

Abstract
Background:
This study aimed to compare the percentage of detection of periarthritis in patients with rheumatoid arthritis using clinical examination and ultrasound methods.
Materials and Methods:
This study is a cross-sectional study which was conducted in Al-Zahra Hospital (Isfahan, Iran) during 2014–2015. In our study, ninety patients were selected based on the American College of Rheumatology 2010 criteria. All patients were examined by a rheumatologist to find the existence of effusion, and the data were filled in the checklist. The ultrasonography for detecting effusion in periarticular structures was done by an expert radiologist with two methods, including high-resolution ultrasonography and power Doppler. The percentage of effusion existence found by physical examination was compared by sonography, and the Chi-square and t-tests were used for data analysis.
Results:
The percentage of effusion found in areas with physical examination by rheumatologist was lower than the frequency distribution of effusions found by sonography (8.3% VS 14.2%) (P < 0.001). In sonography, rotator cuff tendonitis is the most common periarthritis. Other findings in sonography were biceps tendinitis (10 cases), wrist tendonitis (13 cases), olecranon bursitis (9 cases), golfers elbow (4 cases), tennis elbow (4 cases), trochanteric bursitis (6 cases), anserine bursitis (6 cases), prepatellar bursitis (11 cases), and ankle tendonitis (7 cases). Tenderness on physical examination was found in 15% of the cases, and the evidence of periarthritis was found in 21/7% through sonography (P < 0.001) and 34% through Doppler sonography (P < 0.001).
Conclusion:
The percentage of periarthritis detection by ultrasonography and power Doppler sonography was higher than clinical examination. Hence, the ultrasonography is more accurate than physical examination.
Keywords: Periarthritis, rheumatoid arthritis, ultrasonography
INTRODUCTION
Rheumatoid arthritis is the most common inflammatory arthritis affecting approximately 1% of the population. Although this disease primarily affects the joints, due to abnormal systemic immune response, it can produce various extra-articular manifestations. The disease is a chronic autoimmune inflammatory process that its main feature is extensive involvement of the synovium, joint inflammation, and destruction that in case of lack of control, lead to destruction of cartilage, bones, ligaments, bursa, and tendons, etc., which in some cases results in the disability of the patients.[1,2] In addition to the involvement of large and small joints symmetrically, it can lead to periarthritis, tenosynovitis, tendon injuries, bursitis, enthesitis, and finally the joint erosion.
Typically, the diagnosis and determination of the activity have been performed by clinical symptoms and laboratory findings. Therefore, clinical assessment is not completely acceptable. The best way to prevent debilitating complications and high cost of treatment is to control the symptoms and complications of the disease. High-frequency ultrasound (HFUS) as one of the imaging methods has many diagnostic applications and can improve musculoskeletal imaging in rheumatology. In this way, high-resolution images of the anatomic structures of more than 0.1 mm can be seen. HFUS is also more sensitive than clinical examination in the diagnosis of periarthritis, and it can be done repeatedly and can improve clinical assessment. Sonography is well tolerated by patients and has no side effects. We can find specific findings using ultrasound that cannot be found by simple physical examination and history taking. Power Doppler sonography (PDUS) is a new imaging method that results in improved sensitivity for blood flow in small vessels and blood flow of low velocity. With this method, we can find indirectly the signs of increased vascularization in inflammatory processes and diseases.[3] Naredo et al. in 2005 reported that ultrasonography in the diagnosis of periarthritis in the glenohumeral joint, sternoclavicular, acromioclavicular, knees, elbows, and hands was a more sensitive method than clinical examination. The ultrasound findings are more relevant to paraclinical tests.[4]
In a study by Schmit in 2014, ultrasonography was mentioned as a complementary tool to assess rheumatoid arthritis including periarthritis.[5] In another study by McAlindon et al. at the American College of Rheumatology, patients with mechanical symptoms of pain and swelling without obvious clinical signs underwent sonography examination of glenohumeral, sternoclavicular, acromioclavicular, elbows, knees, ankles, and hips. In this study, sonography was considered as an alternative method for examination with a high sensitivity.[6] In a study by Hermann et al. which was carried out on the shoulder joint, sonography has been proposed as an alternative method in the evaluation of the shoulder joint, especially in the early diagnostic stages.[7] In 2001, guidelines in musculoskeletal sonography were proposed as an alternative of early diagnosis of upper extremity periarthritis, and treatment has been proposed.[8] In another study conducted in 2006 by Naredo et al., periarticular sonography has been proposed as a good interventional method for diagnosis.[9] In a study by Boutry et al., sonography has been proposed as an early diagnostic method.[10] Despite the cited cases, the current use of sonography in the evaluation of periarthritis in rheumatoid arthritis is controversial due to the lack of adequate studies and findings in the field. Given that sonography is more sensitive than clinical assessment in the diagnosis of periarthritis and also because the method is cheap, accessible, and without complications, it can be used as a supplement or even replace clinical methods used for diagnosis. This study aimed to compare periarthritis detection in patients with rheumatoid arthritis by two clinical and sonography methods because any study about periarthritis was not performed in Iran.
MATERIALS AND METHODS
This cross-sectional study was conducted in Al-Zahra Medical Center (Isfahan, Iran) during 2014–2015. The study patients were those with confirmed rheumatoid arthritis who referred to the outpatient clinic.
Patients referred to the rheumatology clinic with defined rheumatoid arthritis based on a diagnosis by expert rheumatologist according to the American College of Rheumatology criteria (2010) were selected for the study. Exclusion criteria included a history of knee surgery 1 year ago, crystal periarthritis and traumatic periarthritis history in the past year, and a history of septic periarthritis (i.e., infective olecranon bursitis) in the last year.
Required sample size
The sample size of the study was calculated using sample size formula for prevalence studies and taking into account the 95% confidence level and the estimated error rate of 0/05; a total of ninety people were estimated that the sampling of these patients was done consecutively from patients with inclusion criteria and they were included in the study until the sample size was reached.
Methods
The diagnosis of rheumatoid arthritis was based on the American College of Rheumatology 2010 criteria by rheumatologist and clinical examination findings (such as tenderness, decreased passive range of motion). Demographic characteristics such as age, sex, disease duration, test results of anticyclic citrullinated peptide (Anti-CCP) and rheumatoid factor (RF) assayed by enzyme-linked immunosorbent assay, C-reactive protein (assayed by immunoassay), and erythrocyte sedimentation rate in the form of data collection were recorded. Furthermore, effusion, tenderness, and decreased passive range of motion are the manifestations of periarthritis in physical examination.
Before completing the questionnaire and sonography, informed consent forms were completed by patients. Sonography of periarticular structures was done by an expert radiologist using two methods, i.e., high-resolution ultrasonography and power Doppler. Ultrasonography was done by linear probe with a frequency range of 7.5–15 MHz (this probe was selected because of the broad superficial field of view and near resolution). The aim of applying two methods of ultrasonography was to determine the sensitivity on the methods. Both radiologist and rheumatologist were blinded to each other. Hyperechoic, band-like, ligament, diffuse thickening and enlargement of tendon, and fluid-filled collection with a well-defined margin are signs of bursitis. Evaluated periarticular structures include the shoulder (long head of biceps tendon, supra and infraspinatus, subscapularis, subacromial tendons and scapularis bursa, and rotator cuff), elbow (olecranon bursa to review bursitis, flexor and extensor tendons binding to internal and external epicondyle including tennis elbow and golfers elbow), wrist (flexor carpi ulnaris and flexor carpi radialis tendon to review tendinitis), hips (trochanteric bursa to check out the trochanteric bursitis), knee (anserine and prepatellar bursa to review bursitis), and ankle (anterior extensor tendon to investigate tendinitis).
Data analysis
The collected data were analyzed with Statistical Package for Social Sciences software (SPSS) version 23 manufactured in International Business Machines Corporation, USA. To describe the data, mean (± standard deviation) and percentage (frequency) were used, and to analyze the data, Chi-square and t-tests were used. Because both clinical examination and ultrasonography were done on the same patients, any bias was controlled in our study.
RESULTS
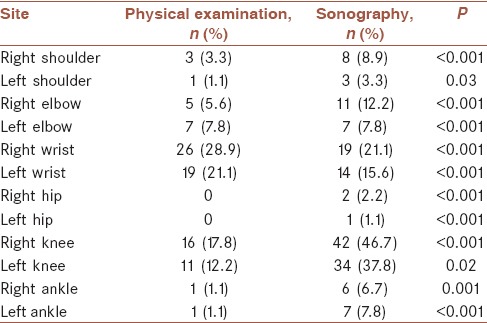
In this study, ninety patients referred to the rheumatology clinic of AlZahra Hospital were studied. The mean age of patients was 49.79 ± 4.5 years with a range of 25–72. Thirteen (14/4%) patients were male and 77 (85/6%) were female. Mean duration of disease was 10 years. Joints morning stiffness duration was 46 min on average. RF in 77% and Anti-CCP in 66/7% patients were positive. In this study, except for the wrist, the percentage of effusion found in areas with physical examination by rheumatologist was lower than the percentage of effusions found by sonography (8/3% vs. 14.2%) (P < 0.001). However, in the left and right wrists, the reported effusion volume by the examiner was greater than ultrasonographic method [Table 1].
Table 1.
Comparison of effusion in physical examination and sonography
In Figure 1, the frequency of periarthritis found in sonography has shown that rotator cuff tendonitis is the most common periarthritis. Others were biceps tendinitis (10 cases), wrist tendonitis (13 cases), olecranon bursitis (9 cases), golfers elbow (4 cases), tennis elbow (4 cases), trochanteric bursitis (6 cases), anserine bursitis (6 cases), prepatellar bursitis (11 cases), and ankle tendonitis (7 cases). Although tenderness on physical examination was found in 15% of the cases, periarthritis was found in 21/7% through sonography (P < 0.001) and in 34% through Doppler sonography (P < 0.001) [Table 2].
Figure 1.
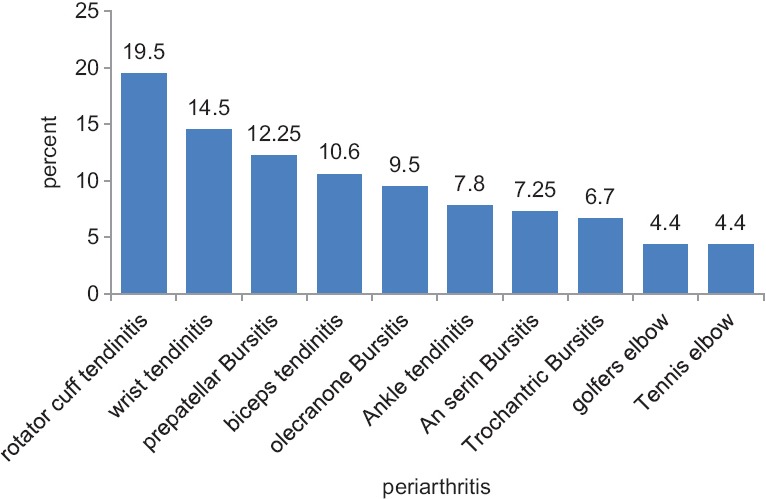
Frequency of periarthritis in sonography
Table 2.
Comparison of periarthritis in physical examination and ultrasonography and Doppler sonography
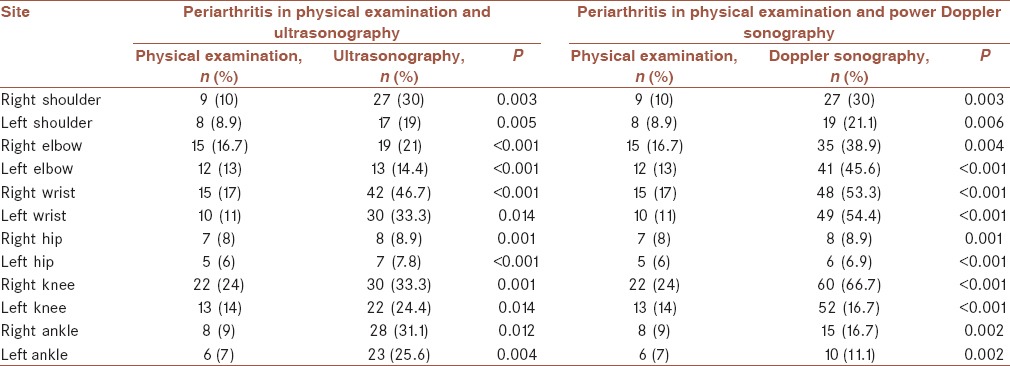
Periarthritis was found in 21/7% and 34% of the cases by high-resolution sonography and PDUS, respectively (P < 0.001).
DISCUSSION
The aim of this study was to compare periarthritis in patients with rheumatoid arthritis with clinical examination and sonography in Al-Zahra Hospital in 2014–2015. In this study, ninety patients referred to the rheumatology clinic in Al-Zahra underwent sonographic examination and then studied accordingly. In this study, the percentage of effusion found on examination in all areas other than the wrist was lower than percentage found through sonography which was in line with the study done by Nared et al. and McAlindon et al.[4,6] The rheumatologist did not report specifically periarthritis in any of these areas, but sonography reported periarthritis. Tenderness as a positive point for the presence of periarthritis was found in only 15% of the cases, but evidence of periarthritis in sonography was seen in 21/7%; in the comparison of the two methods, sonography was more sensitive than clinical examination which indicates that it was consistent with the findings of Naredo et al. and McAlindon et al.[4,6] It also found that tenderness on physical examination compared with the evidence of periarthritis in power Doppler ultrasound suggests more cases of periarthritis indicates higher sensitivity in the evaluation of power Doppler ultrasound for periarthritis that it was consistent with the findings of Boutry et al. and Hermann et al.[7,10] The PDUS reported periarthritis in 34% of the cases and high-resolution sonography reported periarthritis in 21/7% of the cases, indicating a higher sensitivity of PDUS than high-resolution sonography. The above findings are consistent with Boutry et al. as well as Hermann et al. and also the musculoskeletal guidelines that had been introduced in 2001.[7,8,10] Furthermore, in rheumatology reference books such as Kelley's and Hochberg and Silman, sonography is introduced as a high-resolution method for periarthritis in early rheumatoid arthritis which is not visible on clinical examination.[1,2] Evidence of periarthritis involving tendinitis and bursitis is found in the early stages of the disease, and sometimes more conflict areas were found in sonography than the clinical examination. As a result, physicians diagnose and start treatment sooner and prevent complications of the disease before symptoms appear during physical examination.[11,12,13] Our study results confirmed the above-mentioned services. Considering the above results, the rate of detection of periarthritis by ultrasonography and was higher than clinical examination.
CONCLUSION
Long-term rheumatoid arthritis has high morbidity and mortality rates and can lead to disability of patients. It is recommended that sonography should be conducted for all patients with rheumatoid arthritis in the early stage of clinical diagnosis.
Financial support and sponsorship
This study was supported by Isfahan University of Medical Sciences, Isfahan, Iran (Research Project Number: 394665).
Conflicts of interest
There are no conflicts of interest.
AUTHORS’ CONTRIBUTION
Contributed in the conception of the work, conducting the study, revising the draft, approval of the final version of the manuscript, and agreedfor all aspects of the work. ZSB: contributed in the conception of the work, drafting and revising the draft, approval of the final version of the manuscript, and agreed for all aspects of the work. MM: contributed in the conception of the work, drafting and revising the draft, approval of the final version of the manuscript, and agreed for all aspects of the work. MK: contributed in the conception of the work, drafting and revising the draft, approval of the final version of the manuscript, and agreed for all aspects of the work.
REFERENCES
- 1.Garys F, Ralph C. Kelleys Text Book of Rhomatology. 9th ed. Philadelphia: Elsevier Saunders Pub; 2013. pp. 1059–137. [Google Scholar]
- 2.Hochberg MC, Silman A. Rheumatology. 5th ed. Philadelphia: Elsevier Mosby Pub; 2014. pp. 823–971. [Google Scholar]
- 3.Andrea DS, Lucrezia R, Stefano B. Ultrasound in the diagnosis and management of rheumatic disease. Ch. 13. 2008;18:155–63. [Google Scholar]
- 4.Naredo E, Bonilla G, Gamero F, Uson J, Carmona L, Laffon A. Assessment of inflammatory activity in rheumatoid arthritis: A comparative study of clinical evaluation with grey scale and power Doppler ultrasonography. Ann Rheum Dis. 2005;64:375–81. doi: 10.1136/ard.2004.023929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Schmidt WA. Ultrasound in rheumatology. Int J Rheum Dis. 2014;17:711–5. doi: 10.1111/1756-185X.12545. [DOI] [PubMed] [Google Scholar]
- 6.McAlindon T, Kissin E, Nazarian L, Ranganath V, Prakash S, Taylor M, et al. American College of Rheumatology report on reasonable use of musculoskeletal ultrasonography in rheumatology clinical practice. Arthritis Care Res (Hoboken) 2012;64:1625–40. doi: 10.1002/acr.21836. [DOI] [PubMed] [Google Scholar]
- 7.Hermann KG, Backhaus M, Schneider U, Labs K, Loreck D, Zühlsdorf S, et al. Rheumatoid arthritis of the shoulder joint: Comparison of conventional radiography, ultrasound, and dynamic contrast-enhanced magnetic resonance imaging. Arthritis Rheum. 2003;48:3338–49. doi: 10.1002/art.11349. [DOI] [PubMed] [Google Scholar]
- 8.Backhaus M, Burmester GR, Gerber T, Grassi W, Machold KP, Swen WA, et al. Guidelines for musculoskeletal ultrasound in rheumatology. Ann Rheum Dis. 2001;60:641–9. doi: 10.1136/ard.60.7.641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Naredo E, Möller I, Moragues C, de Agustín JJ, Scheel AK, Grassi W, et al. Interobserver reliability in musculoskeletal ultrasonography: Results from a ’teach the teachers’ rheumatologist course. Ann Rheum Dis. 2006;65:14–9. doi: 10.1136/ard.2005.037382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Boutry N, Morel M, Flipo RM, Demondion X, Cotten A. Early rheumatoid arthritis: A review of MRI and sonographic findings. AJR Am J Roentgenol. 2007;189:1502–9. doi: 10.2214/AJR.07.2548. [DOI] [PubMed] [Google Scholar]
- 11.Pavlovic V, Dimic A, Milenkovic S, Krtinic D. Serum levels of IL-17, IL-4, and INFγ in Serbian patients with early rheumatoid arthritis. J Res Med Sci. 2014;19:18–22. [PMC free article] [PubMed] [Google Scholar]
- 12.Aryaeian N, Djalali M, Shahram F, Djazayery A, Eshragian MR. Effect of conjugated linoleic acid, Vitamin E, alone or combined on immunity and inflammatory parameters in adults with active rheumatoid arthritis: A randomized controlled trial. Int J Prev Med. 2014;5:1567–77. [PMC free article] [PubMed] [Google Scholar]
- 13.Jafari Shapoorabadi Y, Vahdatpour B, Salesi M, Ramezanian H. Effects of aerobic exercise on hematologic indices of women with rheumatoid arthritis: A randomized clinical trial. J Res Med Sci. 2016;21:9. doi: 10.4103/1735-1995.177356. [DOI] [PMC free article] [PubMed] [Google Scholar]