

Abstract
Roughly 10% of lung transplant recipients experience airway complications. Although the incidence has decreased dramatically since the first lung transplants were performed in the 1960s, airway complications have continued to adversely affect outcomes. Bronchoscopic interventions such as balloon dilation, airway stenting, and endobronchial electrocautery play an important role in ameliorating the morbidity and mortality associated with these complications. This review describes the array of bronchoscopic interventions used to treat airway complications after lung transplant and how these techniques can be used in nontransplant settings as well.
Keywords: lung transplant, airway stenosis, bronchomalacia, balloon dilation, endobronchial cryotechniques, endobronchial electrocautery
Introduction
Airway anastomotic complications were a significant source of early morbidity/mortality in the years following the first lung transplant (LT) in 1963, with the reported incidence higher than 50%.1–5 The arrival of cyclosporine in the 1980s, which allowed for a steroid-sparing regimen, and the refinement of surgical techniques both helped to reduce airway complications. In the 1980s, balloon catheter dilation was first reported to provide palliative benefit in patients with acquired bronchial stenosis associated with sleeve resection, tuberculosis, and sarcoidosis.6 Keller and Frost described a simple adjunct technique for the management of bronchial stenosis following lung transplantation performed at Houston Methodist Hospital.7
Airway Complications in Lung Transplant Recipients
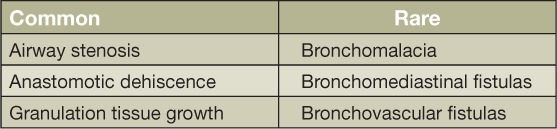
Airway stenosis, anastomotic dehiscence, and granulation tissue growth are the common airway complications in LT recipients, while bronchomalacia, bronchomediastinal fistulas, and bronchovascular fistulas are uncommon airway complications (Table 1). About one in every ten LT recipients is affected with an airway complication.8
Table 1.
Airway complications in lung transplant recipients.
Airway stenosis may occur at the anastomoses or at a nonanastomotic location. Examples of nonanastomotic locations are bronchus intermedius (leading to vanishing airway syndrome) and lobar ostia. Airway ischemia is the likely mechanism, as there is a lack of bronchial artery revascularization in LT recipients, and the airway tissue depends on the retrograde flow from pulmonary vasculature. Other common mechanisms are infections and surgical technique. During the previous 2 years (2014–2015), the incidence of airway stenosis has been 5% at Houston Methodist Hospital. Onset generally is 1 to 2 months posttransplant. Periodic interventions with a combination of dilation, stent, and/or argon plasma coagulation or cryotechniques are needed. By 1 year, most stenoses are resolved. The incidence of anastomotic dehiscence has been 2.3% at Houston Methodist Hospital over the previous 2 years (2014–15). An uncovered metal stent may be placed to stimulate closure of leaks through granulation tissue growth. Tissue patch repair may be needed for large dehiscence.
Granulation tissue growth may respond to periodic cryodestruction, electrocautery knife, and argon plasma coagulation interventions. Bronchomalacia may respond to overall improvement in the LT patient's medical and nutritional condition and may occasionally respond to bronchial stent placement. There has been a significant improvement in airway complications and outcomes over the years due to improved surgical techniques, meticulous antibiotic prophylaxis, frequent bronchoscopies for pulmonary toileting, and routine use of intervention pulmonary techniques.
Common Transplant Pulmonary Interventions
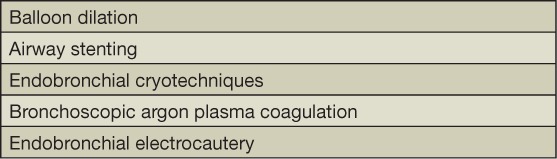
Common transplant pulmonary interventions are balloon dilation, airway stenting, endobronchial cryotechniques, bronchoscopic argon plasma coagulation, and endobronchial electrocautery (Table 2).
Table 2.
Transplant pulmonary interventions
Balloon dilation is a simple and rapid method to dilate a stenosis. It may be used alone or in conjunction with cryotherapy, electrocautery, and postdilation stenting. If longer procedural time is expected due to severity of lesions, general anesthesia may be preferable. Different configurations of inflated outer diameters are available. A bronchoscope with a working channel diameter of 2.8 mm is needed. Symptomatic improvement is often immediate, but periodic dilatations may be needed every 2 to 4 weeks (Figure 1). Transient, self-limited hemorrhage is common and easily responds to epinephrine instillation or argon plasma coagulation.
Figure 1.
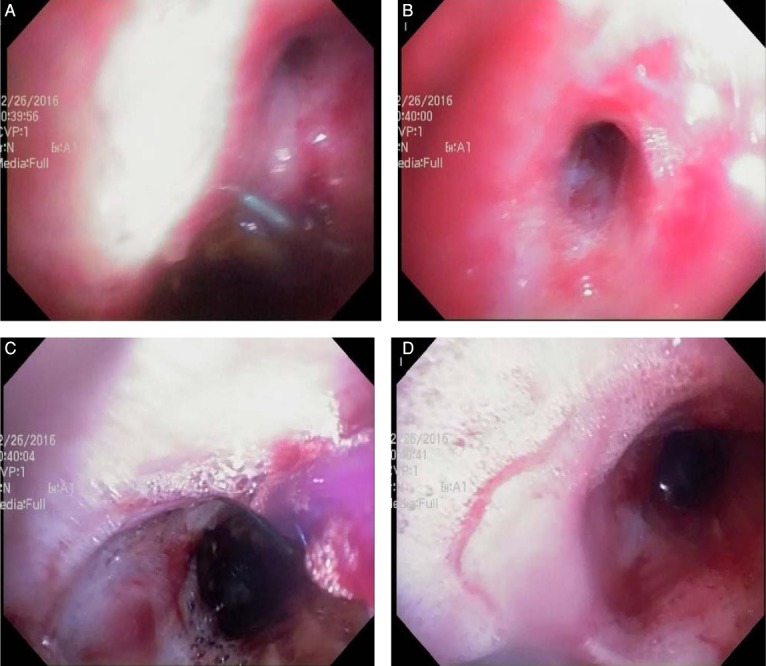
(A, B) Right upper lobe stenosis. (C) A 10-mm balloon dilator was placed and inflated in the right upper lobe bronchus. (D) Post-dilatation. A metal stent is noted in bronchus intermedius.
Airway stenting is of three types: (1) silicone, which needs a rigid bronchoscopy, (2) metal, which is self-expanding and resists extrinsic compression, and (3) hybrid, a combination of metal and a material such as silicone or polyurethane that resists extrinsic compression and minimizes ingrowth of granulation tissue due to metal. Common stents used in lung transplantation are metal or hybrid, with the metal part made of nitinol (nickel-titanium alloy). Nitinol has shape memory: It expands as it warms up to body temperature. Airway stents in bronchi can be placed using a therapeutic bronchoscope. Fluoroscopy is used with a metallic marker attached to the chest wall to correspond to the desired distal stent location. The stent is placed over a guidewire into the airway. Resolution of symptoms is substantial and immediate using a mainstem bronchial stenting with a maximal internal diameter of at least 10 mm. Hybrid stents often get coated and plugged with mucus, and granulation tissue ingrowth is a challenge with metal stents. Stents also can migrate and become colonized with organisms.
Endobronchial cryotechniques work by contact through a liquid nitrogen-cooled probe. This causes cell death through intracellular ice crystal formation. Necrosis and sloughing off take days to occur after cryodestruction.
Argon plasma coagulation is often used to achieve hemostasis. Argon plasma is expelled from a probe, and a high-voltage current is passed along the probe. There is a risk of airway fire, which is avoided by reducing fractional oxygen concentration to below 40%. There are rare case reports of gas embolism.
Endobronchial electrocautery works through electrical as well as thermal effects. An electrocautery knife can be used to enhance the effectiveness of balloon dilation through radial cuts. Granulation tissue debulking can be done using a snare or knife.
Applications in Nontransplant Patients
Airway lesions leading to symptomatic airway stenosis can be encountered in granulomatosis polyangiitis, tuberculosis, sarcoidosis, carcinoid, and malignancies. Electrocautery snare can be used to resect a carcinoid lesion. Hybrid stents can be useful in plugging a bronchomediastinal fistula resulting from impaired wound healing after a lobectomy. Periodic balloon dilation can be used in palliation of malignant strictures.
Conclusion
Common transplant interventions play an important role in improving posttransplant morbidity and mortality in lung transplant recipients and also have utility in several nontransplant indications.
Key Points
Airway complications are common in lung transplant recipients.
Common transplant bronchoscopic interventions play an important role in improving posttransplant morbidity and mortality in lung transplant recipients.
Bronchoscopic interventions also find usefulness in several nontransplant indications.
Conflict of Interest Disclosure
The author has completed and submitted the Methodist DeBakey Cardiovascular Journal Conflict of Interest Statement and none were reported.
References
- 1. Kapoor BS, May B, Panu N, Kowalik K, Hunter DW.. Endobronchial stent placement for the management of airway complications after lung transplantation. J Vasc Interv Radiol. 2007; 18( 5): 629– 32. [DOI] [PubMed] [Google Scholar]
- 2. Mulligan MS. Endoscopic management of airway complications after lung transplantation. Chest Surg Clin N Am. 2001. November; 11( 4): 907– 15. [PubMed] [Google Scholar]
- 3. Lonchyna VA, Arcidi JM Jr, Garrity ER Jr, . et al. Refractory post-transplant airway strictures: successful management with wire stents. Eur J Cardiothorac Surg. 1999; 15: 842– 9. [DOI] [PubMed] [Google Scholar]
- 4. Kshettry VR, Kroshus TJ, Hertz MI, . et al. Early and late airway complications after lung transplantation: incidence and management. Ann Thorac Surg. 1997. June; 63( 6): 1576– 83. [DOI] [PubMed] [Google Scholar]
- 5. Alvarez A, Algar J, Santos F, . et al. Airway complications after lung transplantation: a review of 151 anastomoses. Eur J Cardiothorac Surg. 2001. April; 19( 4): 381– 7. [DOI] [PubMed] [Google Scholar]
- 6. Carlin BW, Harrell JH 2nd, Moser K.. The treatment of endobronchial stenosis using balloon catheter dilation. Chest. 1988. June; 93( 6): 1148– 51. [DOI] [PubMed] [Google Scholar]
- 7. Keller C, Frost A.. Fiberoptic bronchoplasty: description of a simple adjunct technique for the management of bronchial stenosis following lung transplantation. Chest. 1992. October; 102( 4): 995– 8. [DOI] [PubMed] [Google Scholar]
- 8. Yserbyt J, Dooms C, Vos R, Dupont LJ, Van Raemdonck DE, Verleden GM.. Anastomotic airway complications after lung transplantation: risk factors, treatment modalities and outcome-a single-centre experience. Eur J Cardiothorac Surg. 2016. January; 49( 1): e1– 8. [DOI] [PubMed] [Google Scholar]