

Abstract
Background:
Childhood injuries claim around a million lives around the world each year. A community-based study on childhood injuries would provide valuable information on the epidemiology of injuries.
Objective:
To assess the prevalence of unintentional childhood injuries in an urban locality and determine various sociodemo graphic factors associated with childhood injuries.
Methods:
The study was done in urban Delhi among 1,639 children aged less than 18 years. Information on injuries in the last one year was collected. Only those injury episodes where treatment was sought or the child was left disabled after the injury were included. Treatment seeking behavior and the impact of injury on the child and the household were also assessed.
Results:
Among 1,639 children, 102 children suffered 116 episodes of various types of injuries in the last one year. Prevalence of injuries was 7.1% (95% CI: 5.9-8.4). Mean age was 8.5 ± 5.1 years. Prevalence was more in boys (8.4%) than girls (5.1%). Accidental falls (37.1%), dog bites (25%), and road traffic injuries (18.9%) were the three most common modes of injury. Two-thirds of children with injuries were taken to the emergency facility for treatment while 40% resorted to home remedies. Treatment expenses in some families led to the need for borrowing money, additional employment by another family member, and selling of household assets.
Conclusions:
The prevalence of childhood injuries in the past one year was 7.1%. Maximum injuries occurred at home and were mostly accidental falls and dog bites. Childhood injuries caused loss of school attendance and financial burden to the family.
Key words: Childhood, India, injuries, unintentional injuries
Introduction
Childhood injury is a major public health problem that requires urgent attention. Injuries is a health concern in every country around the world, affecting both developed and developing countries, causing over 5.8 million deaths per year or 15,000 deaths per day.[1]
It is a major killer of children throughout the world, responsible for about 950 000 deaths in children and young people under the age of 18 years each year.[2] Unintentional injuries account for almost 90% of these cases. They are the leading cause of death for children aged 10–19 years.[2] Injuries collectively caused 11.2% of DALY’s with many different injuries making important contributions. The majority was contributed by road traffic injuries, which accounted to 27% of total injuries. Overall, according to the Global Burden of Disease study in 2010, injuries contributed to 278, 665,000 DALYs in all age groups.[3]
Most literature on childhood injuries is from hospital-based studies or emergency room data. Since most of the injuries go unreported and are not serious enough to warrant a visit to the hospital, the true burden of injuries in children may be underestimated. Hence, a community based study on childhood injuries would provide valuable information on the epidemiology of injuries. The objective of this study is to study the prevalence of childhood injuries in an urban locality in Delhi and also to determine the various sociodemographic factors associated with childhood injuries.
Materials and Methods
A community-based cross-sectional study was conducted in Dakshinpuri Extension, Dr. Ambedkar Nagar, New Delhi. The Centre for Community Medicine, All India Institute of Medical Sciences, has been working in this area since 2002. The study was based in an urban resettlement area, which included six blocks, with a population of about 30,000. Total number of children under 18 years was approximately 12,000. Data collection was carried out between December 2012 and May 2013. The study population included all children below 18 years who were living in the locality for the past 6 months.
According to Baker, injury is defined as “external force/non contagious substance, striking the body or entering into the body and causing anatomical discontinuity of tissue or derange physiological function of the body.”[4]
In this study, the operational definition used for “Injury” was—all recallable bodily injury—in the last one year to any individual less than 18 years, which were unintentional. It did not include minor injuries, which were not recallable at the time of interview. Injuries that incapacitated the child for a minimum of 1 day from normal activities and also necessitated the need for seeking any form of treatment for the same were included in the study.[5] Mental injury was not included in the study. The informant was the parent or primary caregiver. If the child was more than 10 years old, he/she was also interviewed. The various definitions of unintentional injuries used in the study were adopted from the TEACH-VIP manual developed by WHO.[6]
Sample Size Estimation and Sampling Strategy
Assuming 9% prevalence,[5] 1.5% relative precision, 10% nonresponse rate, the sample size was calculated to be 1,617. Systematic random sampling was carried out, and every 7th house was included in the study. This was derived based on the information that there are about 6,000 households in the study area; assuming that there would be two eligible children per household at least 800 households would be required to capture 1,600 children. So, in order to get 800 households, the sampling interval was calculated to be 6,000/800 = 7.
A pretested questionnaire for estimation of prevalence of childhood injuries and sociodemographic factors associated with different types of injuries was used. The study received ethical clearance from the Ethics Committee of All India Institute of Medical Sciences, New Delhi. Written informed consent was obtained from all the informants.
Statistical Analysis
Data was entered in Epi Info Version 7.0 and an analysis was done in STATA 9.0 (College Station, Texas, USA). Prevalence of childhood injuries was calculated as the number of episodes/100 children. Prevalence of injuries across various subgroups was calculated and compared using chi square test. Univariate and multivariate logistic regression model was applied to find the sociodemographic factors associated with childhood injury, and the results were presented as odds ratio (95% CI). A “P” value of less than 0.05 was taken as statistically significant.
Results
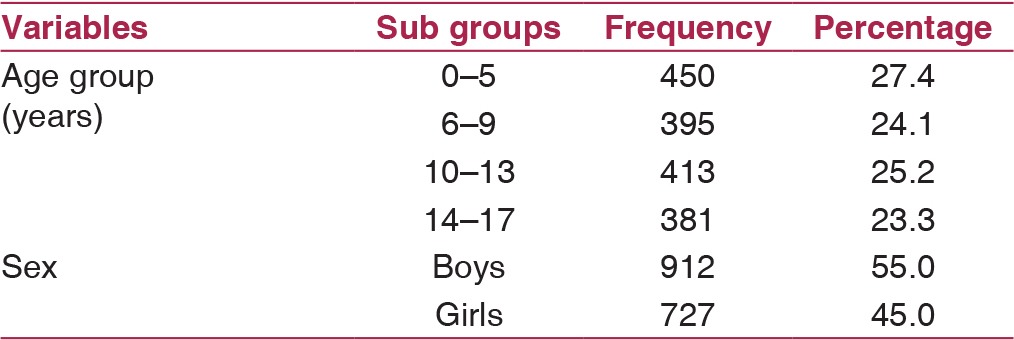
A total of 827 households were approached for the study. Out of these, 82 households were excluded (73 households did not have any children less than 18 years of age and in 9 households the informant could not comprehend the questions). Hence, 745 households were included into the study. Out of these, 21 households were locked and informants in 12 households refused to give consent. Finally, 712 households were included and 1,639 eligible children present in these households were enrolled. The nonresponse rate came out to be 4.4%. Among the 1,639 children, 27.4% were in the age group of 0–5 years and 25.2% of the children were in the age group of 10–13 years. Out of the total 1,639 children, 912 (55%) were boys and 727 (45%) were girls. [Table 1] shows across all age groups, the number of boys was greater than girls.
Table 1.
Age and sex wise distribution of the participants (n = 1,639)
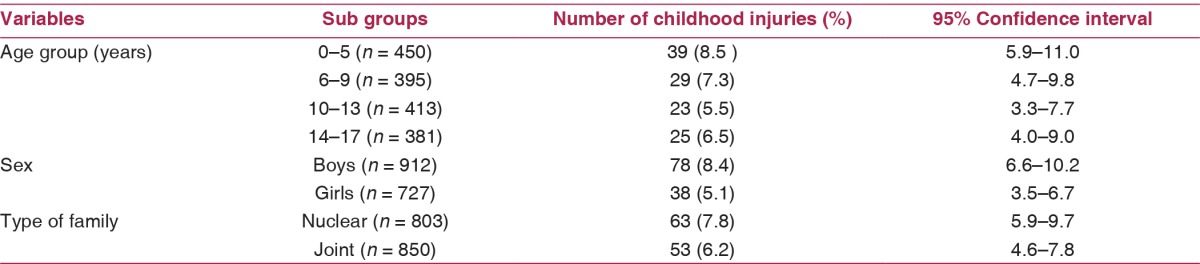
Out of the 1,639 children, 102 children had history of one or more of the injuries in the past one year. Since some of them had sustained more than one injury, there were 116 different episodes of injuries. The prevalence of childhood injuries in the urban resettlement colony in the last one year was 116/1639 = 7.1% (95% CI is 5.9–8.4%). The mean age of children with injuries was 8.5 ± 5.1 years. The prevalence of childhood injuries was maximum in the age group of 0–5 years, boys, and nuclear families [Table 2].
Table 2.
Distribution of childhood injuries by sociodemographic factors (n = 1,639)
The childhood injuries were categorized broadly under road traffic injuries, accidental falls, burns, dog bites, poisoning, and miscellaneous injuries. Of the 116 episodes, 37% of injuries were due to accidental falls followed by dog bites and road traffic injuries. Of the 116 episodes, 43% of the injury episodes occurred at home, followed by road and play ground. [Figures 1 and 2] show the distribution of various modes and places of injuries.
Figure 1.
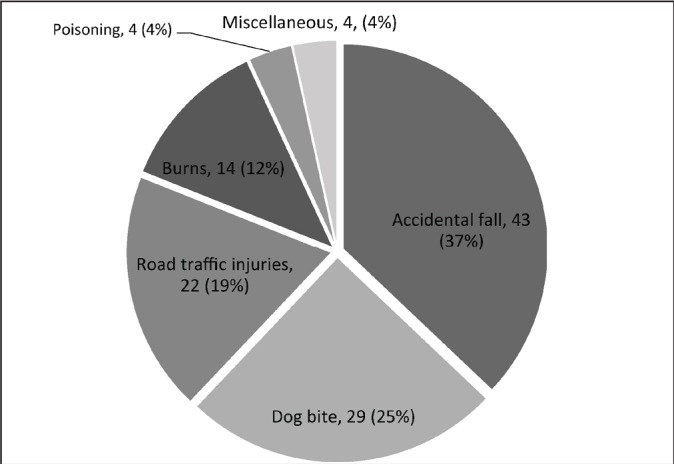
Distribution by modes of injury (n=116)
Figure 2.
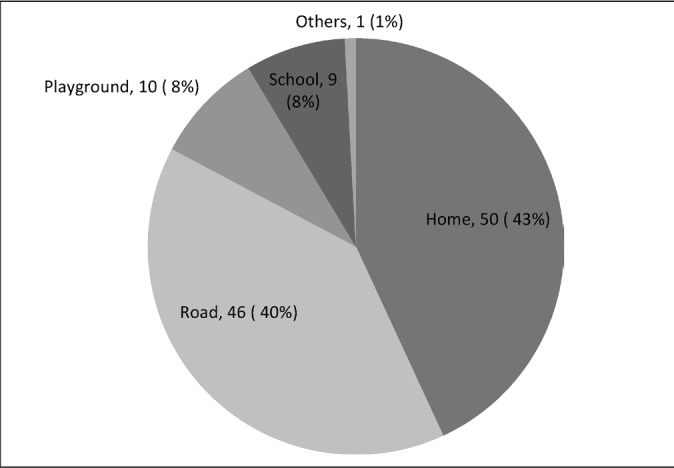
Distribution by place of injury (n=116)
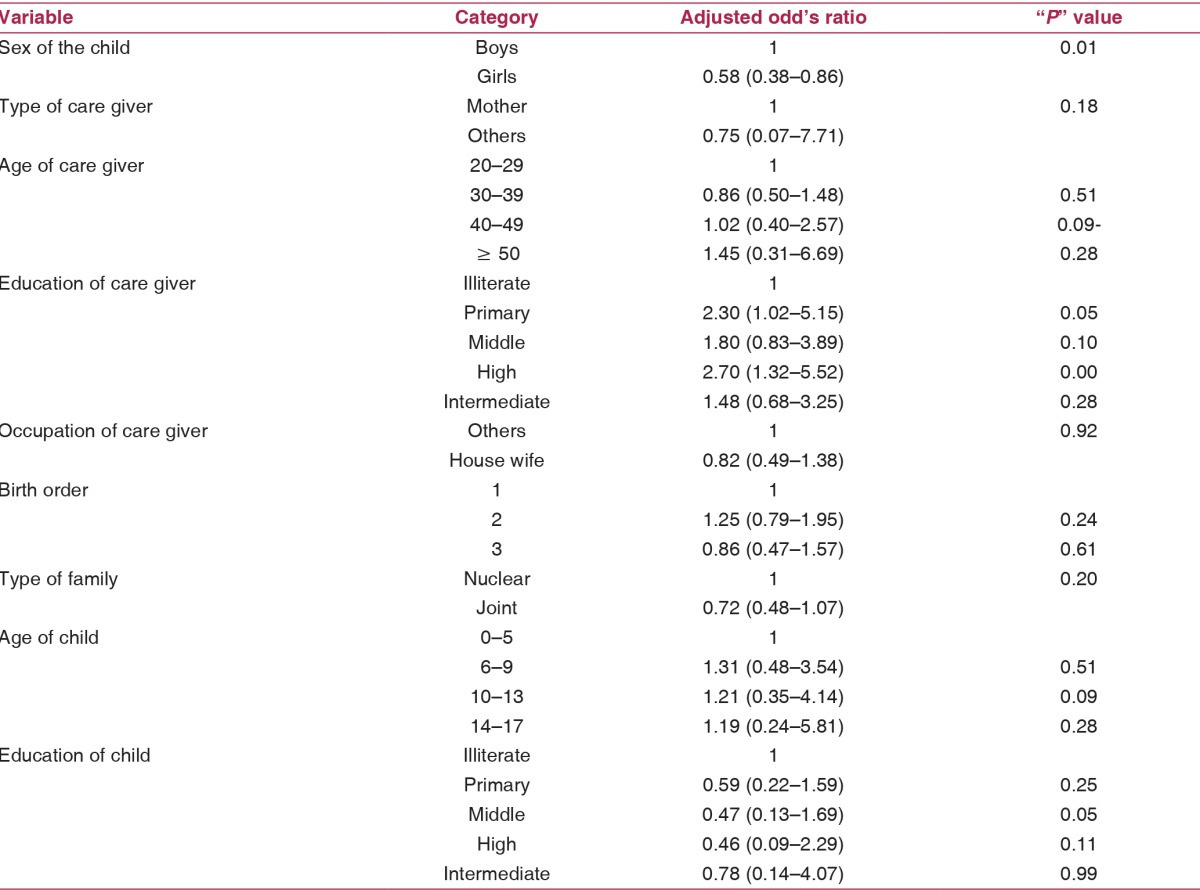
Childhood injuries were common in boys, adjusted odd’s ratio of 0.58 (0.38–0.86). Education of care giver also yielded significant adjusted odd’s ratio. However, multivariate analysis of sociodemographic variables like type of care giver, age of care giver, occupation of care giver, the type of family, birth order, child’s age, and education did not have any statistically significant difference [Table 3].
Table 3.
Distribution of childhood injuries by various sociodemographic variables
Health Seeking Practices and Injury Burden
In 53% of the injuries, home remedy was the first resort that included turmeric paste for swelling and chili powder application for dog bites. 63% were taken to the emergency facility in case of accidental falls. Overall because of injuries, a child had to take sick leave from school for an average of 7 days (SD-9.7) with a range of 1–50 days. Number of leaves from school was maximum in case of road traffic injuries, which was an average of 17.6 days (SD-14.1). Financial burden of households due to the injuries is shown in [Table 4]. Some families had resorted to borrowing and selling of household assets to meet treatment expenses.
Table 4.
Impact of injuries on the financial condition of households (n = 116)

The maximum expenses incurred by the family to treat the injured child were in case of road traffic injuries. On an average, a family had to spend INR 3,759 for treatment. The expenses in case of a road traffic injury ranged from INR 200 to INR 15,000. Overall, the expenses incurred by the family to treat an injured child were on an average INR 1,408, ranging from INR 100 to 15,000.
Discussion
The prevalence of childhood injuries in the present study was 7.1%. The prevalence of childhood injuries was more among boys, under-five children and nuclear families. Falls were the most common mode of injury and home was the most common place of injury.
The community-based study done in Municipal Corporation of Delhi (MCD) area by the WHO[5] estimated an annual incidence rate of 90.7/1,000 population in children aged below 5 years. Similar findings were reported by Zaidi et al.[7] (11%) and Mohan D et al.[8] (Annual incidence rate of 6,737/1, 00,000). In this study, 33.6% of injuries occurred in children under 5 years of age. In fact the prevalence among under-fives was the highest (8.5%) in all the age groups of children studied. Similar finding was reported in the WHO study[5] and Mahalakshmy et al.[9] In the present study, boys suffered 70% of all injuries while girls suffered 30%. The prevalence in boys was 8.4% (95% CI: 6.6-10.2) and in girls it was 5.1% (95% CI:3.5-6.7). Similar finding was also reported by Zaidi et al.[7] in which boys (65%) had more domestic accidents as compared to girls (35%). In WHO study,[5] the annual incidence rate was almost double in boys (94.9) as compared to that in girls (47.6) similar to Mohan D et al.,[8] Mahalakshmy T et al.,[9]and Lasi et al.[10] In the present study, the prevalence of injuries was reported more in nuclear families as compared to joint families. It was 7.8% (95% CI: 5.9-9.7) in the former and 6.2% (95% CI: 4.6-7.8) in the latter. This similar finding was found in Growing up in Australia study.[11] These findings suggest that there is a family related psychosocial association with the incidence of childhood injuries. Nuclear families tend to have less care and low psychosocial support as compared to joint families, which tend to provide more care, attention, and psychosocial support to the growing children in the family. In the present study, the prevalence of injuries was less in 1st birth order children as compared to children with subsequent birth order. It was 6.6% (95% CI: 4.7-8.4) in the former as compared to the latter 7.2% (95% CI: 5.6-8.9). Similar finding was found in the study conducted by Orton E et al.,[12] where they reported increased odds of having childhood injury in various modes of injury with an increasing birth order.
In this study, 37.1% of injuries in children were due to accidental falls. Falls contributed to majority of injuries in studies conducted by Zia et al.,[13] Zaidi et al.,[7] the WHO Study,[5] Mohan D et al.,[8] Mahalakshmy et al.,[9] and Lasi S et al.[10] In developing countries like India, falls are usually the most common cause of injury seen in hospitals, accounting for 25–52% of all treated child injuries.[14] Home was the most common place (43.1%) for occurrence of injuries in the present study. Zia et al.,[13] Zaidi et al.,[7] the WHO study,[5] Mohan D et al.,[8] Mahalakshmy et al.,[9]and Lasi S et al.,[10] reported that majority of injuries studied occurred at home. Home appears to be the most common site of injury in young children as they spend most of their time there. So, on combining falls, homes, and under-fives, it is evident that childhood injuries are more likely at home where under-five children play and spend most of their time, making them prone to accidents and sustain injuries.
The strength of the study is that it is a community-based study with adequate sample size and good precision with a response rate of 95.6%. The locality and the households surveyed closely approximate to a typical low-middle income urban colony in India. A major limitation of this study is that the injury episodes were self-reported, and injury episodes may have been underestimated due to recall bias. Medical records or any investigation pertaining to the treatment sought for injury were hardly available in majority of households.
Conclusion
In conclusion, injuries were traditionally viewed as random unavoidable “accidents” but a better understanding of the nature of injuries has changed these perspectives. Both intentional and unintentional injuries are increasingly being viewed as largely preventable events. Childhood injuries cause loss of school attendance and financial burden to the family. As a result of this shift in perception, injuries and health implications have demanded the attention of decision makers worldwide, sensitizing the need for policy measures to educate the community and making efforts to provide a safe environment for children.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
We acknowledge the families who participated in this study.
References
- 1.WHO Injuries and violence: The facts. 1st ed. Geneva, Switzerland: World Health Organization; 2010. [Google Scholar]
- 2.World Health Organization, UNICEF World report on child injury prevention. 1st ed. Geneva, Switzerland: World Health Organization; 2008. [Google Scholar]
- 3.Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Study 2010. The Lancet. 2012;380:2197–223. doi: 10.1016/S0140-6736(12)61689-4. [DOI] [PubMed] [Google Scholar]
- 4.Susan P, Baker, Brian O'Neill, Marvin J, Ginsburg, Guohua Li. The injury fact book. 2nd ed. Lexington, MA: Lexington Books; 1992. [Google Scholar]
- 5.WHO Publication: Injury Prevention Control: An Epidemiological study of injuries in the area of Municipal Corporation of Delhi; Disability/Injury Prevention Rehabilitation, Department of Sustainable development and Healthy Environment. WHO Regional Office for South East Asia, New Delhi. 2003 Sep [Google Scholar]
- 6.Training Educating and Advancing Collaboration in Health on Violence and Injury Prevention Users' manual. Geneva, Switzerland: World Health Organization; [Last accessed 2015 March 3]. Available from: http://whqlibdoc.who.int/publications/2012/9789241503464_eng.pdf?ua=1 . [Google Scholar]
- 7.Zaidi SHN, Khan Z, Khalique N. Injury pattern in children: a population-based study. Indian Journal of Community Health. 2013;25:45–51. [Google Scholar]
- 8.Mohan D, Kumar A, Varghese M. Childhood injuries in rural north India. International Journal of Injury Control and Safety Promotion. 2010;17:45–52. doi: 10.1080/17457300903524862. [DOI] [PubMed] [Google Scholar]
- 9.Mahalakshmy T, Dongre AR, Kalaiselvan G. Epidemiology of childhood injuries in rural Puducherry, South India. Indian Journal of Pediatrics. 2011;78:821–25. doi: 10.1007/s12098-010-0343-3. [DOI] [PubMed] [Google Scholar]
- 10.Lasi S, Rafique G, Peermohamed H. Childhood injuries in Pakistan: results from two communities. Journal of Health and Population Nutrition. 2010;28:392–98. doi: 10.3329/jhpn.v28i4.6046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Richardson N, Higgins DJ, Bromfield LM, Tooley G, Stokes M. The relationship between childhood injuries and family type. Family matters. 2005;72:44–9. [Google Scholar]
- 12.Orton E, Kendrick D, West J, Tata LJ. Independent risk factors for injury in pre-school children: three population-based nested case-control studies using routine primary care data. PLOS One. 2012;7 doi: 10.1371/journal.pone.0035193. e35193-doi:10.1371/journal.pone.0035193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Zia N, Khan UR, Razzak JA, Puvanachandra P, Hyder AA. Understanding unintentional childhood home injuries: pilot surveillance data from Karachi, Pakistan. BMC Research Notes. 2012;5:37. doi: 10.1186/1756-0500-5-37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Khambalia A, Joshi P, Brussoni M, Raina P, Morrangiello B, Macarthur C. Risk factors for unintentional injuries due to falls in children aged 0-6 years: a systematic review. Injury prevention. 2006;12:378–85. doi: 10.1136/ip.2006.012161. [DOI] [PMC free article] [PubMed] [Google Scholar]