: a review. Burns. 2016;42(2):258–266. doi: 10.1016/j.burns.2015.04.006. [DOI] [PubMed] [Google Scholar]
- Othman N., Kendrick D. Epidemiology of burn injuries in the East Mediterranean Region: a systematic review. BMC Public Health. 2010;10:83. doi: 10.1186/1471-2458-10-83. Feb 20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Parbhoo A., Louw Q.A., Grimmer-Somers K. Burn prevention programs for children in developing countries require urgent attention: a targeted literature review. Burns. 2010;36(2):164–175. doi: 10.1016/j.burns.2009.06.215. [DOI] [PubMed] [Google Scholar]
- Peck M.D. Epidemiology of burns throughout the world. Part I: distribution and risk factors. Burns. 2011;37:1087–1100. doi: 10.1016/j.burns.2011.06.005. [DOI] [PubMed] [Google Scholar]
- Peden M., Oyegbite K., Ozanne-Smith J. World Health Organization; Geneva: 2008. World Report on Child Injury Prevention. [PubMed] [Google Scholar]
- Pickett K.E., Wilkinson R.G. The ethical and policy implications of research on income inequality and child well-being. Pediatrics. 2015;135(Suppl. 2):S39–S47. doi: 10.1542/peds.2014-3549E. [DOI] [PubMed] [Google Scholar]
- Pickett K.E., Wilkinson R.G. Income inequality and health: a causal review. Soc. Sci. Med. 2015;128:316–326. doi: 10.1016/j.socscimed.2014.12.031. [DOI] [PubMed] [Google Scholar]
- Rybarczyk M.M. A systematic review of burn injuries in low- and middle-income countries: epidemiology in the WHO-defined African Region. Afr. J. Emerg. Med. 2017 doi: 10.1016/j.afjem.2017.01.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Semyonov M., Lewin-Epstein N., Maskileyson D. Where wealth matters more for health: the wealth-health gradient in 16 countries. Soc. Sci. Med. 2013;81:10–17. doi: 10.1016/j.socscimed.2013.01.010. [DOI] [PubMed] [Google Scholar]
- Sengoelge M., Elling B., Laflamme L., Hasselberg M. Country-level economic disparity and child mortality related to housing and injuries: a study in 26 European countries. Inj. Prev. 2013;19(5):311–315. doi: 10.1136/injuryprev-2012-040624. [DOI] [PubMed] [Google Scholar]
- Sengoelge M., Hasselberg M., Ormandy D., Laflamme L. Housing, income inequality and child injury mortality in Europe: a cross-sectional study. Child Care Health Dev. 2014;40(2):283–291. doi: 10.1111/cch.12027. [DOI] [PubMed] [Google Scholar]
- Solt Frederick. The standardized world income inequality database. Soc. Sci. Q. 2016;97(5):1267–1281. [Google Scholar]
- StataCorp . StataCorp LP; College Station, TX: 2011. Stata Statistical Software: Release 12. [Google Scholar]
- The World Bank Available: http://data.worldbank.org (Date of access 23 December 2015)
- United Nations World Population Prospects. 2015. https://esa.un.org/unpd/wpp/ Revision. (Date of access 15 December 2015)
- World Bank . World Bank; Washington, DC: 2016. Poverty and Shared Prosperity 2016: Taking on Inequality. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Child burn mortality rate by country from the Global Burden of Disease Study 2013.